More than Pneumonia: Distinctive Features of SARS-Cov-2 Infection. From Autopsy Findings to Clinical Implications: A Systematic Review

 , ,
, ,  , ,
, , 

Abstract
:1. Introduction
2. Materials and Methods
2.1. Eligibility Criteria
2.2. Search Criteria and Critical Appraisal
3. Results
3.1. Search Results and Included Studies
3.2. Study Characteristics
3.3. Risk of Bias
3.4. Full Autopsy and Safety Protocol
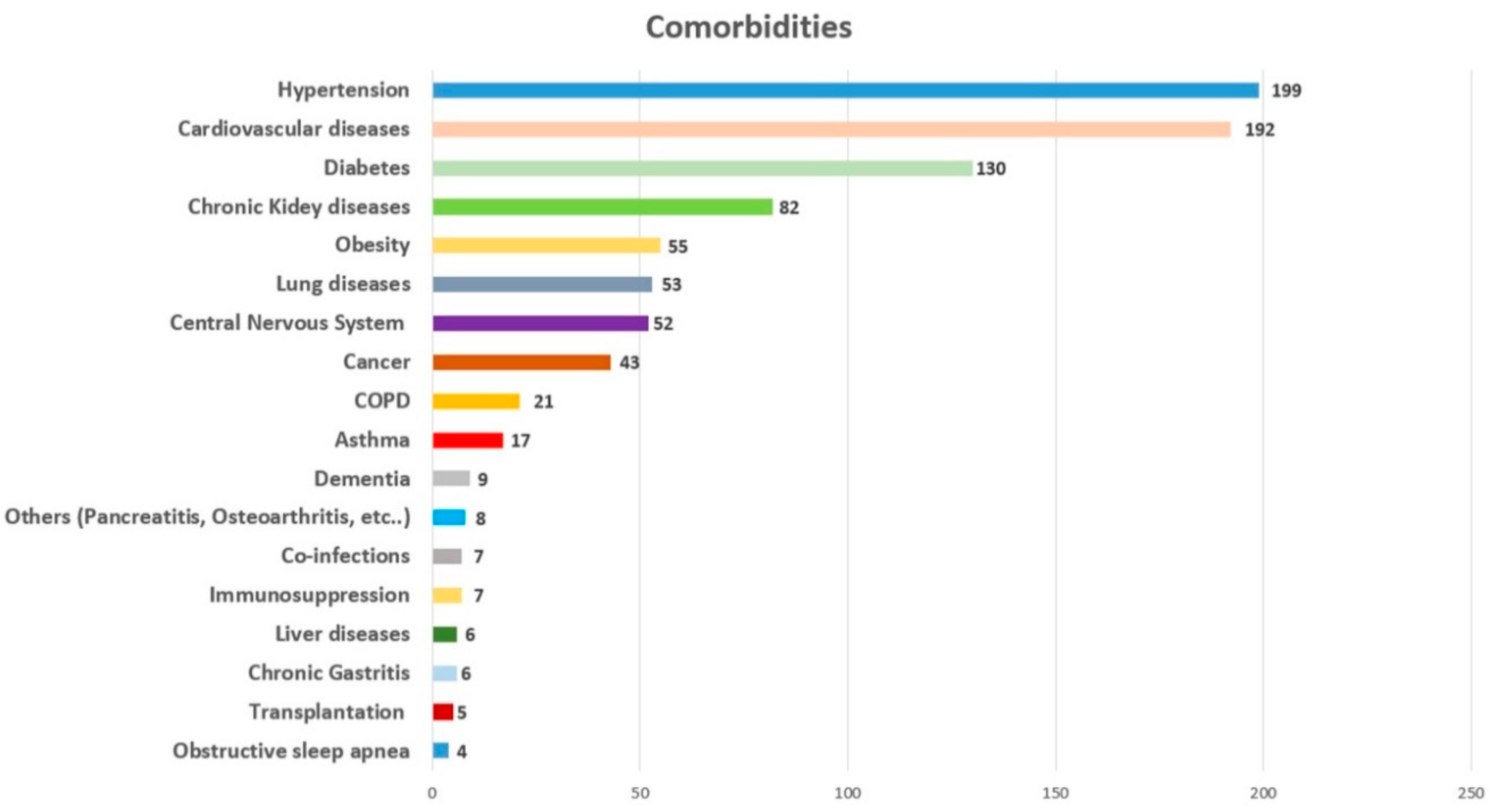
3.5. Comorbidities
3.6. Post-Mortem Investigations
3.7. Lungs
3.8. Heart
3.9. Kidneys
3.10. Central Nervous System (CNS)
3.11. Other Organs
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Pomara, C.; Volti, G.L.; Cappello, F. COVID-19 Deaths: Are We Sure It Is Pneumonia? Please, Autopsy, Autopsy, Autopsy! J. Clin. Med. 2020, 9, 1259. [Google Scholar] [CrossRef] [PubMed]
- Centers for Disease Control and Prevention Collection and Submission of Postmortem Specimens from Deceased Persons with Known or Suspected COVID-19. Available online: https://eaaf.org/wp-content/uploads/covid19-PDFs/EEUU/CDC-guidance-postmortem-specimens.pdf (accessed on 18 August 2020).
- Osborn, M.; Lucas, S.B.; Stewart, R.; Swift, B.; Youd, E. Autopsy Practice Relating to Possible Cases of COVID-19 (2019-nCov, Novel Coronavirus from China 2019/2020). Available online: https://www.rcpath.org/uploads/assets/d5e28baf-5789-4b0f-acecfe370eee6223/447e37d0-29dd-4994-a11fe27b93de0905/Briefing-on-COVID-19-autopsy-Feb-2020.pdf (accessed on 18 August 2020).
