
Temporomandibular Disorders, Bruxism, Perceived Stress, and Coping Strategies among Medical University Students in Times of Social Isolation during Outbreak of COVID-19 Pandemic

 , , ,
, , , 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
Abbreviations
| TMD | temporomandibular disorders |
| AB | awake bruxism |
| SB | sleep bruxism |
| TMJ | temporomandibular joint |
| PSS-10 | Perceived Stress Scale |
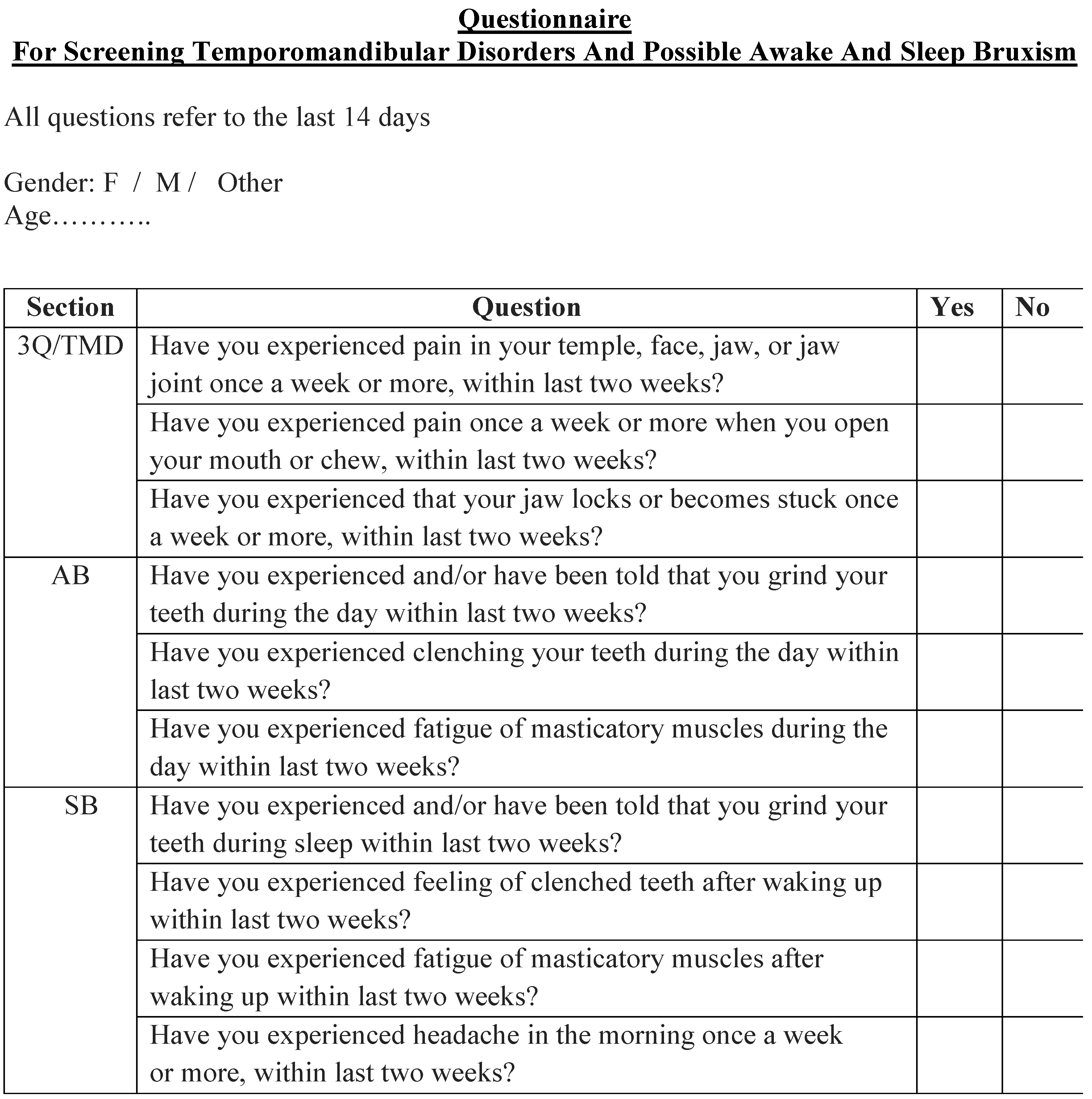
Appendix A

Appendix B

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Strategy | Planning | Active Coping | Self-Blaming | Seeking Instrumental Support | Seeking Emotional Support | Acceptance |
|---|---|---|---|---|---|---|
| Planning | ||||||
| Active coping | chi2 = 0.674; p = 0.4110 | |||||
| Self-Blaming | chi2 = 0.934; p = 0.3340 | chi2 = 0.106; p = 0.7750 | ||||
| Seeking instrumental Support | chi2 = 8.980; p = 0.0027 | chi2 = 2.916; p = 0.0880 | chi2 = 19.758; p = 0.000 | |||
| Seeking Emotional Support | chi2 = 12.025; p = 0.0005 | chi2 = 4.752; p = 0.0293 | chi2 = 6.277; p = 0.0122 | chi2 = 0.223; p = 0.6370 | ||
| Acceptance | chi2 = 29.154; p = 0.0000 | chi2 = 16.991; p = 0.0000 | chi2 = 19.758; p = 0.0000 | chi2 = 5.871; p = 0.0154 | chi2 = 3.812; p = 0.0510 |
| Strategy | Planning | Active Coping | Self-Blaming | Seeking Instrumental Support | Seeking Emotional Support | Acceptance |
|---|---|---|---|---|---|---|
| Planning | ||||||
| Active coping | chi2 = 0.005; p = 0.9430 | |||||
| Self-Blaming | chi2 = 0.000; p = 1.0000 | chi2 = 0.005; p = 0.9430 | ||||
| Seeking instrumental Support | chi2 = 4.389; p = 0.0362 | chi2 = 4.679; p = 0.0305 | chi2 = 4.389; p = 0.0362 | |||
| Seeking Emotional Support | chi2 = 5.447; p = 0.0196 | chi2 = 5.770; p = 0.0163 | chi2 = 5.447; p = 0.0196 | chi2 = 0.570; p = 0.4500 | ||
| Acceptance | chi2 = 16.385; p = 0.0000 | chi2 = 16.934; p = 0.0000 | 16.385; p = 0.0000 | chi2 = 3.874; p = 0.0490 | chi2 = 2.997; p = 0.0830 |
| Strategy | Planning | Active Coping | Self-Blaming | Seeking Instrumental Support | Seeking Emotional Support | Acceptance |
|---|---|---|---|---|---|---|
| Planning | ||||||
| Active coping | chi2 = 0.544; p = 0.4610 | |||||
| Self-Blaming | chi2 = 0.305; p = 0.5810 | chi2 = 0.034; p = 0.8540 | ||||
| Seeking instrumental Support | chi2 = 7.556; p = 0.0060 | chi2 = 4.057; p = 0.0440 | chi2 = 4.836; p = 0.0279 | |||
| Seeking Emotional Support | chi2 = 5.357; p = 0.0206 | chi2 = 2.492; p = 0.1140 | chi2 = 3.111; p = 0.0780 | chi2 = 0.668; p = 0.4140 | ||
| Acceptance | chi2 = 24.828; p = 0.0000 | chi2 = 18.113; p = 0.0000 | chi2 = 19.705; p = 0.0000 | chi2 = 3.873; p = 0.0490 | chi2 = 2.997; p = 0.0830 |
References
- Marsicano, C.R.; Barnshaw, J.; Letukas, L. Crisis and change: How COVID-19 exacerbated institutional inequality and how institutions are responding. New Dir. Inst. Res. 2020, 2020, 7. [Google Scholar] [CrossRef]
- Patelarou, A.; Mechili, E.A.; Galanis, P.; Zografakis-Sfakianakis, M.; Konstantinidis, T.; Saliaj, A.; Bucaj, J.; Alushi, E.; Carmona-Torres, J.M.; Cobo-Cuenca, A.I.; et al. Nursing students, mental health status during COVID-19 quarantine: Evidence from three European countries. J. Ment. Health 2021, 30, 164–169. [Google Scholar] [CrossRef] [PubMed]
