
Prevalence of Psychological Impacts on Healthcare Providers during COVID-19 Pandemic in Asia


Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Search Strategy
2.2. Eligibility Criteria
2.3. Study Selection and Screening
2.4. Quality Assessment and Bias
2.5. Data Extraction
2.6. Data Synthesis and Analysis
3. Results
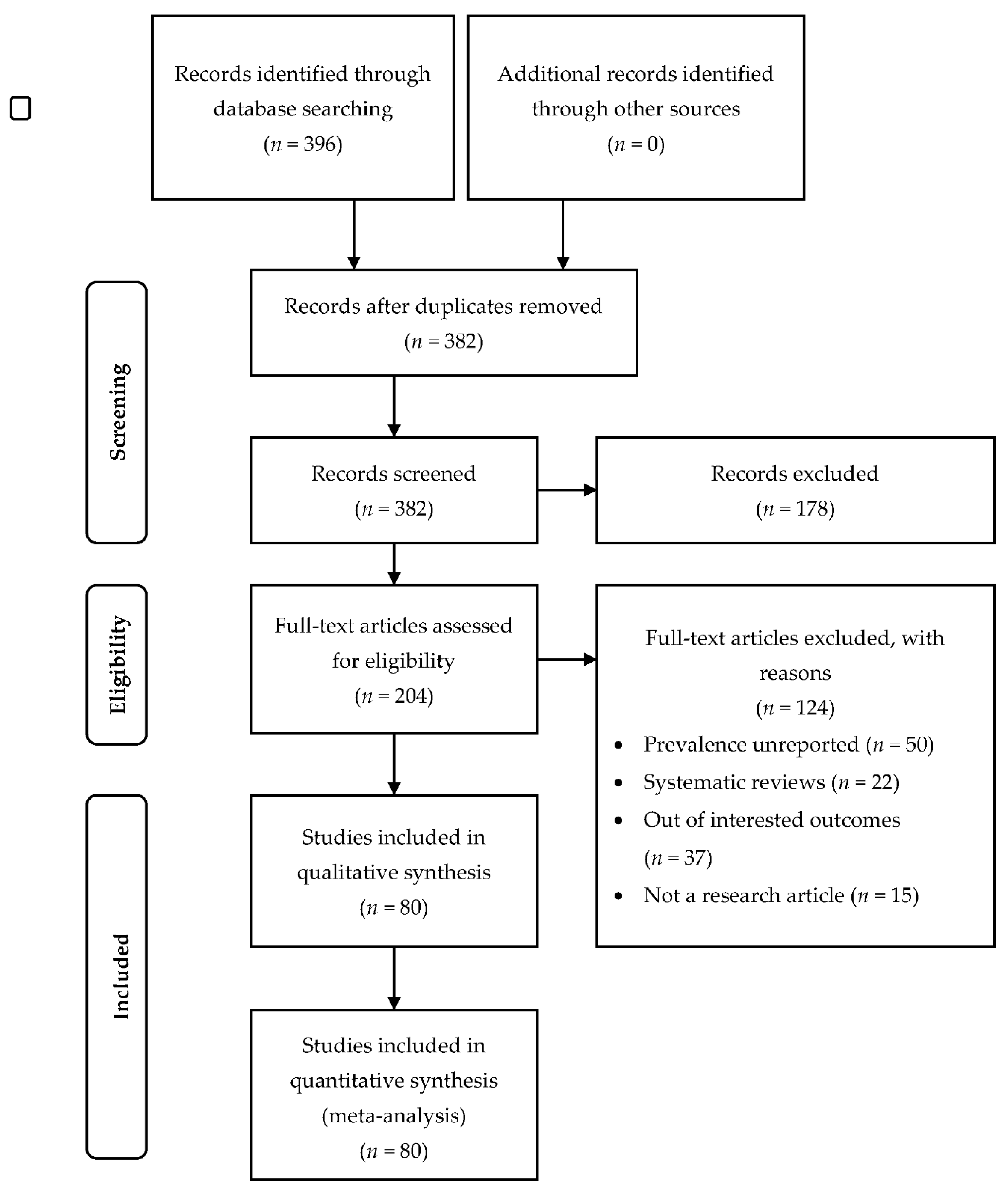
3.1. Searching Results and Study Characteristics
3.2. Prevalence of Anxiety
3.3. Prevalence of Depression
3.4. Prevalence of Stress
3.5. Prevalence of Insomnia
3.6. Prevalence of Post-Traumatic Stress Disorder (PTSD)
3.7. Prevalence of Fear
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- de Oliveira, A.M.; Buchain, P.C.; Vizzotto, A.D.B.; Elkis, H.; Cordeiro, Q. Psychosocial Impact. In Encyclopedia of Behavioral Medicine; Gellman, M.D., Turner, J.R., Eds.; Springer: New York, NY, USA, 2013; pp. 1583–1584. [Google Scholar] [CrossRef]
- Salzberger, B.; Buder, F.; Lampl, B.; Ehrenstein, B.; Hitzenbichler, F.; Holzmann, T.; Schmidt, B.; Hanses, F. Epidemiology of SARS-CoV-2. Infection 2021, 49, 233–239. [Google Scholar] [CrossRef]
- Coto, J.; Restrepo, A.; Cejas, I.; Prentiss, S. The impact of COVID-19 on allied health professions. PLoS ONE 2020, 15, e0241328. [Google Scholar] [CrossRef]
- Naser, A.Y.; Dahmash, E.Z.; Al-Rousan, R.; Alwafi, H.; Alrawashdeh, H.M.; Ghoul, I.; Abidine, A.; Bokhary, M.A.; Al-Hadithi, H.T.; Ali, D.; et al. Mental health status of the general population, healthcare professionals, and university students during 2019 coronavirus disease outbreak in Jordan: A cross-sectional study. Brain Behav. 2020, 10, e01730. [Google Scholar] [CrossRef] [PubMed]
- Deng, Y.; Chen, Y.; Zhang, B. Different prevalence trend of depression and anxiety among healthcare workers and general public before and after the peak of COVID-19 occurred in China: A meta-analysis. Asian J. Psychiatry 2021, 56, 102547. [Google Scholar] [CrossRef] [PubMed]
- Luo, M.; Guo, L.; Yu, M.; Jiang, W.; Wang, H. The psychological and mental impact of coronavirus disease 2019 (COVID-19) on medical staff and general public—A systematic review and meta-analysis. Psychiatry Res. 2020, 291, 113190. [Google Scholar] [CrossRef]
- Shreffler, J.; Petrey, J.; Huecker, M. The Impact of COVID-19 on Healthcare Worker Wellness: A Scoping Review. West. J. Emerg. Med. 2020, 21, 1059–1066. [Google Scholar] [CrossRef] [PubMed]
- Cai, Q.; Feng, H.; Huang, J.; Wang, M.; Wang, Q.; Lu, X.; Xie, Y.; Wang, X.; Liu, Z.; Hou, B.; et al. The mental health of frontline and non-frontline medical workers during the coronavirus disease 2019 (COVID-19) outbreak in China: A case-control study. J. Affect. Disord. 2020, 275, 210–215. [Google Scholar] [CrossRef]
- Liu, C.Y.; Yang, Y.Z.; Zhang, X.M.; Xu, X.; Dou, Q.L.; Zhang, W.W.; Cheng, A.S.K. The prevalence and influencing factors in anxiety in medical workers fighting COVID-19 in China: A cross-sectional survey. Epidemil. Infect. 2020, 148, e98. [Google Scholar] [CrossRef]
- Yang, S.; Kwak, S.G.; Ko, E.J.; Chang, M.C. The Mental Health Burden of the COVID-19 Pandemic on Physical Therapists. Int. J. Environ. Res. Public Health 2020, 17, 3723. [Google Scholar] [CrossRef] [PubMed]
- Zhang, W.R.; Wang, K.; Yin, L.; Zhao, W.F.; Xue, Q.; Peng, M.; Min, B.Q.; Tian, Q.; Leng, H.X.; Du, J.L.; et al. Mental Health and Psychosocial Problems of Medical Health Workers during the COVID-19 Epidemic in China. Psychother. Psychosom. 2020, 89, 242–250. [Google Scholar] [CrossRef]
- Cabarkapa, S.; Nadjidai, S.E.; Murgier, J.; Ng, C.H. The psychological impact of COVID-19 and other viral epidemics on frontline healthcare workers and ways to address it: A rapid systematic review. Brain Behav. Immun. Health 2020, 8, 100144. [Google Scholar] [CrossRef] [PubMed]
- Zvolensky, M.J.; Garey, L.; Rogers, A.H.; Schmidt, N.B.; Vujanovic, A.A.; Storch, E.A.; Buckner, J.D.; Paulus, D.J.; Alfano, C.; Smits, J.A.J.; et al. Psychological, addictive, and health behavior implications of the COVID-19 pandemic. Behav. Res. Ther. 2020, 134, 103715. [Google Scholar] [CrossRef]
- Sarapultseva, M.; Zolotareva, A.; Kritsky, I.; Nasretdinova, N.; Sarapultsev, A. Psychological Distress and Post-Traumatic Symptomatology Among Dental Healthcare Workers in Russia: Results of a Pilot Study. Int. J. Environ. Res. Public Health 2021, 18, 708. [Google Scholar] [CrossRef] [PubMed]
- Babicki, M.; Szewczykowska, I.; Mastalerz-Migas, A.; Galeazzi, G.M. Mental Health in the Era of the Second Wave of SARS-CoV-2: A Cross-Sectional Study Based on an Online Survey among Online Respondents in Poland. Int. J. Environ. Res. Public Health 2021, 18, 2522. [Google Scholar] [CrossRef]
