
Pulmonary Rehabilitation in SARS-CoV-2: A Systematic Review and Meta-Analysis of Post-Acute Patients
 ,
,  , ,
, ,  and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Eligibility Criteria
2.2. Outcome Measures
2.3. Data Sources and Search Strategy
2.4. Data Screening and Extraction
2.5. Quality Assessment
2.6. Certainty of Evidence
2.7. Data Synthesis
3. Results
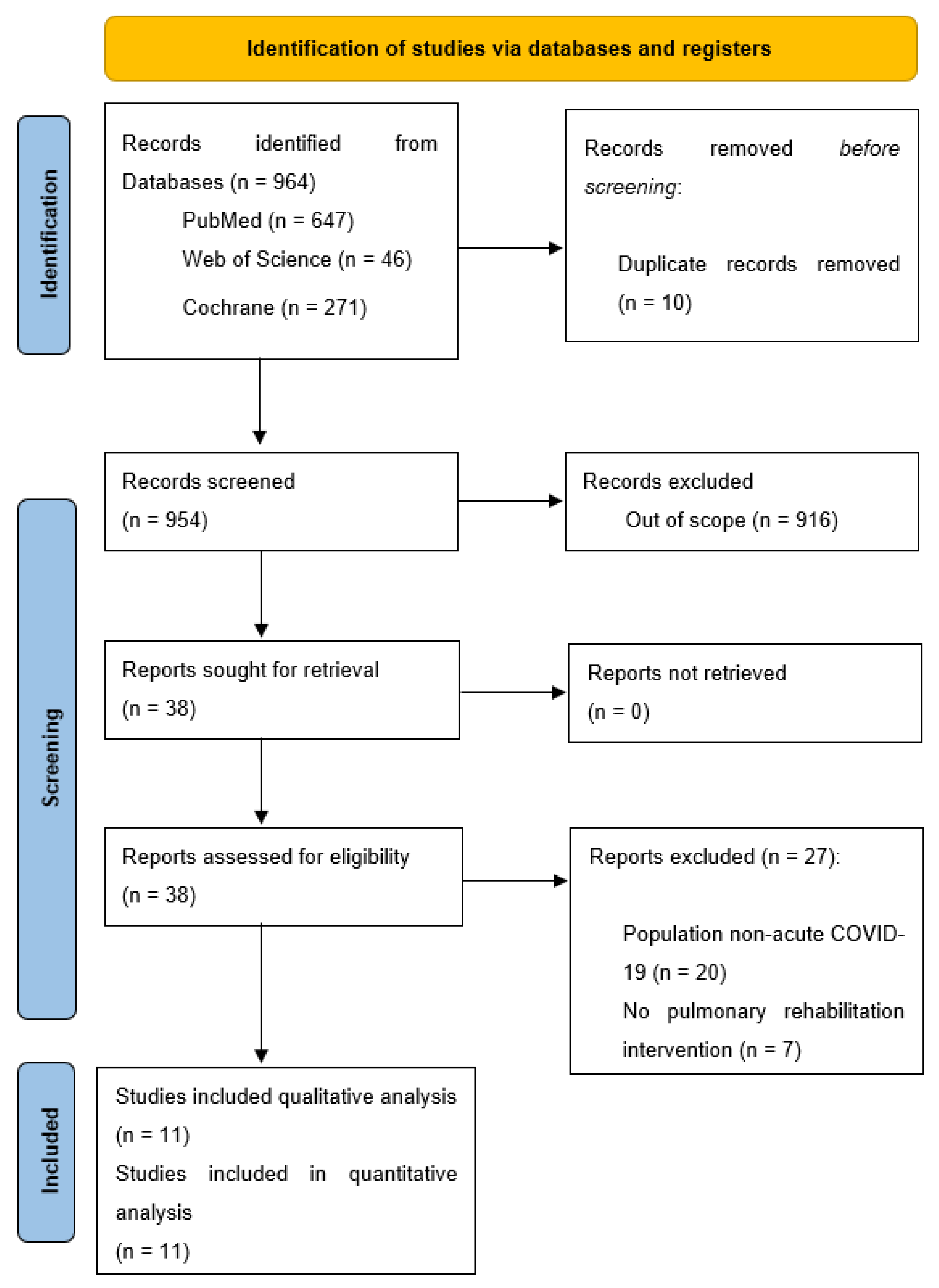
3.1. Characteristics of the Included Studies
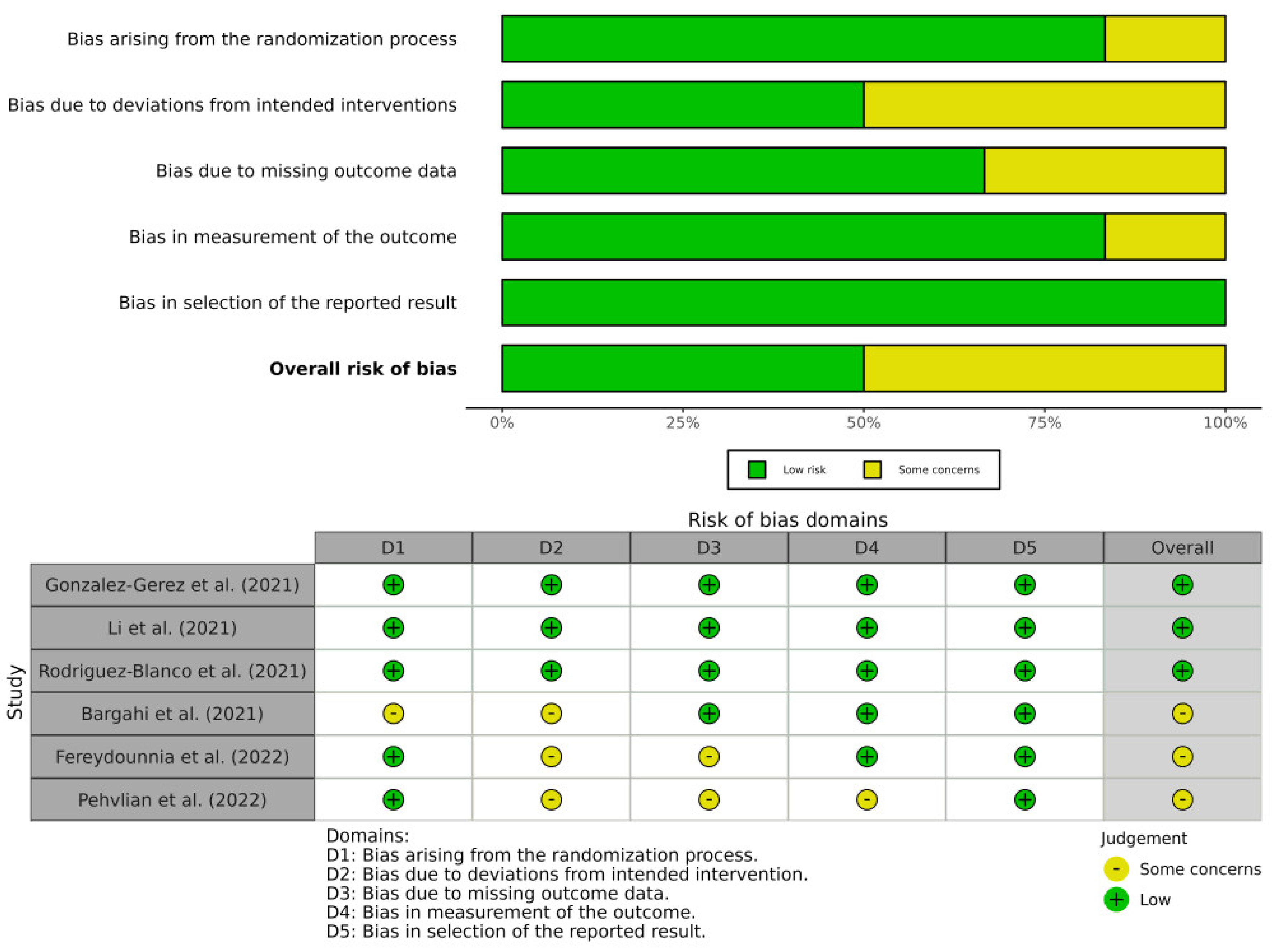
3.2. Methodological Quality and Risk of Bias of the Included Studies
3.3. Quality of Evidence
3.4. Data from Studies
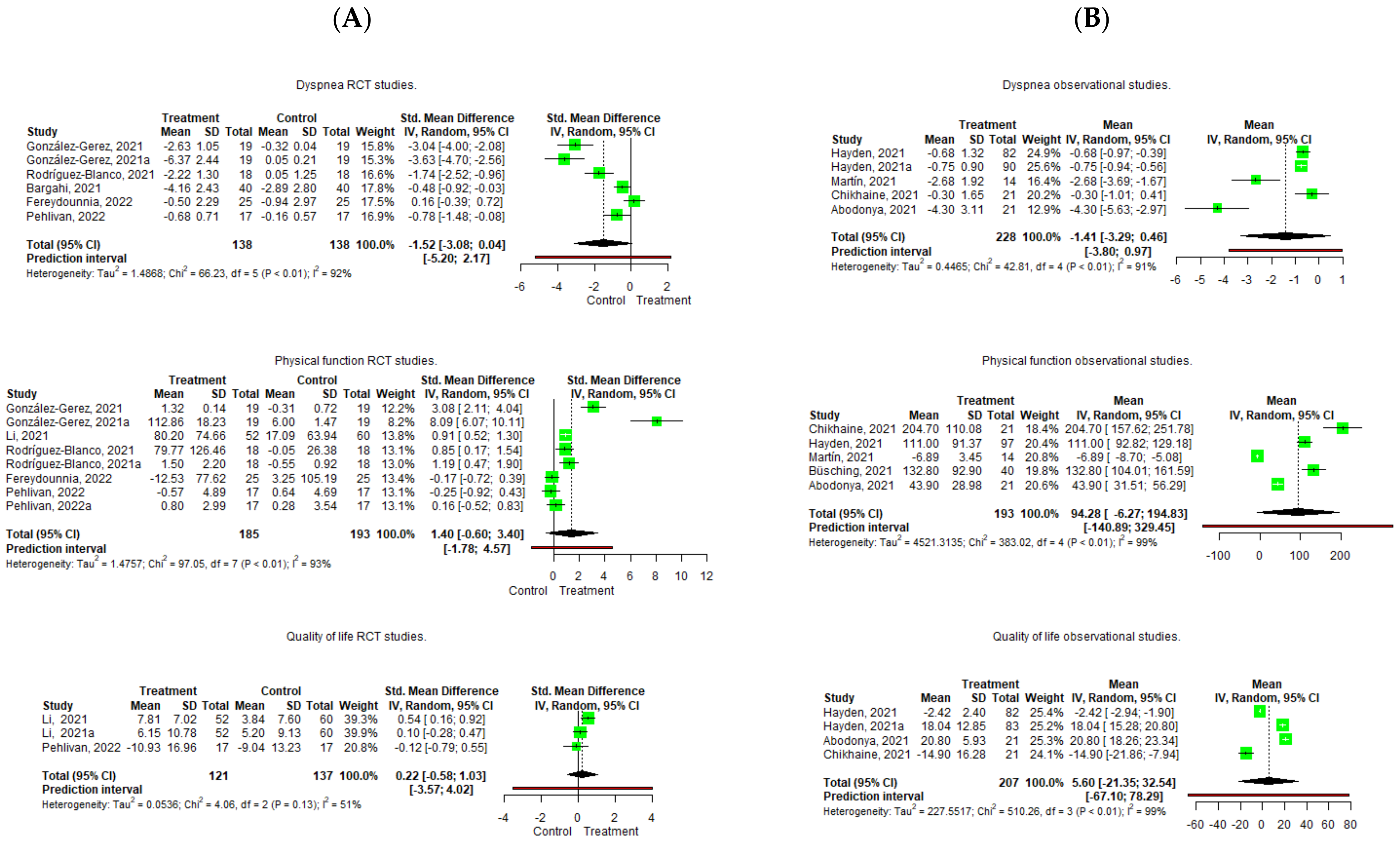
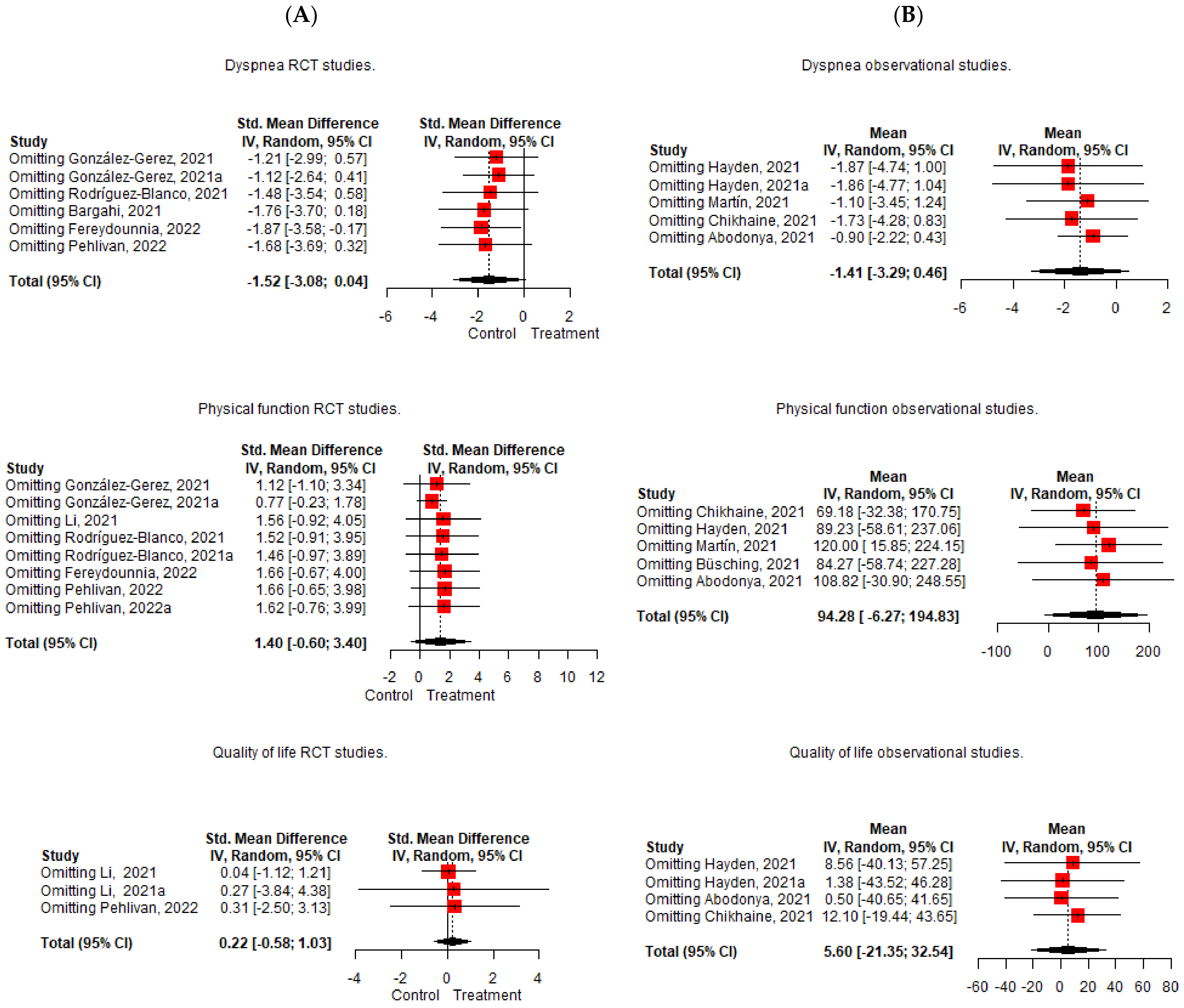
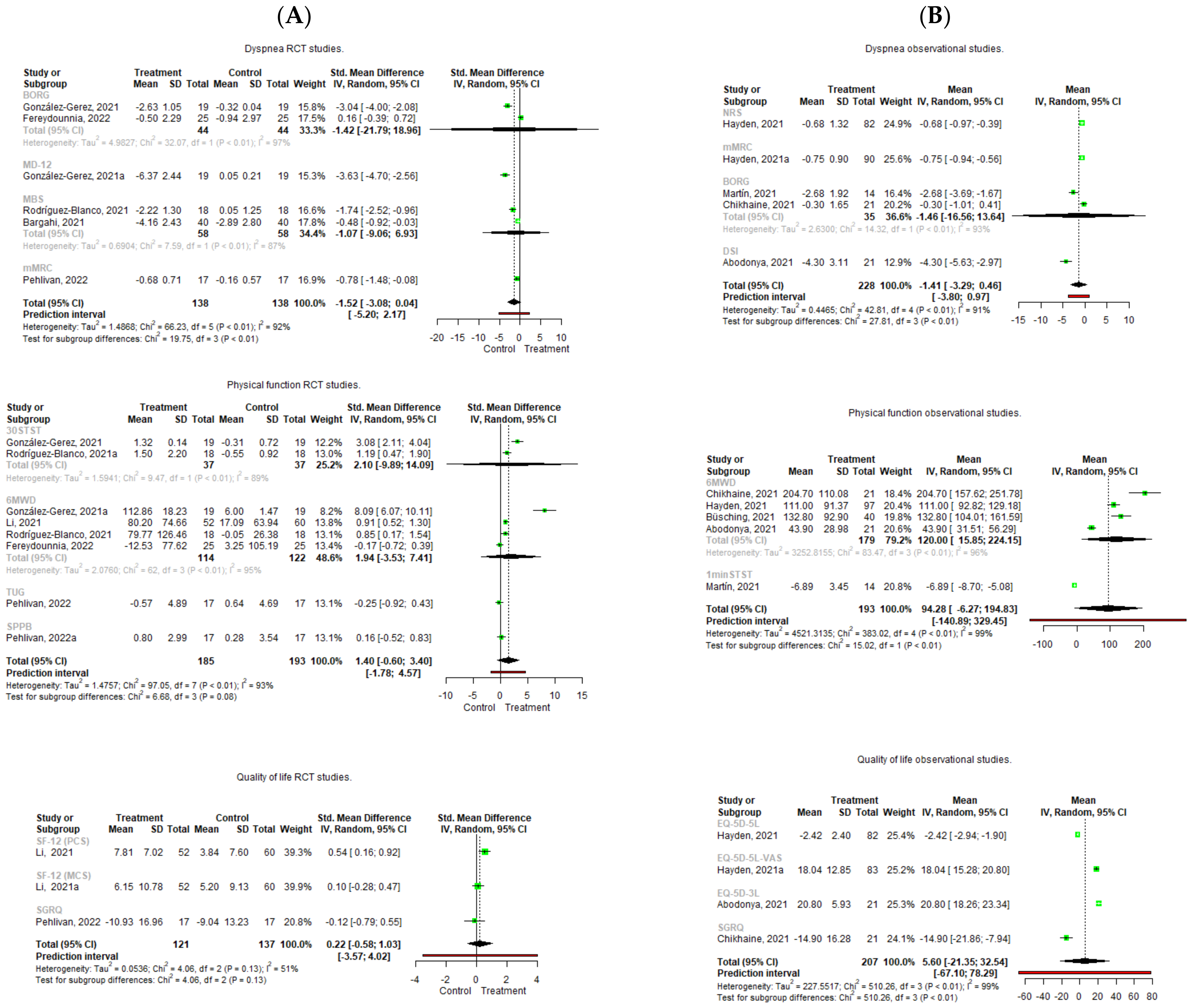
3.4.1. Effect of Pulmonary Rehabilitation on Dyspnea
3.4.2. Effect of Pulmonary Rehabilitation on Physical Function
3.4.3. Effect of Pulmonary Rehabilitation on Quality of Life
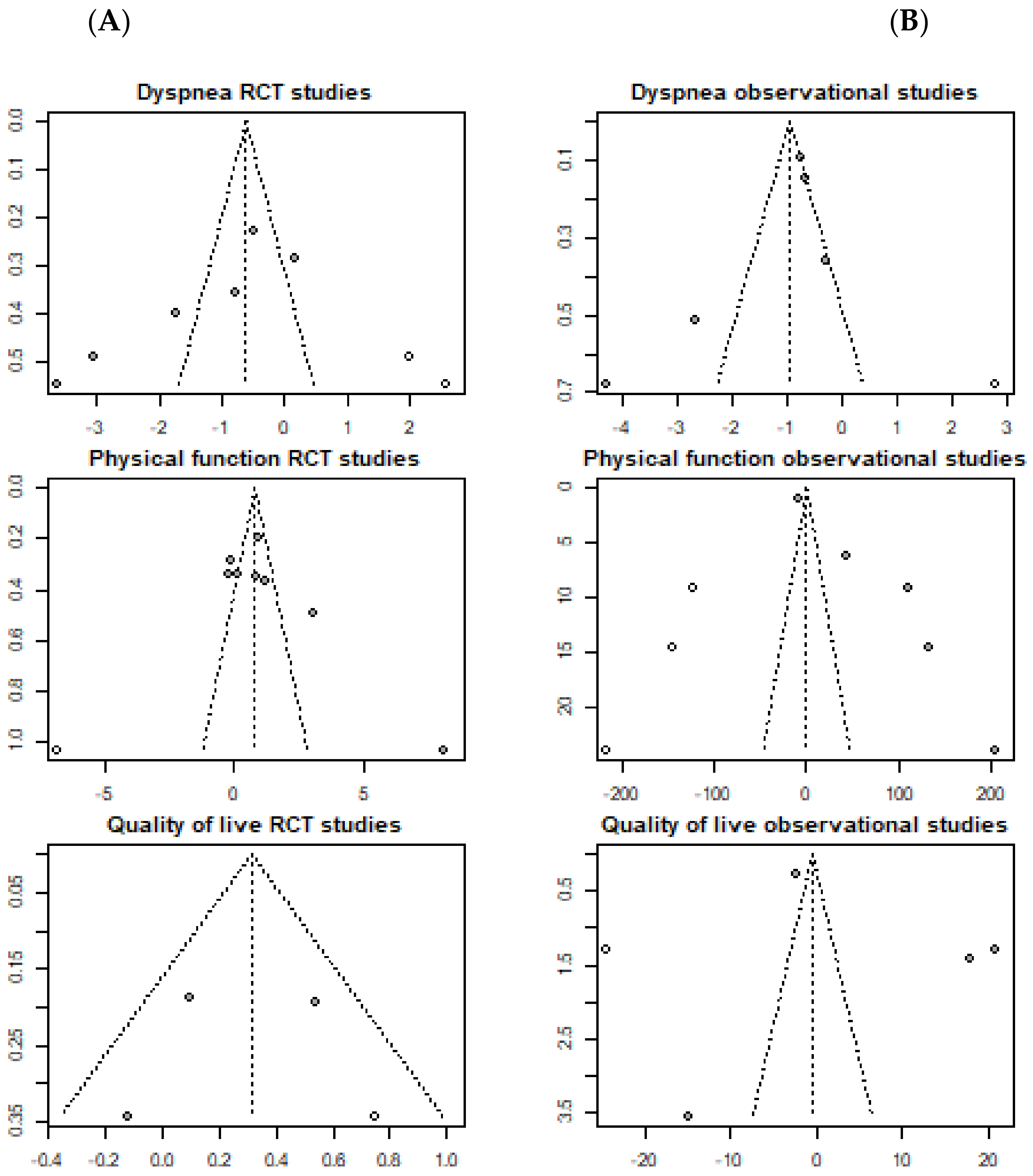
3.4.4. Publication Bias of Included Studies
4. Discussion
4.1. Future Directions
4.2. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Micah, A.E.; Cogswell, I.E.; Cunningham, B.; Ezoe, S.; Harle, A.C.; Maddison, E.R.; McCracken, D.; Nomura, S.; Simpson, K.E.; Stutzman, H.N.; et al. Tracking development assistance for health and for COVID-19: A review of development assistance, government, out-of-pocket, and other private spending on health for 204 countries and territories, 1990–2050. Lancet 2021, 398, 1317–1343. [Google Scholar] [CrossRef] [PubMed]
- Pancera, S.; Bianchi, L.; Porta, R.; Galeri, S.; Carrozza, M.C.; Villafañe, J.H. Feasibility of subacute rehabilitation for mechanically ventilated patients with COVID-19 disease: A retrospective case series. International journal of rehabilitation research. Internationale Zeitschrift fur Rehabilitationsforschung. Rev. Int. Rech. Readapt. 2021, 44, 77–81. [Google Scholar]
- Fiore, E.; Corbellini, C.; Acucella, L.; Gargano, S.; Sánchez-Romero, E.A.; Cotella, D.; Villafañe, J.H. Dolor musculoesquelético en supervivientes del COVID-19 tras la hospitalización: Una breve revision (Musculoskeletal pain related to COVID-19 survivors after hospitalization: A short review). Retos 2022, 44, 789–795. [Google Scholar] [CrossRef]
- Romero, E.A.S.; Rolando, L.M.; Villafañe, J.H. Impact of Lockdown on Patients with Fibromyalgia. Electron. J. Gen. Med. 2022, 19, em366. [Google Scholar] [CrossRef] [PubMed]
- Ballesteros Reviriego, G.; Planas Pascual, B.; Rojo Ruiz, A.; Sánchez Romero, E.A.; Corbelini, C.; Villafañe, J.H. Spanish Experience of Pulmonary Rehabilitation Efficacy for Patients Affected by the Novel SARS-CoV-2 (COVID-19): A Case Report. Top. Geriatr. Rehabil. 2020, 36, 212–214. [Google Scholar] [CrossRef]
- Sánchez Romero, E.A.; Alonso Pérez, J.L.; Vinuesa Suárez, I.; Corbellini, C.; Villafañe, J.H. Spanish experience on the efficacy of airways clearance techniques in SARS-CoV-2 (COVID-19) at intensive care unit: An editorial and case report. SAGE Open Med. Case Rep. 2022, 10. [Google Scholar] [CrossRef]
- Barker-Davies, R.M.; O’Sullivan, O.; Senaratne, K.P.P.; Baker, P.; Cranley, M.; Dharm-Datta, S.; Ellis, H.; Goodall, D.; Gough, M.; Lewis, S.; et al. The Stanford Hall consensus statement for post-COVID-19 rehabilitation. Br. J. Sports Med. 2020, 54, 949–959. [Google Scholar] [CrossRef]
- Corbellini, C.; Villafane, J.; Gugliotta, E.; Tavella, S.; Zampese, S.; Pessina, P.; Monti, R.; Carnuccio, C.; Romero, E.A.S.; Meroni, R. Late Breaking Abstract—Pulmonary Rehabilitation in Post—COVID Subjects with Moderate Lung Restriction, A Case Series. Eur. Respir. J. 2021, 58 (Suppl. 65), PA2003. [Google Scholar] [CrossRef]