- Limón-Vázquez, A.K.; Guillén-Ruiz, G.; Herrera-Huerta, E.V. The Social Isolation Triggered by COVID-19: Effects on Mental Health and Education in Mexico. In Health and Academic Achievement-New Findings; IntechOpen: London, UK, 2021; ISBN 978-1-83881-090-0. [Google Scholar]
- Behrens, F.; Kret, M.E. The Interplay Between Face-to-Face Contact and Feedback on Cooperation During Real-Life Interactions. J. Nonverbal Behav. 2019, 43, 513–528. [Google Scholar] [CrossRef] [Green Version]
- Soffer, T.; Nachmias, R. Effectiveness of learning in online academic courses compared with face-to-face courses in higher education. J. Comput. Assist. Learn. 2018, 34, 534–543. [Google Scholar] [CrossRef]
- List, T.; Jensen, R.H. Temporomandibular disorders: Old ideas and new concepts. Cephalalgia 2017, 37, 692–704. [Google Scholar] [CrossRef] [PubMed]
- Gauer, R.L.; Semidey, M.J. Diagnosis and treatment of temporomandibular disorders. Am. Fam. Physician 2015, 91, 378–386. [Google Scholar]
- Ohayon, M.M.; Li, K.K.; Guilleminault, C. Risk Factors for Sleep Bruxism in the General Population. Chest 2001, 119, 53–61. [Google Scholar] [CrossRef] [Green Version]
- Manfredini, D.; Winocur, E.; Guarda-Nardini, L.; Paesani, D.; Lobbezoo, F. Epidemiology of bruxism in adults: A systematic review of the literature. J. Orofac. Pain 2013, 27, 99–110. [Google Scholar] [CrossRef] [Green Version]
- Thorpy, M. International classification of sleep disorders. In Sleep Disorders Medicine: Basic Science, Technical Considerations and Clinical Aspects: Fourth Edition; Springer: Darien, IL, USA, 2017; pp. 475–484. ISBN 9781493965786. [Google Scholar]
- Lobbezoo, F.; Ahlberg, J.; Raphael, K.G.; Wetselaar, P.; Glaros, A.G.; Kato, T.; Santiago, V.; Winocur, E.; De Laat, A.; De Leeuw, R.; et al. International consensus on the assessment of bruxism: Report of a work in progress. J. Oral Rehabil. 2018, 45, 837–844. [Google Scholar] [CrossRef]
- Huynh, N.; Kato, T.; Rompré, P.H.; Okura, K.; Saber, M.; Lanfranchi, P.A.; Montplaisir, J.Y.; Lavigne, G.J. Sleep bruxism is associated to micro-arousals and an increase in cardiac sympathetic activity. J. Sleep Res. 2006, 15, 339–346. [Google Scholar] [CrossRef]
- Nukazawa, S.; Yoshimi, H.; Sato, S. Autonomic nervous activities associated with bruxism events during sleep. CRANIO-J. Craniomandib. Pract. 2018, 36, 106–112. [Google Scholar] [CrossRef] [PubMed]
- Han, K.; Wang, C.; Zhong, Z.; Xu, M.; Zou, X.; Yu, B.; Wang, K.; Yao, D. Characterisation of the relationships between rhythmic masticatory muscle activities and limb movements in patients with sleep bruxism. J. Oral Rehabil. 2018, 46, 399–408. [Google Scholar] [CrossRef] [PubMed]
- Manfredini, D.; Visscher, C.M.; Guarda-Nardini, L.; Lobbezoo, F. Occlusal factors are not related to self-reported bruxism. J. Orofac. Pain 2012, 26, 163–167. [Google Scholar] [PubMed]
- Wieckiewicz, M.; Paradowska-Stolarz, A.; Wieckiewicz, W. Psychosocial Aspects of Bruxism: The Most Paramount Factor Influencing Teeth Grinding. BioMed Res. Int. 2014, 2014, 469187. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rintakoski, K.; Ahlberg, J.; Hublin, C.; Broms, U.; Madden, P.A.F.; Könönen, M.; Koskenvuo, M.; Lobbezoo, F.; Kaprio, J. Bruxism Is Associated with Nicotine Dependence: A Nationwide Finnish Twin Cohort Study. Nicotine Tob. Res. 2010, 12, 1254–1260. [Google Scholar] [CrossRef] [PubMed]