- Wu, K.; Wei, X. Analysis of Psychological and Sleep Status and Exercise Rehabilitation of Front-Line Clinical Staff in the Fight Against COVID-19 in China. Med. Sci. Monit. Basic Res. 2020, 26, e924085. [Google Scholar] [CrossRef]
- Temsah, M.H.; Al-Sohime, F.; Alamro, N.; Al-Eyadhy, A.; Al-Hasan, K.; Jamal, A.; Al-Maglouth, I.; Aljamaan, F.; Al Amri, M.; Barry, M.; et al. The psychological impact of COVID-19 pandemic on health care workers in a MERS-CoV endemic country. J. Infect. Public Health 2020, 13, 877–882. [Google Scholar] [CrossRef]
- Salazar de Pablo, G.; Vaquerizo-Serrano, J.; Catalan, A.; Arango, C.; Moreno, C.; Ferre, F.; Shin, J.I.; Sullivan, S.; Brondino, N.; Solmi, M.; et al. Impact of coronavirus syndromes on physical and mental health of health care workers: Systematic review and meta-analysis. J. Affect. Disord. 2020, 275, 48–57. [Google Scholar] [CrossRef]
- Li, Y.; Scherer, N.; Felix, L.; Kuper, H. Prevalence of depression, anxiety and post-traumatic stress disorder in health care workers during the COVID-19 pandemic: A systematic review and meta-analysis. PLoS ONE 2021, 16, e0246454. [Google Scholar] [CrossRef]
- Batra, K.; Singh, T.P.; Sharma, M.; Batra, R.; Schvaneveldt, N. Investigating the Psychological Impact of COVID-19 among Healthcare Workers: A Meta-Analysis. Int. J. Environ. Res. Public Health 2020, 17, 9096. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. Ann. Intern. Med. 2009, 151, 264–269. [Google Scholar] [CrossRef] [Green Version]
- Aromataris, E.; Munn, Z. JBI Manual for Evidence Synthesis; JBI: Adelaide, Australia, 2020. [Google Scholar] [CrossRef]
- Munn, Z.; Moola, S.; Lisy, K.; Riitano, D.; Tufanaru, C. Methodological guidance for systematic reviews of observational epidemiological studies reporting prevalence and cumulative incidence data. Int. J. Evid. Based Healthc. 2015, 13, 147–153. [Google Scholar] [CrossRef]
- Higgins, J.; Thomas, J.; Chandler, J.; Cumpston, M.; Li, T.; Page, M.; Welch, V. Cochrane Handbook for Systematic Reviews of Interventions Version 6.2 (Updated February 2021); Cochrane: Oxford, UK, 2021. [Google Scholar]
- Borenstein, M.; Higgins, J.P.T. Meta-Analysis and Subgroups. Prev. Sci. 2013, 14, 134–143. [Google Scholar] [CrossRef] [PubMed]
- An, Y.; Sun, Y.; Liu, Z.; Chen, Y. Investigation of the mental health status of frontier-line and non-frontier-line medical staff during a stress period. J. Affect. Disord. 2021, 282, 836–839. [Google Scholar] [CrossRef]
- Awano, N.; Oyama, N.; Akiyama, K.; Inomata, M.; Kuse, N.; Tone, M.; Takada, K.; Muto, Y.; Fujimoto, K.; Akagi, Y.; et al. Anxiety, Depression, and Resilience of Healthcare Workers in Japan During the Coronavirus Disease 2019 Outbreak. Intern. Med. 2020, 59, 2693–2699. [Google Scholar] [CrossRef] [PubMed]
- Cai, Z.; Cui, Q.; Liu, Z.; Li, J.; Gong, X.; Liu, J.; Wan, Z.; Yuan, X.; Li, X.; Chen, C.; et al. Nurses endured high risks of psychological problems under the epidemic of COVID-19 in a longitudinal study in Wuhan China. J. Psychiatr. Res. 2020, 131, 132–137. [Google Scholar] [CrossRef]
- Chen, J.; Liu, X.; Wang, D.; Jin, Y.; He, M.; Ma, Y.; Zhao, X.; Song, S.; Zhang, L.; Xiang, X.; et al. Risk factors for depression and anxiety in healthcare workers deployed during the COVID-19 outbreak in China. Soc. Psychiatry Psychiatr. Epidemiol. 2021, 56, 47–55. [Google Scholar] [CrossRef] [PubMed]
- Guo, W.-P.; Min, Q.; Gu, W.-W.; Yu, L.; Xiao, X.; Yi, W.-B.; Li, H.-L.; Huang, B.; Li, J.-L.; Dai, Y.-J.; et al. Prevalence of mental health problems in frontline healthcare workers after the first outbreak of COVID-19 in China: A cross-sectional study. Health Qual. Life Outcomes 2021, 19, 103. [Google Scholar] [CrossRef]
- Han, L.; Wong, F.K.Y.; She, D.L.M.; Li, S.Y.; Yang, Y.F.; Jiang, M.Y.; Ruan, Y.; Su, Q.; Ma, Y.; Chung, L.Y.F. Anxiety and Depression of Nurses in a North West Province in China During the Period of Novel Coronavirus Pneumonia Outbreak. J. Nurs. Scholarsh. 2020, 52, 564–573. [Google Scholar] [CrossRef]
- Hong, S.; Ai, M.; Xu, X.; Wang, W.; Chen, J.; Zhang, Q.; Wang, L.; Kuang, L. Immediate psychological impact on nurses working at 42 government-designated hospitals during COVID-19 outbreak in China: A cross-sectional study. Nurs. Outlook 2021, 69, 6–12. [Google Scholar] [CrossRef]
- Huang, L.; Wang, Y.; Liu, J.; Ye, P.; Chen, X.; Xu, H.; Qu, H.; Ning, G. Factors Influencing Anxiety of Health Care Workers in the Radiology Department with High Exposure Risk to COVID-19. Med. Sci. Monit. Int. Med. J. Exp. Clin. Res. 2020, 26, e926008. [Google Scholar] [CrossRef]
