
Laboratory Findings and Clinical Outcomes of ICU-admitted COVID-19 Patients: A Retrospective Assessment of Particularities Identified among Romanian Minorities

 ,
,  ,
,  , ,
, , 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Ethics
2.2. Inclusion Criteria and Variables
2.3. Statistical Analysis
3. Results
Patients’ Background Characteristics
4. Discussion
4.1. Literature Findings
4.2. Study Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Mattoo, S.U.; Kim, S.J.; Ahn, D.G.; Myoung, J. Escape and Over-Activation of Innate Immune Responses by SARS-CoV-2: Two Faces of a Coin. Viruses 2022, 14, 530. [Google Scholar] [CrossRef] [PubMed]
- Marincu, I.; Bratosin, F.; Vidican, I.; Bostanaru, A.-C.; Frent, S.; Cerbu, B.; Turaiche, M.; Tirnea, L.; Timircan, M. Predictive Value of Comorbid Conditions for COVID-19 Mortality. J. Clin. Med. 2021, 10, 2652. [Google Scholar] [CrossRef]
- Timircan, M.; Bratosin, F.; Vidican, I.; Suciu, O.; Tirnea, L.; Avram, V.; Marincu, I. Exploring Pregnancy Outcomes Associated with SARS-CoV-2 Infection. Medicina 2021, 57, 796. [Google Scholar] [CrossRef] [PubMed]
- Ball, L.; Silva, P.L.; Giacobbe, D.R.; Bassetti, M.; Zubieta-Calleja, G.R.; Rocco, P.R.M.; Pelosi, P. Understanding the pathophysiology of typical acute respiratory distress syndrome and severe COVID-19. Expert Rev. Respir. Med. 2022, 16, 437–446. [Google Scholar] [CrossRef] [PubMed]
- Stoicescu, E.R.; Manolescu, D.L.; Iacob, R.; Cerbu, S.; Dima, M.; Iacob, E.R.; Ciuca, I.M.; Oancea, C.; Iacob, D. The Assessment of COVID-19 Pneumonia in Neonates: Observed by Lung Ultrasound Technique and Correlated with Biomarkers and Symptoms. J. Clin. Med. 2022, 11, 3555. [Google Scholar] [CrossRef] [PubMed]
- Manolescu, D.; Timar, B.; Bratosin, F.; Rosca, O.; Citu, C.; Oancea, C. Predictors for COVID-19 Complete Remission with HRCT Pattern Evolution: A Monocentric, Prospective Study. Diagnostics 2022, 12, 1397. [Google Scholar] [CrossRef]
- Mocanu, A.; Lazureanu, V.; Cut, T.; Laza, R.; Musta, V.; Nicolescu, N.; Marinescu, A.; Nelson-Twakor, A.; Dumache, R.; Mederle, O. Angiocatheter Decompression on a COVID-19 Patient with severe Pneumonia, Pneumothorax, and Subcutaneous Emphysema. Clin. Lab. 2022, 68. [Google Scholar] [CrossRef]
- Mocanu, A.; Noja, G.G.; Istodor, A.V.; Moise, G.; Leretter, M.; Rusu, L.C.; Marza, A.M.; Mederle, A.O. Individual Characteristics as Prognostic Factors of the Evolution of Hospitalized COVID-19 Romanian Patients: A Comparative Observational Study between the First and Second Waves Based on Gaussian Graphical Models and Structural Equation Modeling. J. Clin. Med. 2021, 10, 1958. [Google Scholar] [CrossRef] [PubMed]
