
Predictors of the Development of Mental Disorders in Hospitalized COVID-19 Patients without Previous Psychiatric History: A Single-Center Retrospective Study in South Korea

 , and
, and
Abstract
:1. Introduction
2. Methods
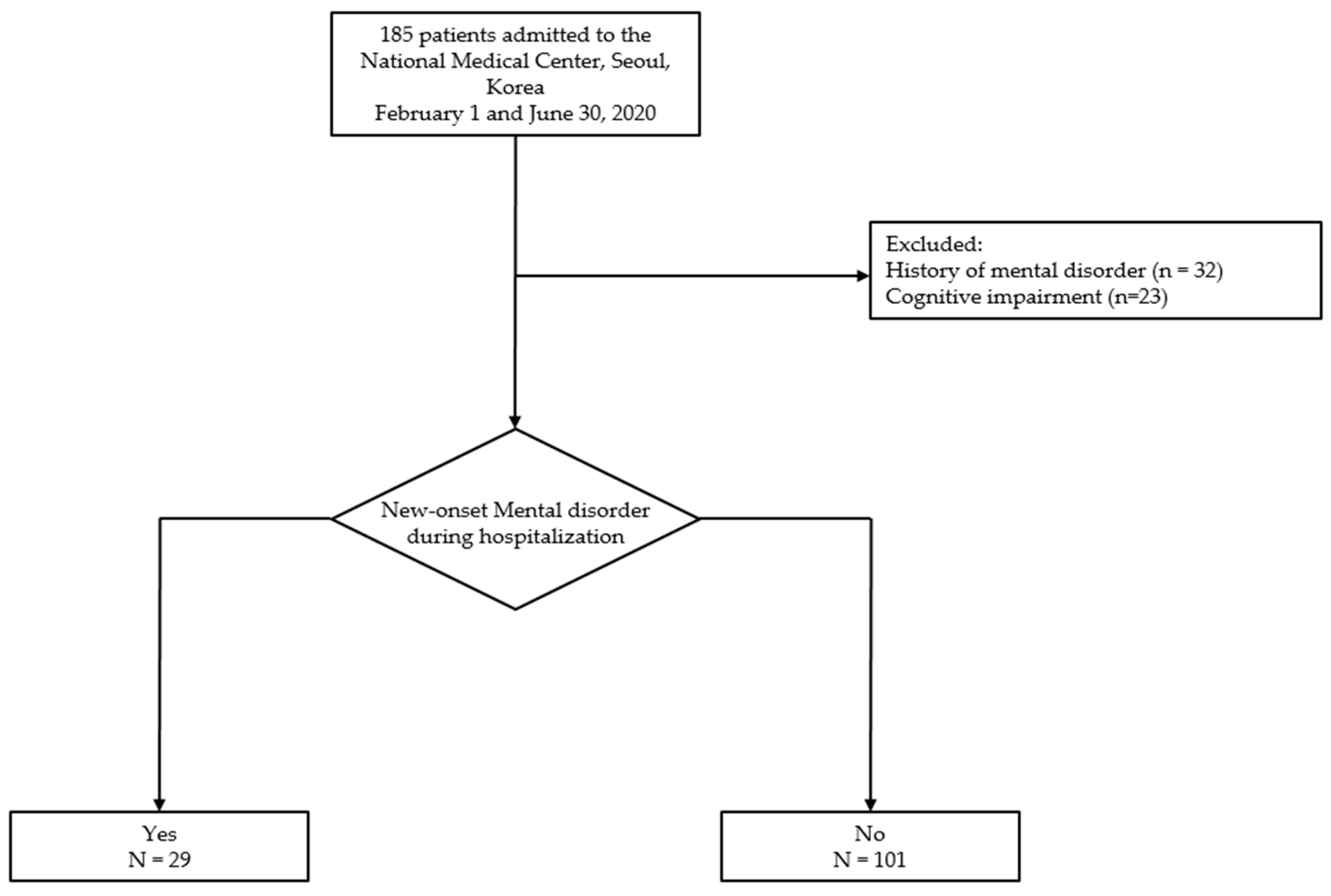
2.1. Study Design and Subjects
2.2. Outcome Variable
2.3. Psychological Instruments
2.4. Data Collection
2.5. Statistical Analysis
3. Results
3.1. Demographic and Clinical Characteristics
3.2. Psychological Assessment