- Sheehy, L.M. Considerations for Postacute Rehabilitation for Survivors of COVID-19. JMIR Public Health Surveill. 2020, 6, e19462. [Google Scholar] [CrossRef]
- Torres-Castro, R.; Vasconcello-Castillo, L.; Alsina-Restoy, X.; Solis-Navarro, L.; Burgos, F.; Puppo, H.; Vilaró, J. Respiratory function in patients post-infection by COVID-19: A systematic review and meta-analysis. Pulmonology 2021, 27, 328–337. [Google Scholar] [CrossRef]
- Mo, X.; Jian, W.; Su, Z.; Chen, M.; Peng, H.; Peng, P.; Lei, C.; Chen, R.; Zhong, N.; Li, S. Abnormal pulmonary function in COVID-19 patients at time of hospital discharge. Eur. Respir. J. 2020, 55, 2001217. [Google Scholar] [CrossRef] [PubMed]
- Corbellini, C.; Vinuesa, I.; Romero, E.A.S.; Reviriego, G.B.; Bernal-Planas, P.; Villafañe, J.H. Late Breaking Abstract—Early ICU physiotherapy on SARS-CoV-2 patients: A Spanish experience case series. Eur. Respir. J. 2020, 56 (Suppl. 64), 334. [Google Scholar] [CrossRef]
- Chung, F.; Dean, E. Pathophysiology and cardiorespiratory consequences of interstitial lung disease—Review and clinical implications: A special communication. Phys. Ther. 1989, 69, 956–966. [Google Scholar] [CrossRef] [PubMed]
- Hansen, J.E.; Wasserman, K. Pathophysiology of activity limitation in patients with interstitial lung disease. Chest 1996, 109, 1566–1576. [Google Scholar] [CrossRef] [PubMed]
- Corbellini, C.; Rossino, E.; Massaccesi, R.; Battaglino, A.; Pedersini, P.; Sánchez Romero, E.A.; Villafañe, J.H. Improvements in Perimeter Thoracic Mobility on Patients with COPD after Pulmonary Rehabilitation: A Case Series. Electron. J. Gen. Med. 2022, 19, em361. [Google Scholar] [CrossRef]
- Pedersini, P.; Corbellini, C.; Villafañe, J.H. Italian Physical Therapists’ Response to the Novel COVID-19 Emergency. Phys. Ther. 2020, 100, 1049–1051. [Google Scholar] [CrossRef]
- Nicolás Cuenca-Zaldivar, J.; Acevedo, Á.M.; Fernández-Carnero, J.; Sánchez-Romero, E.A.; Villafañe, J.H.; Barragán Carballar, C. Effects of a Multicomponent Exercise Program on Improving Frailty in Post-COVID-19 Older Adults after Intensive Care Units: A Single-Group Retrospective Cohort Study. Biology 2022, 11, 1084. [Google Scholar] [CrossRef]
- Martínez Rolando, L.; Villafañe, J.H.; Cercadillo García, S.; Sanz Argüello, A.; Villanueva Rosa, M.; Sánchez Romero, E.A. Multicomponent Exercise Program to Improve the Immediate Sequelae of COVID-19: A Prospective Study with a Brief Report of 2-Year Follow-Up. Int. J. Environ. Res. Public Health 2022, 19, 12396. [Google Scholar] [CrossRef]
- Sánchez Romero, E.A.; Fernández Carnero, J.; Alonso Pérez, J.L.; Martínez Rolando, L.; Villafañe, J.H. Addressing post-COVID-19 musculoskeletal symptoms through telemedicine: A study protocol. F1000Research 2022, 11, 898. [Google Scholar] [CrossRef]
- Bolton, C.E.; Bevan-Smith, E.F.; Blakey, J.D.; Crowe, P.; Elkin, S.L.; Garrod, R.; Greening, N.J.; Heslop, K.; Hull, J.H.; Man, W.D.-C.; et al. British Thoracic Society guideline on pulmonary rehabilitation in adults. Thorax 2013, 68 (Suppl. 2), ii1–ii30. [Google Scholar] [CrossRef] [Green Version]
- Spruit, M.A.; Singh, S.J.; Garvey, C.; ZuWallack, R.; Nici, L.; Rochester, C.; Hill, K.; Holland, A.E.; Lareau, S.C.; Man, W.D.-C.; et al. An official American Thoracic Society/European Respiratory Society statement: Key concepts and advances in pulmonary rehabilitation. Am. J. Respir. Crit. Care Med. 2013, 188, e13–e64. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Corbellini, C.; Tavella, S.; Gugliotta, E.; Zampese, S.; Romero, E.A.S.; Villafane, J. Hypercapnia and Functional Improvements during Pulmonary Rehabilitation. Eur. Respir. J. 2021, 58, PA1827. [Google Scholar] [CrossRef]
- Dowman, L.; Hill, C.J.; Holland, A.E. Pulmonary rehabilitation for interstitial lung disease. Cochrane Database Syst. Rev. 2014, 2014, CD006322. [Google Scholar] [CrossRef] [PubMed]