- Hojyo, S.; Uchida, M.; Tanaka, K.; Hasebe, R.; Tanaka, Y.; Murakami, M.; Hirano, T. How COVID-19 induces cytokine storm with high mortality. Inflamm. Regen. 2020, 40, 37. [Google Scholar] [CrossRef] [PubMed]
- Pilut, C.N.; Citu, C.; Gorun, F.; Bratosin, F.; Gorun, O.M.; Burlea, B.; Citu, I.M.; Grigoras, M.L.; Manolescu, D.; Gluhovschi, A. The Utility of Laboratory Parameters for Cardiac Inflammation in Heart Failure Patients Hospitalized with SARS-CoV-2 Infection. Diagnostics 2022, 12, 824. [Google Scholar] [CrossRef]
- Mocanu, A.; Lazureanu, V.E.; Marinescu, A.R.; Cut, T.G.; Laza, R.; Rusu, L.-C.; Marza, A.M.; Nelson-Twakor, A.; Negrean, R.A.; Popescu, I.-M.; et al. A Retrospective Assessment of Laboratory Findings and Cytokine Markers in Severe SARS-CoV-2 Infection among Patients of Roma Population. J. Clin. Med. 2022, 11, 6777. [Google Scholar] [CrossRef] [PubMed]
- Citu, I.M.; Citu, C.; Gorun, F.; Neamtu, R.; Motoc, A.; Burlea, B.; Rosca, O.; Bratosin, F.; Hosin, S.; Manolescu, D.; et al. Using the NYHA Classification as Forecasting Tool for Hospital Readmission and Mortality in Heart Failure Patients with COVID-19. J. Clin. Med. 2022, 11, 1382. [Google Scholar] [CrossRef] [PubMed]
- Merad, M.; Subramanian, A.; Wang, T.T. An aberrant inflammatory response in severe COVID-19. Cell Host Microbe 2021, 29, 1043–1047. [Google Scholar] [CrossRef] [PubMed]
- Zeng, F.; Huang, Y.; Guo, Y.; Yin, M.; Chen, X.; Xiao, L.; Deng, G. Association of inflammatory markers with the severity of COVID-19: A meta-analysis. Int. J. Infect. Dis. 2020, 96, 467–474. [Google Scholar] [CrossRef]
- Turaiche, M.; Feciche, B.; Gluhovschi, A.; Bratosin, F.; Bogdan, I.; Bota, A.V.; Grigoras, M.L.; Gurban, C.V.; Cerbu, B.; Toma, A.-O.; et al. Biological Profile and Clinical Features as Determinants for Prolonged Hospitalization in Adult Patients with Measles: A Monocentric Study in Western Romania. Pathogens 2022, 11, 1018. [Google Scholar] [CrossRef]
- Frediansyah, A.; Tiwari, R.; Sharun, K.; Dhama, K.; Harapan, H. Antivirals for COVID-19: A critical review. Clin. Epidemiol. Glob. Health 2021, 9, 90–98. [Google Scholar] [CrossRef]
- Tirnea, L.; Bratosin, F.; Vidican, I.; Cerbu, B.; Turaiche, M.; Timircan, M.; Margan, M.-M.; Marincu, I. The Efficacy of Convalescent Plasma Use in Critically Ill COVID-19 Patients. Medicina 2021, 57, 257. [Google Scholar] [CrossRef]
