
Dynamics and Determinants of SARS-CoV-2 RT-PCR Testing on Symptomatic Individuals Attending Healthcare Centers during 2020 in Bahia, Brazil

 ,
,  , , ,
, , , {kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
2.1. RT-PCR Full Dataset from Bahia
2.2. RT-PCR Sub Datasets from Bahia
2.3. SARS-CoV-2 Time Series from Brazil
2.4. Modelling RT-PCR Results
3. Results
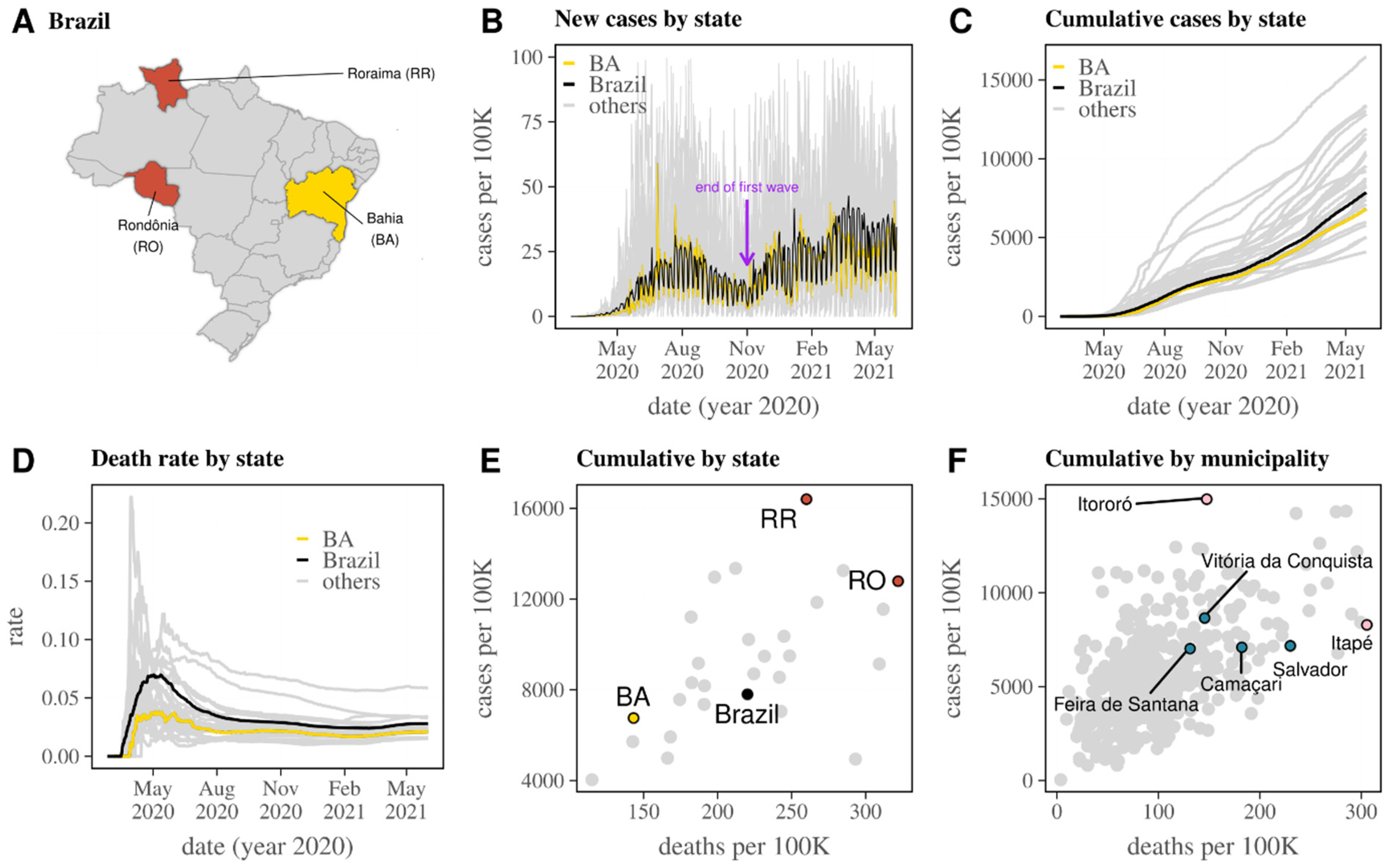