- Huang, Y.; Zhao, N. Mental health burden for the public affected by the COVID-19 outbreak in China: Who will be the high-risk group? Psychol. Health Med. 2021, 26, 23–34. [Google Scholar] [CrossRef] [Green Version]
- Li, J.; Xu, J.; Zhou, H.; You, H.; Wang, X.; Li, Y.; Liang, Y.; Li, S.; Ma, L.; Zeng, J.; et al. Working conditions and health status of 6,317 front line public health workers across five provinces in China during the COVID-19 epidemic: A cross-sectional study. BMC Public Health 2021, 21, 106. [Google Scholar] [CrossRef]
- Li, R.; Chen, Y.; Lv, J.; Liu, L.; Zong, S.; Li, H.; Li, H. Anxiety and related factors in frontline clinical nurses fighting COVID-19 in Wuhan. Medicine 2020, 99, e21413. [Google Scholar] [CrossRef]
- Li, X.; Li, S.; Xiang, M.; Fang, Y.; Qian, K.; Xu, J.; Li, J.; Zhang, Z.; Wang, B. The prevalence and risk factors of PTSD symptoms among medical assistance workers during the COVID-19 pandemic. J. Psychosom. Res. 2020, 139, 110270. [Google Scholar] [CrossRef] [PubMed]
- Liang, Y.; Wu, K.; Zhou, Y.; Huang, X.; Zhou, Y.; Liu, Z. Mental Health in Frontline Medical Workers during the 2019 Novel Coronavirus Disease Epidemic in China: A Comparison with the General Population. Int. J. Environ. Res. Public Health 2020, 17, 6550. [Google Scholar] [CrossRef]
- Liu, Y.; Chen, H.; Zhang, N.; Wang, X.; Fan, Q.; Zhang, Y.; Huang, L.; Hu, B.; Li, M. Anxiety and depression symptoms of medical staff under COVID-19 epidemic in China. J. Affect. Disord. 2021, 278, 144–148. [Google Scholar] [CrossRef]
- Lu, P.; Li, X.; Lu, L.; Zhang, Y. The psychological states of people after Wuhan eased the lockdown. PLoS ONE 2020, 15, e0241173. [Google Scholar] [CrossRef] [PubMed]
- Lu, W.; Wang, H.; Lin, Y.; Li, L. Psychological status of medical workforce during the COVID-19 pandemic: A cross-sectional study. Psychiatry Res. 2020, 288, 112936. [Google Scholar] [CrossRef]
- Ning, X.; Yu, F.; Huang, Q.; Li, X.; Luo, Y.; Huang, Q.; Chen, C. The mental health of neurological doctors and nurses in Hunan Province, China during the initial stages of the COVID-19 outbreak. BMC Psychiatry 2020, 20, 436. [Google Scholar] [CrossRef]
- Pan, X.; Xiao, Y.; Ren, D.; Xu, Z.-M.; Zhang, Q.; Yang, L.-Y.; Liu, F.; Hao, Y.-S.; Zhao, F.; Bai, Y.-H. Prevalence of mental health problems and associated risk factors among military healthcare workers in specialized COVID-19 hospitals in Wuhan, China: A cross-sectional survey. Asia-Pac. Psychiatry 2020. [Google Scholar] [CrossRef]
- Pang, Y.; Fang, H.; Li, L.; Chen, M.; Chen, Y.; Chen, M. Predictive factors of anxiety and depression among nurses fighting coronavirus disease 2019 in China. Int. J. Ment. Health Nurs. 2021, 30, 524–532. [Google Scholar] [CrossRef]
- Park, C.; Hwang, J.M.; Jo, S.; Bae, S.J.; Sakong, J. COVID-19 Outbreak and Its Association with Healthcare Workers’ Emotional Stress: A Cross-Sectional Study. J. Korean Med. Sci. 2020, 35, e372. [Google Scholar] [CrossRef] [PubMed]
- Park, S.Y.; Kim, B.; Jung, D.S.; Jung, S.I.; Oh, W.S.; Kim, S.W.; Peck, K.R.; Chang, H.H. Psychological distress among infectious disease physicians during the response to the COVID-19 outbreak in the Republic of Korea. BMC Public Health 2020, 20, 1811. [Google Scholar] [CrossRef]
- Si, M.Y.; Su, X.Y.; Jiang, Y.; Wang, W.J.; Gu, X.F.; Ma, L.; Li, J.; Zhang, S.K.; Ren, Z.F.; Ren, R.; et al. Psychological impact of COVID-19 on medical care workers in China. Infect. Dis. Poverty 2020, 9, 113. [Google Scholar] [CrossRef]
- Song, X.; Fu, W.; Liu, X.; Luo, Z.; Wang, R.; Zhou, N.; Yan, S.; Lv, C. Mental health status of medical staff in emergency departments during the Coronavirus disease 2019 epidemic in China. Brain Behav. Immun. 2020, 88, 60–65. [Google Scholar] [CrossRef]
- Tu, Z.H.; He, J.W.; Zhou, N. Sleep quality and mood symptoms in conscripted frontline nurse in Wuhan, China during COVID-19 outbreak: A cross-sectional study. Medicine 2020, 99, e20769. [Google Scholar] [CrossRef]
- Wang, L.Q.; Zhang, M.; Liu, G.M.; Nan, S.Y.; Li, T.; Xu, L.; Xue, Y.; Zhang, M.; Wang, L.; Qu, Y.D.; et al. Psychological impact of coronavirus disease (2019) (COVID-19) epidemic on medical staff in different posts in China: A multicenter study. J. Psychiatr. Res. 2020, 129, 198–205. [Google Scholar] [CrossRef]
- Wang, M.; Zhao, Q.; Hu, C.; Wang, Y.; Cao, J.; Huang, S.; Li, J.; Huang, Y.; Liang, Q.; Guo, Z.; et al. Prevalence of psychological disorders in the COVID-19 epidemic in China: A real world cross-sectional study. J. Affect. Disord. 2021, 281, 312–320. [Google Scholar] [CrossRef]