- Gil-Etayo, F.J.; Suàrez-Fernández, P.; Cabrera-Marante, O.; Arroyo, D.; Garcinuño, S.; Naranjo, L.; Pleguezuelo, D.E.; Allende, L.M.; Mancebo, E.; Lalueza, A.; et al. T-Helper Cell Subset Response Is a Determining Factor in COVID-19 Progression. Front. Cell. Infect. Microbiol. 2021, 11, 624483. [Google Scholar] [CrossRef]
- Zanza, C.; Romenskaya, T.; Manetti, A.C.; Franceschi, F.; La Russa, R.; Bertozzi, G.; Maiese, A.; Savioli, G.; Volonnino, G.; Longhitano, Y. Cytokine Storm in COVID-19: Immunopathogenesis and Therapy. Medicina 2022, 58, 144. [Google Scholar] [CrossRef]
- Montazersaheb, S.; Hosseiniyan Khatibi, S.M.; Hejazi, M.S.; Tarhriz, V.; Farjami, A.; Ghasemian Sorbeni, F.; Farahzadi, R.; Ghasemnejad, T. COVID-19 infection: An overview on cytokine storm and related interventions. Virol. J. 2022, 19, 92. [Google Scholar] [CrossRef]
- Cidade, J.P.; Coelho, L.; Costa, V.; Morais, R.; Moniz, P.; Morais, L.; Fidalgo, P.; Tralhão, A.; Paulino, C.; Nora, D.; et al. Predictive value of D-dimer in the clinical outcome of severe COVID19 patients: Are we giving it too much credit? Clin. Appl. Thromb. Hemost. 2022, 28, 10760296221079612. [Google Scholar] [CrossRef] [PubMed]
- Ramatillah, D.L.; Gan, S.H.; Pratiwy, I.; Syed Sulaiman, S.A.; Jaber, A.A.S.; Jusnita, N.; Lukas, S.; Abu Bakar, U. Impact of cytokine storm on severity of COVID-19 disease in a private hospital in West Jakarta prior to vaccination. PLoS ONE 2022, 17, e0262438. [Google Scholar] [CrossRef] [PubMed]
- Armitage, R.; Nellums, L.B. COVID-19 and the Gypsy, Roma and Traveller population. Public Health 2020, 185, 48. [Google Scholar] [CrossRef] [PubMed]
- Citu, I.M.; Citu, C.; Gorun, F.; Sas, I.; Tomescu, L.; Neamtu, R.; Motoc, A.; Gorun, O.M.; Burlea, B.; Bratosin, F.; et al. Immunogenicity Following Administration of BNT162b2 and Ad26.COV2.S COVID-19 Vaccines in the Pregnant Population during the Third Trimester. Viruses 2022, 14, 307. [Google Scholar] [CrossRef] [PubMed]
- Fatima, S.; Zafar, A.; Afzal, H.; Ejaz, T.; Shamim, S.; Saleemi, S.; Subhan Butt, A. COVID-19 infection among vaccinated and unvaccinated: Does it make any difference? PLoS ONE 2022, 17, e0270485. [Google Scholar] [CrossRef]
- Cerbu, B.; Pantea, S.; Bratosin, F.; Vidican, I.; Turaiche, M.; Frent, S.; Borsi, E.; Marincu, I. Liver Impairment and Hematological Changes in Patients with Chronic Hepatitis C and COVID-19: A Retrospective Study after One Year of Pandemic. Medicina 2021, 57, 597. [Google Scholar] [CrossRef]