3.1. Reported SARS-CoV-2 Epidemic in Brazil and Bahia
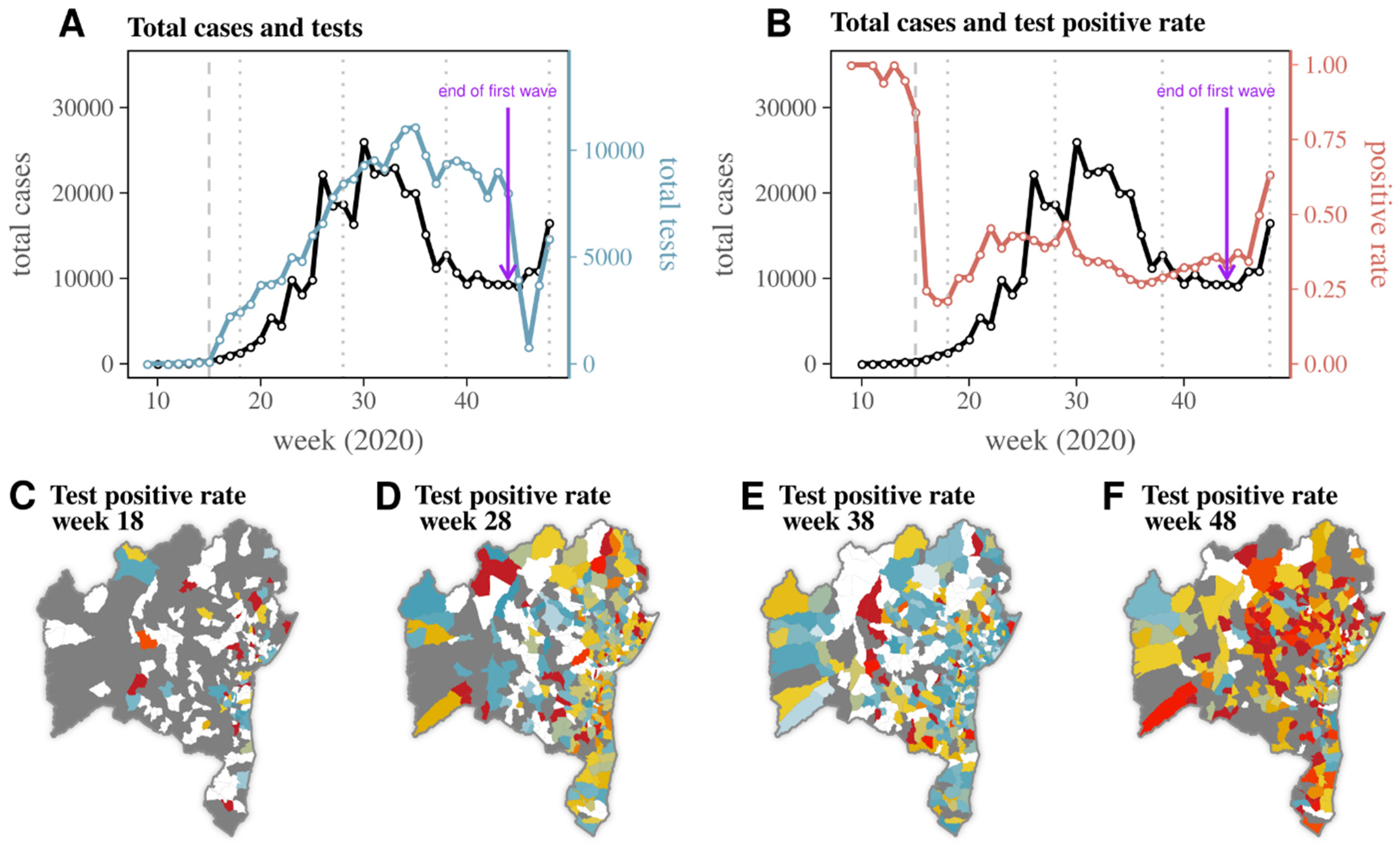
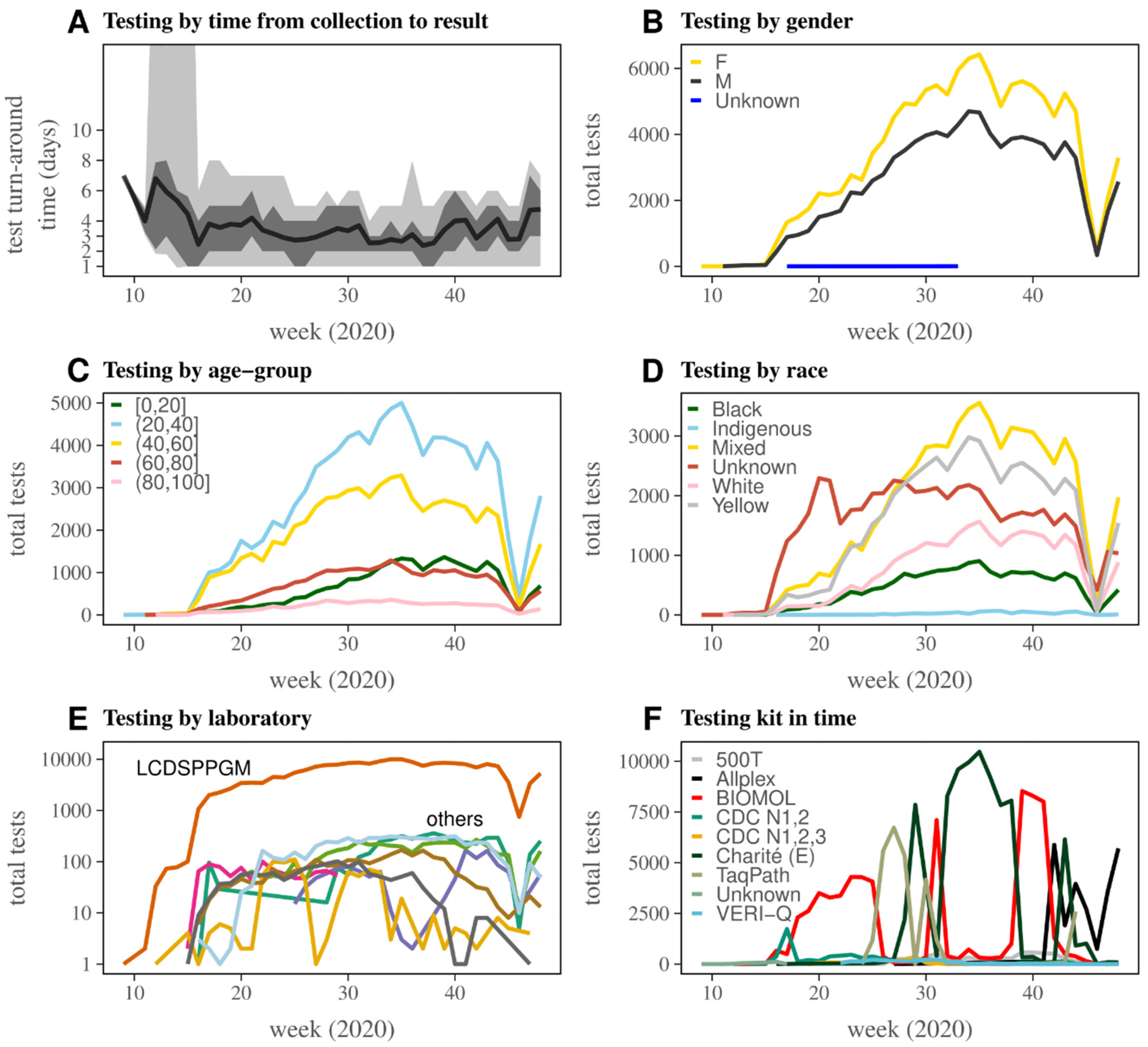
3.2. Dynamics of SARS-CoV-2 RT-PCR Testing in Bahia
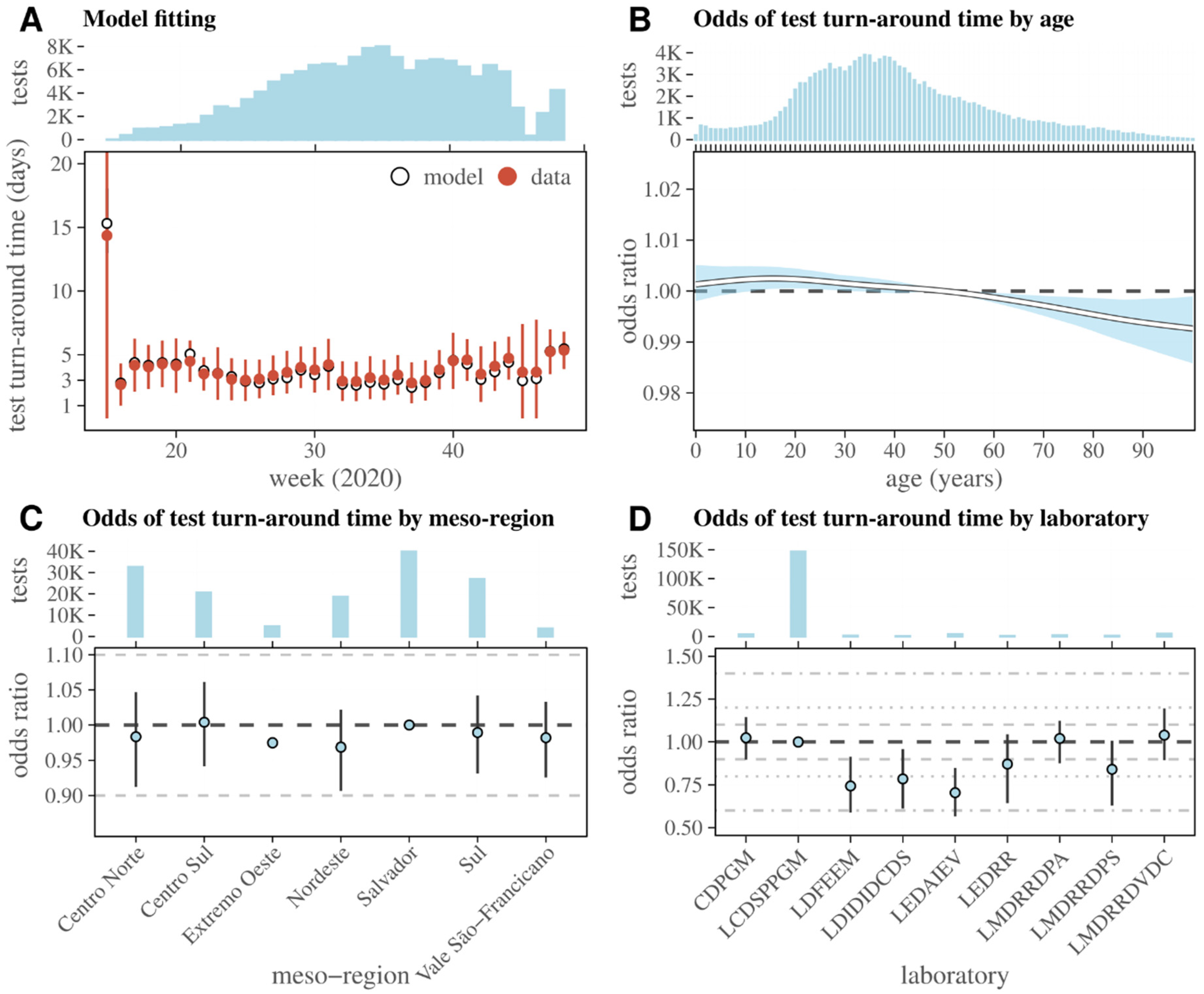
3.3. Dynamics of RT-PCR Test Turn-Around Time in Bahia
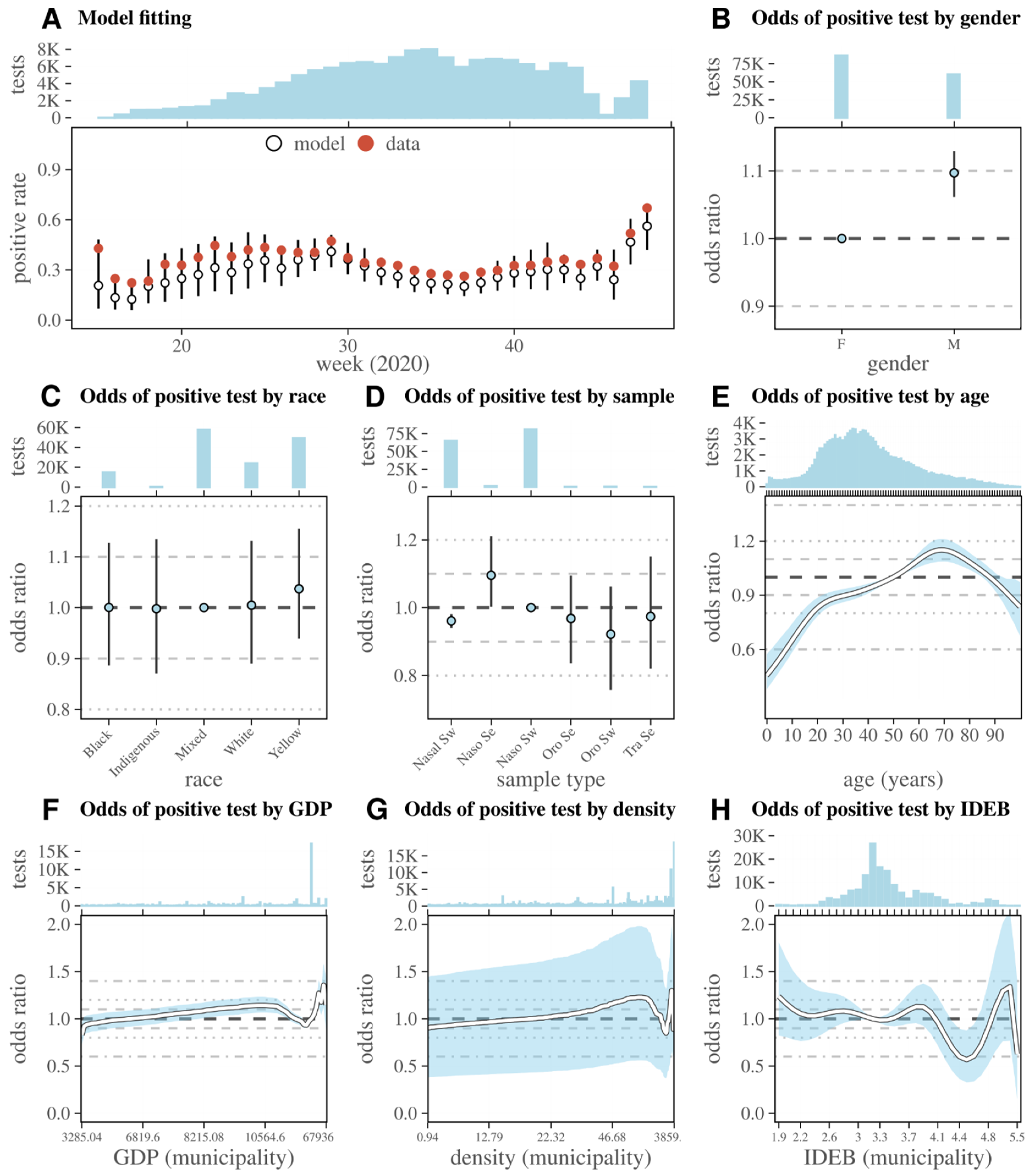
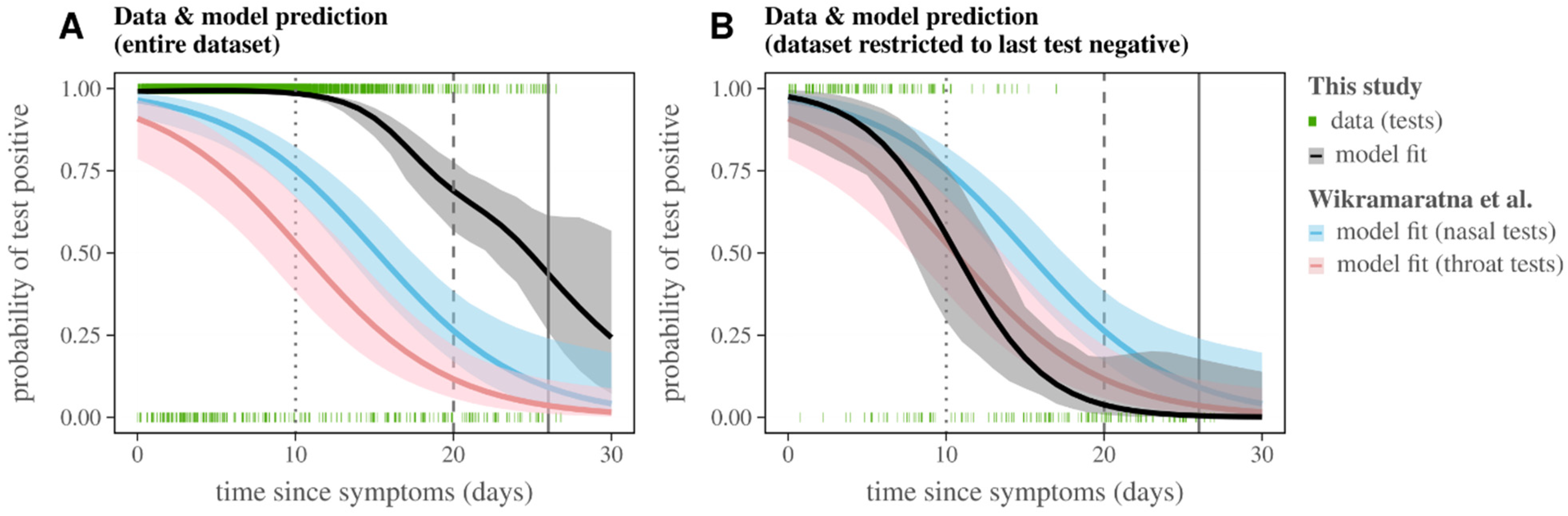
3.4. Probability of RT-PCR Positive Test by Time from Symptom Onset
