Article Text

Abstract
Objectives Using the National Child Mortality Database (NCMD), this work aims to investigate and quantify the characteristics of children dying of COVID-19, and to identify any changes in rate of childhood mortality during the pandemic.
Design We compared the characteristics of the children who died in 2020, split by SARS-CoV-2 status. A negative binomial regression model was used to compare mortality rates in lockdown (23 March–28 June), with those children who died in the preceding period (6 January–22 March), as well as a comparable period in 2019.
Setting England.
Participants Children (0–17 years).
Main outcome measures Characteristics and number of the children who died in 2020, split by SARS-CoV-2 status.
Results 1550 deaths of children between 6th of January and 28 June 2020 were notified to the NCMD; 437 of the deaths were linked to SARS-CoV-2 virology records, 25 (5.7%) had a positive PCR result. PCR-positive children were less likely to be white (37.5% vs 69.4%, p=0.003) and were older (12.2 vs 0.7 years, p<0.0006) compared with child deaths without evidence of the virus. All-cause mortality rates were similar during lockdown compared with both the period before lockdown in 2020 (rate ratio (RR) 0.93 (0.84 to 1.02)) and a similar period in 2019 (RR 1.02 (0.92 to 1.13)).
Conclusions There is little to suggest that there has been excess mortality during the period of lockdown. The apparent higher frequency of SARS-CoV-2-positive tests among children from black, Asian and minority ethnic groups is consistent with findings in adults. Ongoing surveillance is essential as the pandemic continues.
- mortality
- epidemiology
- Covid-19
Data availability statement
Data may be obtained from a third party and are not publicly available. Aggregate data may be available on request to the corresponding author, and subject to approval by HQIP.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
What is already known on this topic?
Childhood SARS-CoV-2 disease may present in a variable way, often without clear respiratory symptoms, and so in many cases ascertainment is difficult.
There are concerns of a hidden impact of SARS-CoV-2 on the health of newborns, infants and children.
The relationship of COVID-19 disease and common chronic diseases of childhood, such as asthma, age and ethnic group, remains unclear.
What this study adds?
Child mortality was lower in 2020 than in 2019 with little to suggest that there has been an excess mortality among children during the period of lockdown.
Children who died and had a positive result for SARS-CoV-2 were more likely to be older and from ethnic minority groups.
We found little to suggest an over-representation of children with underlying health conditions.
Background
The COVID-19 pandemic is one of the biggest global challenges faced in our lifetime. In England, by 30 June, over 244 336 people had tested positive for COVID-19, and over 39 962 COVID-19-related deaths had been identified.1 While publications report little evidence for a significant excess mortality in children in the initial stages of the lockdown,2 there remain concerns of a hidden impact on the health of newborns, infants and children,3–5 with reports of adverse pregnancy outcomes,6 7 dramatic reductions in emergency hospital contacts,8 delayed presentation of serious illness,9 and increases in child maltreatment,10 malnutrition,11 and mental health problems.12–14
Despite the unprecedented research efforts arising from the pandemic, few data have been published on the overall direct and indirect disease impact on child mortality. Standard national mortality registration does not have complete ascertainment in real time, meaning that the key question of ‘excess mortality’ will be difficult to assess for some time to come.15 To compound this, much of the current literature is based on case series or inpatient data. Initial data suggested that SARS-CoV-2 infection causes a similar disease in children to that seen in adults,16 but as the pandemic has progressed, novel presentations of hyperinflammatory states,5 17 abdominal symptoms and neurological pathology have been described.3 In addition, while we are aware of specific underlying disease states which appear to put adults at greater risk of severe disease,18 the relationship of COVID-19 disease and common chronic diseases of childhood, such as asthma, is unclear. SARS-CoV-2 may also have direct effects on the risk of perinatal events, although the exact impact is not known. Increased rates of preterm birth and perinatal asphyxia have been reported by some,19 while others report lower rates20; as well as recent reports of possible increases in stillbirth rates.6
Rapid population-based analyses during a pandemic are therefore essential to provide unbiased information on incidence and outcomes. The National Child Mortality Database (NCMD) was established in 2019, with the core aim to study and analyse the patterns, causes and associated risk factors of child mortality in England. Notification is required by statute within 48 hours.