- Samara, A.A.; Boutlas, S.; Janho, M.B.; Gourgoulianis, K.I.; Sotiriou, S. COVID-19 Severity and Mortality after Vaccination against SARS-CoV-2 in Central Greece. J. Pers. Med. 2022, 12, 1423. [Google Scholar] [CrossRef]
- Li, X.; Zhong, X.; Wang, Y.; Zeng, X.; Luo, T.; Liu, Q. Clinical determinants of the severity of COVID-19: A systematic review and meta-analysis. PLoS ONE 2021, 16, e0250602. [Google Scholar] [CrossRef]
- Bogdan, I.; Citu, C.; Bratosin, F.; Malita, D.; Romosan, I.; Gurban, C.V.; Bota, A.V.; Turaiche, M.; Bratu, M.L.; Pilut, C.N.; et al. The Impact of Multiplex PCR in Diagnosing and Managing Bacterial Infections in COVID-19 Patients Self-Medicated with Antibiotics. Antibiotics 2022, 11, 437. [Google Scholar] [CrossRef]
- Munne, K.; Bhanothu, V.; Bhor, V.; Patel, V.; Mahale, S.D.; Pande, S. Detection of SARS-CoV-2 infection by RT-PCR test: Factors influencing interpretation of results. Virusdisease 2021, 32, 187–189. [Google Scholar] [CrossRef]
- Enache, G.; Rusu, E.; Ilinca, A.; Rusu, F.; Costache, A.; Jinga, M.; Pănuş, C.; Radulian, G. Prevalence of Overweight and Obesity In a Roma Population from Southern Romania—Calarasi County. Acta Endocrinol. 2018, 14, 122–130. [Google Scholar] [CrossRef] [PubMed]
- Abate, S.M.; Ahmed Ali, S.; Mantfardo, B.; Basu, B. Rate of Intensive Care Unit admission and outcomes among patients with coronavirus: A systematic review and Meta-analysis. PLoS ONE 2020, 15, e0235653. [Google Scholar] [CrossRef] [PubMed]
- Negrut, N.; Codrean, A.; Hodisan, I.; Bungau, S.; Tit, D.M.; Marin, R.; Behl, T.; Banica, F.; Diaconu, C.C.; Nistor-Cseppento, D.C. Efficiency of antiviral treatment in COVID-19. Exp. Ther. Med. 2021, 21, 648. [Google Scholar] [CrossRef]
- Orton, L.; de Cuevas, R.A.; Stojanovski, K.; Gamella, J.F.; Greenfields, M.; La Parra, D.; Marcu, O.; Matras, Y.; Donert, C.; Frost, D.; et al. Roma populations and health inequalities: A new perspective. Int. J. Hum. Rights Healthc. 2019, 12, 319–327. [Google Scholar] [CrossRef]
- Tombat, K.; van Dijk, J.P. Roma Health: An Overview of Communicable Diseases in Eastern and Central Europe. Int. J. Environ. Res. Public Health 2020, 17, 7632. [Google Scholar] [CrossRef] [PubMed]
- de Graaf, P.; Rotar Pavlič, D.; Zelko, E.; Vintges, M.; Willems, S.; Hanssens, L. Primary care for the Roma in Europe: Position paper of the European forum for primary care. Zdr. Varst. 2016, 55, 218–224. [Google Scholar] [CrossRef] [Green Version]