- Basso, C.; Calabrese, F.; Sbaraglia, M.; Del Vecchio, C.; Carretta, G.; Saieva, A.; Donato, D.; Flor, L.; Crisanti, A.; Tos, A.P.D. Feasibility of postmortem examination in the era of COVID-19 pandemic: The experience of a Northeast Italy University Hospital. Virchows Arch. 2020, 477, 341–347. [Google Scholar] [CrossRef]
- Fineschi, V.; Aprile, A.; Aquila, I.; Arcangeli, M.; Asmundo, A.; Bacci, M.; Cingolani, M.; Cipolloni, L.; D’Errico, S.; de Casamassimi, I.; et al. Management of the corpse with suspect, probable or confirmed COVID-19 respiratory infection—Italian interim recommendations for personnel potentially exposed to material from corpses, including body fluids, in morgue structures, during autopsy practice. Pathol. J. Ital. Soc. Anat. Pathol. Diagn. Cytopathol. 2020, 112, 64–77. [Google Scholar]
- Santurro, A.; Scopetti, M.; D’Errico, S.; Fineschi, V. A technical report from the Italian SARS-CoV-2 outbreak. Postmortem sampling and autopsy investigation in cases of suspected or probable COVID-19. Forensic Sci. Med. Pathol. 2020, 16, 471–476. [Google Scholar] [CrossRef]
- Hanley, B.; Lucas, S.B.; Youd, E.; Swift, B.; Osborn, M. Autopsy in suspected COVID-19 cases. J. Clin. Pathol. 2020, 73, 239–242. [Google Scholar] [CrossRef] [Green Version]
- Sapino, A.; Facchetti, F.; Bonoldi, E.; Gianatti, A.; Barbareschi, M. The autopsy debate during the COVID-19 emergency: The Italian experience. Virchows Arch. 2020, 476, 821–823. [Google Scholar] [CrossRef] [PubMed]
- Keten, D.; Okdemir, E.; Keten, A. Precautions in postmortem examinations in Covid-19 - Related deaths: Recommendations from Germany. J. Forensic Leg. Med. 2020, 73, 102000. [Google Scholar] [CrossRef] [PubMed]
- Edler, C.; Schröder, A.S.; Aepfelbacher, M.; Fitzek, A.; Heinemann, A.; Heinrich, F.; Klein, A.; Langenwalder, F.; Lütgehetmann, M.; Meißner, K.; et al. Dying with SARS-CoV-2 infection—An autopsy study of the first consecutive 80 cases in Hamburg, Germany. Int. J. Legal Med. 2020, 134, 1275–1284. [Google Scholar] [CrossRef] [PubMed]
- Buja, L.M.; Wolf, D.; Zhao, B.; Akkanti, B.; McDonald, M.; Lelenwa, L.; Reilly, N.; Ottaviani, G.; Elghetany, M.T.; Trujillo, D.O.; et al. The emerging spectrum of cardiopulmonary pathology of the coronavirus disease 2019 (COVID-19): Report of 3 autopsies from Houston, Texas, and review of autopsy findings from other United States cities. Cardiovasc. Pathol. 2020, 48, 107233. [Google Scholar] [CrossRef] [PubMed]
- Salerno, M.; Sessa, F.; Piscopo, A.; Montana, A.; Torrisi, M.; Patanè, F.; Murabito, P.; Li Volti, G.; Pomara, C. No Autopsies on COVID-19 Deaths: A Missed Opportunity and the Lockdown of Science. J. Clin. Med. 2020, 9, 1472. [Google Scholar] [CrossRef]
- Pomara, C.; Li Volti, G.; Cappello, F. The post-lockdown era: What is next in Italy? Front. Pharmacol. 2020, 11, 1074. [Google Scholar] [CrossRef]
- Tzankov, A.; Jonigk, D. Unlocking the lockdown of science and demystifying COVID-19: How autopsies contribute to our understanding of a deadly pandemic. Virchows Arch. 2020, 477, 331–333. [Google Scholar] [CrossRef]
- Barth, R.F.; Xu, X.; Buja, L.M. A Call to Action: The Need for Autopsies to Determine the Full Extent of Organ Involvement Associated With COVID-19. Chest 2020, 158, 43–44. [Google Scholar] [CrossRef] [PubMed]
- Püschel, K.; Sperhake, J.P. Corona deaths in Hamburg, Germany. Int. J. Legal Med. 2020, 134, 1267–1269. [Google Scholar] [CrossRef] [PubMed]
- Stroup, D.F.; Berlin, J.A.; Morton, S.C.; Olkin, I.; Williamson, G.D.; Rennie, D.; Moher, D.; Becker, B.J.; Sipe, T.A.; Thacker, S.B. Meta-analysis of observational studies in epidemiology: A proposal for reporting. J. Am. Med. Assoc. 2000, 283, 2008–2012. [Google Scholar] [CrossRef] [PubMed]
- Carsana, L.; Sonzogni, A.; Nasr, A.; Rossi, R.S.; Pellegrinelli, A.; Zerbi, P.; Rech, R.; Colombo, R.; Antinori, S.; Corbellino, M.; et al. Pulmonary post-mortem findings in a series of COVID-19 cases from northern Italy: A two-centre descriptive study. Lancet Infect. Dis. 2020, 20, 1135–1140. [Google Scholar] [CrossRef]
- Bryce, C.; Grimes, Z.; Pujadas, E.; Ahuja, S.; Beasley, M.B.; Albrecht, R.; Hernandez, T.; Stock, A.; Zhao, Z.; Al Rasheed, M.; et al. Pathophysiology of SARS-CoV-2: Targeting of endothelial cells renders a complex disease with thrombotic microangiopathy and aberrant immune response. The Mount Sinai COVID-19 autopsy experience. medRxiv 2020. [Google Scholar] [CrossRef]
