
Global Healthcare Needs Related to COVID-19: An Evidence Map of the First Year of the Pandemic

 , , , , , and
, , , , , and
Abstract
:1. Introduction
1.1. Evidence Mapping
1.2. Objectives
2. Materials and Methods
2.1. Protocol Registration and Guideline
2.2. Literature Search
2.3. Eligibility Criteria
2.4. Study Selection
2.5. Data Extraction
2.6. Data Coding and Synthesis
3. Results
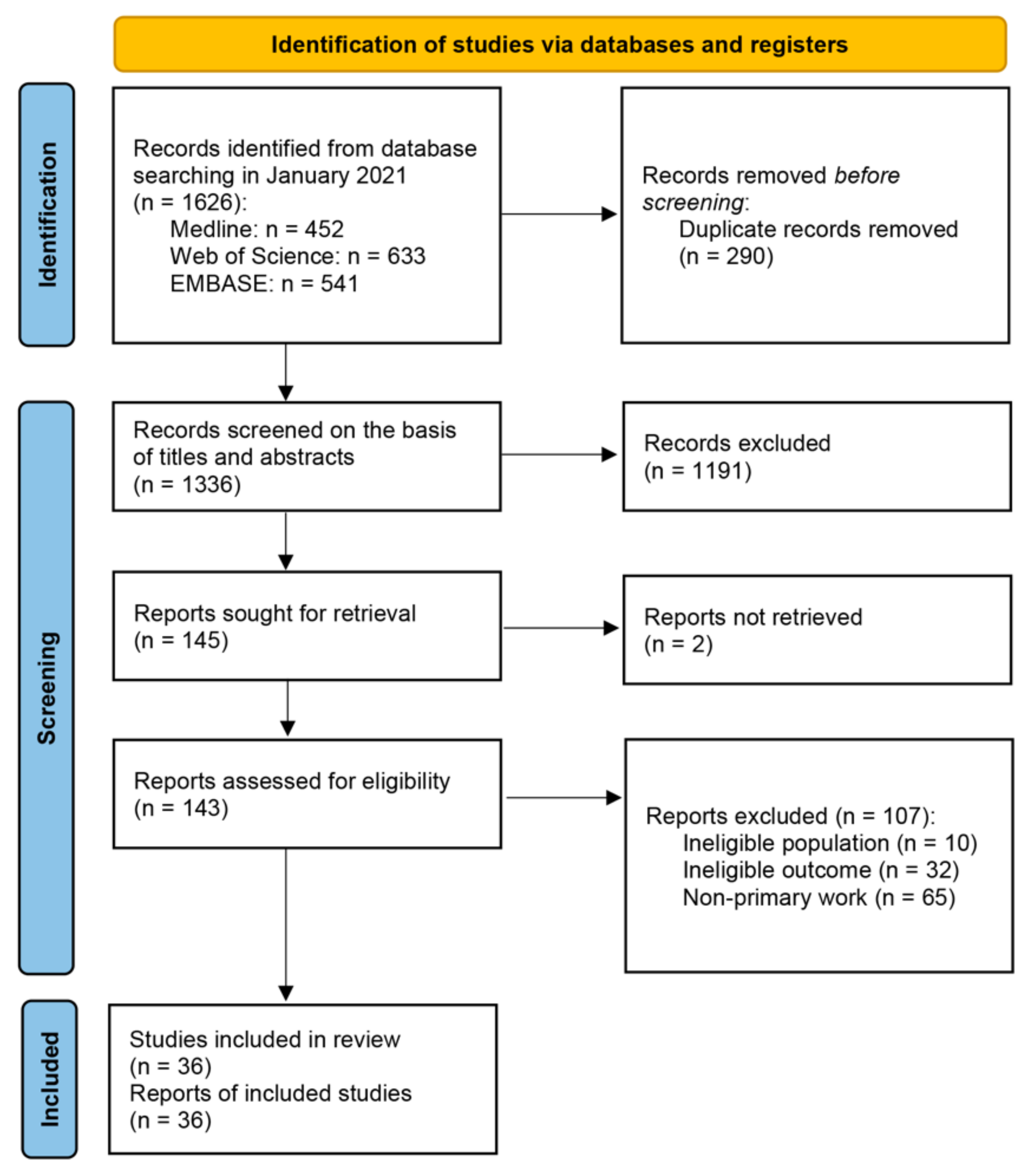
3.1. Literature Search and Selection Process
3.2. Key Characteristics of the Included Studies
3.3. Type of Needs and Evidence Clusters
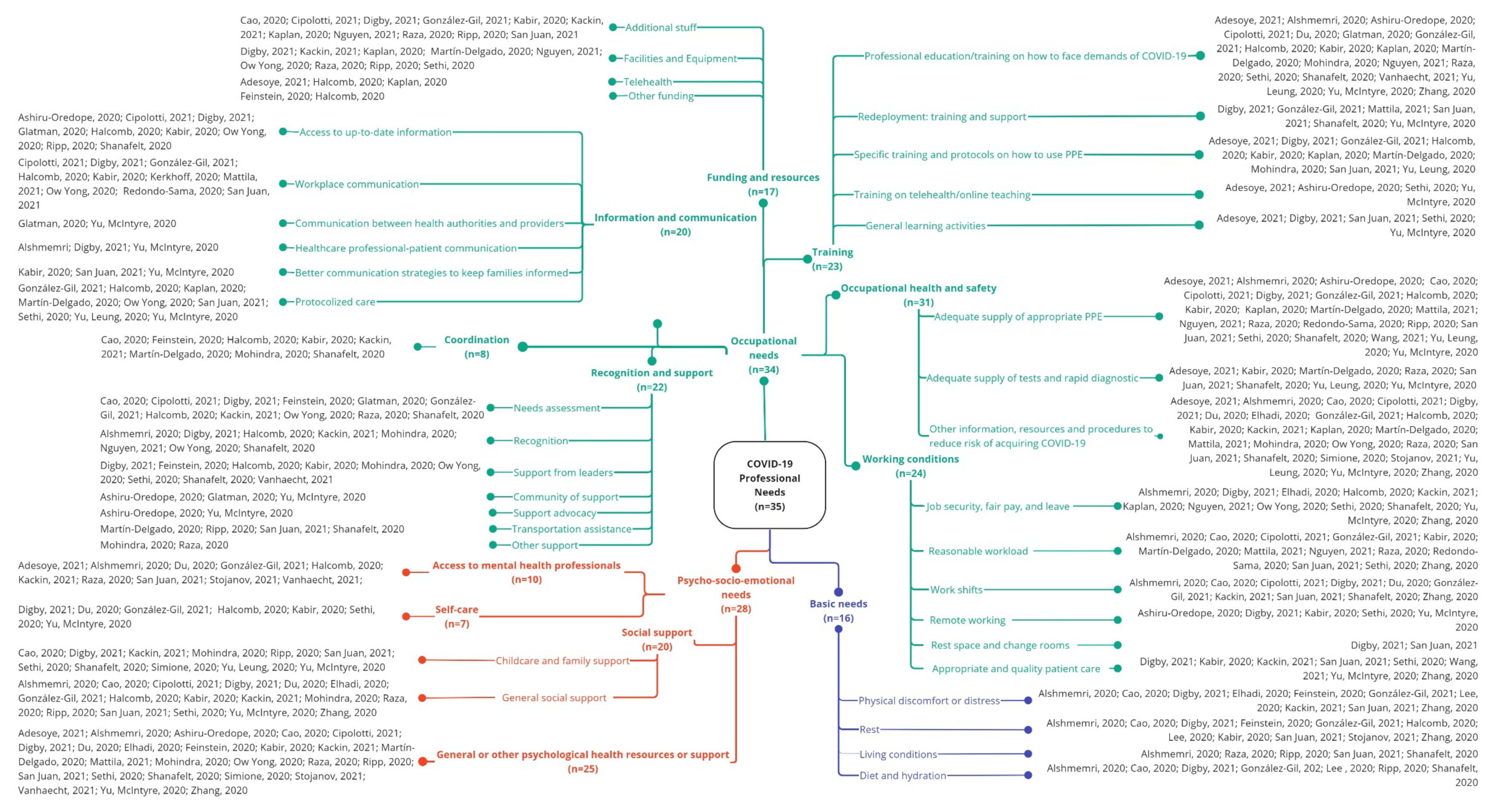
3.3.1. Professionals’ Needs during the First Year of COVID-19
3.3.1.1. Basic Needs
3.3.1.2. Occupational Needs

- Funding and Resources (n = 17)
- Coordination (n = 8)
- Information and Communication (n = 20)
- Recognition and Support (n = 22)
- Training (n = 23)
- Occupational Health and Safety (n = 31)
- Working Conditions (n = 24)
3.3.1.3. Psycho-Socio-Emotional Needs
- Access to Mental Health Professionals (n = 10)
- Self-Care (n = 7)
- Social Support (n = 20)
- General Psychological Health Support or Other Psychological Health Resources (n = 25)
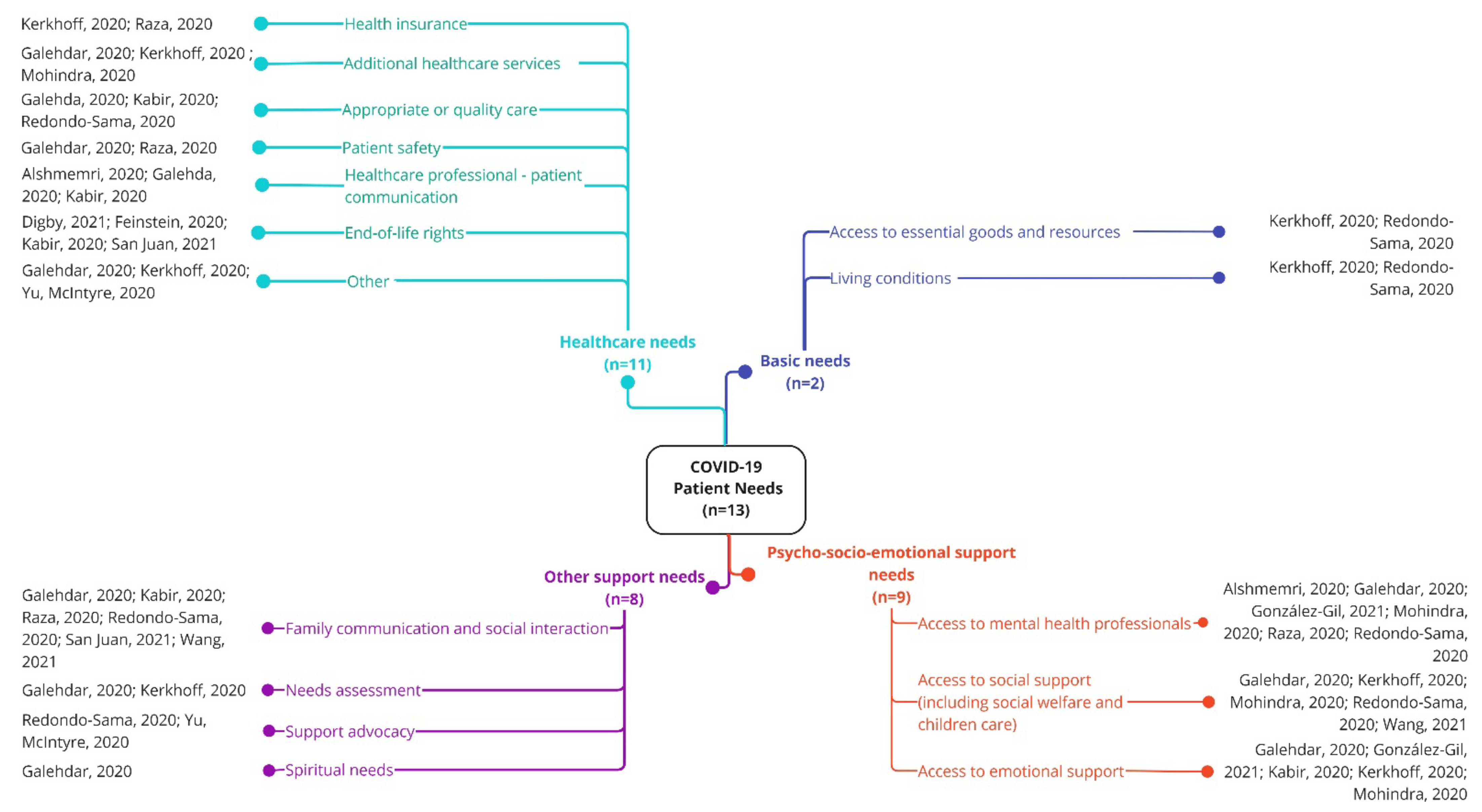
3.3.2. Patients’ Needs during the First Year of COVID-19
3.3.2.1. Basic Needs
3.3.2.2. Healthcare Needs
3.3.2.3. Psycho-Socio-Emotional Needs
3.3.2.4. Other Support Needs
3.3.3. Family Members’ Needs during the First Year of COVID-19
3.3.3.1. Psycho-Socio-Emotional Needs
3.3.3.2. Communication Needs
3.3.4. Transversal Needs during the First Year of COVID-19
3.3.4.1. Public Safety Needs
3.3.4.2. Information and Communication Needs
3.3.4.3. Other Needs
4. Discussion
4.1. Evidence Clusters
4.2. Evidence Gaps
4.3. Implications for Practice
- Macro-level Interventions
- Meso-level Interventions
- Clinical level Interventions
4.4. Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Hui, D.S.; Azhar, E.I.; Madani, T.A.; Ntoumi, F.; Kock, R.; Dar, O.; Ippolito, G.; Mchugh, T.D.; Memish, Z.A.; Drosten, C.; et al. The Continuing 2019-NCoV Epidemic Threat of Novel Coronaviruses to Global Health—The Latest 2019 Novel Coronavirus Outbreak in Wuhan, China. Int. J. Infect. Dis. 2020, 91, 264–266. [Google Scholar] [CrossRef]
- WHO Announces COVID-19 Outbreak a Pandemic. Available online: https://www.euro.who.int/en/health-topics/health-emergencies/coronavirus-covid-19/news/news/2020/3/who-announces-covid-19-outbreak-a-pandemic (accessed on 21 April 2022).
- Legido-Quigley, H.; Mateos-García, J.T.; Campos, V.R.; Gea-Sánchez, M.; Muntaner, C.; McKee, M. The Resilience of the Spanish Health System against the COVID-19 Pandemic. Lancet Public Health 2020, 5, e251–e252. [Google Scholar] [CrossRef]
- Litewka, S.G.; Heitman, E. Latin American Healthcare Systems in Times of Pandemic. Dev. World Bioeth. 2020, 20, 69–73. [Google Scholar] [CrossRef]
- Juan, V.N.S.; Aceituno, D.; Djellouli, N.; Sumray, K.; Regenold, N.; Syversen, A.; Symmons, S.M.; Dowrick, A.; Mitchinson, L.; Singleton, G.; et al. Mental Health and Well-Being of Healthcare Workers during the COVID-19 Pandemic in the UK: Contrasting Guidelines with Experiences in Practice. BJPsych Open 2021, 7, E15. [Google Scholar] [CrossRef]
- Rana, B.K. COVID-19 Response in South-East Asia: Promoting Healthcare Quality through Political Engagement. IJQHC Commun. 2022, 1, lyab009. [Google Scholar] [CrossRef]