- Nici, L.; Donner, C.; Wouters, E.; Zuwallack, R.; Ambrosino, N.; Bourbeau, J.; Carone, M.; Celli, B.; Engelen, M.; Fahy, B.; et al. American Thoracic Society/European Respiratory Society statement on pulmonary rehabilitation. Am. J. Respir. Crit. Care Med. 2006, 173, 1390–1413. [Google Scholar] [CrossRef] [PubMed]
- Rodriguez-Morales, A.J.; Cardona-Ospina, J.A.; Gutiérrez-Ocampo, E.; Villamizar-Peña, R.; Holguin-Rivera, Y.; Escalera-Antezana, J.P.; Alvarado-Arnez, L.E.; Bonilla-Aldana, D.K.; Franco-Paredes, C.; Henao-Martinez, A.F.; et al. Clinical, laboratory and imaging features of COVID-19: A systematic review and meta-analysis. Travel Med. Infect. Dis. 2020, 34, 101623. [Google Scholar] [CrossRef] [PubMed]
- Yang, J.; Zheng, Y.; Gou, X.; Pu, K.; Chen, Z.; Guo, Q.; Ji, R.; Wang, H.; Wang, Y.; Zhou, Y. Prevalence of comorbidities and its effects in patients infected with SARS-CoV-2: A systematic review and meta-analysis. Int. J. Infect. Dis. 2020, 94, 91–95. [Google Scholar] [CrossRef] [PubMed]
- Ahmed, I.; Mustafaoglu, R.; Yeldan, I.; Yasaci, Z.; Erhan, B. Effect of Pulmonary Rehabilitation Approaches on Dyspnea, Exercise Capacity, Fatigue, Lung Functions, and Quality of Life in Patients With COVID-19: A Systematic Review and Meta-analysis. Arch. Phys. Med. Rehabil. 2022, 103, 2051–2062. [Google Scholar] [CrossRef]
- Vieira AG da, S.; Pinto, A.C.P.N.; Garcia, B.M.S.P.; Eid, R.A.C.; Mól, C.G.; Nawa, R.K. Telerehabilitation improves physical function and reduces dyspnoea in people with COVID-19 and post-COVID-19 conditions: A systematic review. J. Physiother. 2022, 68, 90–98. [Google Scholar] [CrossRef]
- Moher, D.; Shamseer, L.; Clarke, M.; Ghersi, D.; Liberati, A.; Petticrew, M.; Shekelle, P.; Stewart, L.A. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015 statement. Syst. Rev. 2015, 4, 148–160. [Google Scholar] [CrossRef] [Green Version]
- Sterne, J.A.C.; Savović, J.; Page, M.J.; Elbers, R.G.; Blencowe, N.S.; Boutron, I.; Cates, C.J.; Cheng, H.Y.; Corbett, M.S.; Eldridge, S.M.; et al. RoB 2: A revised tool for assessing risk of bias in randomised trials. BMJ 2019, 366, l4898. [Google Scholar] [CrossRef] [Green Version]
- Ma, L.L.; Wang, Y.Y.; Yang, Z.H.; Huang, D.; Weng, H.; Zeng, X.T. Methodological quality (risk of bias) assessment tools for primary and secondary medical studies: What are they and which is better? Mil. Med. Res. 2020, 7, 7. [Google Scholar] [CrossRef] [PubMed]
- Ejiri, M.; Kawai, H.; Ishii, K.; Oka, K.; Obuchi, S. Predictors of older adults’ objectively measured social isolation: A systematic review of observational studies. Arch. Gerontol. Geriatr. 2021, 94, 104357. [Google Scholar] [CrossRef] [PubMed]
- Fingleton, C.; Smart, K.; Moloney, N.; Fullen, B.M.; Doody, C. Pain sensitization in people with knee osteoarthritis: A systematic review and meta-analysis. Osteoarthr. Cartil. 2015, 23, 1043–1056. [Google Scholar] [CrossRef] [Green Version]
- Sánchez Romero, E.A.; Martínez-Pozas, O.; García-González, M.; de-Pedro, M.; González-Álvarez, M.E.; Esteban-González, P.; Cid-Verdejo, R.; Villafañe, J.H. Association between Sleep Disorders and Sleep Quality in Patients with Temporomandibular Joint Osteoarthritis: A Systematic Review. Biomedicines 2022, 10, 2143. [Google Scholar] [CrossRef] [PubMed]
- McHugh, M.L. Interrater reliability: The kappa statistic. Biochem. Med. 2012, 22, 276–282. [Google Scholar] [CrossRef]
- Schulté, B.; Nieborak, L.; Leclercq, F.; Villafañe, J.H.; Romero, E.A.S.; Corbellini, C. The Comparison of High-Intensity Interval Training Versus Moderate-Intensity Continuous Training after Coronary Artery Bypass Graft: A Systematic Review of Recent Studies. J. Cardiovasc. Dev. Dis. 2022, 9, 328. [Google Scholar] [CrossRef]