- Bradley, B.T.; Maioli, H.; Johnston, R.; Chaudhry, I.; Fink, S.L.; Xu, H.; Najafian, B.; Deutsch, G.; Lacy, J.M.; Williams, T.; et al. Histopathology and ultrastructural findings of fatal COVID-19 infections in Washington State: A case series. Lancet 2020, 396, 320–332. [Google Scholar] [CrossRef]
- Giacca, M.; Bussani, R.; Schneider, E.; Zentilin, L.; Collesi, C.; Ali, H.; Braga, L.; Secco, I.; Volpe, M.C.; Colliva, A.; et al. Persistence of viral RNA, widespread thrombosis and abnormal cellular syncytia are hallmarks of COVID-19 lung pathology. medRxiv 2020. [Google Scholar] [CrossRef]
- Copin, M.C.; Parmentier, E.; Duburcq, T.; Poissy, J.; Mathieu, D.; The Lille COVID-19 ICU and Anatomopathology Group. Time to consider histologic pattern of lung injury to treat critically ill patients with COVID-19 infection. Intensive Care Med. 2020, 46, 1124–1126. [Google Scholar] [CrossRef] [Green Version]
- Duarte-Neto, A.N.; de Almeida Monteiro, R.A.; da Silva, L.F.F.; Malheiros, D.M.A.C.; de Oliveira, E.P.; Theodoro Filho, J.; Pinho, J.R.R.; Soares Gomes-Gouvêa, M.; Salles, A.P.M.; de Oliveira, I.R.S.; et al. Pulmonary and systemic involvement of COVID-19 assessed by ultrasound-guided minimally invasive autopsy. Histopathology 2020. [Google Scholar] [CrossRef] [PubMed]
- Menter, T.; Haslbauer, J.D.; Nienhold, R.; Savic, S.; Hopfer, H.; Deigendesch, N.; Frank, S.; Turek, D.; Willi, N.; Pargger, H.; et al. Post-mortem examination of COVID19 patients reveals diffuse alveolar damage with severe capillary congestion and variegated findings of lungs and other organs suggesting vascular dysfunction. Histopathology 2020, 77, 198–209. [Google Scholar] [CrossRef]
- Xu, X.; Chang, X.N.; Pan, H.X.; Su, H.; Huang, B.; Yang, M.; Luo, D.J.; Weng, M.X.; Ma, L.; Nie, X. Pathological changes of the spleen in ten patients with coronavirus disease 2019(COVID-19) by postmortem needle autopsy. Zhonghua Bing Li Xue Za Zhi Chin. J. Pathol. 2020, 49, 576–582. [Google Scholar]
- Yan, L.; Mir, M.; Sanchez, P.; Beg, M.; Peters, J.; Enriquez, O.; Gilbert, A. Autopsy Report with Clinical Pathological Correlation. Arch. Pathol. Lab. Med. 2020. [Google Scholar]
- Dell’Aquila, M.; Cattani, P.; Fantoni, M.; Marchetti, S.; Aquila, I.; Stigliano, E.; Carbone, A.; Oliva, A.; Arena, V. Postmortem swabs in the Sars-CoV-2 Pandemic: Report on 12 complete clinical autopsy cases. Arch. Pathol. Lab. Med. 2020. [Google Scholar] [CrossRef]
- Bösmüller, H.; Traxler, S.; Bitzer, M.; Häberle, H.; Raiser, W.; Nann, D.; Frauenfeld, L.; Vogelsberg, A.; Klingel, K.; Fend, F. The evolution of pulmonary pathology in fatal COVID-19 disease: An autopsy study with clinical correlation. Virchows Arch. 2020, 477, 349–357. [Google Scholar] [CrossRef] [PubMed]
- Conde, P.N.; Monraval, P.A.; Medina, C.M.; Sánchez, A.J.; Teruel, J.C.; Marco, J.F.; Santos, V.P.; Aranda, E.M. Mayordomo Aranda, E. Autopsy findings from the first known death from Severe Acute Respiratory Syndrome SARS-CoV-2 in Spain. Rev. Esp. Patol. 2020, 53, 188–192. [Google Scholar]
- Casagrande, M.; Fitzek, A.; Püschel, K.; Aleshcheva, G.; Schultheiss, H.P.; Berneking, L.; Spitzer, M.S.; Schultheiss, M. Detection of SARS-CoV-2 in Human Retinal Biopsies of Deceased COVID-19 Patients. Ocul. Immunol. Inflamm. 2020. [Google Scholar] [CrossRef]
- Löffler, K.U.; Reinhold, A.; Herwig-Carl, M.C.; Tzankov, A.; Holz, F.G.; Scholl, H.P.N.; Meyer, P. Ocular post-mortem findings in patients having died from COVID-19. Ophthalmologe 2020, 117, 648–651. [Google Scholar] [CrossRef]
- Liu, Q.; Wang, R.S.; Qu, G.Q. Gross Examination Report of a COVID-19 Death Autopsy. J. Forensic Med. 2020, 36, 21. [Google Scholar]
- Ackermann, M.; Verleden, S.E.; Kuehnel, M.; Haverich, A.; Welte, T.; Laenger, F.; Vanstapel, A.; Werlein, C.; Stark, H.; Tzankov, A.; et al. Pulmonary Vascular Endothelialitis, Thrombosis, and Angiogenesis in Covid-19. N. Engl. J. Med. 2020, 383, 120–128. [Google Scholar] [CrossRef] [PubMed]
- Aguiar, D.; Lobrinus, J.A.; Schibler, M.; Fracasso, T.; Lardi, C. Inside the lungs of COVID-19 disease. Int. J. Legal Med. 2020, 1–4. [Google Scholar] [CrossRef]
- Barton, L.M.; Duval, E.J.; Stroberg, E.; Ghosh, S.; Mukhopadhyay, S. COVID-19 Autopsies, Oklahoma, USA. Am. J. Clin. Pathol. 2020, 153, 725–733. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cipolloni, L.; Sessa, F.; Bertozzi, G.; Baldari, B.; Cantatore, S.; Testi, R.; D’Errico, S.; Di Mizio, G.; Asmundo, A.; Castorina, S.; et al. Preliminary Post-Mortem COVID-19 Evidence of Endothelial Injury and Factor VIII Hyperexpression. Diagnostics 2020, 10, 575. [Google Scholar] [CrossRef] [PubMed]