- McMahon, M.; Nadigel, J.; Thompson, E.; Glazier, R.H. Informing Canada’s Health System Response to COVID-19: Priorities for Health Services and Policy Research. Healthc. Policy 2020, 16, 112–124. [Google Scholar] [CrossRef] [PubMed]
- Bramucci, A.; Prante, F.; Truger, A. Decades of Tight Fiscal Policy Have Left the Health Care System in Italy Ill-Prepared to Fight the COVID-19 Outbreak. Intereconomics 2020, 2020, 147–152. [Google Scholar]
- Vasileiou, E. Fighting a War without Weapons? Lessons from the COVID-19 Outbreak. World Med. Health Policy 2021, 13, 383–390. [Google Scholar] [CrossRef] [PubMed]
- Alqahtani, F.; Khan, A.; Alowais, J.; Alaama, T.; Jokhdar, H. Bed Surge Capacity in Saudi Hospitals during the COVID-19 Pandemic. Disaster Med. Public Health Prep. 2021, 19, 1–7. [Google Scholar] [CrossRef]
- Xu, H.; Intrator, O.; Bowblis, J.R. Shortages of Staff in Nursing Homes during the COVID-19 Pandemic: What Are the Driving Factors? J. Am. Med. Dir. Assoc. 2020, 21, 1371–1377. [Google Scholar] [CrossRef]
- Lupu, D.; Tiganasu, R. COVID-19 and the Efficiency of Health Systems in Europe. Health Econ. Rev. 2022, 12, 14. [Google Scholar] [CrossRef]
- Alshmemri, M.S.; Ramaiah, P. Nurses Experiences and Challenges during COVID 19: Mixed Method Approach. J. Pharm. Res. Int. 2020, 32, 81–87. [Google Scholar] [CrossRef]
- Ramaci, T.; Barattucci, M.; Ledda, C.; Rapisarda, V. Social Stigma during COVID-19 and Its Impact on HCWs Outcomes. Sustainability 2020, 12, 3834. [Google Scholar] [CrossRef]
- Norful, A.A.; Rosenfeld, A.; Schroeder, K.; Travers, J.L.; Aliyu, S. Primary Drivers and Psychological Manifestations of Stress in Frontline Healthcare Workforce during the Initial COVID-19 Outbreak in the United States. Gen. Hosp. Psychiatry 2021, 69, 20–26. [Google Scholar] [CrossRef]
- Martinez, M.; Stewart, N.H.; Koza, A.L.; Dhaon, S.; Shoushtari, C.; Arora, V.M. The Effect of Redeployment during the COVID-19 Pandemic on Development of Anxiety, Depression, and Insomnia in Healthcare Workers. J. Gen. Intern. Med. 2022, 37, 1003–1005. [Google Scholar] [CrossRef]
- Ballantyne, H.; Achour, N. The Challenges of Nurse Redeployment and Opportunities for Leadership during COVID-19 Pandemic. Disaster Med. Public Health Prep. 2022, 14, 1–7. [Google Scholar] [CrossRef]
- Chang, A.Y.; Cullen, M.R.; Harrington, R.A.; Barry, M. The Impact of Novel Coronavirus COVID-19 on Noncommunicable Disease Patients and Health Systems: A Review. J. Intern. Med. 2021, 289, 450–462. [Google Scholar] [CrossRef]
- Golinelli, D.; Sanmarchi, F.; Capodici, A.; Gribaudo, G.; Altini, M.; Rosa, S.; Esposito, F.; Fantini, M.P.; Lenzi, J. Variations of the Quality of Care during the COVID-19 Pandemic Affected the Mortality Rate of Non-COVID-19 Patients with Hip Fracture. PLoS ONE 2022, 17, e0263944. [Google Scholar] [CrossRef]
- Tuczyńska, M.; Staszewski, R.; Matthews-Kozanecka, M.; Żok, A.; Baum, E. Quality of the Healthcare Services during COVID-19 Pandemic in Selected European Countries. Front. Public Health 2022, 10, 870314. [Google Scholar] [CrossRef]