- Guyatt, G.H.; Oxman, A.D.; Vist, G.E.; Kunz, R.; Falck-Ytter, Y.; Alonso-Coello, P.; Schünemann, H.J. GRADE: An emerging consensus on rating quality of evidence and strength of recommendations. BMJ 2008, 336, 924–926. [Google Scholar] [CrossRef] [Green Version]
- Andrews, J.; Guyatt, G.; Oxman, A.D.; Alderson, P.; Dahm, P.; Falck-Ytter, Y.; Nasser, M.; Meerpohl, J.; Post, P.N.; Kunz, R.; et al. GRADE guidelines: 14. Going from evidence to recommendations: The significance and presentation of recommendations. J. Clin. Epidemiol. 2013, 66, 719–725. [Google Scholar] [CrossRef]
- Meléndez Oliva, E.; Villafañe, J.H.; Alonso Pérez, J.L.; Sal, A.A.; Carlier, G.M.; García, A.Q.; Turroni, S.; Martínez-Pozas, O.; Izquierdo, N.V.; Romero, E.A.S. Effect of Exercise on Inflammation in Hemodialysis Patients: A Systematic Review. J. Pers. Med. 2022, 12, 1188. [Google Scholar] [CrossRef]
- Luo, D.; Wan, X.; Liu, J.; Tong, T. Optimally estimating the sample mean from the sample size, median, mid-range, and/or mid-quartile range. Stat. Methods Med. Res. 2018, 27, 1785–1805. [Google Scholar] [CrossRef] [Green Version]
- Shi, J.; Luo, D.; Weng, H.; Zeng, X.; Lin, L.; Chu, H.; Tong, T. Optimally estimating the sample standard deviation from the five-number summary. Res. Synth. Methods. 2020, 11, 641–654. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.P.T.; Thomas, J.; Chandler, J.; Cumpston, M.; Li, T.; Page, M.J.; Welch, V.A. (Eds.) Cochrane Handbook for Systematic Reviews of Interventions; Wiley: Chichester, UK, 2019. [Google Scholar] [CrossRef]
- Rosenthal, R. Meta-Analytic Procedures for Social Research; SAGE Publications, Inc.: Thousand Oaks, CA, USA, 1991. [Google Scholar] [CrossRef]
- Berlim, M.T.; McGirr, A.; Rodrigues dos Santos, N.; Tremblay, S.; Martins, R. Efficacy of theta burst stimulation (TBS) for major depression: An exploratory meta-analysis of randomized and sham-controlled trials. J. Psychiatr. Res. 2017, 90, 102–109. [Google Scholar] [CrossRef] [PubMed]
- Kallapiran, K.; Koo, S.; Kirubakaran, R.; Hancock, K. Review: Effectiveness of mindfulness in improving mental health symptoms of children and adolescents: A meta-analysis. Child Adolesc. Ment. Health 2015, 20, 182–194. [Google Scholar] [CrossRef] [PubMed]
- McGirr, A.; Berlim, M.T.; Bond, D.J.; Neufeld, N.H.; Chan, P.Y.; Yatham, L.N.; Lam, R.W. A systematic review and meta-analysis of randomized controlled trials of adjunctive ketamine in electroconvulsive therapy: Efficacy and tolerability. J. Psychiatr. Res. 2015, 62, 23–30. [Google Scholar] [CrossRef] [PubMed]
- Rothstein, H.R.; Sutton, A.J.; Borenstein, M. Publication Bias in Meta-Analysis: Prevention, Assessment and Adjustments. 2005. Available online: https://www.wiley.com/en-us/Publication+Bias+in+Meta+Analysis%3A+Prevention%2C+Assessment+and+Adjustments-p-9780470870143 (accessed on 19 October 2022).
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef] [PubMed]
- Gonzalez-Gerez, J.J.; Saavedra-Hernandez, M.; Anarte-Lazo, E.; Bernal-Utrera, C.; Perez-Ale, M.; Rodriguez-Blanco, C. Short-Term Effects of a Respiratory Telerehabilitation Program in Confined COVID-19 Patients in the Acute Phase: A Pilot Study. Int. J. Environ. Res. Public Heal. 2021, 18, 7511. [Google Scholar] [CrossRef] [PubMed]
- Li, J.; Xia, W.; Zhan, C.; Liu, S.; Yin, Z.; Wang, J.; Chong, Y.; Zheng, C.; Fang, X.; Cheng, W.; et al. A telerehabilitation programme in post-discharge COVID-19 patients (TERECO): A randomised controlled trial. Thorax 2021, 77, 697–706. [Google Scholar] [CrossRef]