- Farkash, E.A.; Wilson, A.M.; Jentzen, J.M. Ultrastructural Evidence for Direct Renal Infection with SARS-CoV-2. J. Am. Soc. Nephrol. 2020, 31, 1683–1687. [Google Scholar] [CrossRef]
- Fox, S.E.; Akmatbekov, A.; Harbert, J.L.; Li, G.; Brown, J.Q.; Vander Heide, R.S. Pulmonary and cardiac pathology in African American patients with COVID-19: An autopsy series from New Orleans. Lancet Respir. Med. 2020, 8, 681–686. [Google Scholar] [CrossRef]
- Grosse, C.; Grosse, A.; Salzer, H.; Dünser, M.; Motz, R.; Langer, R. Analysis of cardiopulmonary findings in COVID-19 fatalities: High incidence of pulmonary artery thrombi and acute suppurative bronchopneumonia. Cardiovasc. Pathol. 2020, 49, 107263. [Google Scholar] [CrossRef] [PubMed]
- Iuga, A.C.; Marboe, C.C.; Yilmaz, M.M.; Lefkowitch, J.H.; Gauran, C.; Lagana, S.M. Adrenal Vascular Changes in COVID-19 Autopsies. Arch. Pathol. Lab. Med. 2020, 144, 1159–1160. [Google Scholar] [CrossRef]
- Konopka, K.E.; Wilson, A.; Myers, J.L. Postmortem Lung Findings in an Asthmatic Patient With Coronavirus Disease 2019. Ann Oncol 2020, 158, e99–e101. [Google Scholar]
- Lacy, J.M.; Brooks, E.G.; Akers, J.; Armstrong, D.; Decker, L.; Gonzalez, A.; Humphrey, W.; Mayer, R.; Miller, M.; Perez, C.; et al. COVID-19: POSTMORTEM DIAGNOSTIC AND BIOSAFETY CONSIDERATIONS. Am. J. Forensic Med. Pathol. 2020. [Google Scholar] [CrossRef]
- Lax, S.F.; Skok, K.; Zechner, P.; Kessler, H.H.; Kaufmann, N.; Koelblinger, C.; Vander, K.; Bargfrieder, U.; Trauner, M. Pulmonary Arterial Thrombosis in COVID-19 With Fatal Outcome: Results From a Prospective, Single-Center, Clinicopathologic Case Series. Ann. Intern. Med. 2020, 173, 350–361. [Google Scholar] [CrossRef] [PubMed]
- Okudela, K. CASE REPORT A Japanese case of COVID-19: An autopsy report. Pathol. Int. 2020, 2, 1–5. [Google Scholar]
- Paniz-Mondolfi, A.; Bryce, C.; Grimes, Z.; Gordon, R.E.; Reidy, J.; Lednicky, J.; Sordillo, E.M.; Fowkes, M. Central nervous system involvement by severe acute respiratory syndrome coronavirus-2 (SARS-CoV-2). J. Med. Virol. 2020, 92, 699–702. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Reichard, R.R.; Kashani, K.B.; Boire, N.A.; Constantopoulos, E.; Guo, Y.; Lucchinetti, C.F. Neuropathology of COVID-19: A spectrum of vascular and acute disseminated encephalomyelitis (ADEM)-like pathology. Acta Neuropathol. 2020, 140, 1–6. [Google Scholar] [CrossRef]
- Remmelink, M.; De Mendoca, R.; D’Haene, N.; De Clercq, S.; Verocq, C.; Lebrun, L.; Lavis, P.; Racu, M.L.; Trepant, A.L.; Maris, C.; et al. Unspecific post-mortem findings despite multiorgan 1 viral spread in COVID-19 patients. medRxiv 2020. [Google Scholar] [CrossRef]
- Santoriello, D.; Khairallah, P.; Bomback, A.S.; Xu, K.; Kudose, S.; Batal, I.; Barasch, J.; Radhakrishnan, J.; D’Agati, V.; Markowitz, G. Postmortem Kidney Pathology Findings in Patients with COVID-19. J. Am. Soc. Nephrol. 2020, 31, 2158–2167. [Google Scholar] [CrossRef]
- Schaller, T.; Hirschbühl, K.; Burkhardt, K.; Braun, G.; Trepel, M.; Märkl, B.; Claus, R. Postmortem Examination of Patients with COVID-19. JAMA 2020, 323, 2518–2520. [Google Scholar] [CrossRef] [PubMed]
- Su, H.; Yang, M.; Wan, C.; Yi, L.X.; Tang, F.; Zhu, H.Y.; Yi, F.; Yang, H.C.; Fogo, A.B.; Nie, X.; et al. Renal histopathological analysis of 26 postmortem findings of patients with COVID-19 in China. Kidney Int. 2020, 98, 219–227. [Google Scholar] [CrossRef]
- Suess, C.; Hausmann, R. Gross and histopathological pulmonary findings in a COVID-19 associated death during self-isolation. Int. J. Legal Med. 2020. [Google Scholar] [CrossRef] [PubMed]
- Tombolini, A.; Scendoni, R. SARS-CoV-2-related deaths in routine forensic autopsy practice: Histopathological patterns. Int. J. Legal Med. 2020. [Google Scholar] [CrossRef]
- Varga, Z.; Flammer, A.J.; Steiger, P.; Haberecker, M.; Andermatt, R.; Zinkernagel, A.S.; Mehra, M.R.; Schuepbach, R.A.; Ruschitzka, F.; Moch, H. Endothelial cell infection and endotheliitis in COVID-19. Lancet 2020, 395, 1417–1418. [Google Scholar] [CrossRef]
- Wang, C.; Xie, J.; Zhao, L.; Fei, X.; Zhang, H.; Tan, Y.; Nie, X.; Zhou, L.; Liu, Z.; Ren, Y.; et al. Alveolar macrophage dysfunction and cytokine storm in the pathogenesis of two severe COVID-19 patients. EBioMedicine 2020, 57, 102833. [Google Scholar] [CrossRef] [PubMed]