- Curnow, E.; Tyagi, V.; Salisbury, L.; Stuart, K.; Melville-Jóhannesson, B.; Nicol, K.; McCormack, B.; Dewing, J.; Magowan, R.; Sagan, O.; et al. Person-Centered Healthcare Practice in a Pandemic Context: An Exploration of People’s Experience of Seeking Healthcare Support. Front. Rehabil. Sci. 2021, 2, 726210. [Google Scholar] [CrossRef]
- Sandhu, S.; Lemmon, M.E.; Eisenson, H.; Crowder, C.; Bettger, J.P. Addressing the Social Determinants of Health during the COVID-19 Pandemic: Ensuring Equity, Quality, and Sustainability. Fam. Community Health 2021, 44, 78–80. [Google Scholar] [CrossRef]
- Wittenberg, E.; Goldsmith, J.V.; Chen, C.; Prince-Paul, M.; Johnson, R.R. Opportunities to Improve COVID-19 Provider Communication Resources: A Systematic Review. Patient Educ. Couns. 2021, 104, 438–451. [Google Scholar] [CrossRef]
- Galehdar, N.; Toulabi, T.; Kamran, A.; Heydari, H. Exploring Nurses’ Perception about the Care Needs of Patients with COVID-19: A Qualitative Study. BMC Nurs. 2020, 19, 119. [Google Scholar] [CrossRef]
- Chen, C.; Haupert, S.R.; Zimmermann, L.; Shi, X.; Fritsche, L.G.; Mukherjee, B. Global Prevalence of Post COVID-19 Condition or Long COVID: A Meta-Analysis and Systematic Review. J. Infect. Dis. 2022. ahead of print. [Google Scholar] [CrossRef]
- Groff, D.; Sun, A.; Ssentongo, A.E.; Ba, D.M.; Parsons, N.; Poudel, G.R.; Lekoubou, A.; Oh, J.S.; Ericson, J.E.; Ssentongo, P.; et al. Short-Term and Long-Term Rates of Postacute Sequelae of SARS-CoV-2 Infection: A Systematic Review. JAMA Netw. Open 2021, 4, e2128568. [Google Scholar] [CrossRef] [PubMed]
- O’Brien, H.; Tracey, M.J.; Ottewill, C.; O’Brien, M.E.; Morgan, R.K.; Costello, R.W.; Gunaratnam, C.; Ryan, D.; McElvaney, N.G.; McConkey, S.J.; et al. An Integrated Multidisciplinary Model of COVID-19 Recovery Care. Ir. J. Med. Sci. 2020, 190, 461–468. [Google Scholar] [CrossRef] [PubMed]
- Masroor, S. Collateral Damage of COVID-19 Pandemic: Delayed Medical Care. J. Card. Surg. 2020, 35, 1345–1347. [Google Scholar] [CrossRef] [PubMed]
- Yancy, C.W. COVID-19 and African Americans. JAMA 2020, 323, 1891–1892. [Google Scholar] [CrossRef]
- Tanoue, Y.; Nomura, S.; Yoneoka, D.; Kawashima, T.; Eguchi, A.; Shi, S.; Harada, N.; Miyata, H. Mental Health of Family, Friends, and Co-Workers of COVID-19 Patients in Japan. Psychiatry Res. 2020, 291, 113067. [Google Scholar] [CrossRef]
- Collaboration for Environmental Evidence. Collaboration for Environmental Evidence Guidelines for Systematic Review and Evidence Synthesis in Environmental Management. Version 4.2; Centre for Evidence-Based Conservation Bangor University: Wales, UK, 2013. [Google Scholar]
- Bates, S.; Clapton, J.; Coren, E. Systematic Maps to Support the Evidence Base in Social Care. Evid. Policy A J. Res. Debate Pract. 2007, 3, 539–551. [Google Scholar] [CrossRef]
- Clapton, J.; Rutter, D.; Sharif, N. SCIE Systematic Mapping Guidance; SCIE: London, UK, 2009. [Google Scholar]
- Gonzalez, A.I.G.; Schmucker, C.; Nothacker, J.; Motschall, E.; Nguyen, T.S.; Brueckle, M.-S.; Blom, J.; van den Akker, M.; Röttger, K.; Wegwarth, O.; et al. Health-Related Preferences of Older Patients with Multimorbidity: An Evidence Map. BMJ Open 2019, 9, e034485. [Google Scholar] [CrossRef]
- Bragge, P.; Clavisi, O.; Turner, T.; Tavender, E.; Collie, A.; Gruen, R.L. The Global Evidence Mapping Initiative: Scoping Research in Broad Topic Areas. BMC Med. Res. Methodol. 2011, 11, 92. [Google Scholar] [CrossRef]