Aims
The two primary aims of these analyses are to:
Identify the number and characteristics of children dying of COVID-19 in England during the first wave of the pandemic.
Identify changes in rate of overall childhood mortality during the lockdown period, compared with the pre-lockdown period in 2020, and a comparable (pre-pandemic) period in 2019.
Methodology
The NCMD commenced data collection on 1 April 2019 and collects data from all 58 Child Death Overview Panels (CDOPs) across England.21 There is a legal responsibility for CDOPs to notify NCMD of every death of anyone before their 18th birthday, including cases referred to the coroner for further investigation.22 From 1 March 2020, linkage with virology PCR results was performed with Public Health England (PHE) for the retrospective and prospective surveillance of COVID-19 child mortality in England and, for practical and workload reasons at the time, was limited to deaths where COVID-19 was a possible cause (ie, not trauma or suicide deaths). In April 2020, the Joint Agency Response to child deaths during the COVID-19 pandemic protocol was amended to include postmortem viral swabs from all children dying suddenly and unexpectedly from no immediately identifiable cause (sudden unexpected death in infancy or childhood, SUDIC).23
Coding of notifications
All deaths reported to the NCMD were coded by four independent coders (three paediatricians and one NCMD manager with CDOP expertise) to identify the most likely category of the cause of death, using a classification system based on that used by the child death review process since 2008.22 All coders reviewed the deaths blind to each other and recorded if the death was likely to be due to malignancy, preterm birth, intrapartum events, infection, trauma, substance misuse, suicide, an underlying medical condition, or if the event should be considered a SUDIC; or that there was insufficient information provided (see online supplemental appendix). To identify the most important factor contributing to the death, the most common category identified by the four coders was used as the most likely category. Where more than one category was identified, the category highest in the following hierarchy was used (based on categorisation used by CDOPs).24
Supplemental material
Suicide.
Substance abuse.
Trauma.
Malignancy.
Underlying medical condition.
Intrapartum event.
Preterm birth.
Infection.
SUDIC.
In addition to the information included in the summary narrative, data were provided or derived from the structured questions in the notification form:
Sex of individual (female, male, other (including not known)).
Ethnic group (Asian or Asian British, black or black British, mixed, other, unknown, white).
Age at death.
Deprivation tenths of the child’s home address using the deciles from the Index of Multiple Deprivation (IMD).25 A lower value suggests greater deprivation.
During lockdown, possible concerns were raised for deaths by suicide, SUDIC or intrapartum events. Consequently, where one or more coders recorded death by one of these categories, they were asked to review their classification. For suicide and intrapartum deaths, additional clarification and validation was sought.
Suicide: additional details were sought from the notifying CDOP. Where there remained disagreement, cases were reviewed by a researcher with expertise in suicide research (DG) blind to the date of death and coded as suicides if the likelihood was considered ‘high’ or ‘moderate’.26
Intrapartum deaths: electronic (BadgerNet) discharge summaries for all babies who had died in a neonatal intensive care unit were obtained. Where there remained disagreement about the likely cause of death, cases were recoded by one independent neonatologist blind to the date of death (PC).
Statistical analysis
The analysis is based on deaths on, or before 28 June 2020. To ensure adequate time for notification, coding and clarification, data were downloaded and finalised 19 days later, on 17 July 2020. To investigate the profile of children dying with evidence of SARS-CoV-2, we compared the characteristics of the children with known SARS-CoV-2 PCR testing; split by those with a positive or negative result. Comparisons were made using Fisher’s exact test for categorical data and Mann-Whitney U test for age and the IMD deprivation category.