- Wichmann, D.; Sperhake, J.-P.; Lütgehetmann, M.; Steurer, S.; Edler, C.; Heinemann, A.; Heinrich, F.; Mushumba, H.; Kniep, I.; Schröder, A.S.; et al. Autopsy Findings and Venous Thromboembolism in Patients With COVID-19. Ann. Intern. Med. 2020, 173, 268–277. [Google Scholar] [CrossRef] [PubMed]
- Youd, E.; Moore, L. COVID-19 autopsy in people who died in community settings: The first series. J. Clin. Pathol. 2020. [Google Scholar] [CrossRef] [PubMed]
- Rapkiewicz, A.V.; Mai, X.; Carsons, S.E.; Pittaluga, S.; Kleiner, D.E.; Berger, J.S.; Thomas, S.; Adler, N.M.; Charytan, D.M.; Gasmi, B.; et al. Megakaryocytes and platelet-fibrin thrombi characterize multi-organ thrombosis at autopsy in COVID-19: A case series. EClinicalMedicine 2020, 24, 100434. [Google Scholar] [CrossRef]
- Martines, R.B.; Ritter, J.M.; Matkovic, E.; Gary, J.; Bollweg, B.C.; Bullock, H.; Goldsmith, C.S.; Silva-Flannery, L.; Seixas, J.N.; Reagan-Steiner, S.; et al. Pathology and Pathogenesis of SARS-CoV-2 Associated with Fatal Coronavirus Disease, United States. Emerg. Infect. Dis. 2020, 26, 2005. [Google Scholar] [CrossRef]
- Barnes, B.J.; Adrover, J.M.; Baxter-Stoltzfus, A.; Borczuk, A.; Cools-Lartigue, J.; Crawford, J.M.; Daßler-Plenker, J.; Guerci, P.; Huynh, C.; Knight, J.S.; et al. Targeting potential drivers of COVID-19: Neutrophil extracellular traps. J. Exp. Med. 2020, 217, e20200652. [Google Scholar] [CrossRef]
- Li, R.; Yin, K.; Zhang, K.; Wang, Y.Y.; Wu, Q.P.; Tang, S.B.; Cheng, J.D. Application Prospects of Virtual Autopsy in Forensic Pathological Investigations on COVID-19. Fa Yi Xue Za Zhi 2020, 36. [Google Scholar] [CrossRef]
- Calabrese, F.; Pezzuto, F.; Fortarezza, F.; Hofman, P.; Kern, I.; Panizo, A.; von der Thüsen, J.; Timofeev, S.; Gorkiewicz, G.; Lunardi, F. Pulmonary pathology and COVID-19: Lessons from autopsy. The experience of European Pulmonary Pathologists. Virchows Arch. 2020, 477, 359–372. [Google Scholar] [CrossRef]
- Lindner, D.; Fitzek, A.; Bräuninger, H.; Aleshcheva, G.; Edler, C.; Meissner, K.; Scherschel, K.; Kirchhof, P.; Escher, F.; Schultheiss, H.-P.; et al. Association of Cardiac Infection With SARS-CoV-2 in Confirmed COVID-19 Autopsy Cases. JAMA Cardiol. 2020. [Google Scholar] [CrossRef]
- Bafunno, V.; Bury, L.; Tiscia, G.L.; Fierro, T.; Favuzzi, G.; Caliandro, R.; Sessa, F.; Grandone, E.; Margaglione, M.; Gresele, P. A novel congenital dysprothrombinemia leading to defective prothrombin maturation. Thromb. Res. 2014, 134, 1135–1141. [Google Scholar] [CrossRef] [PubMed]
- Santacroce, R.; Santoro, R.; Sessa, F.; Iannaccaro, P.; Sarno, M.; Longo, V.; Gallone, A.; Vecchione, G.; Muleo, G.; Margaglione, M. Screening of mutations of hemophilia A in 40 Italian patients: A novel G-to-A mutation in intron 10 of the F8 gene as a putative cause of mild hemophilia a in southern Italy. Blood Coagul. Fibrinolysis 2008, 19, 197–202. [Google Scholar] [CrossRef] [PubMed]
- Sessa, F.; Bertozzi, G.; Cipolloni, L.; Baldari, B.; Cantatore, S.; D’Errico, S.; Di Mizio, G.; Asmundo, A.; Castorina, S.; Salerno, M.; et al. Clinical-Forensic Autopsy Findings to Defeat COVID-19 Disease: A Literature Review. J. Clin. Med. 2020, 9, 2026. [Google Scholar] [CrossRef] [PubMed]
- Angileri, F.; Legare, S.; Marino Gammazza, A.; Conway de Macario, E.; JL Macario, A.; Cappello, F. Molecular mimicry may explain multi-organ damage in COVID-19. Autoimmun. Rev. 2020, 19, 102591. [Google Scholar] [CrossRef]
- Huang, S.; Wang, J.; Liu, F.; Liu, J.; Cao, G.; Yang, C.; Liu, W.; Tu, C.; Zhu, M.; Xiong, B. COVID-19 patients with hypertension have more severe disease: A multicenter retrospective observational study. Hypertens. Res. 2020, 43, 824–831. [Google Scholar] [CrossRef]
- Ma, L.; Song, K.; Huang, Y. Coronavirus Disease-2019 (COVID-19) and Cardiovascular Complications. J. Cardiothorac. Vasc. Anesth. 2020. [Google Scholar] [CrossRef]
- Rubino, F.; Amiel, S.A.; Zimmet, P.; Alberti, G.; Bornstein, S.; Eckel, R.H.; Mingrone, G.; Boehm, B.; Cooper, M.E.; Chai, Z.; et al. New-Onset Diabetes in Covid-19. N. Engl. J. Med. 2020, 383, 789–790. [Google Scholar] [CrossRef]
- Henry, B.M.; Lippi, G. Chronic kidney disease is associated with severe coronavirus disease 2019 (COVID-19) infection. Int. Urol. Nephrol. 2020, 52, 1193–1194. [Google Scholar] [CrossRef] [Green Version]