- Haddaway, N.R.; Bernes, C.; Jonsson, B.-G.; Hedlund, K. The Benefits of Systematic Mapping to Evidence-Based Environmental Management. Ambio 2016, 45, 613–620. [Google Scholar] [CrossRef]
- Miake-Lye, I.M.; Hempel, S.; Shanman, R.; Shekelle, P.G. What Is an Evidence Map? A Systematic Review of Published Evidence Maps and Their Definitions, Methods, and Products. Syst. Rev. 2016, 5, 28. [Google Scholar] [CrossRef]
- Tricco, A.C.; Lillie, E.; Zarin, W.; O’Brien, K.K.; Colquhoun, H.; Levac, D.; Moher, D.; Peters, M.D.J.; Horsley, T.; Weeks, L.; et al. PRISMA Extension for Scoping Reviews (PRISMA-ScR): Checklist and Explanation. Ann. Intern. Med. 2018, 169, 467–473. [Google Scholar] [CrossRef]
- Department of Health and Social Care. National Framework for NHS Continuing Healthcare and NHS-Funded Nursing Care; Department of Health and Social Care: London, UK, 2022; Volume 187. [Google Scholar]
- Omole, F.S.; Sow, C.M.; Fresh, E.; Babalola, D.; Strothers, H. Interacting with Patients’ Family Members during the Office Visit. Am. Fam. Physician 2011, 84, 780–784. [Google Scholar]
- Ouzzani, M.; Hammady, H.; Fedorowicz, Z.; Elmagarmid, A. Rayyan—A Web and Mobile App for Systematic Reviews. Available online: https://www.rayyan.ai/ (accessed on 30 June 2022).
- Morgan, D.L. Qualitative Content Analysis: A Guide to Paths Not Taken. Qual. Health Res. 1993, 3, 112–121. [Google Scholar] [CrossRef]
- Elo, S.; Kyngäs, H. The Qualitative Content Analysis Process. J. Adv. Nurs. 2008, 62, 107–115. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 Statement: An Updated Guideline for Reporting Systematic Reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Kerkhoff, A.D.; Sachdev, D.; Mizany, S.; Rojas, S.; Gandhi, M.; Peng, J.; Black, D.; Jones, D.; Rojas, S.; Jacobo, J.; et al. Evaluation of a Novel Community-Based COVID-19 “Test-to-Care” Model for Low-Income Populations. PLoS ONE 2020, 15, e0239400. [Google Scholar] [CrossRef]
- Cao, J.; Wei, J.; Zhu, H.; Duan, Y.; Geng, W.; Hong, X.; Jiang, J.; Zhao, X.; Zhu, B. A Study of Basic Needs and Psychological Wellbeing of Medical Workers in the Fever Clinic of a Tertiary General Hospital in Beijing during the COVID-19 Outbreak. Psychother. Psychosom. 2020, 89, 252–254. [Google Scholar] [CrossRef]
- Digby, R.; Winton-Brown, T.; Finlayson, F.; Dobson, H.; Bucknall, T. Hospital Staff Well-Being during the First Wave of COVID-19: Staff Perspectives. Int. J. Ment. Health Nurs. 2021, 30, 440–450. [Google Scholar] [CrossRef]
- Elhadi, M.; Msherghi, A.; Elgzairi, M.; Alhashimi, A.; Bouhuwaish, A.; Biala, M.; Abuelmeda, S.; Khel, S.; Khaled, A.; Alsoufi, A.; et al. Burnout Syndrome among Hospital Healthcare Workers during the COVID-19 Pandemic and Civil War: A Cross-Sectional Study. Front. Psychiatry 2020, 11, 579563. [Google Scholar] [CrossRef]
- Feinstein, R.E.; Kotara, S.; Jones, B.; Shanor, D.; Nemeroff, C.B. A Health Care Workers Mental Health Crisis Line in the Age of COVID-19. Depress. Anxiety 2020, 37, 822–826. [Google Scholar] [CrossRef] [PubMed]