- Wang, Y.; Ma, S.; Yang, C.; Cai, Z.; Hu, S.; Zhang, B.; Tang, S.; Bai, H.; Guo, X.; Wu, J.; et al. Acute psychological effects of Coronavirus Disease 2019 outbreak among healthcare workers in China: A cross-sectional study. Transl. Psychiatry 2020, 10, 348. [Google Scholar] [CrossRef] [PubMed]
- Xia, Y.; Zhang, H.; Xia, Y.; Li, H.; Zhai, L.; Wang, H. The self-psychological safety maintenance and its influencing factors of community frontline staff during COVID-19 pandemic. Medicine 2021, 100, e24140. [Google Scholar] [CrossRef] [PubMed]
- Xiao, X.; Zhu, X.; Fu, S.; Hu, Y.; Li, X.; Xiao, J. Psychological impact of healthcare workers in China during COVID-19 pneumonia epidemic: A multi-center cross-sectional survey investigation. J. Affect. Disord. 2020, 274, 405–410. [Google Scholar] [CrossRef]
- Xiaoming, X.; Ming, A.; Su, H.; Wo, W.; Jianmei, C.; Qi, Z.; Hua, H.; Xuemei, L.; Lixia, W.; Jun, C.; et al. The psychological status of 8817 hospital workers during COVID-19 Epidemic: A cross-sectional study in Chongqing. J. Affect. Disord. 2020, 276, 555–561. [Google Scholar] [CrossRef] [PubMed]
- Xing, J.; Sun, N.; Xu, J.; Geng, S.; Li, Y. Study of the mental health status of medical personnel dealing with new coronavirus pneumonia. PLoS ONE 2020, 15, e0233145. [Google Scholar] [CrossRef] [PubMed]
- Xu, X.; Wang, W.; Chen, J.; Ai, M.; Shi, L.; Wang, L.; Hong, S.; Zhang, Q.; Hu, H.; Li, X.; et al. Suicidal and self-harm ideation among Chinese hospital staff during the COVID-19 pandemic: Prevalence and correlates. Psychiatry Res. 2021, 296, 113654. [Google Scholar] [CrossRef]
- Zhan, Y.X.; Zhao, S.Y.; Yuan, J.; Liu, H.; Liu, Y.F.; Gui, L.L.; Zheng, H.; Zhou, Y.M.; Qiu, L.H.; Chen, J.H.; et al. Prevalence and Influencing Factors on Fatigue of First-line Nurses Combating with COVID-19 in China: A Descriptive Cross-Sectional Study. Curr. Med. Sci. 2020, 40, 625–635. [Google Scholar] [CrossRef]
- Zhang, H.; Shi, Y.; Jing, P.; Zhan, P.; Fang, Y.; Wang, F. Posttraumatic stress disorder symptoms in healthcare workers after the peak of the COVID-19 outbreak: A survey of a large tertiary care hospital in Wuhan. Psychiatry Res. 2020, 294, 113541. [Google Scholar] [CrossRef]
- Zhao, S.; Cao, J.; Sun, R.; Zhang, L.; Liu, B. Analysis of anxiety-related factors amongst frontline dental staff during the COVID-19 pandemic in Yichang, China. BMC Oral Health 2020, 20, 342. [Google Scholar] [CrossRef] [PubMed]
- Zheng, R.; Zhou, Y.; Fu, Y.; Xiang, Q.; Cheng, F.; Chen, H.; Xu, H.; Fu, L.; Wu, X.; Feng, M.; et al. Prevalence and associated factors of depression and anxiety among nurses during the outbreak of COVID-19 in China: A cross-sectional study. Int. J. Nurs. Stud. 2021, 114, 103809. [Google Scholar] [CrossRef]
- Zhu, W.; Wei, Y.; Meng, X.; Li, J. The mediation effects of coping style on the relationship between social support and anxiety in Chinese medical staff during COVID-19. BMC Health Serv. Res. 2020, 20, 1007. [Google Scholar] [CrossRef]
- Tan, B.Y.Q.; Kanneganti, A.; Lim, L.J.H.; Tan, M.; Chua, Y.X.; Tan, L.; Sia, C.H.; Denning, M.; Goh, E.T.; Purkayastha, S.; et al. Burnout and Associated Factors Among Health Care Workers in Singapore During the COVID-19 Pandemic. J. Am. Med. Dir. Assoc. 2020, 21, 1751–1758.e1755. [Google Scholar] [CrossRef] [PubMed]
- Sunjaya, D.K.; Herawati, D.M.D.; Siregar, A.Y.M. Depressive, anxiety, and burnout symptoms on health care personnel at a month after COVID-19 outbreak in Indonesia. BMC Public Health 2021, 21, 227. [Google Scholar] [CrossRef]
- Mohd Fauzi, M.F.; Mohd Yusoff, H.; Muhamad Robat, R.; Mat Saruan, N.A.; Ismail, K.I.; Mohd Haris, A.F. Doctors’ Mental Health in the Midst of COVID-19 Pandemic: The Roles of Work Demands and Recovery Experiences. Int. J. Environ. Res. Public Health 2020, 17, 7340. [Google Scholar] [CrossRef]
- Tran, T.V.; Nguyen, H.C.; Pham, L.V.; Nguyen, M.H.; Nguyen, H.C.; Ha, T.H.; Phan, D.T.; Dao, H.K.; Nguyen, P.B.; Trinh, M.V.; et al. Impacts and interactions of COVID-19 response involvement, health-related behaviours, health literacy on anxiety, depression and health-related quality of life among healthcare workers: A cross-sectional study. BMJ Open 2020, 10, e041394. [Google Scholar] [CrossRef]
- Sim, S.K.; Lau, B.L.; Zaila, S.R.; Hazira, N.; Aniqah, N.M.; Panicker, J.; Hamzah, A.S. Psychological symptoms among healthcare workers handling COVID-19 patients. Med. J. Malays. 2021, 76, 138–144. [Google Scholar]
- Amin, F.; Sharif, S.; Saeed, R.; Durrani, N.; Jilani, D. COVID-19 pandemic- knowledge, perception, anxiety and depression among frontline doctors of Pakistan. BMC Psychiatry 2020, 20, 459. [Google Scholar] [CrossRef]