Initially, we quantified the number of deaths that were reported to the NCMD and graphed the output (smoothing using the arithmetic means up to 7 days either side of point estimate). UK-wide restrictions to reduce the impact of the pandemic started on 23 March 2020. To investigate the characteristics of the deaths during the lockdown period (as infection rates rose, but also with widespread changes to social distancing, healthcare and education), we compared the sociodemographic characteristics of the children who died during lockdown, with those children who died in the period immediately before (23 March–28 June 2020 compared with 6 January–22 March 2020). In a second comparison, to adjust for seasonal changes, we then compared deaths during a slightly different period of the lockdown (30 March–28 June 2020) with a comparable period in pre-pandemic 2019 (1 April–30 June 2019) as we did not have data before the start of NCMD in 2019. Data were collapsed to provide frequency counts of events per day. The incidence of events during lockdown was compared with the rate in 2020 before lockdown using a negative binomial regression model to derive a rate ratio (RR) (and 95% CI) for the comparison. An estimate of the population under 18 years old (n=12 023 568) was based on the Office for National Statistics (ONS) 2019 estimates.27 The analysis was repeated comparing deaths during lockdown with those in 2019 and split by the age of the child at their death (birth–27 days, 28 days–1 year, 1–4 years, 5–9 years, 10–14 years, 15–17 years).
Sensitivity analyses
Policy and guidance changed during the lockdown period with two distinct periods: before, and, on or after, 17 May 2020, when lockdown restrictions were eased. For the pre-lockdown comparison, the regression model was repeated, estimating the RR for the two periods of lockdown compared with deaths in the pre-lockdown period. For the comparison with lockdown versus 2019 pre-pandemic, the regression model was repeated allowing any association between year and the outcome to be modified by the period of lockdown; and separate RRs derived for the two periods. Models were compared with the main analysis to test (using the likelihood ratio test) if there was evidence that they fitted the data more precisely.
As exploratory analyses, the main analysis was repeated for the children who died in each provisional category of death (above) to give an indication of profile of causes of child mortality during lockdown.
Data were compared with provisional ONS data to ascertain data coverage. ONS mortality statistics are based on information recorded when deaths are certified and registered; and while most deaths are registered within 5 days, there are circumstances when there may be a substantial delay in issuing a Medical Certificate of Cause of Death, such as deaths reported to a coroner. The total number of child deaths registered by ONS from 11 January to 26 June 2020 for England, by age groups and week of death, was compared with NCMD data for the same period. Due to the fast-changing COVID-19 pandemic in England, prior to publication, the analysis was repeated with the most recent total deaths. In this analysis, using the same methodology as above, we compared the number of deaths reported to the NCMD between 1 April 2020 and 31 December 2020 with the number in the same period of 2019.
Data are presented as median (IQR), number (%) or RR (95% CI). Where frequency counts were below 5, or could be derived, absolute numbers were not presented. Analysis was performed using Stata V.14. Data were analysed on 21 July 2020.
Role of funding source
National Health Service England funded the rapid set-up of the real-time surveillance system and staff time to support its function, but had no input into the data analysis or interpretation.
Results
Between Monday 6 January and Friday 28 June (175 days), a total of 1550 deaths of children were notified to the NCMD (as of 17 July 2020). From 1 March 2020, 968 requests for SARS-CoV-2 PCR results were requested from PHE on the previously agreed criteria (above); 412 children had at least one negative result identified, 25 had a positive result recorded at some point and for 531 no test was performed. Children who died with positive SARS-CoV-2 virology were less likely to be recorded as having white ethnicity (37.5% vs 69.4%, p=0.003) and were older (12.2 vs 0.7 years, p<0.0006) when compared with those who died with negative virology (table 1).