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Zhou, W.; Wang, W.; Wang, H.; Lu, R.; Tan, W. First infection by all four non-severe acute respiratory syndrome human coronaviruses takes place during childhood. BMC Infect. Dis. 2013, 13, 433. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Walsh, E.E.; Shin, J.H.; Falsey, A.R. Clinical impact of human coronaviruses 229E and OC43 infection in diverse adult populations. J. Infect. Dis. 2013, 208, 1634–1642. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hu, B.; Guo, H.; Zhou, P.; Shi, Z.-L. Characteristics of SARS-CoV-2 and COVID-19. Nat. Rev. Microbiol. 2021, 19, 141–154. [Google Scholar] [CrossRef] [PubMed]
- Wang, C.; Wang, Z.; Wang, G.; Lau, J.Y.-N.; Zhang, K.; Li, W. COVID-19 in early 2021: Current status and looking forward. Signal. Transduct. Target Ther. 2021, 6, 114. [Google Scholar] [CrossRef]
- Zhou, P.; Yang, X.-L.; Wang, X.-G.; Hu, B.; Zhang, L.; Zhang, W.; Si, H.-R.; Zhu, Y.; Li, B.; Huang, C.-L.; et al. A pneumonia outbreak associated with a new coronavirus of probable bat origin. Nature 2020, 579, 270–273. [Google Scholar] [CrossRef] [Green Version]
- Coronavirus Disease (COVID-19) Situation Reports. Available online: https://www.who.int/emergencies/diseases/novel-coronavirus-2019/situation-reports (accessed on 14 October 2020).