- McFadden, A.; Siebelt, L.; Gavine, A.; Atkin, K.; Bell, K.; Innes, N.; Jones, H.; Jackson, C.; Haggi, H.; MacGillivray, S. Gypsy, Roma and Traveller access to and engagement with health services: A systematic review. Eur. J. Public Health 2018, 28, 74–81. [Google Scholar] [CrossRef] [Green Version]
- Santa Cruz, A.; Mendes-Frias, A.; Oliveira, A.I.; Dias, L.; Matos, A.R.; Carvalho, A.; Capela, C.; Pedrosa, J.; Castro, A.G.; Silvestre, R. Interleukin-6 Is a Biomarker for the Development of Fatal Severe Acute Respiratory Syndrome Coronavirus 2 Pneumonia. Front. Immunol. 2021, 12, 613422. [Google Scholar] [CrossRef]
- Avila-Nava, A.; Cortes-Telles, A.; Torres-Erazo, D.; López-Romero, S.; Chim Aké, R.; Gutiérrez Solis, A.L. Serum IL-6: A potential biomarker of mortality among SARS-CoV-2 infected patients in Mexico. Cytokine 2021, 143, 155543. [Google Scholar] [CrossRef]
- Broască, L.; Trușculescu, A.A.; Ancușa, V.M.; Ciocârlie, H.; Oancea, C.-I.; Stoicescu, E.-R.; Manolescu, D.L. A Novel Method for Lung Image Processing Using Complex Networks. Tomography 2022, 8, 1928–1946. [Google Scholar] [CrossRef]
- Grifoni, E.; Valoriani, A.; Cei, F.; Lamanna, R.; Gelli, A.M.G.; Ciambotti, B.; Vannucchi, V.; Moroni, F.; Pelagatti, L.; Tarquini, R.; et al. Interleukin-6 as prognosticator in patients with COVID-19. J. Infect. 2020, 81, 452–482. [Google Scholar] [CrossRef] [PubMed]
- Ahnach, M.; Zbiri, S.; Nejjari, S.; Ousti, F.; Elkettani, C. C-reactive protein as an early predictor of COVID-19 severity. J. Med. Biochem. 2020, 39, 500–507. [Google Scholar] [CrossRef] [PubMed]
- Kudlinski, B.; Zgoła, D.; Stolińska, M.; Murkos, M.; Kania, J.; Nowak, P.; Noga, A.; Wojciech, M.; Zaborniak, G.; Zembron-Lacny, A. Systemic Inflammatory Predictors of In-Hospital Mortality in COVID-19 Patients: A Retrospective Study. Diagnostics 2022, 12, 859. [Google Scholar] [CrossRef]
- Ikeagwulonu, R.C.; Ugwu, N.I.; Ezeonu, C.T.; Ikeagwulonu, Z.C.; Uro-Chukwu, H.C.; Asiegbu, U.V.; Obu, D.C.; Briggs, D.C. C-Reactive Protein and COVID-19 Severity: A Systematic Review. West Afr. J. Med. 2021, 38, 1011–1023. [Google Scholar]
- Moisa, E.; Corneci, D.; Negutu, M.I.; Filimon, C.R.; Serbu, A.; Popescu, M.; Negoita, S.; Grintescu, I.M. Development and Internal Validation of a New Prognostic Model Powered to Predict 28-Day All-Cause Mortality in ICU COVID-19 Patients—The COVID-SOFA Score. J. Clin. Med. 2022, 11, 4160. [Google Scholar] [CrossRef] [PubMed]