3.3. Newly Developed Mental Disorders and Prescribed Psychotropic Medications
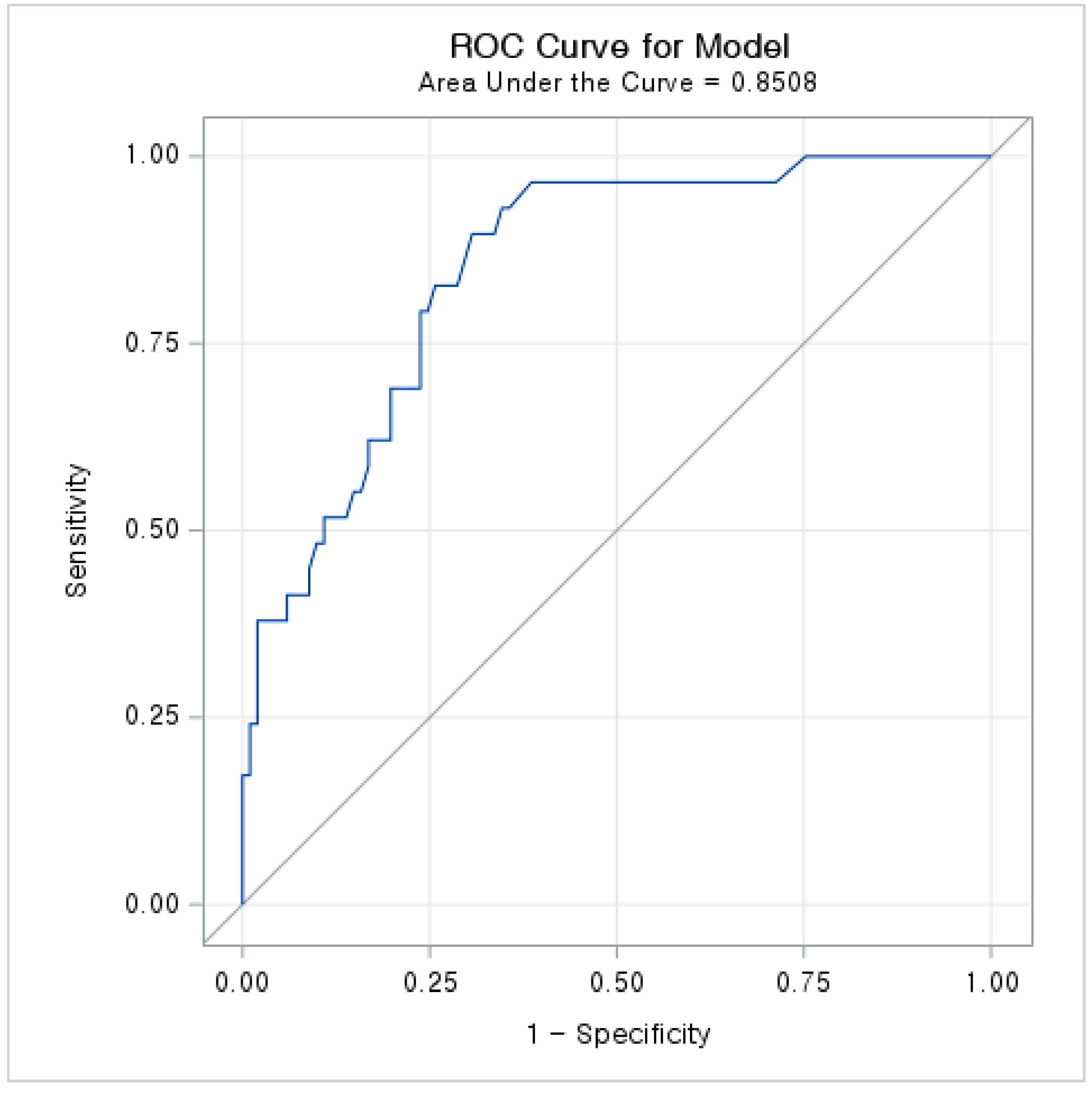
3.4. Predictors of New-Onset Mental Disorders
4. Discussion
5. Limitations
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization (WHO). Weekly Epidemiological Update on COVID-19—28 December 2021. Available online: https://www.who.int/publications/m/item/weekly-epidemiological-update-on-covid-19---28-december-2021 (accessed on 7 December 2021).