- Rodriguez-Blanco, C.; Gonzalez-Gerez, J.J.; Bernal-Utrera, C.; Anarte-Lazo, E.; Perez-Ale, M.; Saavedra-Hernandez, M. Short-Term Effects of a Conditioning Telerehabilitation Program in Confined Patients Affected by COVID-19 in the Acute Phase. A Pilot Randomized Controlled Trial. Medicina 2021, 57, 684. [Google Scholar] [CrossRef]
- Bargahi, M.; Rastgoo, N.; Aryanejad, F.; Esmaielzade, S.; Nemati, R.; Ghaebi, M.; Bajelan, A.; Soltani, S. Effect of Balloon-Blowing on Dyspnea and Oxygenation in Hospitalized COVID-19 Patients: A Pilot Study. Acta Med. Iran. 2022, 60. [Google Scholar] [CrossRef]
- Fereydounnia, S.; Shadmehr, A.; Tahmasbi, A.; Salehi, R.S. The Comparison of the Effectiveness of Respiratory Physiotherapy Plus Myofascial Release Therapy Versus Respiratory Physiotherapy Alone on Cardiorespiratory Parameters in Patients With COVID-19. Int. J. Ther. Massage Bodyw. 2022, 15, 4–14. [Google Scholar] [CrossRef]
- Pehlivan, E.; Palali, İ.; Atan, S.G.; Turan, D.; Çinarka, H.; Çetinkaya, E. The effectiveness of POST-DISCHARGE telerehabilitation practices in COVID-19 patients: Tele-COVID study-randomized controlled trial. Ann. Thorac. Med. 2022, 17, 110. [Google Scholar] [CrossRef] [PubMed]
- Al Chikhanie, Y.; Veale, D.; Schoeffler, M.; Pépin, J.L.; Verges, S.; Hérengt, F. Effectiveness of pulmonary rehabilitation in COVID-19 respiratory failure patients post-ICU. Respir. Physiol. Neurobiol. 2021, 287, 103639. [Google Scholar] [CrossRef] [PubMed]
- Hayden, M.C.; Limbach, M.; Schuler, M.; Merkl, S.; Schwarzl, G.; Jakab, K.; Nowak, D.; Schultz, K. Effectiveness of a Three-Week Inpatient Pulmonary Rehabilitation Program for Patients after COVID-19: A Prospective Observational Study. Int. J. Environ. Res. Public Health 2021, 18, 9001. [Google Scholar] [CrossRef] [PubMed]
- Martin, I.; Braem, F.; Baudet, L.; Poncin, W.; Fizaine, S.; Aboubakar, F.; Froidure, A.; Pilette, C.; Liistro, G.; De Greef, J.; et al. Follow-up of functional exercise capacity in patients with COVID-19: It is improved by telerehabilitation. Respir. Med. 2021, 183, 106438. [Google Scholar] [CrossRef] [PubMed]
- Büsching, G.; Zhang, Z.; Schmid, J.-P.; Sigrist, T.; Khatami, R. Effectiveness of Pulmonary Rehabilitation in Severe and Critically Ill COVID-19 Patients: A Controlled Study. Int. J. Environ. Res. Public Health 2021, 18, 8956. [Google Scholar] [CrossRef] [PubMed]
- Abodonya, A.M.; Abdelbasset, W.K.; Awad, E.A.; Elalfy, I.E.; Salem, H.A.; Elsayed, S.H. Inspiratory muscle training for recovered COVID-19 patients after weaning from mechanical ventilation: A pilot control clinical study. Medicine 2021, 100, e25339. [Google Scholar] [CrossRef]
- Hanada, M.; Kasawara, K.T.; Mathur, S.; Rozenberg, D.; Kozu, R.; Hassan, S.A.; Reid, W.D. Aerobic and breathing exercises improve dyspnea, exercise capacity and quality of life in idiopathic pulmonary fibrosis patients: Systematic review and meta-analysis. Thorac. Dis. 2020, 12, 1041–1055. [Google Scholar] [CrossRef]
- Reina-Gutiérrez, S.; Torres-Costoso, A.; Martínez-Vizcaíno, V.; Núñez de Arenas-Arroyo, S.; Fernández-Rodríguez, R.; Pozuelo-Carrascosa, D.P. Effectiveness of Pulmonary Rehabilitation in Interstitial Lung Disease, Including Coronavirus Diseases: A Systematic Review and Meta-analysis. Arch. Phys. Med. Rehabil. 2021, 102, 1989–1997.e3. [Google Scholar] [CrossRef]
- Wang, T.J.; Chau, B.; Lui, M.; Lam, G.T.; Lin, N.; Humbert, S. Physical Medicine and Rehabilitation and Pulmonary Rehabilitation for COVID-19. Am. J. Phys. Med. Rehabil. 2020, 99, 769–774. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author (Year) | Study Design | Population | Sample Size | Intervention | Control Group | Outcomes | Results |
|---|---|---|---|---|---|---|---|