- Bertazzo-Silveira, E.; Kruger, C.M.; De Toledo, I.P.; Porporatti, A.; Dick, B.; Flores-Mir, C.; Canto, G.D.L. Association between sleep bruxism and alcohol, caffeine, tobacco, and drug abuse: A systematic review. J. Am. Dent. Assoc. 2016, 147, 859–866.e4. [Google Scholar] [CrossRef]
- Hamza, C.A.; Ewing, L.; Heath, N.L.; Goldstein, A.L. When social isolation is nothing new: A longitudinal study psychological distress during COVID-19 among university students with and without preexisting mental health concerns. Can. Psychol. 2020, undefined. [Google Scholar] [CrossRef]
- Cacioppo, J.T.; Cacioppo, S. Social Relationships and Health: The Toxic Effects of Perceived Social Isolation. Soc. Pers. Personal. Compass 2014, 8, 58–72. [Google Scholar] [CrossRef]
- Stanisławski, K. The Coping Circumplex Model: An Integrative Model of the Structure of Coping with Stress. Front. Psychol. 2019, 10, 694. [Google Scholar] [CrossRef]
- Endler, N.S.; Parker, J.D.A. Multidimensional assessment of coping: A critical evaluation. J. Pers. Soc. Psychol. 1990, 58, 844–854. [Google Scholar] [CrossRef]
- Lembas, D.; Starkowska, A.; Mak, M.; Konecka, M.; Bikowska, M.; Groszewska, K.; Korzonek, M. Impact of demographic factors on usage of stress coping strategies chosen by elderly people. Fam. Med. Prim. Care Rev. 2017, 1, 34–38. [Google Scholar] [CrossRef]
- Saczuk, K.; Lapinska, B.; Wilmont, P.; Pawlak, L.; Lukomska-Szymanska, M. Relationship between Sleep Bruxism, Perceived Stress, and Coping Strategies. Int. J. Environ. Res. Public Health 2019, 16, 3193. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Klein, E.M.; Brähler, E.; Dreier, M.; Reinecke, L.; Müller, K.W.; Schmutzer, G.; Wölfling, K.; Beutel, M.E. The German version of the Perceived Stress Scale–psychometric characteristics in a representative German community sample. BMC Psychiatry 2016, 16, 1–10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lesage, F.-X.; Berjot, S.; Deschamps, F. Psychometric properties of the French versions of the Perceived Stress Scale. Int. J. Occup. Med. Environ. Health 2012, 25, 178–184. [Google Scholar] [CrossRef]
- Zinurova, E.; Dehart, R. Perceived Stress, Stressors, and Coping Mechanisms Among PGY1 Pharmacy Residents. Am. J. Pharm. Educ. 2018, 82, 6574. [Google Scholar] [CrossRef]
- Mocny-Pachońska, K.; Trzcionka, A.; Doniec, R.; Sieciński, S.; Tanasiewicz, M. The Influence of Gender and Year of Study on Stress Levels and Coping Strategies among Polish Dental. Medicina 2020, 56, 531. [Google Scholar] [CrossRef]
- Jordan, R.K.; Shah, S.S.; Desai, H.; Tripi, J.; Mitchell, A.; Worth, R.G. Variation of stress levels, burnout, and resilience throughout the academic year in first-year medical students. PLoS ONE 2020, 15, e0240667. [Google Scholar] [CrossRef]
- Worku, D.; Dirriba, A.B.; Wordofa, B.; Fetensa, G. Perceived Stress, Depression, and Associated Factors among Undergraduate Health Science Students at Arsi University in 2019 in Oromia, Ethiopia. Psychiatry J. 2020, 2020, 4956234. [Google Scholar] [CrossRef]
- Cavallo, P.; Carpinelli, L.; Savarese, G. Perceived stress and bruxism in university students. BMC Res. Notes 2016, 9, 514. [Google Scholar] [CrossRef] [Green Version]
- Ribeiro, I.J.; Pereira, R.; Freire, I.V.; de Oliveira, B.G.; Casotti, C.A.; Boery, E.N. Stress and Quality of Life Among University Students: A Systematic Literature Review. Health Prof. Educ. 2018, 4, 70–77. [Google Scholar] [CrossRef]