- Xie, Q.; Liu, X.B.; Xu, Y.M.; Zhong, B.L. Understanding the psychiatric symptoms of COVID-19: A meta-analysis of studies assessing psychiatric symptoms in Chinese patients with and survivors of COVID-19 and SARS by using the Symptom Checklist-90-Revised. Transl. Psychiatry 2021, 11, 290. [Google Scholar] [CrossRef]
- Kaseda, E.T.; Levine, A.J. Post-traumatic stress disorder: A differential diagnostic consideration for COVID-19 survivors. Clin. Neuropsychol. 2020, 34, 1498–1514. [Google Scholar] [CrossRef]
- Holmes, E.A.; O’Connor, R.C.; Perry, V.H.; Tracey, I.; Wessely, S.; Arseneault, L.; Ballard, C.; Christensen, H.; Cohen Silver, R.; Everall, I.; et al. Multidisciplinary research priorities for the COVID-19 pandemic: A call for action for mental health science. Lancet Psychiatry 2020, 7, 547–560. [Google Scholar] [CrossRef]
- Huang, C.; Huang, L.; Wang, Y.; Li, X.; Ren, L.; Gu, X.; Kang, L.; Guo, L.; Liu, M.; Zhou, X.; et al. 6-month consequences of COVID-19 in patients discharged from hospital: A cohort study. Lancet 2021, 397, 220–232. [Google Scholar] [CrossRef]
- Park, H.Y.; Song, I.A.; Lee, S.H.; Sim, M.Y.; Oh, H.S.; Song, K.H.; Yu, E.S.; Park, H.Y.; Oh, T.K. Prevalence of mental illness among COVID-19 survivors in South Korea: Nationwide cohort. BJPsych Open 2021, 7, e183. [Google Scholar] [CrossRef] [PubMed]
- Yuan, B.; Li, W.; Liu, H.; Cai, X.; Song, S.; Zhao, J.; Hu, X.; Li, Z.; Chen, Y.; Zhang, K.; et al. Correlation between immune response and self-reported depression during convalescence from COVID-19. Brain Behav. Immun. 2020, 88, 39–43. [Google Scholar] [CrossRef]
- Rogers, J.P.; Chesney, E.; Oliver, D.; Pollak, T.A.; McGuire, P.; Fusar-Poli, P.; Zandi, M.S.; Lewis, G.; David, A.S. Psychiatric and neuropsychiatric presentations associated with severe coronavirus infections: A systematic review and meta-analysis with comparison to the COVID-19 pandemic. Lancet Psychiatry 2020, 7, 611–627. [Google Scholar] [CrossRef]
- Kim, J.W.; Stewart, R.; Kang, S.J.; Jung, S.I.; Kim, S.W.; Kim, J.M. Telephone based Interventions for Psychological Problems in Hospital Isolated Patients with COVID-19. Clin. Psychopharmacol. Neurosci. Off. Sci. J. Korean Coll. Neuropsychopharmacol. 2020, 18, 616–620. [Google Scholar] [CrossRef] [PubMed]
- Bellizzi, S.; Pichierri, G.; Farina, G.; Cegolon, L.; Abdelbaki, W. Violence Against Healthcare: A Public Health Issue beyond Conflict Settings. Am. J. Trop. Med. Hyg. 2021, 106, 15–16. [Google Scholar] [CrossRef] [PubMed]
- Epstein, D.; Andrawis, W.; Lipsky, A.M.; Ziad, H.A.; Matan, M. Anxiety and Suicidality in a Hospitalized Patient with COVID-19 Infection. Eur. J. Case Rep. Intern. Med. 2020, 7, 001651. [Google Scholar] [CrossRef] [PubMed]