- González-Gil, M.T.; González-Blázquez, C.; Parro-Moreno, A.I.; Pedraz-Marcos, A.; Palmar-Santos, A.; Otero-García, L.; Navarta-Sánchez, M.V.; Alcolea-Cosín, M.T.; Argüello-López, M.T.; Canalejas-Pérez, C.; et al. Nurses’ Perceptions and Demands Regarding COVID-19 Care Delivery in Critical Care Units and Hospital Emergency Services. Intensive Crit. Care Nurs. 2021, 62, 102966. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.; Venugopal, V.; Latha, P.K.; Alhadad, S.B.; Leow, C.H.W.; de Goh, N.Y.; Tan, E.; Kjellstrom, T.; Morabito, M.; Lee, J.K.W. Heat Stress and Thermal Perception amongst Healthcare Workers during the COVID-19 Pandemic in India and Singapore. Int. J. Environ. Res. Public Health 2020, 17, 8100. [Google Scholar] [CrossRef]
- Kackin, O.; Ciydem, E.; Aci, O.S.; Kutlu, F.Y. Experiences and Psychosocial Problems of Nurses Caring for Patients Diagnosed with COVID-19 in Turkey: A Qualitative Study. Int. J. Soc. Psychiatry 2021, 67, 158–167. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Wang, C.; Pan, W.; Zheng, J.; Gao, J.; Huang, X.; Cai, S.; Zhai, Y.; Latour, J.M.; Zhu, C. Stress, Burnout, and Coping Strategies of Frontline Nurses during the COVID-19 Epidemic in Wuhan and Shanghai, China. Front. Psychiatry 2020, 11, 1154. [Google Scholar] [CrossRef]
- Raza, A.; Matloob, S.; Rahim, N.F.A.; Halim, H.A.; Khattak, A.; Ahmed, N.H.; Nayab, D.-E.; Hakeem, A.; Zubair, M. Factors Impeding Health-Care Professionals to Effectively Treat Coronavirus Disease 2019 Patients in Pakistan: A Qualitative Investigation. Front. Psychol. 2020, 11, 572450. [Google Scholar] [CrossRef]
- Ripp, J.; Peccoralo, L.; Charney, D. Attending to the Emotional Well-Being of the Health Care Workforce in a New York City Health System during the COVID-19 Pandemic. Acad. Med. 2020, 95, 1136–1139. [Google Scholar] [CrossRef]
- Shanafelt, T.; Ripp, J.; Trockel, M. Understanding and Addressing Sources of Anxiety among Health Care Professionals during the COVID-19 Pandemic. JAMA J. Am. Med. Assoc. 2020, 323, 2133–2134. [Google Scholar] [CrossRef]
- Halcomb, E.; Williams, A.; Ashley, C.; McInnes, S.; Stephen, C.; Calma, K.; James, S. The Support Needs of Australian Primary Health Care Nurses during the COVID-19 Pandemic. J. Nurs. Manag. 2020, 28, 1553–1560. [Google Scholar] [CrossRef]
- Kabir, Z.N.; Boström, A.-M.; Konradsen, H. In Conversation with a Frontline Worker in a Care Home in Sweden during the COVID-19 Pandemic. J. Cross-Cult. Gerontol. 2020, 35, 493–500. [Google Scholar] [CrossRef]
- Stojanov, J.; Malobabic, M.; Stanojevic, G.; Stevic, M.; Milosevic, V.; Stojanov, A. Quality of Sleep and Health-Related Quality of Life among Health Care Professionals Treating Patients with Coronavirus Disease-19. Int. J. Soc. Psychiatry 2021, 67, 175–181. [Google Scholar] [CrossRef]
- Martin-Delgado, J.; Viteri, E.; Mula, A.; Serpa, P.; Pacheco, G.; Prada, D.; de Andrade Lourenção, D.C.; Baptista, P.C.P.; Ramirez, G.; Mira, J.J. Availability of Personal Protective Equipment and Diagnostic and Treatment Facilities for Healthcare Workers Involved in COVID-19 Care: A Cross-Sectional Study in Brazil, Colombia, and Ecuador. PLoS ONE 2020, 15, e0242185. [Google Scholar] [CrossRef]
- Yong, L.M.O.; Xin, X.; Wee, J.M.L.; Poopalalingam, R.; Kwek, K.Y.C.; Thumboo, J. Perception Survey of Crisis and Emergency Risk Communication in an Acute Hospital in the Management of COVID-19 Pandemic in Singapore. BMC Public Health 2020, 20, 1919. [Google Scholar] [CrossRef]