- Arshad, A.R.; Islam, F. COVID-19 and Anxiety amongst Doctors: A Pakistani Perspective. J. Coll. Physicians Surg. Pak. JCPSP 2020, 30, 106–109. [Google Scholar] [CrossRef]
- Barua, L.; Zaman, M.S.; Omi, F.R.; Faruque, M. Psychological burden of the COVID-19 pandemic and its associated factors among frontline doctors of Bangladesh: A cross-sectional study. F1000Research 2020, 9, 1304. [Google Scholar] [CrossRef]
- Das, A.; Sil, A.; Jaiswal, S.; Rajeev, R.; Thole, A.; Jafferany, M.; Ali, S.N. A Study to Evaluate Depression and Perceived Stress Among Frontline Indian Doctors Combating the COVID-19 Pandemic. Prim. Care Companion CNS Disord. 2020, 22. [Google Scholar] [CrossRef] [PubMed]
- Gupta, B.; Sharma, V.; Kumar, N.; Mahajan, A. Anxiety and Sleep Disturbances Among Health Care Workers During the COVID-19 Pandemic in India: Cross-Sectional Online Survey. JMIR Public Health Surveill. 2020, 6, e24206. [Google Scholar] [CrossRef]
- Hassannia, L.; Taghizadeh, F.; Moosazadeh, M.; Zarghami, M.; Taghizadeh, H.; Dooki, A.F.; Fathi, M.; Alizadeh-Navaei, R.; Hedayatizadeh-Omran, A.; Dehghan, N. Anxiety and Depression in Health Workers and General Population During COVID-19 in IRAN: A Cross-Sectional Study. Neuropsychopharmacol. Rep. 2021, 41, 40–49. [Google Scholar] [CrossRef]
- Kafle, K.; Shrestha, D.B.; Baniya, A.; Lamichhane, S.; Shahi, M.; Gurung, B.; Tandan, P.; Ghimire, A.; Budhathoki, P. Psychological distress among health service providers during COVID-19 pandemic in Nepal. PLoS ONE 2021, 16, e0246784. [Google Scholar] [CrossRef]
- Khanal, P.; Devkota, N.; Dahal, M.; Paudel, K.; Joshi, D. Mental health impacts among health workers during COVID-19 in a low resource setting: A cross-sectional survey from Nepal. Glob. Health 2020, 16, 89. [Google Scholar] [CrossRef] [PubMed]
- Khanna, R.C.; Honavar, S.G.; Metla, A.L.; Bhattacharya, A.; Maulik, P.K. Psychological impact of COVID-19 on ophthalmologists-in-training and practising ophthalmologists in India. Indian J. Ophthalmol. 2020, 68, 994–998. [Google Scholar] [CrossRef]
- Khatun, M.F.; Parvin, M.F.; Rashid, M.M.; Alam, M.S.; Kamrunnahar, M.; Talukder, A.; Rahman Razu, S.; Ward, P.R.; Ali, M. Mental Health of Physicians During COVID-19 Outbreak in Bangladesh: A Web-Based Cross-Sectional Survey. Front. Public Health 2021, 9, 592058. [Google Scholar] [CrossRef]
- Kumar, D.; Saghir, T.; Ali, G.; Yasin, U.; Furnaz, S.; Karim, M.; Hussain, M.; Kumari, R.; Bai, R.; Kumar, H. Psychosocial Impact of COVID-19 on Healthcare Workers at a Tertiary Care Cardiac Center of Karachi Pakistan. J. Occup. Environ. Med. 2021, 63, e59–e62. [Google Scholar] [CrossRef] [PubMed]
- Moayed, M.S.; Vahedian-Azimi, A.; Mirmomeni, G.; Rahimi-Bashar, F.; Goharimoghadam, K.; Pourhoseingholi, M.A.; Abbasi-Farajzadeh, M.; Hekmat, M.; Sathyapalan, T.; Guest, P.C.; et al. Survey of Immediate Psychological Distress Levels Among Healthcare Workers in the COVID-19 Epidemic: A Cross-Sectional Study. Adv. Exp. Med. Biol. 2021, 1321, 237–243. [Google Scholar] [CrossRef]
- Mohammadian Khonsari, N.; Shafiee, G.; Zandifar, A.; Mohammad Poornami, S.; Ejtahed, H.S.; Asayesh, H.; Qorbani, M. Comparison of psychological symptoms between infected and non-infected COVID-19 health care workers. BMC Psychiatry 2021, 21, 170. [Google Scholar] [CrossRef]
- Pandey, A.; Sharma, C.; Chapagain, R.H.; Devkota, N.; Ranabhat, K.; Pant, S.; Adhikari, K. Stress, Anxiety, Depression and Their Associated Factors among Health Care Workers During COVID -19 Pandemic in Nepal. J. Nepal Health Res. Counc. 2021, 18, 655–660. [Google Scholar] [CrossRef]
- Parthasarathy, R.; Ts, J.; K., T.; Murthy, P. Mental health issues among health care workers during the COVID-19 pandemic—A study from India. Asian J. Psychiatry 2021, 58, 102626. [Google Scholar] [CrossRef]
- Perera, B.; Wickramarachchi, B.; Samanmalie, C.; Hettiarachchi, M. Psychological experiences of healthcare professionals in Sri Lanka during COVID-19. BMC Psychol. 2021, 9, 49. [Google Scholar] [CrossRef]
- Saeed, R.; Amin, F.; Talha, M.; Randenikumara, S.; Shariff, I.; Durrani, N.; Salman, S. COVID-19 Pandemic Prevalence and Risk Factors for Depression among Health Care Workers in South Asia. Asia Pac. J. Public Health 2021. [Google Scholar] [CrossRef]
- Suryavanshi, N.; Kadam, A.; Dhumal, G.; Nimkar, S.; Mave, V.; Gupta, A.; Cox, S.R.; Gupte, N. Mental health and quality of life among healthcare professionals during the COVID-19 pandemic in India. Brain Behav. 2020, 10, e01837. [Google Scholar] [CrossRef] [PubMed]