- Park, H.Y.; Jung, J.; Park, H.Y.; Lee, S.H.; Kim, E.S.; Kim, H.B.; Song, K.H. Psychological Consequences of Survivors of COVID-19 Pneumonia 1 Month after Discharge. J. Korean Med. Sci. 2020, 35, e409. [Google Scholar] [CrossRef]
- Kang, E.; Lee, S.Y.; Kim, M.S.; Jung, H.; Kim, K.H.; Kim, K.N.; Park, H.Y.; Lee, Y.J.; Cho, B.; Sohn, J.H. The Psychological Burden of COVID-19 Stigma: Evaluation of the Mental Health of Isolated Mild Condition COVID-19 Patients. J. Korean Med. Sci. 2021, 36, e33. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.C.; Yoo, S.Y.; Lee, B.H.; Lee, S.H.; Shin, H.S. Psychiatric Findings in Suspected and Confirmed Middle East Respiratory Syndrome Patients Quarantined in Hospital: A Retrospective Chart Analysis. Psychiatry Investig. 2018, 15, 355–360. [Google Scholar] [CrossRef]
- Kroenke, K.; Spitzer, R.L.; Williams, J.B. The PHQ-9: Validity of a brief depression severity measure. J. Gen. Intern. Med. 2001, 16, 606–613. [Google Scholar] [CrossRef]
- Lee, S.; Huh, Y.; Kim, J. Finding optimal cut off points of the Korean version of the Patient Health Questionnaire-9 (PHQ-9) for screening depressive disorders. Mood Emot. 2014, 12, 32–36. [Google Scholar]
- Shin, J.-H.; Kim, H.-C.; Jung, C.-H.; Kim, J.-B.; Jung, S.-W.; Cho, H.-J.; Jung, S.-h. The Standardization of the Korean Version of the Patient Health Questionnaire-2. J. Korean Neuropsychiatr. Assoc. 2013, 52, 115–121. [Google Scholar] [CrossRef] [Green Version]
- Lee, S.H.; Shin, C.; Kim, H.; Jeon, S.W.; Yoon, H.K.; Ko, Y.H.; Pae, C.U.; Han, C. Validation of the Korean version of the Generalized Anxiety Disorder 7 self-rating Scale. Asia-Pac. Psychiatry Off. J. Pac. Rim Coll. Psychiatr. 2020, e12421. [Google Scholar] [CrossRef]
- Jung, Y.E.; Kim, D.; Kim, W.H.; Roh, D.; Chae, J.H.; Park, J.E. A Brief Screening Tool for PTSD: Validation of the Korean Version of the Primary Care PTSD Screen for DSM-5 (K-PC-PTSD-5). J. Korean Med. Sci. 2018, 33, e338. [Google Scholar] [CrossRef] [PubMed]
- Blevins, C.A.; Weathers, F.W.; Davis, M.T.; Witte, T.K.; Domino, J.L. The Posttraumatic Stress Disorder Checklist for DSM-5 (PCL-5): Development and Initial Psychometric Evaluation. J. Trauma. Stress 2015, 28, 489–498. [Google Scholar] [CrossRef] [PubMed]
- Dube, P.; Kurt, K.; Bair, M.J.; Theobald, D.; Williams, L.S. The p4 screener: Evaluation of a brief measure for assessing potential suicide risk in 2 randomized effectiveness trials of primary care and oncology patients. Prim. Care Companion J. Clin. Psychiatry 2010, 12. [Google Scholar] [CrossRef] [PubMed]
- Charlson, M.E.; Charlson, R.E.; Peterson, J.C.; Marinopoulos, S.S.; Briggs, W.M.; Hollenberg, J.P. The Charlson comorbidity index is adapted to predict costs of chronic disease in primary care patients. J. Clin. Epidemiol. 2008, 61, 1234–1240. [Google Scholar] [CrossRef] [PubMed]