Characteristics of all deaths between 6 January and 28 June 2020 split by COVID-19 status
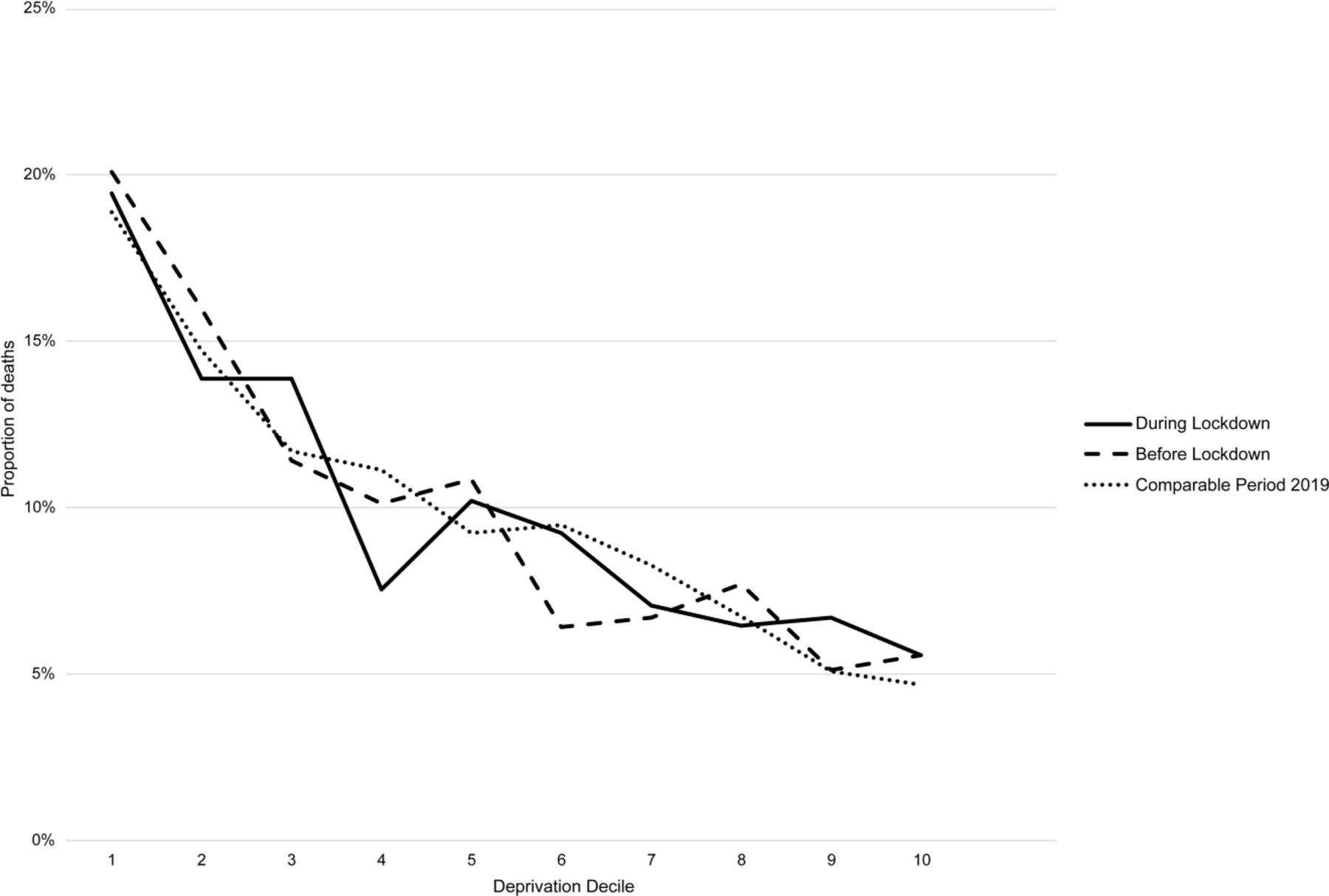
A total of 711 deaths occurred in the 77 days before the first 2020 national lockdown, compared with 839 deaths during lockdown (98 days) (figure 1). Children who died during lockdown had similar ages (table 2 and figure 2), sex, ethnicity, deprivation measures (figure 3) and locations as those dying pre-lockdown. However, during lockdown, fewer deaths occurred in hospital (73.8% vs 79.2%, p=0.016). A total of 756 deaths occurred in the comparable period in 2019, compared with 771 during lockdown (both covering the 91 days); and had similar ages, sex, ethnicity, deprivation measures and locations as those during lockdown. Overall rates of death were similar during lockdown compared with the 2020 period before lockdown (RR 0.93 (0.84 to 1.02)) and during lockdown compared with 2019 (RR 1.02 (0.92 to 1.13) (table 3)).