- Lövgren, A.; Marklund, S.; Visscher, C.M.; Lobbezoo, F.; Häggman-Henrikson, B.; Wänman, A. Outcome of three screening questions for temporomandibular disorders (3Q/TMD) on clinical decision-making. J. Oral Rehabil. 2017, 44, 573–579. [Google Scholar] [CrossRef] [PubMed]
- Lövgren, A.; Parvaneh, H.; Lobbezoo, F.; Häggman-Henrikson, B.; Wänman, A.; Visscher, C.M. Diagnostic accuracy of three screening questions (3Q/TMD) in relation to the DC/TMD in a specialized orofacial pain clinic. Acta Odontol. Scand. 2018, 76, 380–386. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Emodi-Perlman, A.; Eli, I.; Smardz, J.; Uziel, N.; Wieckiewicz, G.; Gilon, E.; Grychowska, N.; Wieckiewicz, M. Temporomandibular Disorders and Bruxism Outbreak as a Possible Factor of Orofacial Pain Worsening during the COVID-19 Pandemic—Concomitant Research in Two Countries. J. Clin. Med. 2020, 9, 3250. [Google Scholar] [CrossRef] [PubMed]
- Van Selms, M.K.A.; Visscher, C.M.; Naeije, M.; Lobbezoo, F. Bruxism and associated factors among Dutch adolescents. Community Dent. Oral Epidemiol. 2013, 41, 353–363. [Google Scholar] [CrossRef] [PubMed]
- Cohen, S.; Kamarck, T.; Mermelstein, R. A global measure of perceived stress. J. Health Soc. Behav. 1983, 24, 385–396. [Google Scholar] [CrossRef]
- Jurczyński, Z.; Ogińska-Bulik, N. PSS-10. In Narzędzia Pomiaru Stresu i Radzenia Sobie ze Stresem; Pracownia Testów Psychologicznych Polskiego Towarzystwa Psychologicznego: Warszawa, Poland, 2009; pp. 45–58. [Google Scholar]
- Carver, C.S. You want to measure coping but your protocol’s too long: Consider the Brief COPE. Int. J. Behav. Med. 1997, 4, 92–100. [Google Scholar] [CrossRef]
- Gunnell, D.; Appleby, L.; Arensman, E.; Hawton, K.; John, A.; Kapur, N.; Khan, M.; O’Connor, R.C.; Pirkis, J.; Caine, E.D. Suicide risk and prevention during the COVID-19 pandemic. Lancet Psychiatry 2020, 7, 468–471. [Google Scholar] [CrossRef]
- Luttik, M.L.A.; Mahrer-Imhof, R.; García-Vivar, C.; Brødsgaard, A.; Dieperink, K.B.; Imhof, L.; Østergaard, B.; Svavarsdottir, E.K.; Konradsen, H. The COVID-19 Pandemic: A Family Affair. J. Fam. Nurs. 2020, 26, 87–89. [Google Scholar] [CrossRef]
- El-Zoghby, S.M.; Soltan, E.M.; Salama, H.M. Impact of the COVID-19 Pandemic on Mental Health and Social Support among Adult Egyptians. J. Community Health 2020, 45, 689–695. [Google Scholar] [CrossRef]
- Kujawa, A.; Green, H.; Compas, B.E.; Dickey, L.; Pegg, S. Exposure to COVID-19 pandemic stress: Associations with depression and anxiety in emerging adults in the United States. Depress. Anxiety 2020, 37, 1280–1288. [Google Scholar] [CrossRef]
- Usher, K.; Bhullar, N.; Jackson, D. Life in the pandemic: Social isolation and mental health. J. Clin. Nurs. 2020, 29, 2756–2757. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gębska, M.; Dalewski, B.; Pałka, Ł.; Kołodziej, Ł.; Sobolewska, E. The Importance of Type D Personality in the Development of Temporomandibular Disorders (TMDs) and Depression in Students during the COVID-19 Pandemic. Brain Sci. 2022, 12, 28. [Google Scholar] [CrossRef] [PubMed]
- Gębska, M.; Dalewski, B.; Pałka, Ł.; Kołodziej, Ł.; Sobolewska, E. Type D Personality and Stomatognathic System Disorders in Physiotherapy Students during the COVID-19 Pandemic. J. Clin. Med. 2021, 10, 4892. [Google Scholar] [CrossRef] [PubMed]
- Di Giacomo, P.; Serritella, E.; Imondi, F.; Di Paolo, C. Psychological impact of COVID-19 pandemic on TMD subjects. Eur. Rev. Med Pharmacol. Sci. 2021, 25, 4616–4626. [Google Scholar] [CrossRef] [PubMed]