| González-Gerez et al. (2021) [49] | RCT | Adults mild-moderate acute COVID-19 | N = 38 | N = 19 (40.79 y/o, ±9.84; 47.4% F) Breathing exercises once a day, 7 days at home, telematic. | N = 19 (40.32 y/o, ±12.53; 42.1% F) Usual care | Physical function (6MWD/30STS) Dyspnea (MD12/BS) | Patients in intervention group improved dyspnea (MD12 and BS p < 0.001), 30STS (p = 0.001) and 6MWT (p = 0.006) after intervention compared to baseline. Patients in control group did not show statistically differences after intervention in any measured outcome compared to baseline. Between groups comparison, intervention group improved dyspnea (MD12 and BS p < 0.001), 30STS (p = 0.001) and 6MWT (p = 0.007) with differences compared to control. |
| Li et al. (2021) [50] | RCT | Adults with moderate dyspnea associated to COVID-19 | N = 119 (55.46% F) Mean age 50.61 ± 10.98 | N = 59 Breathing exercises Aerobic exercise Strength exercise 3–4 sessions per week, during 6 weeks | N = 60 Educational instructions at baseline | Physical function (6MWD) Dyspnea (mMRC) Quality of life (SF-12) | 6MWD improved in both groups, but intervention group improved with statistically differences (p < 0.001). Quality of life improved in both groups, but intervention group improved with statistically differences in physical component (p = 0.004). Differences in mental component were not statistically significant (p = 0.116). Dyspnea improved in both groups, but intervention group improved with statistically differences (p = 0.001). |
| Rodríguez-Blanco et al. (2021) [51] | RCT | Adults mild-moderate acute COVID-19 | N = 36 | N = 18 (50% F) Age: 39.39 (±11.74) Resistance training once a day, for 7 days | N = 18 (55.5% F) Age: 41.33 (±12.13) Usual care | Physical function (6MWD/30STS) Dyspnea (MBS) | Patients in intervention group improved with statistically differences 6MWT (p = 0.016), 30STS (p = 0.011) and dyspnea (p < 0.001) compared to baseline, while control group improved 30STS (p = 0.026) and not 6MWT (p = 0.993) compared to baseline. Between groups comparison, intervention group improved 6MWT with statistically differences compared to usual care (p = 0.026) as well as 30STS (p = 0.001) and dyspnea (p < 0.001). |
| Bargahi et al. (2021) [52] | RCT | Adults with COVID-19 associated dyspnea and SpO2 < 94%. | N = 80 (38.75% F) | N = 40 Age: 57.1 (±18.7) Respiratory training 5 sets of 5 repetitions each day, for 3 days | N = 40 Age: 58 (±17.13) Usual care | Dyspnea (MBS) | Dyspnea improved after treatment in intervention group compared to control at rest (p = 0.007) and after walking 50 m (p = 0.017) |
| Fereydounnia et al. (2022) [53] | RCT | Adults with acute COVID-19 and oxygen therapy | N = 50 (42% F) | N = 25 Age: 49.44 (±14.78) Myofascial release therapy + Respiratory physical therapy, 3 times per week for 1 week | N = 25 Age: 45 (±12.75) Respiratory physical therapy, 3 times per week for 1 week | Dyspnea (MBS) Physical function (6MWD) | Statistically differences between groups were found in dyspnea perception (p < 0.01). 6MWD improved in control group but not in intervention. |
| Pehlivan et al. (2022) [54] | RCT | Adults with post-acute COVID-19 | N = 34 | N = 17 (18% F) Age: 50.76 (32–82) Education Aerobic Exercise Breathing Exercise Strength Exercise 3 days per week, for 6 weeks | N = 17 (35% F) Age: 43.24 (23–71) Exercises to be performed at home without supervision | Physical function (TUG/SPPB) Dyspnea (mMRC) Quality of life (SGRQ) | Both groups improved outcomes but only with differences intra-group in terms of dyspnea (p = 0.035), TUG (p = 0.005) and SGRQ (p = 0.002) in intervention group. No intra-group differences were found in control group. Between groups, only SGRQ improved with statistically differences in intervention group compared to control (p = 0.042). |