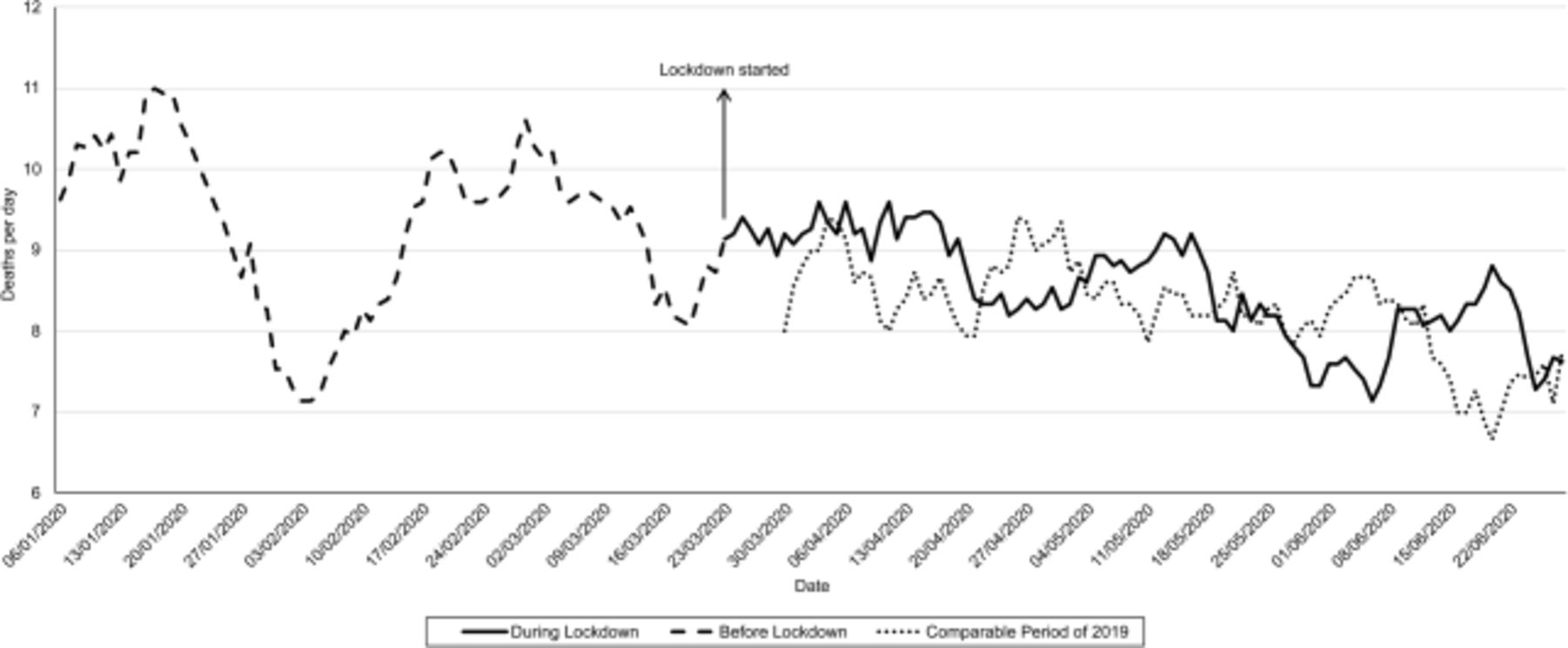
Mean number of deaths per day (15 days smoother average) split by time period. *Lockdown started 23 March 2020. 2019 comparison data from 1 April 2019 onwards.