- Citu, C.; Citu, I.M.; Motoc, A.; Forga, M.; Gorun, O.M.; Gorun, F. Predictive Value of SOFA and qSOFA for In-Hospital Mortality in COVID-19 Patients: A Single-Center Study in Romania. J. Pers. Med. 2022, 12, 878. [Google Scholar] [CrossRef] [PubMed]
- Hu, H.; Pan, H.; Li, R.; He, K.; Zhang, H.; Liu, L. Increased Circulating Cytokines Have a Role in COVID-19 Severity and Death With a More Pronounced Effect in Males: A Systematic Review and Meta-Analysis. Front. Pharmacol. 2022, 13, 802228. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Variables * | Cases (n = 71) | Controls (n = 213) | p-Value |
|---|---|---|---|
| Background Data | |||
| Age | 0.997 | ||
| 18–40 years | 13 (18.3%) | 39 (18.3%) | |
| 40–65 years | 24 (33.8%) | 73 (34.3%) | |
| >65 years | 34 (47.9%) | 101 (47.4%) | |
| Sex | 0.448 | ||
| Men | 42 (59.2%) | 115 (54.0%) | |
| Women | 29 (40.8%) | 98 (46.0%) | |
| BMI | 0.043 | ||
| Underweight (<18.5 kg/m2) | 4 (4.8%) | 14 (5.1%) | |
| Normal weight (18.5–25.0 kg/m2) | 27 (37.3%) | 1115 (54.2%) | |
| Overweight (>25.0 kg/m2) | 40 (57.8%) | 84 (40.7%) | |
| Other characteristics | |||
| Area of residence (urban) | 32 (45.1%) | 132 (62.0%) | 0.012 |
| Occupation (unemployed) | 27 (38.0%) | 55 (25.8%) | 0.049 |
| Relationship status (married) | 66 (93.0%) | 194 (91.1%) | 0.622 |
| Substance use behavior | |||
| Chronic smoking | 27 (38.0%) | 53 (24.9%) | 0.032 |
| Chronic alcohol use | 6 (8.5%) | 14 (6.6%) | 0.592 |
| Number of comorbidities | 0.017 | ||
| 0 | 7 (9.9%) | 36 (16.9%) | |
| 1 | 12 (16.9%) | 31 (14.6%) | |
| 2 | 14 (19.7%) | 72 (33.8%) | |
| ≥3 | 38 (53.5%) | 74 (34.7%) | |
| Wave of SARS-CoV-2 infection | 0.506 | ||
| 1 | 13 (18.3%) | 33 (15.5%) | |
| 2 | 16 (22.5%) | 41 (19.2%) | |
| 3 | 8 (11.3%) | 15 (7.0%) | |
| 4 | 9 (12.7%) | 22 (10.3%) | |
| 5 | 18 (25.4%) | 66 (31.0%) | |
| 6 | 7 (9.9%) | 36 (16.9%) | |
| COVID-19 vaccination status | 0.916 | ||
| Yes | 9 (12.7%) | 26 (12.2%) | |
| No | 62 (87.3%) | 187 (87.8%) | |
| COVID-19 vaccine | (n = 9) | (n = 26) | 0.757 |
| BNT162b2 | 3 (33.3%) | 11 (42.3%) | |
| mRNA-1273 | 2 (22.2%) | 7 (26.9%) | |
| Ad26.COV2.S | 4 (44.4%) | 8 (30.8%) | |
| COVID-19 transmission source | 0.882 | ||
| Community | 11 (15.5%) | 38 (17.8%) | |
| Family | 27 (38.0%) | 76 (35.7%) | |
| Unknown source | 33 (46.5%) | 99 (46.5%) |
| Variables * | Cases (n = 71) | Controls (n = 213) | p-Value |
|---|---|---|---|
| Signs and Symptoms | |||
| Cough | 52 (62.7%) | 160 (67.8%) | 0.393 |