- Wieckiewicz, M.; Grychowska, N.; Wojciechowski, K.; Pelc, A.; Augustyniak, M.; Sleboda, A.; Ziętek, M. Prevalence and Correlation between TMD Based on RDC/TMD Diagnoses, Oral Parafunctions and Psychoemotional Stress in Polish University Students. BioMed Res. Int. 2014, 2014, 472346. [Google Scholar] [CrossRef]
- Gerasimova, L.P.; Kabirova, M.F.; Kuznetzova, N.S.; Farhutdinova, L.V.; Khaibullina, R.R. Vzaimosviaz’ funktsional’nogo sostoianiia zubocheliustnoĭ sistemy i psikhoémotsional’nogo napriazheniia u lits molodogo vozrasta. Stomatologiia (Mosk). 2017, 96, 34–36. [Google Scholar] [CrossRef]
- Ahuja, V.; Ranjan, V.; Passi, D.; Jaiswal, R. Study of stress-induced temporomandibular disorders among dental students: An institutional study. Natl. J. Maxillofac. Surg. 2018, 9, 147–154. [Google Scholar] [CrossRef]
- Kim, J.E.; Lee, S.T.; Kim, Y.E.; Bae, S.H.; Shin, H.J.; Jo, J.E.; Kim, S.H. Influence of stress on the oral health and quality of life of university students. J. Korean Soc. Dent. Hyg. 2018, 18, 797–806. [Google Scholar] [CrossRef]
- Karayanni, H.; Dror, A.A.; Oren, D.; Sela, E.; Granot, I.; Srouji, S. Exacerbation of chronic myofascial pain during COVID-19. Adv. Oral Maxillofac. Surg. 2021, 1, 100019. [Google Scholar] [CrossRef]
- Saccomanno, S.; Bernabei, M.; Scoppa, F.; Pirino, A.; Mastrapasqua, R.; Visco, M.A. Coronavirus Lockdown as a Major Life Stressor: Does It Affect TMD Symptoms? Int. J. Environ. Res. Public Health 2020, 17, 8907. [Google Scholar] [CrossRef]
- Lee, E.-H. Review of the Psychometric Evidence of the Perceived Stress Scale. Asian Nurs. Res. (Korean. Soc. Nurs. Sci.) 2012, 6, 121–127. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Quek, T.T.-C.; Tam, W.W.-S.; Tran, B.X.; Zhang, M.; Zhang, Z.; Ho, C.S.H.; Ho, R.C.M. The Global Prevalence of Anxiety Among Medical Students: A Meta-Analysis. Int. J. Environ. Res. Public Health 2019, 16, 2735. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Elani, H.W.; Allison, P.J.; Kumar, R.A.; Mancini, L.; Lambrou, A.; Bedos, C. A Systematic Review of Stress in Dental Students. J. Dent. Educ. 2014, 78, 226–242. [Google Scholar] [CrossRef] [PubMed]
- Kupcewicz, E.; Grochans, E.; Kadučáková, H.; Mikla, M.; Jóźwik, M. Analysis of the Relationship between Stress Intensity and Coping Strategy and the Quality of Life of Nursing Students in Poland, Spain and Slovakia. Int. J. Environ. Res. Public Health 2020, 17, 4536. [Google Scholar] [CrossRef]
- Machul, M.; Bieniak, M.; Chałdaś-Majdańska, J.; Bąk, J.; Chrzan-Rodak, A.; Mazurek, P.; Pawłowski, P.; Makuch-Kuśmierz, D.; Obuchowska, A.; Bartoszek, A.; et al. Lifestyle Practices, Satisfaction with Life and the Level of Perceived Stress of Polish and Foreign Medical Students Studying in Poland. Int. J. Environ. Res. Public Health 2020, 17, 4445. [Google Scholar] [CrossRef]
- Bodys-Cupak, I.; Majda, A.; Kurowska, A.; Ziarko, E.; Zalewska-Puchała, J. Psycho-social components determining the strategies of coping with stress in undergraduate Polish nursing students. BMC Nurs. 2021, 20, 129. [Google Scholar] [CrossRef]
- Awoke, M.; Mamo, G.; Abdu, S.; Terefe, B. Perceived Stress and Coping Strategies Among Undergraduate Health Science Students of Jimma University Amid the COVID-19 Outbreak: Online Cross-Sectional Survey. Front. Psychol. 2021, 12, 639955. [Google Scholar] [CrossRef]