- Taquet, M.; Luciano, S.; Geddes, J.R.; Harrison, P.J. Bidirectional associations between COVID-19 and psychiatric disorder: Retrospective cohort studies of 62 354 COVID-19 cases in the USA. Lancet Psychiatry 2021, 8, 130–140. [Google Scholar] [CrossRef]
- Tyrer, P. COVID-19 health anxiety. World Psychiatry Off. J. World Psychiatr. Assoc. 2020, 19, 307–308. [Google Scholar] [CrossRef]
- Sahoo, S.; Mehra, A.; Suri, V.; Malhotra, P.; Yaddanapudi, L.N.; Dutt Puri, G.; Grover, S. Lived experiences of the corona survivors (patients admitted in COVID wards): A narrative real-life documented summaries of internalized guilt, shame, stigma, anger. Asian J. Psychiatry 2020, 53, 102187. [Google Scholar] [CrossRef] [PubMed]
- Bastiani, L.; Fortunato, L.; Pieroni, S.; Bianchi, F.; Adorni, F.; Prinelli, F.; Giacomelli, A.; Pagani, G.; Maggi, S.; Trevisan, C.; et al. Rapid COVID-19 Screening Based on Self-Reported Symptoms: Psychometric Assessment and Validation of the EPICOVID19 Short Diagnostic Scale. J. Med. Internet Res. 2021, 23, e23897. [Google Scholar] [CrossRef] [PubMed]
- Mansbach, W.E.; Mace, R.A.; Tanner, M.A. A New Tool for Detecting COVID-19 Psychological Burden Among Postacute and Long-term Care Residents (Mood-5 Scale): Observational Study. JMIR Aging 2021, 4, e26340. [Google Scholar] [CrossRef]
- Niedzwiedz, C.L.; Green, M.J.; Benzeval, M.; Campbell, D.; Craig, P.; Demou, E.; Leyland, A.; Pearce, A.; Thomson, R.; Whitley, E.; et al. Mental health and health behaviours before and during the initial phase of the COVID-19 lockdown: Longitudinal analyses of the UK Household Longitudinal Study. J. Epidemiol. Community Health 2021, 75, 224–231. [Google Scholar] [CrossRef] [PubMed]
- Ann-Yi, S.; Bruera, E.; Wu, J.; Liu, D.D.; Agosta, M.; Williams, J.L.; Balankari, V.R.; Carmack, C.L. Characteristics and Outcomes of Psychology Referrals in a Palliative Care Department. J. Pain Symptom Manag. 2018, 56, 344–351. [Google Scholar] [CrossRef]
- Hao, F.; Tam, W.; Hu, X.; Tan, W.; Jiang, L.; Jiang, X.; Zhang, L.; Zhao, X.; Zou, Y.; Hu, Y.; et al. A quantitative and qualitative study on the neuropsychiatric sequelae of acutely ill COVID-19 inpatients in isolation facilities. Transl. Psychiatry 2020, 10, 355. [Google Scholar] [CrossRef]
- Hu, Y.; Chen, Y.; Zheng, Y.; You, C.; Tan, J.; Hu, L.; Zhang, Z.; Ding, L. Factors related to mental health of inpatients with COVID-19 in Wuhan, China. Brain Behav. Immun. 2020, 89, 587–593. [Google Scholar] [CrossRef]
- Zhang, Z.; Feng, Y.; Song, R.; Yang, D.; Duan, X. Prevalence of psychiatric diagnosis and related psychopathological symptoms among patients with COVID-19 during the second wave of the pandemic. Glob. Health 2021, 17, 44. [Google Scholar] [CrossRef] [PubMed]