- Fontanet, A.; Autran, B.; Lina, B.; Kieny, M.P.; Karim, S.S.A.; Sridhar, D. SARS-CoV-2 variants and ending the COVID-19 pandemic. Lancet 2021, 397, 952–954. [Google Scholar] [CrossRef]
- Kelvin, A.A.; Halperin, S. COVID-19 in children: The link in the transmission chain. Lancet Infect. Dis. 2020, 20, 633–634. [Google Scholar] [CrossRef] [Green Version]
- Taylor, L. Covid-19: Brazil’s spiralling crisis is increasingly affecting young people. BMJ 2021, 373, n879. [Google Scholar] [CrossRef]
- Kakodkar, P.; Kaka, N.; Baig, M.N. A Comprehensive Literature Review on the Clinical Presentation, and Management of the Pandemic Coronavirus Disease 2019 (COVID-19). Cureus 2020, 12, e7560. [Google Scholar] [CrossRef] [Green Version]
- Mahmoudi, S.; Rezaei, M.; Mansouri, N.; Marjani, M.; Mansouri, D. Immunologic Features in Coronavirus Disease 2019: Functional Exhaustion of T Cells and Cytokine Storm. J. Clin. Immunol. 2020, 40, 974–976. [Google Scholar] [CrossRef]
- Amore, S.; Puppo, E.; Melara, J.; Terracciano, E.; Gentili, S.; Liotta, G. Impact of COVID-19 on older adults and role of long-term care facilities during early stages of epidemic in Italy. Sci. Rep. 2021, 11, 12530. [Google Scholar] [CrossRef] [PubMed]
- Kubina, R.; Dziedzic, A. Molecular and Serological Tests for COVID-19 a Comparative Review of SARS-CoV-2 Coronavirus Laboratory and Point-of-Care Diagnostics. Diagnostics 2020, 10, 434. [Google Scholar] [CrossRef]
- Vogels, C.B.F.; Brito, A.F.; Wyllie, A.L.; Fauver, J.R.; Ott, I.M.; Kalinich, C.C.; Petrone, M.E.; Casanovas-Massana, A.; Muenker, M.C.; Moore, A.J.; et al. Analytical sensitivity and efficiency comparisons of SARS-CoV-2 RT-qPCR primer-probe sets. Nat. Microbiol. 2020, 5, 1299–1305. [Google Scholar] [CrossRef] [PubMed]
- Kevadiya, B.D.; Machhi, J.; Herskovitz, J.; Oleynikov, M.D.; Blomberg, W.R.; Bajwa, N.; Soni, D.; Das, S.; Hasan, M.; Patel, M.; et al. Diagnostics for SARS-CoV-2 infections. Nat. Mater. 2021, 20, 593–605. [Google Scholar] [CrossRef] [PubMed]
- Xavier, J.; Giovanetti, M.; Adelino, T.; Fonseca, V.; da Costa, A.V.B.; Ribeiro, A.A.; Felicio, K.N.; Duarte, C.G.; Silva, M.V.F.; Salgado, Á.; et al. The ongoing COVID-19 epidemic in Minas Gerais, Brazil: Insights from epidemiological data and SARS-CoV-2 whole genome sequencing. Emerg. Microbes Infect. 2020, 9, 1824–1834. [Google Scholar] [CrossRef] [PubMed]
- Smyrlaki, I.; Ekman, M.; Lentini, A.; de Sousa, N.R.; Papanicolaou, N.; Vondracek, M.; Aarum, J.; Safari, H.; Muradrasoli, S.; Rothfuchs, A.G.; et al. Massive and rapid COVID-19 testing is feasible by extraction-free SARS-CoV-2 RT-PCR. Nat. Commun. 2020, 11, 4812. [Google Scholar] [CrossRef]
- Corman, V.M.; Landt, O.; Kaiser, M.; Molenkamp, R.; Meijer, A.; Chu, D.K.W.; Bleicker, T.; Brünink, S.; Schneider, J.; Schmidt, M.L.; et al. Detection of 2019 novel coronavirus (2019-nCoV) by real-time RT-PCR. Eurosurveillance 2020, 25, 2000045. [Google Scholar] [CrossRef] [Green Version]
- Ministério da Saúde (Brazilian Ministry of Health, PT). Ministério da Saúde. Boletim Epidemiológico Especial-14/SE 18-26 de abril de 2020 COE-COVID19. 2020.
- Giovanetti, M.; Slavov, S.N.; Fonseca, V.; Wilkinson, E.; Tegally, H.; Patané, J.S.L.; Viala, V.L.; San, J.E.; Rodrigues, E.S.; Santos, E.V.; et al. Genomic epidemiology reveals how restriction measures shaped the SARS-CoV-2 epidemic in Brazil. bioRxiv 2021. [Google Scholar] [CrossRef]
- Candido, D.D.S.; Watts, A.; Abade, L.; Kraemer, M.U.G.; Pybus, O.G.; Croda, J.; de Oliveira, W.; Khan, K.; Sabino, E.C.; Faria, N.R. Routes for COVID-19 importation in Brazil. J. Travel Med. 2020, 27, taaa042. [Google Scholar] [CrossRef] [Green Version]
- Candido, D.S.; Claro, I.M.; de Jesus, J.G.; Souza, W.M.; Moreira, F.R.; Dellicour, S.; Mellan, T.A.; du Plessis, L.; Pereira, R.H.M.; Sales, F.C.S.; et al. Evolution and epidemic spread of SARS-CoV-2 in Brazil. Science 2020, 369, 1255–1260. [Google Scholar] [CrossRef]
- Hallal, P.C.; Hartwig, F.P.; Horta, B.L.; Silveira, M.F.; Struchiner, C.J.; Vidaletti, L.P.; Neumann, N.A.; Pellanda, L.C.; Dellagostin, O.A.; Burattini, M.N.; et al. SARS-CoV-2 antibody prevalence in Brazil: Results from two successive nationwide serological household surveys. Lancet Glob. Health 2020, 8, e1390–e1398. [Google Scholar] [CrossRef]
- Sabino, E.C.; Buss, L.F.; Carvalho, M.P.S.; Prete, C.A., Jr.; Crispim, M.A.E.; Fraiji, N.A.; Pereira, R.H.M.; Parag, K.V.; da Silva Peixoto, P.; Kraemer, M.U.G.; et al. Resurgence of COVID-19 in Manaus, Brazil, despite high seroprevalence. Lancet 2021, 397, 452–455. [Google Scholar] [CrossRef]
- Coronavírus Brasil. Available online: https://covid.saude.gov.br (accessed on 4 November 2020).