| Chikhaine et al. (2021) [55] | Observational | Adults with COVID-19 compared with Adults non-COVID-19 with respiratory failure | N = 42 (35.71% F) | N = 21 Age: 70.9 ± 10.6 Breathing Exercises Muscle strengthening Aerobic Exercise | N = 21 Age: 69.1 ± 9.4 Breathing Exercises Muscle strengthening Aerobic Exercise | Physical function (6MWD) Quality of life (SGRQ) | Pulmonary rehabilitation showed no differences in 6MWT improvements in COVID-19 patients compared to non-COVID-19 patients with respiratory failure (p < 0.001). Quality of life improved after treatment, but without statistically significant differences. However, both groups still showed impairment in respiratory function and physical performance at discharge. |
| Hayden et al. (2021) [56] | Observational | Adults post-acute to mild COVID-19 | N = 108 (45.4% F) Age: 55.6 (±10.1) | Endurance training (3–5 sessions per week, 30–60 min) Breathing exercise (1 per week, 45 min) Physical Therapy Education (45 min) Psychosocial support Nutritional counseling Occupational therapy | No control | Dyspnea (NRS/mMRC) Physical function (6MWD) Quality of life (EQ-5D-5L) | Moderate to large pre-post changes for intensity in exertional dyspnea. 50% of patients improved with clinically differences (ES: 0.64 ± 0.23). 6MWD improved significantly with large effect size (ES: 1.36 ± 0.27). Quality of life improved significantly with high effect sizes (ES: 0.95 ± 0.26). |
| Martín et al. (2021) [57] | Observational | Adults with severe COVID-19 | N = 48 | N = 14 (21.4% F)Age: 60.8 (±10.4)Telerehabilitation program based on exercise, twice a week, for 6 weeks. 50 min per session. | N = 13 (53.8% F)Age: 61.9 (±10.7)Usual Care | Physical function (1min-STS) | At 3 months of follow-up, there were statistically differences favoring intervention group (p = 0.004) in terms of physical function improvements. |
| Büsching et al. (2021) [58] | Observational | Adults with pneumonia associated to COVID-19 compared to patients with other non-COVID-19 pneumonia | N = 102 | N = 51 (25% F) Age: 65.8 (±11.7) Aerobic exercise Strength exercise Breathing exercise Relaxation techniques Psychological and nutritional counseling | N = 51 (55% F) Age: 69.8 (±9.6) Aerobic exercise Strength exercise Breathing exercise Relaxation techniques Psychological and nutritional counseling | Physical function (6MWD) | After intervention, both groups improved in 6MWD compared with baseline. Additionally, patients with pneumonia associated with COVID-19 improved more in 6MWD than patients with other causes pneumonia (p = 0.026). |
| Abodonya et al. (2021) [59] | Observational | Adults with post-acute COVID-19 compared to age-matched controls without COVID-19 | N = 42 | N = 21 (19% F) Age: 48.3 (±8.5) Breathing exercises Inspiratory muscle trainer, 2 sessions/day, 5 days/week, for 2 weeks. | N = 21 (23.8% F) Age: 47.8 (±9.2) Breathing exercises 2 times daily for 2 weeks | Dyspnea (DSI) Quality of life (EQ-5D-3L) Physical function (6MWD) | Intra-group analysis found statistically differences in intervention group in dyspnea (p = 0.039), quality of life (p < 0.001) and 6MWD (p < 0.001). However, there were improvements in control group, but without statistically differences. Between groups comparison found statistically differences favoring intervention group in dyspnea (p = 0.032), quality of life (p = 0.021) and 6MWD (p = 0.028) when compared to control. |
| Author (Year) | Random Sequence Generation | Deviations from the Intended Interventions | Missing Outcome Data | Measurement of Outcomes | Selection of the Reported Results | Overall Risk of Bias |
|---|---|---|---|---|---|---|
| Gonzalez-Gerez et al. (2021) [49] | Low risk | Low risk | Low risk | Low risk | Low risk | Low risk |