- Ahlberg, J.; Savolainen, A.; Rantala, M.; Lindholm, H.; Könönen, M. Reported bruxism and biopsychosocial symptoms: A longitudinal study. Community Dent. Oral Epidemiol. 2004, 32, 307–311. [Google Scholar] [CrossRef]
- Clark, G.T.; Rugh, J.D.; Handelman, S.L. Nocturnal Masseter Muscle Activity and Urinary Catecholamine Levels in Bruxers. J. Dent. Res. 1980, 59, 1571–1576. [Google Scholar] [CrossRef]
- Vanderas, A.P.; Menenakou, M.; Kouimtzis, T.H.; Papagiannoulis, L. Urinary catecholamine levels and bruxism in children. J. Oral Rehabil. 1999, 26, 103–110. [Google Scholar] [CrossRef]
- Ahlberg, J.; Lobbezoo, F.; Ahlberg, K.; Manfredini, D.; Hublin, C.; Sinisalo, J.; Könönen, M.; Savolainen, A. Self-reported bruxism mirrors anxiety and stress in adults. Med. Oral Patol. Oral Cir. Bucal 2013, 18, e7–e11. [Google Scholar] [CrossRef] [PubMed]
- Pierce, C.J.; Chrisman, K.; Bennett, M.E.; Close, J.M. Stress, anticipatory stress, and psychologic measures related to sleep bruxism. J. Orofac. Pain 1995, 9, 51–56. [Google Scholar] [PubMed]
- Watanabe, T.; Ichikawa, K.; Clark, G.T. Bruxism levels and daily behaviors: 3 weeks of measurement and correlation. J. Orofac. Pain 2003, 17, 65–73. [Google Scholar] [PubMed]
- Da Silva, A.M.; Oakley, D.A.; Hemmings, K.W.; Newman, H.N.; Watkins, S. Psychosocial factors and tooth wear with a significant component of attrition. Eur. J. Prosthodont. Restor. Dent. 1997, 5, 51–55. [Google Scholar]
- Tsai, C.-M.; Chou, S.-L.; Gale, E.N.; McCall, W.D. Human masticatory muscle activity and jaw position under experimental stress. J. Oral Rehabil. 2002, 29, 44–51. [Google Scholar] [CrossRef]
- Ebner, K.; Singewald, N. Individual differences in stress susceptibility and stress inhibitory mechanisms. Curr. Opin. Behav. Sci. 2017, 14, 54–64. [Google Scholar] [CrossRef]
- Kato, T. Frequently Used Coping Scales: A Meta-Analysis. Stress Health 2015, 31, 315–323. [Google Scholar] [CrossRef]
- Reissmann, D.R.; John, M.T.; Schierz, O.; Seedorf, H.; Doering, S. Stress-related adaptive versus maladaptive coping and temporomandibular disorder pain. J. Orofac. Pain 2012, 26, 181–190. [Google Scholar]
- Taylor, S.E.; Stanton, A.L. Coping Resources, Coping Processes, and Mental Health. Annu. Rev. Clin. Psychol. 2007, 3, 377–401. [Google Scholar] [CrossRef] [Green Version]
- Nurunnabi, M.; Hossain, S.F.A.H.; Chinna, K.; Sundarasen, S.; Khoshaim, H.B.; Kamaludin, K.; Baloch, G.M.; Sukayt, A.; Shan, X. Coping strategies of students for anxiety during the COVID-19 pandemic in China: A cross-sectional study. F1000Research 2020, 9, 1115. [Google Scholar] [CrossRef]
- Baloran, E.T. Knowledge, Attitudes, Anxiety, and Coping Strategies of Students during COVID-19 Pandemic. J. Loss Trauma 2020, 25, 635–642. [Google Scholar] [CrossRef]
- Babicka-Wirkus, A.; Wirkus, L.; Stasiak, K.; Kozłowski, P. University students’ strategies of coping with stress during the coronavirus pandemic: Data from Poland. PLoS ONE 2021, 16, e0255041. [Google Scholar] [CrossRef] [PubMed]
- Manfredini, D.; Arreghini, A.; Lombardo, L.; Visentin, A.; Cerea, S.; Castroflorio, T.; Siciliani, G. Assessment of Anxiety and Coping Features in Bruxers: A Portable Electromyographic and Electrocardiographic Study. J. Oral Facial Pain Headache 2016, 30, 249–254. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schneider, C.; Schaefer, R.; Ommerborn, M.A.; Giraki, M.; Goertz, A.; Raab, W.H.-M.; Franz, M. Maladaptive coping strategies in patients with bruxism compared to non-bruxing controls. Int. J. Behav. Med. 2007, 14, 257–261. [Google Scholar] [CrossRef]