- Sethi, B.A.; Sethi, A.; Ali, S.; Aamir, H.S. Impact of Coronavirus Disease (COVID-19) Pandemic on Health Professionals. Pak. J. Med. Sci. 2020, 36, S6. [Google Scholar] [CrossRef]
- Adesoye, T.; Davis, C.H.; Del Calvo, H.; Shaikh, A.F.; Chegireddy, V.; Chan, E.Y.; Martinez, S.; Pei, K.Y.; Zheng, F.; Tariq, N. Optimization of Surgical Resident Safety and Education during the COVID-19 Pandemic—Lessons Learned. J. Surg. Educ. 2021, 78, 315–320. [Google Scholar] [CrossRef]
- Ashiru-Oredope, D.; Chan, A.H.Y.; Olaoye, O.; Rutter, V.; Babar, Z.-U.-D.; Anderson, C.; Anderson, R.; Halai, M.; Matuluko, A.; Nambatya, W.; et al. Needs Assessment and Impact of COVID-19 on Pharmacy Professionals in 31 Commonwealth Countries. J. Pharm. Policy Pract. 2020, 13, 72. [Google Scholar] [CrossRef]
- Glatman-Freedman, A.; Bromberg, M.; Ram, A.; Lutski, M.; Bassal, R.; Michailevich, O.; Saban, M.; Frankental, D.; Dichtiar, R.; Kruglikov-Moldavsky, A.; et al. A COVID-19 Call Center for Healthcare Providers: Dealing with Rapidly Evolving Health Policy Guidelines. Isr. J. Health Policy Res. 2020, 9, 73. [Google Scholar] [CrossRef]
- Cipolotti, L.; Chan, E.; Murphy, P.; van Harskamp, N.; Foley, J.A. Factors Contributing to the Distress, Concerns, and Needs of UK Neuroscience Health Care Workers during the COVID-19 Pandemic. Psychol. Psychother. Theory Res. Pract. 2021, 94, 536–543. [Google Scholar] [CrossRef]
- Mattila, E.; Peltokoski, J.; Neva, M.H.; Kaunonen, M.; Helminen, M.; Parkkila, A.K. COVID-19: Anxiety among Hospital Staff and Associated Factors. Ann. Med. 2021, 53, 237–246. [Google Scholar] [CrossRef] [PubMed]
- Redondo-Sama, G.; Matulic, V.; Munté-Pascual, A.; de Vicente, I. Social Work during the COVID-19 Crisis: Responding to Urgent Social Needs. Sustainability 2020, 12, 8595. [Google Scholar] [CrossRef]
- Yu, J.C.; McIntyre, M.; Dow, H.; Robinson, L.; Winston, P. Changes to Rehabilitation Service Delivery and the Associated Physician Perspectives during the COVID-19 Pandemic: A Mixed-Methods Needs Assessment Study. Am. J. Phys. Med. Rehabil. 2020, 99, 775–782. [Google Scholar] [CrossRef] [PubMed]
- Yu, E.Y.T.; Leung, W.L.H.; Wong, S.Y.S.; Liu, K.S.N.; Wan, E.Y.F. How Are Family Doctors Serving the Hong Kong Community during the COVID-19 Outbreak? A Survey of Hkcfp Members. Hong Kong Med. J. 2020, 26, 176–183. [Google Scholar] [CrossRef] [PubMed]
- Mohindra, R.; Ravaki, R.; Suri, V.; Bhalla, A.; Singh, S.M. Issues Relevant to Mental Health Promotion in Frontline Health Care Providers Managing Quarantined/Isolated COVID19 Patients. Asian J. Psychiatry 2020, 51, 102084. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, E.; Owens, C.T.; Daniels, T.; Boyle, J.; Robinson, R.F. Pharmacists’ Willingness to Provide Coronavirus Disease (COVID-19) Services and the Needs to Support COVID-19 Testing, Management, and Prevention. J. Community Health 2021, 46, 752–757. [Google Scholar] [CrossRef] [PubMed]
- Kaplan, L.J.; Kleinpell, R.; Maves, R.C.; Doersam, J.K.; Raman, R.; Ferraro, D.M. Critical Care Clinician Reports on Coronavirus Disease 2019: Results From a National Survey of 4875 ICU Providers. Crit. Care Explor. 2020, 2, e0125. [Google Scholar] [CrossRef]
- Vanhaecht, K.; Seys, D.; Bruyneel, L.; Cox, B.; Kaesemans, G.; Cloet, M.; van den Broeck, K.; Cools, O.; De Witte, A.; Lowet, K.; et al. COVID-19 Is Having a Destructive Impact on Health-Care Workers’ Mental Well-Being. Int. J. Qual. Health Care 2021, 33, mzaa158. [Google Scholar] [CrossRef]