| Li et al. (2021) [50] | Low risk | Low risk | Low risk | Low risk | Low risk | Low risk |
| Rodriguez-Blanco et al. (2021) [51] | Low risk | Low risk | Low risk | Low risk | Low risk | Low risk |
| Bargahi et al. (2021) [52] | Some concerns | Some concerns | Low risk | Low risk | Low risk | Some concerns |
| Fereydounnia et al. (202) [53] | Low risk | Some concerns | Some concerns | Low risk | Low risk | Some concerns |
| Pehvlian et al. (2022) [54] | Low risk | Some concerns | Some concerns | Some concerns | Low risk | Some concerns |
| Study Name | Selection | Comparability | Exposure/Outcome | Total | |||||
|---|---|---|---|---|---|---|---|---|---|
| 1 | 2 | 3 | 4 | 1 | 1 | 2 | 3 | ||
| Chikhaine et al., 2021 [55] | Y | Y | N | Y | Y N | N | Y | Y | 6 |
| Hayden et al., 2021 [56] | Y | Y | N | N | N N | N | Y | Y | 4 |
| Martín et al., 2021 [57] | Y | Y | N | N | Y N | Y | Y | Y | 6 |
| Büsching et al., 2021 [58] | Y | Y | N | Y | Y Y | Y | N | Y | 7 |
| Abodonya et al., 2021 [59] | Y | Y | Y | Y | Y Y | Y | N | Y | 8 |
| Quality assessment of pulmonary rehabilitation improving dyspnea of post-acute COVID-19 patients | |||||||
| Number of studies (Subjects) | Risk of bias | Inconsistency | Indirectness | Imprecision | Publication Bias | Quality | Grade of recomendation |
| N = 7 (471) | Serious * | Serious ‡ | Not serious | Serious ≠ | Serious + | Very low quality | Weak in favor |
| Quality assessment of pulmonary rehabilitation improving physical function of post-acute COVID-19 patients | |||||||
| Number of studies (Subjects) | Risk of bias | Inconsistency | Indirectness | Imprecision | Publication Bias | Quality | Grade of recommendation |
| N = 10 (598) | Serious * | Serious ‡ | Not serious | Serious ≠ | Serious + | Very low quality | Weak in favor |
| Quality assessment of pulmonary rehabilitation improving quality of life of post-acute COVID-19 patients | |||||||
| Number of studies (Subjects) | Risk of bias | Inconsistency | Indirectness | Imprecision | Publication Bias | Quality | Grade of recommendation |
| N = 4 (303) | Serious * | Serious ‡ | Not serious | Serious ≠ | Serious + | Very Low quality | Weak in favor |
| Outcome and Study | Begg Test | Eggers Test |
|---|---|---|
| Dyspnea RCT | Kendall’s τ = −0.867, p = 0.017 | t(4) = −5.193, p = 0.007 |
| Physical function RCT | Kendall’s τ = 0.643, p = 0.031 | t(6) = 5.976, p = 0.001 |
| Quality of life RCT | Kendall’s τ = −0.333, p > 0.999 | t(1) = −0.877, p = 0.542 |
| Dyspnea OBS | Kendall’s τ = −0.4, p = 0.483 | t(3) = −2.45, 0.092 |
| Physical function OBS | Kendall’s τ = 0.4, p = 0.483 | t(3) = 6.971, p = 0.006 |
| Quality of life OBS | Kendall’s τ = 0, p > 0.999 | t(2) = 0.824, p = 0.496 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Reinert, G.; Müller, D.; Wagner, P.; Martínez-Pozas, O.; Cuenca-Záldivar, J.N.; Fernández-Carnero, J.; Sánchez Romero, E.A.; Corbellini, C. Pulmonary Rehabilitation in SARS-CoV-2: A Systematic Review and Meta-Analysis of Post-Acute Patients. Diagnostics 2022, 12, 3032. https://doi.org/10.3390/diagnostics12123032
Reinert G, Müller D, Wagner P, Martínez-Pozas O, Cuenca-Záldivar JN, Fernández-Carnero J, Sánchez Romero EA, Corbellini C. Pulmonary Rehabilitation in SARS-CoV-2: A Systematic Review and Meta-Analysis of Post-Acute Patients. Diagnostics. 2022; 12(12):3032. https://doi.org/10.3390/diagnostics12123032
Chicago/Turabian StyleReinert, Glenn, Daniel Müller, Pit Wagner, Oliver Martínez-Pozas, Juan Nicolás Cuenca-Záldivar, Josué Fernández-Carnero, Eleuterio A. Sánchez Romero, and Camilo Corbellini. 2022. "Pulmonary Rehabilitation in SARS-CoV-2: A Systematic Review and Meta-Analysis of Post-Acute Patients" Diagnostics 12, no. 12: 3032. https://doi.org/10.3390/diagnostics12123032