- AlAteeq, D.A.; Aljhani, S.; Althiyabi, I.; Majzoub, S. Mental health among healthcare providers during coronavirus disease (COVID-19) outbreak in Saudi Arabia. J. Infect. Public Health 2020, 13, 1432–1437. [Google Scholar] [CrossRef]
- Alenazi, T.H.; BinDhim, N.F.; Alenazi, M.H.; Tamim, H.; Almagrabi, R.S.; Aljohani, S.M.; M, H.B.; Almubark, R.A.; Althumiri, N.A.; Alqahtani, S.A. Prevalence and predictors of anxiety among healthcare workers in Saudi Arabia during the COVID-19 pandemic. J. Infect. Public Health 2020, 13, 1645–1651. [Google Scholar] [CrossRef]
- Almater, A.I.; Tobaigy, M.F.; Younis, A.S.; Alaqeel, M.K.; Abouammoh, M.A. Effect of 2019 Coronavirus Pandemic on Ophthalmologists Practicing in Saudi Arabia: A Psychological Health Assessment. Middle East Afr. J. Ophthalmol. 2020, 27, 79–85. [Google Scholar] [CrossRef]
- Alrubaiee, G.G.; Al-Qalah, T.A.H.; Al-Aawar, M.S.A. Knowledge, attitudes, anxiety, and preventive behaviours towards COVID-19 among health care providers in Yemen: An online cross-sectional survey. BMC Public Health 2020, 20, 1541. [Google Scholar] [CrossRef]
- Alsairafi, Z.; Naser, A.Y.; Alsaleh, F.M.; Awad, A.; Jalal, Z. Mental Health Status of Healthcare Professionals and Students of Health Sciences Faculties in Kuwait during the COVID-19 Pandemic. Int. J. Environ. Res. Public Health 2021, 18, 2203. [Google Scholar] [CrossRef]
- Alshekaili, M.; Hassan, W.; Al Said, N.; Al Sulaimani, F.; Jayapal, S.K.; Al-Mawali, A.; Chan, M.F.; Mahadevan, S.; Al-Adawi, S. Factors associated with mental health outcomes across healthcare settings in Oman during COVID-19: Frontline versus non-frontline healthcare workers. BMJ Open 2020, 10, e042030. [Google Scholar] [CrossRef]
- Arafa, A.; Mohammed, Z.; Mahmoud, O.; Elshazley, M.; Ewis, A. Depressed, anxious, and stressed: What have healthcare workers on the frontlines in Egypt and Saudi Arabia experienced during the COVID-19 pandemic? J. Affect. Disord. 2021, 278, 365–371. [Google Scholar] [CrossRef] [PubMed]
- Balay-Odao, E.M.; Alquwez, N.; Inocian, E.P.; Alotaibi, R.S. Hospital Preparedness, Resilience, and Psychological Burden Among Clinical Nurses in Addressing the COVID-19 Crisis in Riyadh, Saudi Arabia. Front. Public Health 2020, 8, 573932. [Google Scholar] [CrossRef]
- Koksal, E.; Dost, B.; Terzi, Ö.; Ustun, Y.B.; Özdin, S.; Bilgin, S. Evaluation of Depression and Anxiety Levels and Related Factors Among Operating Theater Workers During the Novel Coronavirus (COVID-19) Pandemic. J. Perianesthesia Nurs. 2020, 35, 472–477. [Google Scholar] [CrossRef] [PubMed]
- Şahin, M.K.; Aker, S.; Şahin, G.; Karabekiroğlu, A. Prevalence of Depression, Anxiety, Distress and Insomnia and Related Factors in Healthcare Workers During COVID-19 Pandemic in Turkey. J. Community Health 2020, 45, 1168–1177. [Google Scholar] [CrossRef] [PubMed]
- Yıldırım, M.; Özaslan, A. Worry, Severity, Controllability, and Preventive Behaviours of COVID-19 and Their Associations with Mental Health of Turkish Healthcare Workers Working at a Pandemic Hospital. Int. J. Ment. Health Addict. 2021, 1–15. [Google Scholar] [CrossRef]
- Yilmaz, A.; Karakoyun, D.O.; Isik, H.S.; Bostan, S. The Effect of the COVID-19 Pandemic on Functioning of Neurosurgery Clinics and the Anxiety Levels of Neurosurgeons in Turkey. Turk. Neurosurg. 2020, 30, 944–951. [Google Scholar] [CrossRef]
- Yörük, S.; Güler, D. The relationship between psychological resilience, burnout, stress, and sociodemographic factors with depression in nurses and midwives during the COVID-19 pandemic: A cross-sectional study in Turkey. Perspect. Psychiatr. Care 2021, 57, 390–398. [Google Scholar] [CrossRef]
- Chew, N.W.S.; Lee, G.K.H.; Tan, B.Y.Q.; Jing, M.; Goh, Y.; Ngiam, N.J.H.; Yeo, L.L.L.; Ahmad, A.; Ahmed Khan, F.; Napolean Shanmugam, G.; et al. A multinational, multicentre study on the psychological outcomes and associated physical symptoms amongst healthcare workers during COVID-19 outbreak. Brain Behav. Immun. 2020, 88, 559–565. [Google Scholar] [CrossRef]
- Chew, N.W.S.; Ngiam, J.N.; Tan, B.Y.-Q.; Tham, S.-M.; Tan, C.Y.-S.; Jing, M.; Sagayanathan, R.; Chen, J.T.; Wong, L.Y.H.; Ahmad, A.; et al. Asian-Pacific perspective on the psychological well-being of healthcare workers during the evolution of the COVID-19 pandemic. BJPsych Open 2020, 6, e116. [Google Scholar] [CrossRef]
- Neto, M.L.R.; Almeida, H.G.; Esmeraldo, J.D.; Nobre, C.B.; Pinheiro, W.R.; de Oliveira, C.R.T.; Sousa, I.D.C.; Lima, O.; Lima, N.N.R.; Moreira, M.M.; et al. When health professionals look death in the eye: The mental health of professionals who deal daily with the 2019 coronavirus outbreak. Psychiatry Res. 2020, 288, 112972. [Google Scholar] [CrossRef]