Characteristics of deaths in the lockdown period, compared with before lockdown and a comparable period in 2019
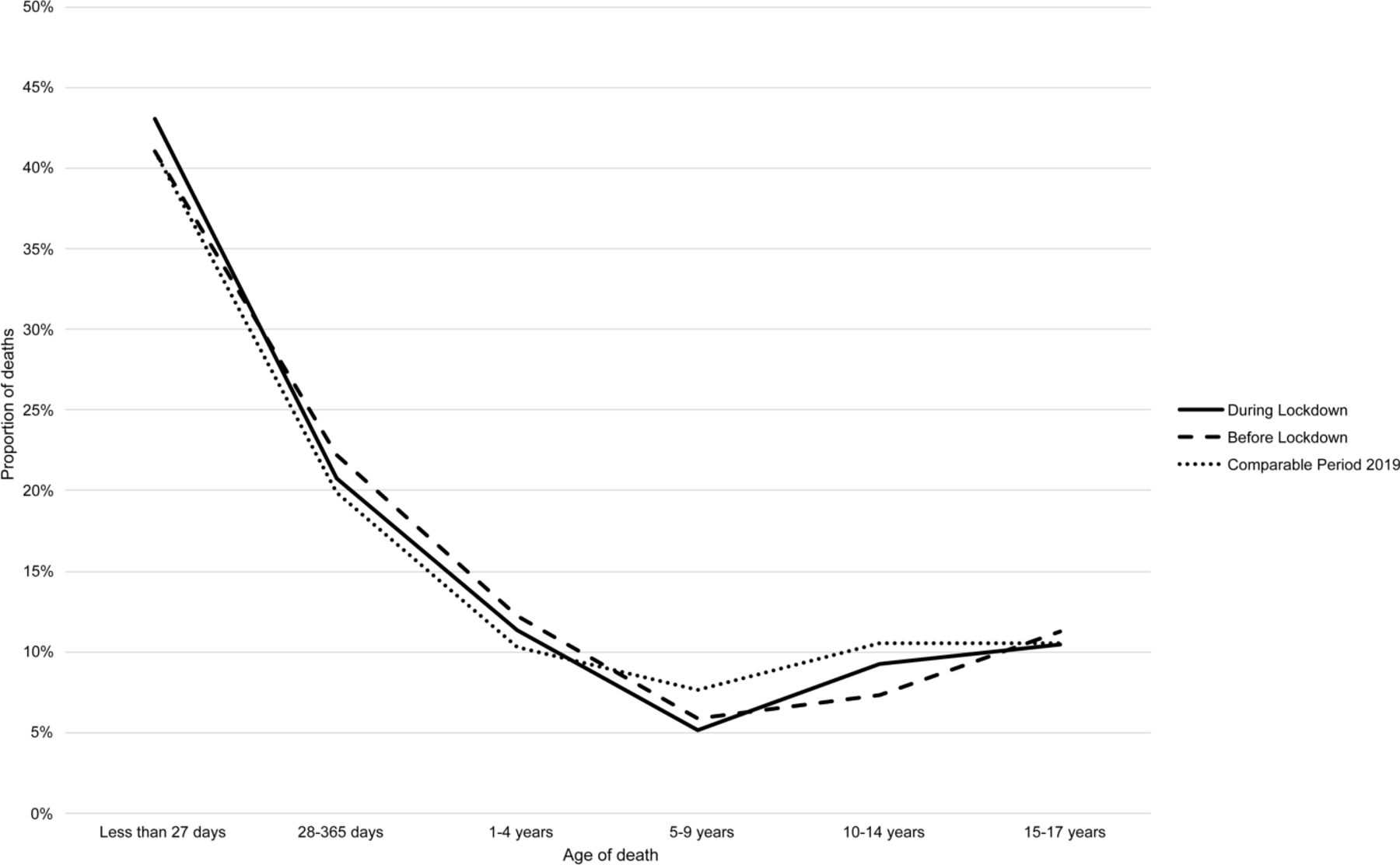
Age of death, split by time period.
{kind=link}
{kind=link}
{kind=link}
Deprivation measure (1–10) at death, split by time period.
Characteristics of deaths in the lockdown period, compared with before lockdown and a comparable period in 2019
Sensitivity analyses
There was little evidence that the incidence of death was different in the two periods of lockdown when compared with before lockdown (p=0.141) or pre-pandemic in 2019 (p=0.773) (table 3).