- Middeldorp, S.; Coppens, M.; van Haaps, T.F.; Foppen, M.; Vlaar, A.P.; Müller, M.C.A.; Bouman, C.C.S.; Beenen, L.F.M.; Kootte, R.S.; Heijmans, J.; et al. Incidence of venous thromboembolism in hospitalized patients with COVID-19. J. Thromb. Haemost. 2020, 18, 1995–2002. [Google Scholar] [CrossRef]
- Zamboni, P. COVID-19 as a Vascular Disease: Lesson Learned from Imaging and Blood Biomarkers. Diagnostics 2020, 10, 440. [Google Scholar] [CrossRef]
- Letko, M.; Marzi, A.; Munster, V. Functional assessment of cell entry and receptor usage for SARS-CoV-2 and other lineage B betacoronaviruses. Nat. Microbiol. 2020, 5, 562–569. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shang, J.; Ye, G.; Shi, K.; Wan, Y.; Luo, C.; Aihara, H.; Geng, Q.; Auerbach, A.; Li, F. Structural basis of receptor recognition by SARS-CoV-2. Nature 2020, 581, 221–224. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Messina, G.; Polito, R.; Monda, V.; Cipolloni, L.; Di Nunno, N.; Di Mizio, G.; Murabito, P.; Carotenuto, M.; Messina, A.; Pisanelli, D.; et al. Functional Role of Dietary Intervention to Improve the Outcome of COVID-19: A Hypothesis of Work. Int. J. Mol. Sci. 2020, 21, 3104. [Google Scholar] [CrossRef] [PubMed]
- Giannopoulos, G.; Vrachatis, D.A.; Deftereos, S.G. Myocardial Injury in COVID-19—Can We Successfully Target Inflammation? JAMA Cardiol. 2020, 5, 1069–1070. [Google Scholar] [CrossRef]
- Zuo, Y.; Yalavarthi, S.; Shi, H.; Gockman, K.; Zuo, M.; Madison, J.A.; Blair, C.; Weber, A.; Barnes, B.J.; Egeblad, M.; et al. Neutrophil extracellular traps in COVID-19. JCI Insight 2020, 5, e138999. [Google Scholar]
- Tavazzi, G.; Pellegrini, C.; Maurelli, M.; Belliato, M.; Sciutti, F.; Bottazzi, A.; Sepe, P.A.; Resasco, T.; Camporotondo, R.; Bruno, R.; et al. Myocardial localization of coronavirus in COVID-19 cardiogenic shock. Eur. J. Heart Fail. 2020, 22, 911–915. [Google Scholar] [CrossRef] [Green Version]
- Monda, V.; Salerno, M.; Sessa, F.; Bernardini, R.; Valenzano, A.; Marsala, G.; Zammit, C.; Avola, R.; Carotenuto, M.; Messina, G.; et al. Functional Changes of Orexinergic Reaction to Psychoactive Substances. Mol. Neurobiol. 2018, 55, 6362–6368. [Google Scholar] [CrossRef]
- Pei, G.; Zhang, Z.; Peng, J.; Liu, L.; Zhang, C.; Yu, C.; Ma, Z.; Huang, Y.; Liu, W.; Yao, Y.; et al. Renal involvement and early prognosis in patients with COVID-19 pneumonia. J. Am. Soc. Nephrol. 2020, 31, 1157–1165. [Google Scholar] [CrossRef]
- Puelles, V.G.; Lütgehetmann, M.; Lindenmeyer, M.T.; Sperhake, J.P.; Wong, M.N.; Allweiss, L.; Chilla, S.; Heinemann, A.; Wanner, N.; Liu, S.; et al. Multiorgan and Renal Tropism of SARS-CoV-2. N. Engl. J. Med. 2020, 383, 590–592. [Google Scholar] [CrossRef]
- Wu, Y.; Xu, X.; Chen, Z.; Duan, J.; Hashimoto, K.; Yang, L.; Liu, C.; Yang, C. Nervous system involvement after infection with COVID-19 and other coronaviruses. Brain. Behav. Immun. 2020, 87, 18–22. [Google Scholar] [CrossRef]
- Solomon, I.H.; Normandin, E.; Bhattacharyya, S.; Mukerji, S.S.; Keller, K.; Ali, A.S.; Adams, G.; Hornick, J.L.; Padera, R.F.; Sabeti, P. Neuropathological Features of Covid-19. N. Engl. J. Med. 2020, 383, 989–992. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.; Xiao, S.Y. Hepatic involvement in COVID-19 patients: Pathology, pathogenesis and clinical implications [Review]. J. Med. Virol. 2020, 92, 1491–1494. [Google Scholar] [CrossRef] [PubMed]
- Ellinghaus, D.; Degenhardt, F.; Bujanda, L.; Buti, M.; Albillos, A.; Invernizzi, P.; Fernández, J.; Prati, D.; Baselli, G.; Asselta, R.; et al. Genomewide Association Study of Severe Covid-19 with Respiratory Failure. N. Engl. J. Med. 2020. [Google Scholar] [CrossRef]
- Marino Gammazza, A.; Légaré, S.; Lo Bosco, G.; Fucarino, A.; Angileri, F.; Conway de Macario, E.; Macario, A.J.; Cappello, F. Human molecular chaperones share with SARS-CoV-2 antigenic epitopes potentially capable of eliciting autoimmunity against endothelial cells: Possible role of molecular mimicry in COVID-19. Cell Stress Chaperones 2020, 25, 737–741. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Source | Country | Full Autopsy (Number and Sex) | Molecular Analysis | Comorbidities |
|---|---|---|---|---|
| Ackermann et al. [33] | Europe (Germany) | 7 (2F; 5M) | NR | Hypertension (2F, 5M); Diabetes, type II (3M); Immunosuppression (1M) |
| Aguiar et al. [34] | Europe (Switzerland) | 1 (F) | RT-PCR | Morbid obesity |
| Barton et al. [35] | USA (OK) | 2 (M) | RT-PCR | Hypertension (1); Deep vein thrombosis (1); Remote pancreatitis (1); Osteoarthritis (1); Myotonic muscular dystrophy (1) |