- Carvalho, T.A.; Boschiero, M.N.; Marson, F.A.L. COVID-19 in Brazil: 150,000 deaths and the Brazilian underreporting. Diagn. Microbiol. Infect. Dis. 2020, 99, 115258. [Google Scholar] [CrossRef] [PubMed]
- E Silva, L.V.; de Andrade Abi, M.D.P.; Dos Santos, A.M.T.B.; de Mattos Teixeira, C.A.; Gomes, V.H.M.; Cardoso, E.H.S.; da Silva, M.S.; Vijaykumar, N.L.; Carvalho, S.V.; de Carvalho, A.P.d.F.; et al. COVID-19 Mortality Underreporting in Brazil: Analysis of Data from Government Internet Portals. J. Med. Internet Res. 2020, 22, e21413. [Google Scholar] [CrossRef]
- do Prado, M.F.; Antunes, B.B.d.P.; Bastos, L.D.S.L.; Peres, I.T.; Silva, A.d.A.B.; da Dantas, L.F.; Baião, F.A.; Maçaira, P.; Hamacher, S.; Bozza, F.A. Analysis of COVID-19 under-reporting in Brazil. Rev. Bras. Ter. Intensiva 2020, 32, 224–228. [Google Scholar] [CrossRef] [PubMed]
- Baqui, P.; Bica, I.; Marra, V.; Ercole, A.; van der Schaar, M. Ethnic and regional variations in hospital mortality from COVID-19 in Brazil: A cross-sectional observational study. Lancet Glob. Health 2020, 8, e1018–e1026. [Google Scholar] [CrossRef]
- De Souza, C.D.F.; de Souza, C.D.F.; Machado, M.F.; do Carmo, R.F. Human development, social vulnerability and COVID-19 in Brazil: A study of the social determinants of health. Infect. Dis. Poverty 2020, 9, 50–59. [Google Scholar] [CrossRef]
- Fortaleza, C.M.C.B.; CM, C.; Guimarães, R.B.; de Almeida, G.B.; Pronunciate, M.; Ferreira, C.P. Taking the inner route: Spatial and demographic factors affecting vulnerability to COVID-19 among 604 cities from inner São Paulo State, Brazil. Epidemiol. Infect. 2020, 148, e118. [Google Scholar] [CrossRef]
- Ribeiro, H.V.; Sunahara, A.S.; Sutton, J.; Perc, M.; Hanley, Q.S. City size and the spreading of COVID-19 in Brazil. PLoS ONE 2020, 15, e0239699. [Google Scholar] [CrossRef]
- Barone, M.T.U.; Harnik, S.B.; de Luca, P.V.; Martins, C. The impact of COVID-19 on people with diabetes in Brazil. Diabetes Res. Clin. Pract. 2020, 166, 108304. [Google Scholar] [CrossRef]
- Passos, L.; Prazeres, F.; Teixeira, A.; Martins, C. Impact on Mental Health Due to COVID-19 Pandemic: Cross-Sectional Study in Portugal and Brazil. Int. J. Environ. Res. Public Health 2020, 17, 6794. [Google Scholar] [CrossRef] [PubMed]
- Goularte, J.F.; Serafim, S.D.; Colombo, R.; Hogg, B.; Caldieraro, M.A.; Rosa, A.R. COVID-19 and mental health in Brazil: Psychiatric symptoms in the general population. J. Psychiatr. Res. 2020, 132, 32–37. [Google Scholar] [CrossRef] [PubMed]
- Bahia Confirma Primeiro Caso Importado do Novo Coronavírus (Covid-19). Available online: http://www.saude.ba.gov.br/2020/03/06/bahia-confirma-primeiro-caso-importado-do-novo-coronavirus-covid-19/ (accessed on 4 November 2020).
- Sistema IBGE de Recuperação Automática—SIDRA. In Brazilian Institute of Geography and Statistics. Available online: https://sidra.ibge.gov.br/ (accessed on 9 November 2020). (In Portuguese)
- Wikramaratna, P.; Paton, R.S.; Ghafari, M.; Lourenco, J. Estimating false-negative detection rate of SARS-CoV-2 by RT-PCR. MedRxiv 2020. [Google Scholar] [CrossRef]
- Kucirka, L.M.; Lauer, S.A.; Laeyendecker, O.; Boon, D.; Lessler, J. Variation in False-Negative Rate of Reverse Transcriptase Polymerase Chain Reaction-Based SARS-CoV-2 Tests by Time Since Exposure. Ann. Intern. Med. 2020, 173, 262–267. [Google Scholar] [CrossRef]
- The R Project for Statistical Computing. Available online: https://www.R-project.org/ (accessed on 16 October 2020).