When looking at the number of deaths split by the likely cause, over the whole lockdown period in comparison with the 2020 pre-lockdown and 2019 pre-pandemic periods, children had similar mortality rates after preterm birth or from malignancy, infection, trauma, substance misuse, suicide and sudden unexpected deaths (table 4). There was however some weak evidence that there was a higher rate of death after intrapartum events (RR 1.46 (0.97 to 2.20)), and stronger evidence that the risk of dying of an underlying condition was also reduced (RR 0.79 (0.65 to 0.97)) when compared with the pre-pandemic period of 2019; although wider, but compatible, CIs when comparing with the earlier pre-lockdown period of 2020 (RR 1.27 (0.84 to 1.94) and RR 0.85 (0.70 to 1.04), respectively).
Characteristics of deaths, by likely category, in the lockdown period, compared with before lockdown and a comparable period in 2019
Between 11 January 2020 and 26 June 2020, provisional ONS data reported 1152 deaths of children under 18 years occurring in England, compared with 1492 deaths notified to the NCMD (29.5% more). Between 1 April 2019 and 31 December 2019, there were a total of 2498 childhood deaths reported to the NCMD; compared with a total of 2264 in the same period of 2020 (RR 0.92 (0.87 to 0.98), p=0.009).
Discussion
Overall child mortality was lower in 2020 than in 2019 although older children and those from black, Asian and minority ethnic (BAME) groups were more likely to have a SARS-CoV-2-positive test, consistent with other work.5 7 28
As with any routine data analysis, there are limitations to our analyses and interpretations. Child deaths in England remain rare, however the precision of the point estimate of overall mortality suggests that it is very unlikely that there has been a substantial change. The biggest limitation is likely to be that of missing data and case ascertainment, as, despite the rapid notification system, some late notifications may be missing. However, numbers reported in the NCMD are statutory and likely to miss only a handful of cases.14 The indications for testing for SARS-CoV-2 are complex and are influenced by clinical suspicion, availability of tests and local policy. It is possible that some children with complex disease (or underlying illness) were not tested as the death was expected or out of hospital. In addition, cause of death is based on limited notification data prior to completion of the full child death review process and so the categories presented should be interpreted with caution as they are based on limited information and some are likely to change when a fuller investigation is performed.21 Finally, we did not have complete data on some other measures (eg, ethnicity) so some degree of reporting bias is possible.
While the overall prevalence of child deaths with a positive SARS-CoV-2 antigen test in England is higher than estimated by others,5 15 many of the positive tests were performed in cases without recognised symptoms of COVID-19, so direct COVID-19 mortality cannot be assumed. In addition, many children were not tested for SARS-CoV-2. In total 1.6% of children dying during the lockdown period we examined were known to be SARS-CoV-2 positive around the time of their death, while a small additional number presented with one of the recognised syndromes associated with SARS-CoV-2 (eg, paediatric inflammatory multisystem syndrome temporally associated with SARS-CoV-2) but with a negative PCR. However, in contrast to emerging data on the mortality seen in adults,29 this national analysis demonstrates no measurable excess mortality in children under 18 years, consistent with other work reporting on an earlier epoch of the UK lockdown.2 We did see an increased risk of a positive COVID-19 test in older children; and in those from BAME backgrounds, consistent with other work.5 7 28 However, in contrast to adult data, we did not see a higher prevalence of underlying medical conditions in those children who died with evidence of SARS-CoV-2 infection, or a measurable impact of sex on mortality.30 Indeed, there is some evidence in this work that dying from an underlying medical condition was less frequent during the second period of lockdown than a comparable period in 2019. This may be due to the unique nature of SARS-CoV-2 in younger children, or that social distancing and shielding was effective in this group. Indeed, overall child mortality between April and December 2020 is 8% lower than the corresponding period in 2019 and further work is needed to identify the reasons for this. Finally, concerns have been raised that social disruption caused by the lockdown (eg, overcrowded accommodation or those experiencing financial insecurity) might lead to increased unexpected infant deaths or increased deaths from child abuse. Our findings with the data collected thus far do not support these concerns. Children with a positive SARS-CoV-2 test had similar deprivation measures to those with a negative test.