- Sepulveda-Loyola, W.; Rodriguez-Sanchez, I.; Perez-Rodriguez, P.; Ganz, F.; Torralba, R.; Oliveira, D.V.; Rodriguez-Manas, L. Impact of Social Isolation Due to COVID-19 on Health in Older People: Mental and Physical Effects and Recommendations. J. Nutr. Health Aging 2020, 24, 938–947. [Google Scholar] [CrossRef] [PubMed]
- Adhanom Ghebreyesus, T. Addressing mental health needs: An integral part of COVID-19 response. World Psychiatry Off. J. World Psychiatr. Assoc. 2020, 19, 129–130. [Google Scholar] [CrossRef] [PubMed]
- Stewart, D.E.; Appelbaum, P.S. COVID-19 and psychiatrists’ responsibilities: A WPA position paper. World Psychiatry Off. J. World Psychiatr. Assoc. 2020, 19, 406–407. [Google Scholar] [CrossRef] [PubMed]
- McDaid, D. Viewpoint: Investing in strategies to support mental health recovery from the COVID-19 pandemic. Eur. Psychiatry J. Assoc. Eur. Psychiatr. 2021, 64, e32. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Overall (n = 130) | Newly Developed Mental Disorders | p Value | ||
|---|---|---|---|---|
| Yes (n = 29) | No (n = 101) | |||
| Age, year | 40 (28–61) | 58 (35–68) | 40 (27–58) | 0.031 |
| Sex | ||||
| Male | 87 (66.9) | 18 (62.1) | 69 (68.3) | 0.528 |
| Female | 43 (33.1) | 11 (37.9) | 32 (31.7) | |
| Marital status | ||||
| Single | 56 (43.1) | 8 (27.6) | 48 (47.5) | 0.056 |
| Married | 74 (56.9) | 21 (72.4)) | 53 (52.5) | |
| Education level | ||||
| High school and under | 65 (50.0) | 19 (65.5) | 46 (45.5) | 0.058 |
| University and higher | 65 (50.0) | 10 (34.5) | 55 (54.5) | |
| Occupation | ||||
| Unemployed | 58 (44.6) | 13 (44.8) | 45 (44.6) | 0.979 |
| Employed | 72 (55.4) | 16 (55.2) | 56 (55.4) | |
| CCI score | ||||
| 0 | 99 (76.2) | 16 (55.2) | 83 (82.2) | 0.006 * |
| 1–2 | 27 (20.8) | 12 (41.4) | 15 (14.9) | |
| 3–4 | 0 (0) | 0 (0) | 0 (0) | |
| ≥5 | 4 (3.1) | 1 (3.5) | 3 (3.0) | |
| Presence of pneumonia on admission | ||||
| No | 48 (36.9) | 6 (20.7) | 42 (41.6) | 0.040 |
| Yes | 82 (63.1) | 23 (79.3) | 59 (58.4) | |
| Oxygen therapy | ||||
| No | 113 (86.9) | 20 (69.0) | 93 (92.1) | 0.003 * |
| Yes | 17 (13.1) | 9 (31.0) | 8 (7.9) | |
| Nasal cannula or simple facial mask | 14 (10.8) | 7 (24.1) | 7 (6.9) | |
| HFNC or ventilator | 3 (2.3) | 2 (6.9) | 1 (1.0) | |
| ICU admission | ||||
| No | 120 (92.3) | 24 (82.8) | 96 (95.0) | 0.029 |
| Yes | 10 (7.7) | 5 (17.2) | 5 (5.0) | |
| Hospital length of stay, days | 31 (18–43) | 44 (33–54) | 26 (16–39) | <0.001 |
| <28 | 59 (45.4) | 5 (17.2) | 54 (53.5) | 0.001 |
| ≥28 | 71 (54.6) | 24 (82.8) | 47 (46.5) | |
| Overall n = 130 | Newly Developed Mental Disorder | p Value | ||
|---|---|---|---|---|
| Yes n = 29 | No n = 101 | |||
| Depressive symptom | ||||
| PHQ-2 (n = 17) | 1 (0–2) | 1 (0–2) | 1 (0–2) | 0.733 |
| PHQ-9 (n = 113) | 3 (0–7) | 8 (3–14) | 3 (0–5) | 0.002 |
| Yes * | 23 (17.7) | 11 (37.9) | 12 (11.9) | |