- Krishnamoorthy, Y.; Nagarajan, R.; Saya, G.K.; Menon, V. Prevalence of psychological morbidities among general population, healthcare workers and COVID-19 patients amidst the COVID-19 pandemic: A systematic review and meta-analysis. Psychiatry Res. 2020, 293, 113382. [Google Scholar] [CrossRef]
- Al Maqbali, M.; Al Sinani, M.; Al-Lenjawi, B. Prevalence of stress, depression, anxiety and sleep disturbance among nurses during the COVID-19 pandemic: A systematic review and meta-analysis. J. Psychosom. Res. 2021, 141, 110343. [Google Scholar] [CrossRef]
- Lai, J.; Ma, S.; Wang, Y.; Cai, Z.; Hu, J.; Wei, N.; Wu, J.; Du, H.; Chen, T.; Li, R.; et al. Factors associated with mental health outcomes among health care workers exposed to Coronavirus Disease 2019. JAMA Netw. Open 2020, 3, e203976. [Google Scholar] [CrossRef]
- Zhang, C.; Yang, L.; Liu, S.; Ma, S.; Wang, Y.; Cai, Z.; Du, H.; Li, R.; Kang, L.; Su, M.; et al. Survey of Insomnia and Related Social Psychological Factors Among Medical Staff Involved in the 2019 Novel Coronavirus Disease Outbreak. Front Psychiatry 2020, 11. [Google Scholar] [CrossRef]
- Okajima, I.; Chung, S.; Suh, S. Validation of the Japanese-version Stress and Anxiety to Viral Epidemics-9 (SAVE-9) and relationship among stress, insomnia, anxiety, and depression in healthcare workers exposed to coronavirus disease 20191. Sleep Med. 2021, 84, 397–402. [Google Scholar] [CrossRef]
- Chang, M.C.; Park, D. Incidence of Post-Traumatic Stress Disorder after Coronavirus Disease. Healthcare 2020, 8, 373. [Google Scholar] [CrossRef]
- Pappa, S.; Chen, J.; Barnet, J.; Chang, A.; Dong, R.K.; Xu, W.; Yin, A.; Chen, B.Z.; Delios, A.; Chen, R.Z.; et al. A Systematic Review and Meta-Analysis of the Mental Health Symptoms during the Covid-19 Pandemic in Southeast Asia. MedRxiv 2021. [Google Scholar] [CrossRef]
- Busch, I.M.; Moretti, F.; Mazzi, M.; Wu, A.W.; Rimondini, M. What We Have Learned from Two Decades of Epidemics and Pandemics: A Systematic Review and Meta-Analysis of the Psychological Burden of Frontline Healthcare Workers. Psychother. Psychosom. 2021, 1–13. [Google Scholar] [CrossRef]
- Mohd Noor, N.; Che Yusof, R.; Yacob, M.A. Anxiety in Frontline and Non-Frontline Healthcare Providers in Kelantan, Malaysia. Int. J. Environ. Res. Public Health 2021, 18, 861. [Google Scholar] [CrossRef] [PubMed]
- Tan, B.Y.Q.; Chew, N.W.S.; Lee, G.K.H.; Jing, M.; Goh, Y.; Yeo, L.L.L.; Zhang, K.; Chin, H.K.; Ahmad, A.; Khan, F.A.; et al. Psychological impact of the COVID-19 pandemic on health care workers in Singapore. Ann. Intern. Med. 2020, 173, 317–320. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chou, W.-P.; Wang, P.-W.; Chen, S.-L.; Chang, Y.-P.; Wu, C.-F.; Lu, W.-H.; Yen, C.-F. Risk Perception, Protective Behaviors, and General Anxiety during the Coronavirus Disease 2019 Pandemic among Affiliated Health Care Professionals in Taiwan: Comparisons with Frontline Health Care Professionals and the General Public. Int. J. Environ. Res. Public Health 2020, 17, 9329. [Google Scholar] [CrossRef] [PubMed]
- Danet Danet, A. Psychological impact of COVID-19 pandemic in Western frontline healthcare professionals. A systematic review. Med. Clínica 2021, 156, 449–458. [Google Scholar] [CrossRef] [PubMed]
- Shaukat, N.; Ali, D.M.; Razzak, J. Physical and mental health impacts of COVID-19 on healthcare workers: A scoping review. Int. J. Emerg. Med. 2020, 13, 40. [Google Scholar] [CrossRef] [PubMed]
- Labrague, L.J.; De Los Santos, J.A.A. COVID-19 anxiety among front-line nurses: Predictive role of organisational support, personal resilience and social support. J. Nurs. Manag. 2020, 28, 1653–1661. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Outcome | No. of Studies | No. of Participants | Prevalence [95% CI] | I2 (%) | p-Value | |
|---|---|---|---|---|---|---|
| Overall anxiety | 68 | 124,925 | 34.81 [30.80, 38.83] | 100 | p < 0.001 | |
| Subgroup | ||||||
| Regions | Eastern Asia | 35 | 90,039 | 28.99 [24.91, 33.07] | 100 | p < 0.001 |
| South-Eastern Asia | 7 | 13,140 | 24.78 [10.51, 39.05] | 100 | p < 0.001 | |
| Southern Asia | 14 | 5449 | 38.42 [22.89, 53.94] | 100 | p < 0.001 | |
| Western Asia | 14 | 16,297 | 46.57 [33.34, 59.80] | 100 | p < 0.001 | |
| Type of healthcare provider | Frontline | 13 | 7816 | 24.02 [15.89, 32.16] | 99 | p < 0.001 |
| Non-frontline | 13 | 13,619 | 24.35 [18.71, 29.99] | 99 | p < 0.001 | |
| Sex | Female | 21 | 19,800 | 36.14 [22.50, 49.78] | 100 | p < 0.001 |
| Male | 21 | 7788 | 32.76 [18.16, 47.36] | 100 | p < 0.001 | |
| Occupation | Doctors | 18 | 7279 | 30.10 [20.56, 39.64] | 99 | p < 0.001 |