Conclusions
In this analysis of child mortality in England, during the first phase of the pandemic, there is little to suggest that there has been excess mortality during the period of lockdown in England. The apparent higher frequency of children from BAME groups testing positive for SARS-CoV-2 is consistent with analyses in adults, and further work will be needed to clarify the impact as the pandemic continues. Changes in delivery of healthcare may affect chronic conditions many months later, and the economic impacts on socioeconomically disadvantaged children may take time to become apparent. Ongoing surveillance of the overall rates of child death and the likely causes and contributory factors is essential as the pandemic continues, to provide rapid support for policymakers and information for the public and professionals.
Data availability statement
Data may be obtained from a third party and are not publicly available. Aggregate data may be available on request to the corresponding author, and subject to approval by HQIP.
Ethics statements
Patient consent for publication
Ethics approval
The NCMD legal basis to collect confidential and personal level data under the Common Law Duty of Confidentiality has been established through the Children Act 2004 Sections M - N, Working Together to Safeguard Children 2018 (https://consult.education.gov.uk/child-protection-safeguarding-and-family-law/working-together-to-safeguard-children-revisions-t/supporting_documents/Working_Together_to_Safeguard_Children.pdf) and associated Child Death Review Statutory & Operational Guidance https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/859302/child-death-review-statutory-and-operational-guidance-england.pdf). The NCMD legal basis to collect personal data under the General Data Protection Regulation (GDPR) without consent is defined by GDPR Article 6 (e) Public task and 9 (h) Health or social care (with a basis in law).
Acknowledgments
We thank all Child Death Overview Panels (CDOPs) who submitted data for the purposes of this report and all child death review professionals for submitting data and providing additional information when requested. Parent and public involvement is at the heart of the NCMD programme. We are indebted to Charlotte Bevan (Sands—Stillbirth and Neonatal Death Charity), Therese McAlorum (Child Bereavement UK) and Jenny Ward (Lullaby Trust), who represent bereaved families on the NCMD programme steering group, for their advice and support with setting up the real-time child mortality surveillance system at the beginning of the COVID-19 pandemic. We also would like to thank the independent expert for coding suicides: Professor David Gunnell (University of Bristol) and independent expert for coding deaths due to intrapartum events: Dr Pamela Cairns (University Hospitals Bristol and Weston NHS Foundation Trust); and Professor Chris Metcalfe (University of Bristol) for his statistical advice. We thank Dr Yvonne Silove (HQIP) for expert advice around data governance and data sharing for the linkage work. We are also indebted to the following: Public Health England’s Field Service and National Child and Maternal Health Intelligence Network teams, for their collaboration in establishing the real-time surveillance system on child deaths potentially related to COVID-19 and ongoing support in the daily linkage with the SARS-CoV-2 test results; the Office for National Statistics for providing the provisional civil registration data; QES for rapidly developing and deploying the COVID-19 module as part of the NCMD child death notification system; and CleverMed for their assistance in providing timely neonatal discharge summary data from BadgerNet to support the real-time child mortality surveillance system. Lastly, we thank the NCMD team for their technical and administrative support.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @KarenLuyt
Contributors DO participated in the study concept and design; contributed to acquisition, analysis and interpretation of data, and drafting and reviewing the manuscript; and approved the final version. SS participated in the study design; contributed to data acquisition, linkage, analysis and interpretation of analysis, and drafting and reviewing the manuscript; and approved the final version. TW participated in the study design; contributed to data acquisition, linkage, analysis and interpretation of data analyses, and reviewing the manuscript; and approved the final version. VS participated in the study design; contributed to acquisition and interpretation of data, and drafting and reviewing the manuscript; and approved the final version. PB participated in the study design; contributed to interpretation of data analysis and reviewing the manuscript; and approved the final version. PF participated in the study concept and design; contributed to acquisition and interpretation of data analysis, and reviewing the manuscript; and approved the final version. IW contributed to study design, interpretation of data analysis, and reviewing the manuscript; and approved the final version. KL obtained funding for this work; participated in the study concept and design; contributed to data acquisition and interpretation of data, and drafting and reviewing the manuscript; and approved the final version.
Funding The National Child Mortality Database (NCMD) Programme, including this work, is funded by NHS England and commissioned by the Healthcare Quality Improvement Partnership (HQIP) as part of the National Clinical Audit and Patient Outcomes Programme (NCAPOP).
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.