- Pedersen, E.J.; Miller, D.L.; Simpson, G.L.; Ross, N. Hierarchical generalized additive models in ecology: An introduction with mgcv. PeerJ 2019, 7, e6876. [Google Scholar] [CrossRef] [Green Version]
- Wikramaratna, P.S.; Paton, R.S.; Ghafari, M.; Lourenço, J. Estimating the false-negative test probability of SARS-CoV-2 by RT-PCR. Eurosurveillance 2020, 25, 2000568. [Google Scholar] [CrossRef]
- Fellows, M.; Paye, V.; Alencar, A.; Nicácio, M.; Castro, I.; Coelho, M.E.; Silva, C.V.J.; Bandeira, M.; Lourival, R.; Basta, P.C. Under-Reporting of COVID-19 Cases Among Indigenous Peoples in Brazil: A New Expression of Old Inequalities. Front. Psychiatry 2021, 12, 638359. [Google Scholar] [CrossRef]
- Kupek, E. How many more? Under-reporting of the COVID-19 deaths in Brazil in 2020. Trop. Med. Int. Health 2021, 26, 1019–1028. [Google Scholar] [CrossRef]
- Jin, J.-M.; Bai, P.; He, W.; Wu, F.; Liu, X.-F.; Han, D.-M.; Liu, S.; Yang, J.-K. Gender Differences in Patients with COVID-19: Focus on Severity and Mortality. Front. Public Health 2020, 8, 152. [Google Scholar] [CrossRef]
- Peckham, H.; de Gruijter, N.M.; Raine, C.; Radziszewska, A.; Ciurtin, C.; Wedderburn, L.R.; Rosser, E.C.; Webb, K.; Deakin, C.T. Male sex identified by global COVID-19 meta-analysis as a risk factor for death and ITU admission. Nat. Commun. 2020, 11, 6317. [Google Scholar] [CrossRef]
- Boccolini, C.S.; de Souza Junior, P.R.B. Inequities in Healthcare utilization: Results of the Brazilian National Health Survey, 2013. Int. J. Equity Health 2016, 15, 150. [Google Scholar] [CrossRef] [PubMed]
- Travassos, C.; Viacava, F.; Pinheiro, R.; Brito, A. Utilização dos serviços de saúde no Brasil: Gênero, características familiares e condição social. Rev. Panam. Salud Publica 2002, 11, 365–373. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schuelter-Trevisol, F.; Raimundo, L.J.; Soccas, H.D.; Antunes, A.F.; Mohr, R.L.D.; Marcon, C.E.M.; Trevisol, D.J. Assessment of patients with Covid-19 hospitalized in southern Santa Catarina. Rev. Soc. Bras. Med. Trop. 2020, 53, e20200579. [Google Scholar] [CrossRef] [PubMed]
- Feitosa, N.M.; da Costa Rodrigues, B.; Petry, A.C.; Nocchi KJ, C.V.; de Moraes Brindeiro, R.; Zilberberg, C.; Monteiro-de-Barros, C.; Mury, F.B.; de Souza-Menezes, J.; Nepomuceno-Silva, J.L.; et al. Molecular testing and analysis of disease spreading during the emergence of COVID-19 in Macaé, the Brazilian National Capital of Oil. Sci. Rep. 2021, 11, 20121. [Google Scholar] [CrossRef]
- Guedes, M.B.O.; de Assis, S.J.C.; Sanchis, G.J.B.; Araujo, D.N.; Da Costa Oliveira, A.G.R.; Lopes, J.M. COVID-19 in Brazilian cities: Impact of social determinants, coverage and quality of primary health care. PLoS ONE 2021, 16, e0257347. [Google Scholar] [CrossRef]
- Li, S.L.; Pereira, R.H.M.; Prete, C.A.; Zarebski, A.; Emanuel, L.; Alves, P.J.H.; Peixoto, P.S.; Braga, C.K.V.; Santos, A.A.D.S.; de Souza, W.M.; et al. Higher risk of death from COVID-19 in low-income and non-White populations of São Paulo, Brazil. BMJ Glob. Health 2021, 6, e004959. [Google Scholar] [CrossRef]






Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pereira, F.M.; Salomão de Araujo, A.; Catarina Martins Reis, A.; Santos da Hora, A.; Pinotti, F.; Paton, R.S.; Vilas Boas Figueiredo, C.; Lopes Damasceno, C.; Carlos dos Santos, D.; Souza de Santana, D.; et al. Dynamics and Determinants of SARS-CoV-2 RT-PCR Testing on Symptomatic Individuals Attending Healthcare Centers during 2020 in Bahia, Brazil. Viruses 2022, 14, 1549. https://doi.org/10.3390/v14071549
Pereira FM, Salomão de Araujo A, Catarina Martins Reis A, Santos da Hora A, Pinotti F, Paton RS, Vilas Boas Figueiredo C, Lopes Damasceno C, Carlos dos Santos D, Souza de Santana D, et al. Dynamics and Determinants of SARS-CoV-2 RT-PCR Testing on Symptomatic Individuals Attending Healthcare Centers during 2020 in Bahia, Brazil. Viruses. 2022; 14(7):1549. https://doi.org/10.3390/v14071549
Chicago/Turabian StylePereira, Felicidade Mota, Aline Salomão de Araujo, Ana Catarina Martins Reis, Anadilton Santos da Hora, Francesco Pinotti, Robert S. Paton, Camylla Vilas Boas Figueiredo, Caroline Lopes Damasceno, Daiana Carlos dos Santos, Daniele Souza de Santana, and et al. 2022. "Dynamics and Determinants of SARS-CoV-2 RT-PCR Testing on Symptomatic Individuals Attending Healthcare Centers during 2020 in Bahia, Brazil" Viruses 14, no. 7: 1549. https://doi.org/10.3390/v14071549