| Bradley et al. [20] | USA (WA) | 14 (8F; 6M) | RT-PCR | Type 2 diabetes (4F, 2M); Hypertension (5F, 5M); Obstructive sleep apnea (1F, 3M); Obesity(3F, 2M); Cardiovascular diseases (4F, 2M); Chronic kidney disease (4F, 3M); Traumatic brain injury (1M); Frontotemporal dementia (1M); Congestive heart failure (3F, 1M); Hypothyroidism (1F); Osteoporosis (2F); Deep vein thrombosis(1F); Breast cancer (2F) |
| Bryce et al. [19] | USA (NY) | 67 (not available) | RT-PCR | Hypertension (42); Diabetes mellitus (27); Cardiovascular diseases (40); Chronic kidney disease (18); Asthma (12); Obesity (8); Co-infections (7); Cancer (5); Transplantation (5); Chronic obstructive pulmonary disease (COPD) (4). |
| Buja et al. [11] | USA (TX) | 3 (3M) | RT-PCR | Obesity (2M); Hypertension (1M); Heart failure (1M); Type II diabetes mellitus (1M); Microcytic anemia (1M) |
| Carsana et al. [18] | Europe (Italy) | 38 (5F; 33M) | RT-PCR | data were available for 31 patients: Diabetes (9); Hypertension (18); Past malignancies (4); Cardiovascular disorders (11); COPD (3) |
| Cipolloni et al. [36] | Europe (Italy) | 2 (2M) | RT-PCR | Data were not available (1M); nil (1M) |
| Edler et al. [10] | Europe (Germany) | 80 (34F; 46M) | RT-PCR | Cardiovascular diseases (68); Lung diseases (44); Kidney diseases (27); Central nervous system (CNS) diseases (28); Diabetes mellitus (17); Carcinomas/hematological diseases (13); 2 F: nil. |
| Farkash et al. [37] | USA (MI) | 1 (M) | RT-PCR | Obesity; Hyperlipidemia |
| Fox et al. [38] | USA (LA) | 10 (not available) | RT-PCR | Hypertension (7), Type II diabetes mellitus (5); chronic kidney disease (1); Thyroidectomy (1); Rheumatoid arthritis (1); Polymyositis (1); Atrial fibrillation (1); End-stage renal disease (1); Not available (1) |
| Grosse et al. [39] | Europe (Austria) | 14 (5F; 9M) | RT-PCR | Heart disease (5F; 9M); Hypertension (3F; 5M); Renal disease (4F; 2M); Neurologic disease (4F; 3M); Diabetes mellitus (2F; 2M); Malignancy (2M); Respiratory disease (5M); Chronic gastritis (3F; 3M); Liver cirrhosis/fibrosis (1M). |
| Iuga et al. [40] | USA (NY) | 5 (1F; 4M) | NR | Hypertension (5); Diabetes (3); Ischemic cardiomyopathy (3); Chronic lung disease (2); Chronic obstructive pulmonary disease (1); Interstitial lung disease (1); Prostate carcinoma (2); recent spinal surgery (1). |
| Konopka et al. [41] | USA (MI) | 1 | NR | Asthma; Diabetes mellitus |
| Lacy et al. [42] | USA (MI) | 1 | RT-PCR | Diabetes mellitus, Obesity, Hyperlipidemia, Mild intermittent asthma |
| Lax et al. [43] | Europe (Austria) | 11 (not available) | RT-PCR | Obesity (2); Hypertension (9); Type 2 diabetes mellitus (5); Cerebrovascular disease (4); Dementia (4); COPD (1); Coronary heart disease(1); History of malignant disease (1); Pulmonary embolism (1) |
| Menter et al. [44] | Europe (Switzerland) | 21 (4F; 17M) | RT-PCR | Hypertension (21); Cardiovascular disease (15); Obesity (19); Diabetes mellitus (7); Chronic neurological condition (5); COPD (3); Malignancy (3); Chronic liver disease (2); Chronic kidney disease (4); Acquired immunosuppression (1) |
| Okudela et al. [45] | Japan | 1 (F) | RT-PCR | not available |
| Paniz Mondolfi et al. [46] | USA (NY) | 1 (M) | RT-PCR | Parkinson’s disease |
| Reichard et al. [47] | USA (MN) | 1 (M) | RT-PCR | Atherosclerosis |
| Remmelink et al. [48] | Europe (Belgium) | 17 (5F; 12M) | RT-PCR | Hypertension (6F; 4M); Chronic renal failure (2F; 1M); Liver cirrhosis (2F; 1M); Coronary artery disease (2F; 2M); Cerebrovascular disease (2F; 2M); Diabetes (4F; 6M); COPD (2M); Cancer (1F; 3M); Nil (2) |
| Santoriello et al. [49] | USA (NY) | 42 (13F; 29M) | NR | Hypertension (30); Diabetes mellitus (17); Coronary artery disease or Cerebrovascular accident (13); Immunosuppression (2); Chronic Kidney diseases (8); Obesity (10); |
| Schaller et al. [50] | Europe (Germany) | 12 (5F; 7M) | RT-PCR | Immunosuppression (2); Hypertension (7); COPD (2); Chronic Kidney diseases (3); Obesity (2); Cardiovascular diseases (5); Adenocarcinoma of the lung (1); Dementia (1) |
| Su et al. [51] | China | 26 (7F; 19M) | NR | Lung cancer (1M; 1F); Pancreas cancer (1M); Gastric cancer (1M); Liver cancer (1M); Skin Cancer (1M); Diabetes mellitus (2M; 1F); Hypertension (7M; 4F); Chronic kidney diseases (1M; 1F); Nil: 4 (2M; 2F); not available 6 (5M; 1F); |
| Suess et al. [52] | Europe (Germany) | 1 (M) | RT-PCR | Hypertension; Diabetes mellitus; |