| Fever | 59 (71.1%) | 173 (73.3%) | 0.695 |
| Dyspnea | 43 (51.8%) | 127 (53.8%) | 0.752 |
| Headache | 10 (12.0%) | 38 (16.1%) | 0.374 |
| Digestive symptoms | 21 (25.3%) | 43 (18.2%) | 0.165 |
| Anosmia/ageusia | 24 (28.9%) | 71 (30.1%) | 0.841 |
| Fatigue | 72 (86.7%) | 194 (82.2%) | 0.338 |
| Myalgia/arthralgia | 22 (26.5%) | 61 (25.8%) | 0.906 |
| Dysphagia | 4 (4.8%) | 13 (5.5%) | 0.809 |
| COVID-19 treatment | |||
| Antivirals | 69 (83.1%) | 201 (85.2%) | 0.657 |
| Corticosteroids | 65 (78.3%) | 19 (83.5%) | 0.291 |
| Antibiotics | 70 (84.3%) | 209 (88.6%) | 0.317 |
| Anticoagulant | 61 (73.5%) | 175 (74.2%) | 0.906 |
| Immune modulators | 23 (27.7%) | 62 (26.3%) | 0.798 |
| Thrombo-embolic complications | 0.312 | ||
| Yes | 6 (8.5%) | 11 (5.2%) | |
| No | 65 (91.5%) | 202 (94.8%) | |
| Clinical features | |||
| Severe imaging features | 29 (40.8%) | 60 (28.2%) | 0.046 |
| Oxygen saturation on admission (<92%) | 22 (31.0%) | 54 (25.4%) | 0.353 |
| Respiratory rate on admission (>20/min) | 38 (53.5%) | 96 (45.1%) | 0.216 |
| Heart rate on admission (>100 bpm) | 35 (66.0%) | 123 (57.7%) | 0.214 |
| Variables * | Cases (n = 71) | Controls (n = 213) | p-Value |
|---|---|---|---|
| Mean duration of hospital stay | 18.2 ± 5.3 | 16.4 ± 6.1 | 0.027 |
| Median duration from symptom onset until hospital admission | 3.5 (4.0) | 4.5 (6.5) | 0.190 |
| Viral clearance | 16.8 ± 6.3 | 14.5 ± 6.8 | 0.012 |
| Median duration from hospital admission to ICU admission | 3.5 (5.5) | 5.0 (7.0) | 0.113 |
| SOFA score | 2.7 (3.1) | 2.2 (3.4) | 0.077 |
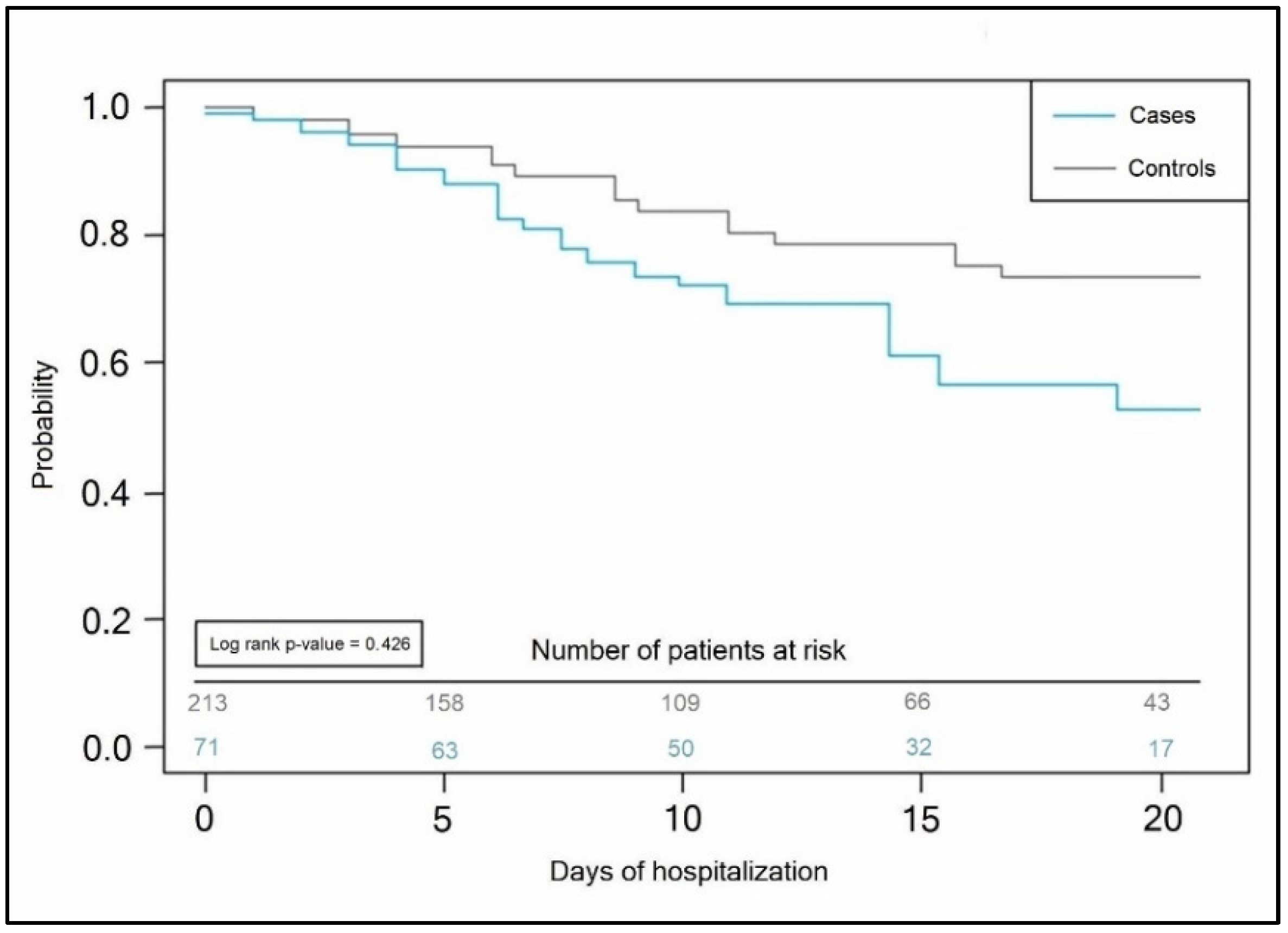
| Median duration of ICU stay | 7 (11) | 5 (8) | <0.001 |
| Severe in-hospital complications | 17 (23.9%) | 66 (31.0%) | 0.258 |
| Intubation | 33 (46.5%) | 104 (48.8%) | 0.737 |
| Mortality | 19 (26.8%) | 46 (21.6%) | 0.369 |
| Variables * | Normal Range | Cases (n = 71) | Controls (n = 213) | p-Value |
|---|---|---|---|---|
| Procalcitonin (ug/L) | 0–0.25 | 0.66 (0.38) | 0.69 (0.33) | 0.629 |
| D-dimers (ng/mL) | <250 | 262 (93) | 268 (98) | 0.551 |
| IL-6 (pg/mL) | 0.8–6.4 | 7.8 (3.9) | 7.1 (3.7) | 0.104 |
| TNF-α (pg/mL) | 7.8–12.2 | 12.5 (4.0) | 12.6 (4.2) | 0.590 |
| Ferritin (ng/mL) | 20–250 | 228 (72) | 214 (66) | 0.282 |
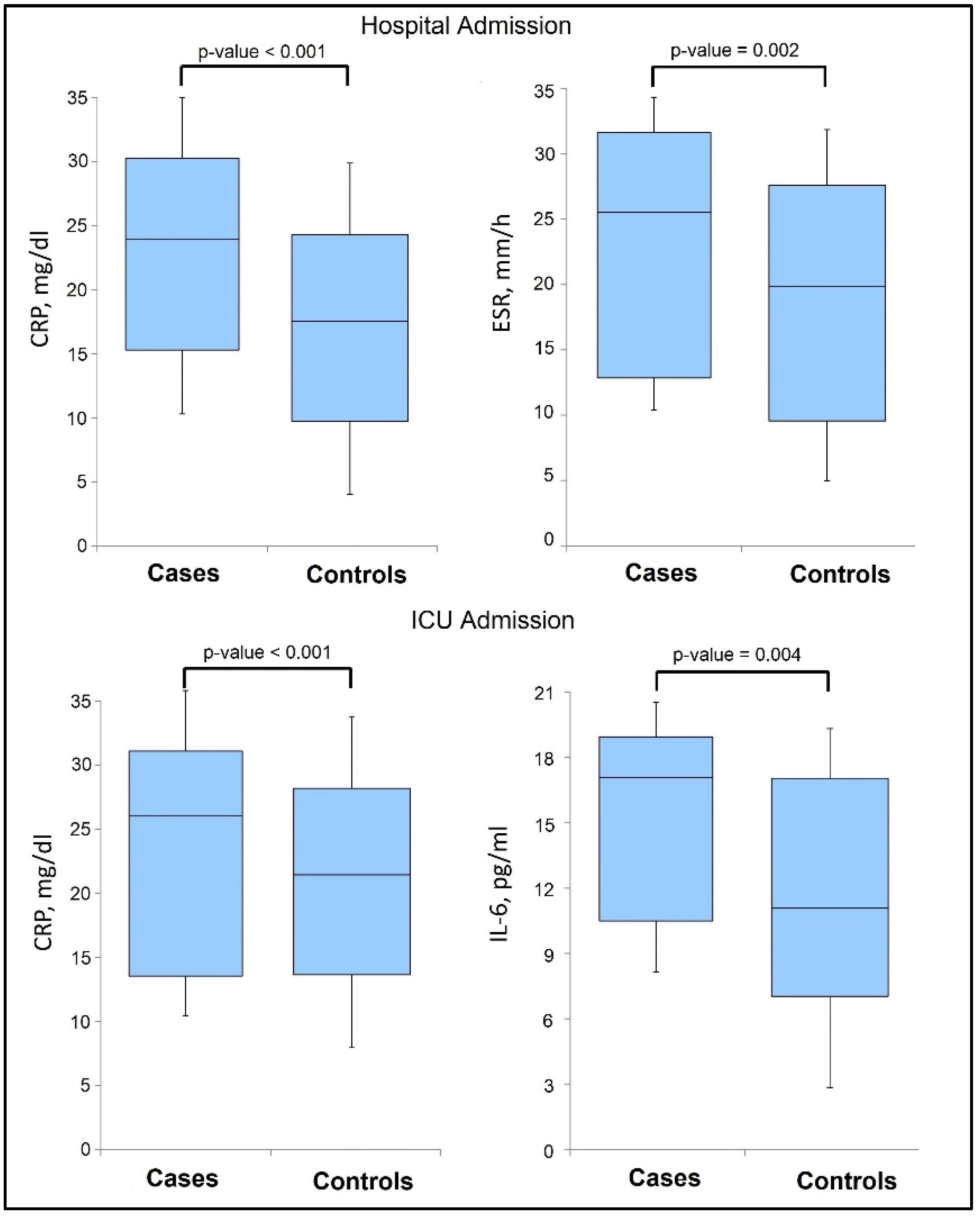
| ESR (mm/h) | 0–22 | 26 (20) | 20 (18) | 0.002 |
| CRP (mg/dL) | 0–10 | 24 (15) | 17 (14) | <0.001 |
| Fibrinogen (g/L) | 2–4 | 4.1 (2.7) | 4.8 (3.0) | 0.088 |