- Giraki, M.; Schneider, C.; Schäfer, R.; Singh, P.; Franz, M.; Raab, W.H.; Ommerborn, M.A. Correlation between stress, stress-coping and current sleep bruxism. Head Face Med. 2010, 6, 2. [Google Scholar] [CrossRef] [Green Version]
- Zadworna, M.; Michalska, P.; Kobylarczyk, M. Stress and Coping Strategies Among Participants of Stress Management Interventions at the Science, Technology and Art Festival. Przegląd Badań Eduk. 2020, 1, 129–156. [Google Scholar] [CrossRef]
- Soto-Goñi, X.A.; Alen, F.; Buiza-González, L.; Marcolino-Cruz, D.; Sánchez-Sánchez, T.; Ardizone-García, I.; Aneiros-López, F.; Jiménez-Ortega, L. Adaptive Stress Coping in Awake Bruxism. Front. Neurol. 2020, 11, 564431. [Google Scholar] [CrossRef]
- Soto-Goñi, X.; Viñals, A.C.; Pérez-González, F.; Sánchez-Labrador, L.; Domínguez-Gordillo, A.; Sánchez-Sánchez, T.; Ardizone-García, I. Stress-related coping styles, anxiety, and neuroticism in university students with myalgia temporomandibular: A case control study. Rev. Psicol. Salud 2021, 8, 36–49. [Google Scholar] [CrossRef]
- Rasskazova, E.; Leontiev, D.A.; Lebedeva, A.A. Pandemic as a Challenge to Subjective Well-Being: Anxiety and Coping. Couns. Psychol. Psychother. 2020, 28, 90–108. [Google Scholar] [CrossRef]
- Asmundson, G.J.G.; Paluszek, M.M.; Landry, C.A.; Rachor, G.S.; McKay, D.; Taylor, S. Do pre-existing anxiety-related and mood disorders differentially impact COVID-19 stress responses and coping? J. Anxiety Disord. 2020, 74, 102271. [Google Scholar] [CrossRef]
- Santana-Mora, U.; López-Cedrún, J.; Suárez-Quintanilla, J.; Varela-Centelles, P.; Mora, M.J.; Da Silva, J.L.; Figueiredo-Costa, F.; Santana-Penín, U. Asymmetry of dental or joint anatomy or impaired chewing function contribute to chronic temporomandibular joint disorders. Ann. Anat.-Anat. Anz. 2021, 238, 151793. [Google Scholar] [CrossRef] [PubMed]
- Reinhardt, R.; Tremel, T.; Wehrbein, H.; Reinhardt, W. The Unilateral Chewing Phenomenon, Occlusion, and TMD. CRANIO® 2006, 24, 166–170. [Google Scholar] [CrossRef] [PubMed]
- Yalçınkaya, E.; Cingi, C.; Muluk, N.B.; Ulusoy, S.; Hanci, D. Are temporomandibular disorders associated with habitual sleeping body posture or nasal septal deviation? Eur. Arch. Oto-Rhino-Laryngol. 2015, 273, 177–181. [Google Scholar] [CrossRef] [PubMed]
- Hibi, H.; Ueda, M. Body posture during sleep and disc displacement in the temporomandibular joint: A pilot study. J. Oral Rehabil. 2005, 32, 85–89. [Google Scholar] [CrossRef]
- Pinelli, C.; Loffredo, L.D.C.M. Reproducibility and validity of self-perceived oral health conditions. Clin. Oral Investig. 2007, 11, 431–437. [Google Scholar] [CrossRef]




| TMD Symptoms | Gender | Total | ||||||
| Female | Male | Other | ||||||
| n | % | n | % | n | % | n | % | |
| Yes | 641 | 81.1 | 138 | 63.0 | 8 | 88.9 | 787 | 77.3 |
| No | 149 | 18.9 | 81 | 37.0 | 1 | 11.1 | 231 | 22.7 |
| Sum | 790 | 100.0 | 219 | 100.0 | 9 | 100.0 | 1018 | 100.0 |
| Comparison | chi2 = 32.806; p < 0.001 | |||||||
| Possible AB | Gender | Total | ||||||
| Female | Male | Other | ||||||
| n | % | n | % | n | % | n | % | |
| Yes | 401 | 50.8 | 79 | 36.1 | 7 | 77.8 | 487 | 47.8 |