| Tombolini et al. [53] | Europe (Italy) | 2 (F) | RT-PCR | Hashimoto’s thyroiditis (1); Diabetes mellitus (1); Nil (1) |
| Varga et al. [54] | Europe (Switzerland) | 3 (1F; 2M) | NR | Coronary artery disease (1M); Hypertension (1F; 2M); Diabetes (1F); Obesity (1F). |
| Wang et al. [55] | China | 2 (1F; 1M) | RT-PCR | Type 2 diabetes (F); Hypertension (F); Nil (M) |
| Wichmann et al. [56] | Europe (Germany) | 12 (3F; 9M) | RT-PCR | Obesity (3M); Parkinson disease (2M); Chronic kidney diseases (1M; 1F); Hypertension (3M); Diabetes mellitus (3M); Asthma (2M); Dementia (1F); Epilepsy (1F); Trisomy 21 (1F); Cardiovascular diseases (6M; 3F); Lung cancer (1F); COPD (1F) |
| Youd et al. [57] | Europe (UK) | 9 (5F; 4M) | RT-PCR | Diabetes (3F; 1M); Hypertension (2F; 2M); COPD (1F; 3M); Asthma (1F); Cardiovascular diseases (3M; 1F); Dementia (1F; 1M); Parkinson’s disease (1M); HIV (1M) |
| Source | Safety Measures | Histological Examination | Immunohistochemistry | Electron Microscopy | Others (Immunofluorescence, RNA-In Situ Hybridization, Post-Mortem Biochemistry) | Focus |
|---|---|---|---|---|---|---|
| [33] | NR | H&E | ACE2; CD3; CD4; CD8; CD15 | Y | NR | Lungs |
| [34] | Y | H&E; SFOG | pankeratin; CD68; CD3 | NR | Post-mortem biochemistry (PCR, procalcitonin) | Full |
| [35] | Y | H&E | CD3; CD4; CD8; CD20; CD68 | NR | NR | Full |
| [20] | Y | H&E | NR | Y | NR | Full |
| [19] | Y | H&E | CD61; CD3; CD4; CD8; ACE2 | Y | Immunofluorescence; RNA-ISH | Full |
| [11] | NR | H&E | CD3; CD4; CD8; CD68; TTF1; CK-7; p40; CK5/6 | Y | NR | Full |
| [18] | Y | H&E; Masson | CD68; CD3; CD45; CD61; TTF1; p40; MIB-1 | Y | NR | Full |
| [36] | Y | H&E; Masson | CD4, CD8, CD20, CD68, CD79 Factor VIII, TNF-alpha, IL6, ACE2 SARS nucleo-capsid protein | NR | NR | Lungs |
| [10] | Y | H&E | NR | NR | RNA-ISH | Full |
| [37] | NR | NR | NR | Y | NR | Kidneys |
| [38] | NR | H&E | CD4; CD8; CD61; CD31 | Y | Immunofluorescence | Heart, lungs |
| [39] | Y | H&E, van Gieson, PAS, Ziehl Nielsen, Grocott methenamine | CD3, CD20, CD68, TTF-1, pancytokeratine | NR | NR | Lungs |
| [40] | NR | H&E; Masson | NR | NR | NR | Adrenal glands |
| [41] | NR | H&E | NR | NR | NR | Lungs |
| [42] | Y | NR | NR | NR | NR | Full |
| [43] | Y | H&E | NR | NR | NR | Full |
| [44] | Y | H&E; aniline blue; Giemsa; periodic acid-Schiff; Congo red; Prussian blue; rhodamine; Gram, Brown-Brenn; Grocott methenamine silver stain | CD3; CD4; CD8; CD20; CD68; MUM1; TTF1; fibrin; ATTR | Y | NR | Full |
| [45] | NR | H&E | NR | NR | NR | Full |
| [46] | NR | NR | NR | Y | NR | CNS |
| [47] | NR | H&E; LFB/PAS; PLP | GFAP; APP | NR | NR | CNS |
| [48] | Y | H&E, Masson trichrome, PAS, Gomori-Grocott | Anti-CMV, anti-HSV, anti-Pneumocystis, nucleo-capsid protein | NR | NR | Full |
| [49] | NR | H&E | NR | NR | ISH | Kidneys |
| [50] | Y | H&E | NR | NR | NR | Full |
| [51] | NR | H&E | CD61; CD31; ACE2; SARS nucleo-capsid protein | Y | Immunofluorescence | Kidneys |
| [52] | NR | H&E; PAS | TTF1: CD68 | NR | NR | Full |
| [53] | NR | H&E | NR | NR | NR | Full |
| [54] | NR | H&E | caspase 3 | Y | NR | Full |
| [55] | Y | H&E; AB-PAS | CD68; CD3; CD4; CD8; CD20; CD56; PD-1; PD-L1; IL6; IL10; TNF-alpha; ACE-2; SARS-CoV2 Rp3 N protein | NR | NR | Full |
| [56] | NR | H&E | cytokeratin AE1/AE3 | NR | NR | Full |
| [57] | Y | H&E | NR | NR | NR | Full |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
D’Errico, S.; Zanon, M.; Montanaro, M.; Radaelli, D.; Sessa, F.; Di Mizio, G.; Montana, A.; Corrao, S.; Salerno, M.; Pomara, C. More than Pneumonia: Distinctive Features of SARS-Cov-2 Infection. From Autopsy Findings to Clinical Implications: A Systematic Review. Microorganisms 2020, 8, 1642. https://doi.org/10.3390/microorganisms8111642
D’Errico S, Zanon M, Montanaro M, Radaelli D, Sessa F, Di Mizio G, Montana A, Corrao S, Salerno M, Pomara C. More than Pneumonia: Distinctive Features of SARS-Cov-2 Infection. From Autopsy Findings to Clinical Implications: A Systematic Review. Microorganisms. 2020; 8(11):1642. https://doi.org/10.3390/microorganisms8111642
Chicago/Turabian StyleD’Errico, Stefano, Martina Zanon, Martina Montanaro, Davide Radaelli, Francesco Sessa, Giulio Di Mizio, Angelo Montana, Salvatore Corrao, Monica Salerno, and Cristoforo Pomara. 2020. "More than Pneumonia: Distinctive Features of SARS-Cov-2 Infection. From Autopsy Findings to Clinical Implications: A Systematic Review" Microorganisms 8, no. 11: 1642. https://doi.org/10.3390/microorganisms8111642