- Du, J.; Mayer, G.; Hummel, S.; Oetjen, N.; Gronewold, N.; Zafar, A.; Schultz, J.-H. Mental Health Burden in Different Professions during the Final Stage of the COVID-19 Lockdown in China: Cross-Sectional Survey Study. J. Med. Internet Res. 2020, 22, e24240. [Google Scholar] [CrossRef]
- Wang, Z. Use the Environment to Prevent and Control COVID-19 in Senior-Living Facilities: An Analysis of the Guidelines Used in China. Health Environ. Res. Des. J. 2021, 14, 130–140. [Google Scholar] [CrossRef]
- Simione, L.; Gnagnarella, C. Differences Between Health Workers and General Population in Risk Perception, Behaviors, and Psychological Distress Related to COVID-19 Spread in Italy. Front. Psychol. 2020, 11, 2166. [Google Scholar] [CrossRef]
- Dorociak, K.E.; Rupert, P.A.; Bryant, F.B.; Zahniser, E. Development of a Self-Care Assessment for Psychologists. J. Couns. Psychol. 2017, 64, 325–334. [Google Scholar] [CrossRef]
- Danet, A.D. Psychological Impact of COVID-19 Pandemic in Western Frontline Healthcare Professionals. A Systematic Review. Med. Clínica 2021, 156, 449–458. [Google Scholar] [CrossRef]
- García-Iglesias, J.J.; Gómez-Salgado, J.; Martín-Pereira, J.; Fagundo-Rivera, J.; Ayuso-Murillo, D.; Martínez-Riera, J.R.; Ruiz-Frutos, C. Impact of SARS-CoV-2 (COVID-19) on the mental health of healthcare professionals: A systematic review. Rev. Esp. Salud. Publica 2020, 94, e202007088. [Google Scholar]
- Abdulla, E.K.; Velladath, S.U.; Varghese, A.; Anju, M. Depression and Anxiety Associated with COVID-19 Pandemic among Healthcare Professionals in India—A Systematic Review and Meta-Analysis. Clin. Epidemiol. Glob. Health 2021, 12, 100888. [Google Scholar] [CrossRef]
- Fiabane, E.; Gabanelli, P.; La Rovere, M.T.; Tremoli, E.; Pistarini, C.; Gorini, A. Psychological and Work-Related Factors Associated with Emotional Exhaustion among Healthcare Professionals during the COVID-19 Outbreak in Italian Hospitals. Nurs. Health Sci. 2021, 23, 670–675. [Google Scholar] [CrossRef]
- Muller, A.E.; Hafstad, E.V.; Himmels, J.P.W.; Smedslund, G.; Flottorp, S.; Stensland, S.Ø.; Stroobants, S.; Van de Velde, S.; Vist, G.E. The Mental Health Impact of the COVID-19 Pandemic on Healthcare Workers, and Interventions to Help Them: A Rapid Systematic Review. Psychiatry Res. 2020, 293, 113441. [Google Scholar] [CrossRef]
- Yıldırım, M.; Arslan, G.; Özaslan, A. Perceived Risk and Mental Health Problems among Healthcare Professionals during COVID-19 Pandemic: Exploring the Mediating Effects of Resilience and Coronavirus Fear. Int. J. Ment. Health Addict. 2022, 20, 1035–1045. [Google Scholar] [CrossRef]
- Ayton, D.; Soh, S.-E.; Berkovic, D.; Parker, C.; Yu, K.; Honeyman, D.; Manocha, R.; MacIntyre, R.; Ananda-Rajah, M. Experiences of Personal Protective Equipment by Australian Healthcare Workers during the COVID-19 Pandemic, 2020: A Cross-Sectional Study. PLoS ONE 2022, 17, e0269484. [Google Scholar] [CrossRef]
- Effective Patient–Physician Communication. Available online: https://www.acog.org/en/clinical/clinical-guidance/committee-opinion/articles/2014/02/effective-patient-physician-communication (accessed on 30 June 2022).