| Nurses | 18 | 11,574 | 36.06 [23.75, 48.38] | 100 | p < 0.001 | |
| Outcome | No. of Studies | No. of Participants | Prevalence [95% CI] | I2 (%) | p-Value | |
|---|---|---|---|---|---|---|
| Overall depression | 60 | 132,308 | 34.61 [30.87, 38.36] | 100 | p < 0.001 | |
| Subgroup | ||||||
| Regions | Eastern Asia | 33 | 103,868 | 31.47 [26.88, 36.05] | 99 | p < 0.001 |
| South-Eastern Asia | 7 | 13,140 | 22.96 [13.23, 32.68] | 98 | p < 0.001 | |
| Southern Asia | 13 | 6563 | 38.51 [22.77, 54.26] | 98 | p < 0.001 | |
| Western Asia | 9 | 8737 | 43.78 [28.36, 59.19] | 99 | p < 0.001 | |
| Type of healthcare provider | Frontline | 12 | 7656 | 32.69 [19.55, 45.84] | 100 | p < 0.001 |
| Non-frontline | 12 | 13,458 | 28.76 [20.43, 37.09] | 99 | p < 0.001 | |
| Sex | Female | 22 | 18,306 | 32.32 [24.36, 40.28] | 100 | p < 0.001 |
| Male | 22 | 7648 | 27.36 [20.31, 34.41] | 99 | p < 0.001 | |
| Occupation | Doctors | 19 | 6845 | 28.34 [18.93, 37.75] | 99 | p < 0.001 |
| Nurses | 19 | 10,159 | 36.64 [27.10, 46.18] | 99 | p < 0.001 | |
| Outcome | No. of Studies | No. of Participants | Prevalence [95% CI] | I2 (%) | p-Value | |
|---|---|---|---|---|---|---|
| Overall stress | 20 | 12,673 | 31.72 [21.25, 42.18] | 100 | p < 0.001 | |
| Subgroup | ||||||
| Regions | Eastern Asia | 4 | 3870 | 19.42 [−4.88, 43.72] | 98 | p < 0.001 |
| South-Eastern Asia | 3 | 1635 | 28.23 [10.50, 45.96] | 95 | p < 0.001 | |
| Southern Asia | 7 | 2885 | 31.41 [13.46, 49.35] | 95 | p < 0.001 | |
| Western Asia | 6 | 5559 | 48.97 [30.67, 67.28] | 99 | p < 0.001 | |
| Type of healthcare provider | Frontline | 2 | 647 | 41.51 [−29.76, 112.79] | 100 | p < 0.001 |
| Non-frontline | 2 | 407 | 38.39 [−31.53, 108.31] | 100 | p < 0.001 | |
| Sex | Female | 5 | 1105 | 59.96 [31.01, 88.92] | 99 | p < 0.001 |
| Male | 5 | 852 | 42.46 [17.56, 67.37] | 99 | p < 0.001 | |
| Occupation | Doctors | 2 | 688 | 61.08 [32.79, 89.37] | 97 | p < 0.001 |
| Nurses | 2 | 315 | 79.19 [72.88, 85.50] | 30 | 0.230 | |
| Outcome | No of Studies | No of Participants | Prevalence [95% CI] | I2 (%) | p-Value | |
|---|---|---|---|---|---|---|
| Overall insomnia | 12 | 14,877 | 37.89 [25.43, 50.35] | 100 | p < 0.001 | |
| Subgroup | ||||||
| Regions | Eastern Asia | 6 | 10,909 | 41.23 [19.75, 62.70] | 100 | p < 0.001 |
| South-Eastern Asia | 0 | NA | ||||
| Southern Asia | 3 | 1783 | 31.30 [17.82, 44.78] | 89 | 0.0001 | |
| Western Asia | 3 | 2185 | 37.80 [13.20, 62.40] | 98 | p < 0.001 | |
| Type of healthcare provider | Frontline | 3 | 2090 | 49.27 [45.42, 53.12] | 64 | 0.060 |
| Non-frontline | 3 | 1904 | 35.10 [25.39, 44.81] | 94 | p < 0.001 | |
| Sex | Female | 3 | 1402 | 51.61 [26.75, 76.47] | 99 | p < 0.001 |
| Male | 3 | 735 | 44.16 [8.05, 80.26] | 99 | p < 0.001 | |
| Occupation | Doctors | 1 | 161 | 29.19 [22.17, 36.22] | NA | |
| Nurses | 1 | 167 | 41.92 [34.43, 49.40] | NA | ||
| Outcome | No of Studies | No of Participants | Prevalence [95% CI] | I2 (%) | p-Value | |
|---|---|---|---|---|---|---|
| Overall PTSD | 9 | 23,012 | 15.29 [11.43, 19.15] | 99 | p < 0.001 | |
| Subgroup | ||||||
| Regions | Eastern Asia | 7 | 20,960 | 17.61 [12.59, 22.62] | 99 | p < 0.001 |
| South-Eastern Asia | 2 | 1242 | 9.73 [5.38, 14.08] | 86 | 0.008 | |
| Southern Asia | 2 | 810 | 4.58 [−0.51, 9.66] | 92 | 0.0004 | |
| Western Asia | 0 | NA | ||||
| Type of healthcare provider | Frontline | 3 | 1249 | 22.86 [11.39, 34.32] | 95 | p < 0.001 |
| Non-frontline | 3 | 1679 | 15.81 [4.61, 27.00] | 96 | p < 0.001 | |
| Sex | Female | 2 | 2300 | 10.81 [9.54, 12.07] | 0 | 0.440 |
| Male | 2 | 688 | 8.12 [4.41, 11.82] | 70 | 0.070 | |
| Occupation | Doctors | 2 | 688 | 9.65 [3.22, 16.07] | 76 | 0.040 |
| Nurses | 2 | 1591 | 13.85 [7.46, 20.25] | 85 | 0.009 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Norhayati, M.N.; Che Yusof, R.; Azman, M.Y. Prevalence of Psychological Impacts on Healthcare Providers during COVID-19 Pandemic in Asia. Int. J. Environ. Res. Public Health 2021, 18, 9157. https://doi.org/10.3390/ijerph18179157
Norhayati MN, Che Yusof R, Azman MY. Prevalence of Psychological Impacts on Healthcare Providers during COVID-19 Pandemic in Asia. International Journal of Environmental Research and Public Health. 2021; 18(17):9157. https://doi.org/10.3390/ijerph18179157
Chicago/Turabian StyleNorhayati, Mohd Noor, Ruhana Che Yusof, and Mohd Yacob Azman. 2021. "Prevalence of Psychological Impacts on Healthcare Providers during COVID-19 Pandemic in Asia" International Journal of Environmental Research and Public Health 18, no. 17: 9157. https://doi.org/10.3390/ijerph18179157