| Variables * | Normal Range | Cases (n = 71) | Controls (n = 213) | p-Value |
|---|---|---|---|---|
| Procalcitonin (ug/L) | 0–0.25 | 0.93 (0.68) | 0.82 (0.50) | 0.063 |
| D-dimers (ng/mL) | <250 | 318 (166) | 304 (157) | 0.292 |
| IL-6 (pg/mL) | 0.8–6.4 | 17 (9) | 11 (10) | 0.004 |
| TNF-α (pg/mL) | 7.8–12.2 | 15.0 (6.4) | 14.9 (6.8) | 0.527 |
| Ferritin (ng/mL) | 20–250 | 242 (92) | 257 (72) | 0.406 |
| ESR (mm/h) | 0–22 | 26 (20) | 20 (18) | 0.094 |
| CRP (mg/dL) | 0–10 | 27 (17) | 21 (11) | <0.001 |
| Fibrinogen (g/L) | 2–4 | 6.1 (3.3) | 5.8 (3.0) | 0.215 |
| General Population | Roma Ethnicity | |||||
|---|---|---|---|---|---|---|
| Constants (Dependent) | β | (95% CI of β) | p-Value | β | (95% CI of β) | p-Value |
| 1× Normal Range | ||||||
| CRP >10 mg/dL | 1.39 | 0.94–1.82 | 0.334 | 1.58 | 0.99–1.93 | 0.217 |
| ESR >22 mm/h | 0.94 | 0.62–1.57 | 0.390 | 1.66 | 0.89–1.87 | 0.195 |
| IL-6 >6.4 pg/mL | 0.86 | 0.70–1.64 | 0.261 | 1.27 | 0.90–1.74 | 0.113 |
| 2× Normal Range | ||||||
| CRP >20 mg/dL | 1.53 | 0.98–2.42 | 0.066 | 1.93 | 1.15–3.66 | 0.020 |
| ESR >44 mm/h | 1.15 | 0.98–1.49 | 0.081 | 1.41 | 1.22–2.38 | 0.104 |
| IL-6 >12.8 pg/mL | 0.98 | 0.91–1.53 | 0.473 | 1.85 | 1.02–2.79 | 0.044 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mocanu, A.; Lazureanu, V.E.; Laza, R.; Marinescu, A.R.; Cut, T.G.; Sincaru, S.-V.; Marza, A.M.; Popescu, I.-M.; Herlo, L.-F.; Nelson-Twakor, A.; et al. Laboratory Findings and Clinical Outcomes of ICU-admitted COVID-19 Patients: A Retrospective Assessment of Particularities Identified among Romanian Minorities. J. Pers. Med. 2023, 13, 195. https://doi.org/10.3390/jpm13020195
Mocanu A, Lazureanu VE, Laza R, Marinescu AR, Cut TG, Sincaru S-V, Marza AM, Popescu I-M, Herlo L-F, Nelson-Twakor A, et al. Laboratory Findings and Clinical Outcomes of ICU-admitted COVID-19 Patients: A Retrospective Assessment of Particularities Identified among Romanian Minorities. Journal of Personalized Medicine. 2023; 13(2):195. https://doi.org/10.3390/jpm13020195
Chicago/Turabian StyleMocanu, Alexandra, Voichita Elena Lazureanu, Ruxandra Laza, Adelina Raluca Marinescu, Talida Georgiana Cut, Suzana-Vasilica Sincaru, Adina Maria Marza, Irina-Maria Popescu, Lucian-Flavius Herlo, Andreea Nelson-Twakor, and et al. 2023. "Laboratory Findings and Clinical Outcomes of ICU-admitted COVID-19 Patients: A Retrospective Assessment of Particularities Identified among Romanian Minorities" Journal of Personalized Medicine 13, no. 2: 195. https://doi.org/10.3390/jpm13020195