- Dong, F.; Liu, H.-L.; Dai, N.; Yang, M.; Liu, J.-P. A Living Systematic Review of the Psychological Problems in People Suffering from COVID-19. J. Affect. Disord. 2021, 292, 172–188. [Google Scholar] [CrossRef] [PubMed]
- Zhang, H.; Xie, F.; Yang, B.; Zhao, F.; Wang, C.; Chen, X. Psychological Experience of COVID-19 Patients: A Systematic Review and Qualitative Meta-Synthesis. Am. J. Infect. Control. 2022, 50, 809–819. [Google Scholar] [CrossRef]
- Shah, R.; Ali, F.M.; Nixon, S.J.; Ingram, J.R.; Salek, S.M.; Finlay, A.Y. Measuring the Impact of COVID-19 on the Quality of Life of the Survivors, Partners and Family Members: A Cross-Sectional International Online Survey. BMJ Open 2021, 11, e047680. [Google Scholar] [CrossRef] [PubMed]
- Kentish-Barnes, N.; Cohen-Solal, Z.; Morin, L.; Souppart, V.; Pochard, F.; Azoulay, E. Lived Experiences of Family Members of Patients with Severe COVID-19 Who Died in Intensive Care Units in France. JAMA Netw. Open 2021, 4, e2113355. [Google Scholar] [CrossRef] [PubMed]
- Chua, A.Q.; Tan, M.M.J.; Verma, M.; Han, E.K.L.; Hsu, L.Y.; Cook, A.R.; Teo, Y.Y.; Lee, V.J.; Legido-Quigley, H. Health System Resilience in Managing the COVID-19 Pandemic: Lessons from Singapore. BMJ Glob. Health 2020, 5, e003317. [Google Scholar] [CrossRef] [PubMed]
- Haegdorens, F.; Franck, E.; Smith, P.; Bruyneel, A.; Monsieurs, K.G.; Van Bogaert, P. Sufficient Personal Protective Equipment Training Can Reduce COVID-19 Related Symptoms in Healthcare Workers: A Prospective Cohort Study. Int. J. Nurs. Stud. 2022, 126, 104132. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Inclusion Criteria | Exclusion Criteria |
|---|---|
| Primary qualitative and/or quantitative work addressing any healthcare-related needs associated with COVID-19 from the perspective of adult patients, their relatives, and the professionals involved in their care. |
|
| Variable | n (%) | |
|---|---|---|
| Type of publication | ||
| Original research | 28 (78%) | |
| Brief report | 3 (8%) | |
| Perspective | 2 (6%) | |
| Letter to the editor/commentary | 2 (6%) | |
| Review | 1 (3%) | |
| Geographical location | ||
| Asia | 12 (33%) | |
| Europe | 10 (28%) | |
| North America | 8 (22%) | |
| Multi-country | 3 (8%) | |
| Australia | 2 (6%) | |
| Africa | 1 (3%) | |
| Healthcare setting | ||
| Hospitals | 16 (44%) | |
| Multiple settings | 14 (39%) | |
| Elderly residential care | 2 (6%) | |
| Primary care | 2 (6%) | |
| Community-based | 1 (3%) | |
| Unspecified | 1 (3%) | |
| Study design | ||
| Quantitative | 14 (39%) | |
| Qualitative | 14 (39%) | |
| Mixed | 8 (22%) | |
| Needs identified by | ||
| Professionals | 35 (97%) | |
| Patients | 1 (3%) | |
| Professionals | Patients | Family Members | Transversal Needs | |
|---|---|---|---|---|
| Total No. of Studies | 35/36 (97%) | 13/36 (36%) | 13/36 (36%) | 16/36 (44%) |
| Evidence clusters | Basic needs (n = 16) Occupational needs (n = 34) Psycho-socio-emotional needs (n = 28) | Basic needs (n = 2) Healthcare needs (n = 11) Psycho-socio-emotional needs (n = 9) Other support needs (n = 8) | Psycho-socio-emotional needs (n = 8) Communication needs (n = 7) | Public safety needs (n = 9) Information and communication needs (n = 16) Other needs: Coordination and support (n = 6) |
| Most frequently reported needs | General or other psychological health resources or support (n = 25) Adequate supply of appropriate personal protective equipment (n = 22) Other information, resources, and procedures to reduce risk of acquiring COVID-19 (n = 24) | Access to emotional support (n = 5) Family communication and social interaction (n = 6) Access to mental health professionals (n = 6) Access to social support (including social welfare and childcare) (n = 5) | Communication and social interaction between family and patients or residents (n = 5) Access to psycho-emotional support (n = 5) | General education and awareness campaigns (n = 11) Clarifying fake news and misinformation (n = 6) Reducing social stigma (n= 6) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Aparicio Betancourt, M.; Duarte-Díaz, A.; Vall-Roqué, H.; Seils, L.; Orrego, C.; Perestelo-Pérez, L.; Barrio-Cortes, J.; Beca-Martínez, M.T.; Molina Serrano, A.; Bermejo-Caja, C.J.; et al. Global Healthcare Needs Related to COVID-19: An Evidence Map of the First Year of the Pandemic. Int. J. Environ. Res. Public Health 2022, 19, 10332. https://doi.org/10.3390/ijerph191610332
Aparicio Betancourt M, Duarte-Díaz A, Vall-Roqué H, Seils L, Orrego C, Perestelo-Pérez L, Barrio-Cortes J, Beca-Martínez MT, Molina Serrano A, Bermejo-Caja CJ, et al. Global Healthcare Needs Related to COVID-19: An Evidence Map of the First Year of the Pandemic. International Journal of Environmental Research and Public Health. 2022; 19(16):10332. https://doi.org/10.3390/ijerph191610332
Chicago/Turabian StyleAparicio Betancourt, Mariana, Andrea Duarte-Díaz, Helena Vall-Roqué, Laura Seils, Carola Orrego, Lilisbeth Perestelo-Pérez, Jaime Barrio-Cortes, María Teresa Beca-Martínez, Almudena Molina Serrano, Carlos Jesús Bermejo-Caja, and et al. 2022. "Global Healthcare Needs Related to COVID-19: An Evidence Map of the First Year of the Pandemic" International Journal of Environmental Research and Public Health 19, no. 16: 10332. https://doi.org/10.3390/ijerph191610332