| No | 389 | 49.2 | 140 | 63.9 | 2 | 22.2 | 531 | 52.2 |
| Sum | 790 | 100.0 | 219 | 100.0 | 9 | 100.0 | 1018 | 100.0 |
| Comparison | chi2 = 18.083; p < 0.001 | |||||||
| Gender | Total | |||||||
| Possible SB | Female | Male | Other | |||||
| n | % | n | % | n | % | n | % | |
| Yes | 482 | 61.0 | 113 | 51.6 | 5 | 55.6 | 600 | 58.9 |
| No | 308 | 39.0 | 106 | 48.4 | 4 | 44.4 | 418 | 41.1 |
| Sum | 790 | 100.0 | 219 | 100.0 | 9 | 100.0 | 1018 | 100.0 |
| Comparison | chi2 = 6.323; p < 0.05 | |||||||
| PSS-10 Score Range | TMD Symptoms | ||||
| Yes | No | Total | |||
| n | % | n | % | n | |
| Low | 65 | 8.3 | 52 | 22.5 | 117 |
| Moderate | 134 | 17.0 | 59 | 25.5 | 193 |
| High | 588 | 74.7 | 120 | 52.0 | 708 |
| Total | 787 | 100.0 | 231 | 100.0 | 1018 |
| Comparison | chi2 = 51.697; p = 0.0000 | ||||
| PSS-10 Score Range | Possible Awake Bruxism | ||||
| Yes | No | Total | |||
| n | % | n | % | n | |
| Low | 35 | 7.2 | 82 | 15.4 | 117 |
| Moderate | 86 | 17.7 | 107 | 20.2 | 193 |
| High | 366 | 75.1 | 342 | 64.4 | 708 |
| Total | 487 | 100.0 | 531 | 100.0 | 1018 |
| Comparison | chi2 = 20.115; p = 0.0000 | ||||
| PSS-10 Score Range | Possible Sleep Bruxism | ||||
| Yes | No | Total | |||
| n | % | n | % | n | |
| Low | 45 | 7.5 | 72 | 17.2 | 117 |
| Moderate | 95 | 15.8 | 98 | 23.5 | 193 |
| High | 460 | 76.7 | 248 | 59.3 | 708 |
| Total | 600 | 100.0 | 418 | 100.0 | 1018 |
| Comparison | chi2 = 38.448; p = 0.0000 | ||||
| PSS-10 Score versus Coping Strategy | Rank Correlation Coefficient | t Test | Significance p |
|---|---|---|---|
| Planning | −0.140 | −4.500 | 0.0000 |
| Active coping | −0.208 | −6.784 | 0.0000 |
| Self-Blaming | 0.375 | 12.887 | 0.0000 |
| Seeking Instrumental Support | −0.099 | −3.164 | 0.0016 |
| Seeking Emotional Support | −0.015 | −0.470 | 0.6382 |
| Acceptance | −0.192 | −6.232 | 0.0000 |
| Positive reframing | −0.264 | −8.718 | 0.0000 |
| Venting | 0.270 | 8.937 | 0.0000 |
| Religion | −0.035 | −1.108 | 0.2681 |
| Humor | −0.142 | −4.557 | 0.0000 |
| Self-Distraction | 0.101 | 3.222 | 0.0013 |
| Substance Use | 0.155 | 4.991 | 0.0000 |
| Behavioral Disengagement | 0.285 | 9.475 | 0.0000 |
| Denial | 0.195 | 6.350 | 0.0000 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Saczuk, K.; Lapinska, B.; Wawrzynkiewicz, A.; Witkowska, A.; Arbildo-Vega, H.I.; Domarecka, M.; Lukomska-Szymanska, M. Temporomandibular Disorders, Bruxism, Perceived Stress, and Coping Strategies among Medical University Students in Times of Social Isolation during Outbreak of COVID-19 Pandemic. Healthcare 2022, 10, 740. https://doi.org/10.3390/healthcare10040740
Saczuk K, Lapinska B, Wawrzynkiewicz A, Witkowska A, Arbildo-Vega HI, Domarecka M, Lukomska-Szymanska M. Temporomandibular Disorders, Bruxism, Perceived Stress, and Coping Strategies among Medical University Students in Times of Social Isolation during Outbreak of COVID-19 Pandemic. Healthcare. 2022; 10(4):740. https://doi.org/10.3390/healthcare10040740
Chicago/Turabian StyleSaczuk, Klara, Barbara Lapinska, Adam Wawrzynkiewicz, Alicja Witkowska, Heber Isac Arbildo-Vega, Monika Domarecka, and Monika Lukomska-Szymanska. 2022. "Temporomandibular Disorders, Bruxism, Perceived Stress, and Coping Strategies among Medical University Students in Times of Social Isolation during Outbreak of COVID-19 Pandemic" Healthcare 10, no. 4: 740. https://doi.org/10.3390/healthcare10040740