| No | 107 (82.3) | 18 (62.1) | 89 (88.1) | 0.001 |
| PTSD symptom | ||||
| PC-PTSD (n = 17) | 1 (0–2) | 1 (0–1) | 1 (1–3) | 0.180 |
| PCL-5 (n = 113) | 3 (0–10) | 7 (1–20) | 2 (0–7) | 0.047 |
| Yes † | 7 (5.4) | 0 (0.0) | 7 (6.9) | |
| No | 123 (94.6) | 29 (100.0) | 94 (93.1) | 0.145 |
| Suicide idea | ||||
| Yes | 4 (3.1) | 2 (6.9) | 2 (2.0) | |
| No | 126 (96.9) | 27 (93.1) | 99 (98.0) | 0.177 |
| Number (%) | |
|---|---|
| New-onset mental disorders | |
| Delirium | 2 (6.9) |
| Panic disorder | 3 (10.3) |
| Adjustment disorder | 14 (48.3) |
| Insomnia | 10 (34.5) |
| Psychotropic medications * | |
| Antipsychotics | 7 (20.5) |
| Antidepressants | 9 (23.1) |
| Antianxieties | 20 (53.8) |
| Univariate Analysis | Multivariate Analysis | |||
|---|---|---|---|---|
| OR (95% CI) | p Value | OR (95% CI) | p Value | |
| Age, years * | 1.027 (1.004–1.051) | 0.020 | ||
| Female sex (vs. male) | 1.318 (0.558–-3.112) | 0.529 | ||
| Low education level (vs. high) | 2.272 (0.961–5.369) | 0.062 | ||
| Unemployed (vs. employed) | 1.011 (0.441–2.320) | 0.9792 | ||
| CCI score ≥ 1 (vs. 0) | 3.747 (1.536–9.140) | 0.004 | 5.115 (1.737–15.058) | 0.003 |
| Pneumonia (vs. no) | 2.729 (1.022–7.283) | 0.045 | ||
| Hospital length of stay, days † | 1.059 (1.030–1.089) | <0.001 | 1.067 (1.035–1.100) | <0.001 |
| Oxygen therapy (vs. no) | 5.231 (1.798–15.219) | 0.002 | ||
| ICU admission (vs. no) | 4.000 (1.071–14.941) | 0.039 | ||
| Depressive symptom ‡ (vs. no) | 4.532 (1.732–11.864) | 0.002 | 5.357 (1.745–16.444) | 0.003 |
| PTSD symptom ‡ (vs. no) | <0.001 | >999.999 | ||
| Suicide idea ‡ (vs. no) | 3.667 (0.493–27.246) | 0.204 | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, J.; Seo, Y.E.; Sung, H.K.; Park, H.Y.; Han, M.H.; Lee, S.H. Predictors of the Development of Mental Disorders in Hospitalized COVID-19 Patients without Previous Psychiatric History: A Single-Center Retrospective Study in South Korea. Int. J. Environ. Res. Public Health 2022, 19, 1092. https://doi.org/10.3390/ijerph19031092
Kim J, Seo YE, Sung HK, Park HY, Han MH, Lee SH. Predictors of the Development of Mental Disorders in Hospitalized COVID-19 Patients without Previous Psychiatric History: A Single-Center Retrospective Study in South Korea. International Journal of Environmental Research and Public Health. 2022; 19(3):1092. https://doi.org/10.3390/ijerph19031092
Chicago/Turabian StyleKim, Jangrae, Yae Eun Seo, Ho Kyung Sung, Hye Yoon Park, Myung Hwa Han, and So Hee Lee. 2022. "Predictors of the Development of Mental Disorders in Hospitalized COVID-19 Patients without Previous Psychiatric History: A Single-Center Retrospective Study in South Korea" International Journal of Environmental Research and Public Health 19, no. 3: 1092. https://doi.org/10.3390/ijerph19031092