
A Blockchain and Artificial Intelligence-Based, Patient-Centric Healthcare System for Combating the COVID-19 Pandemic: Opportunities and Applications



Abstract
:1. Introduction
- We conceptually redefined the traditional healthcare model by integrating blockchain and AI for tackling COVID-19 in a patient-centric paradigm.
- We exploited the existing public health strategies, such as patient information sharing, data management for diagnosing the infection, contact tracing, monitoring, and mitigation of the impact on healthcare, using the proposed decentralized, patient-centric frameworks.
- Based on the study, we discussed the challenges, solutions, and future research directions that are anticipated to be of significant value for patients and healthcare organizations.
2. Related work
2.1. Blockchain and AI in Healthcare Systems
2.2. Trends in Related Research
3. Overview
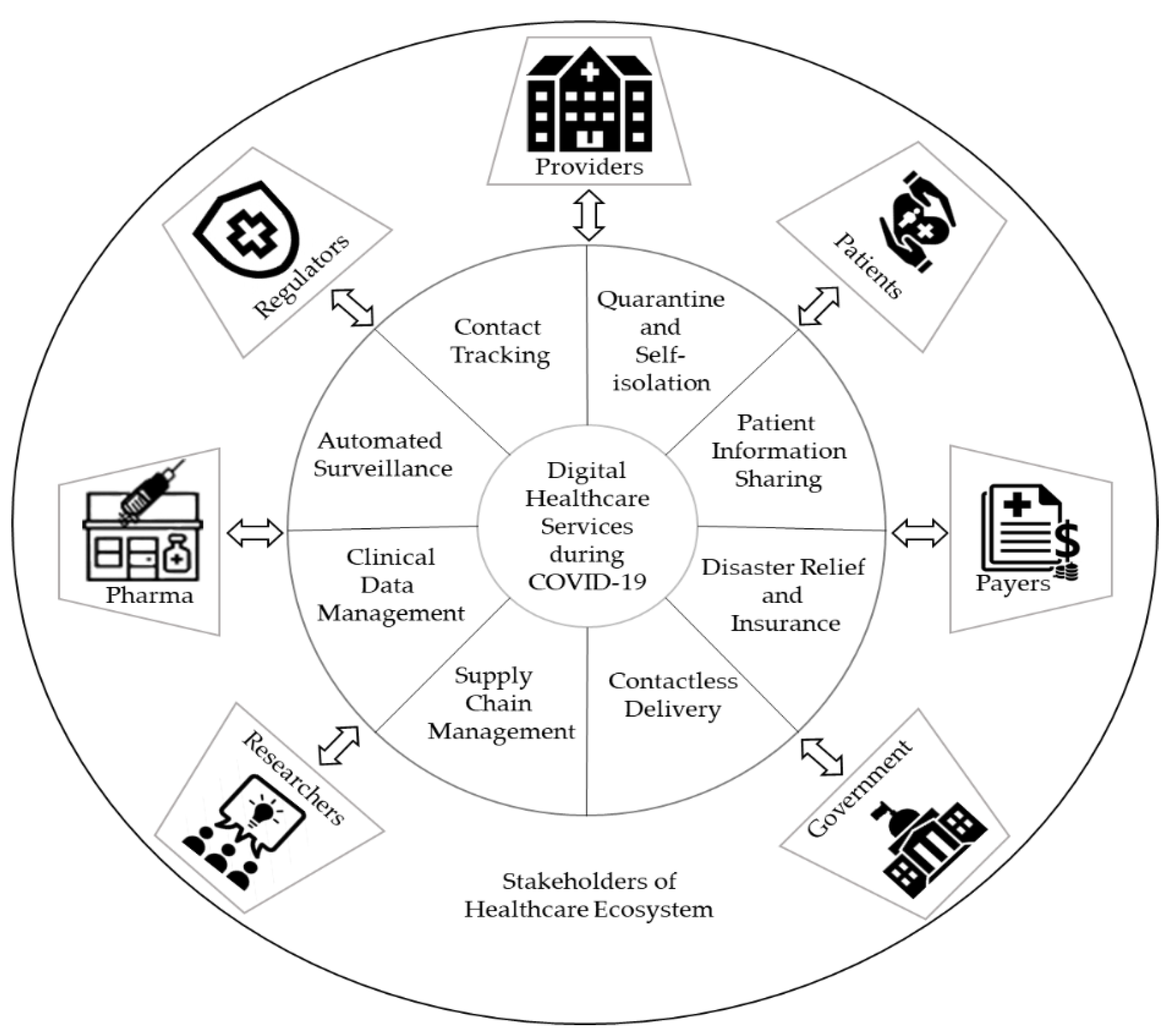
3.1. Digital Healthcare Services during the COVID-19 Pandemic
- Patient—anyone who seeks medical care can be termed a patient, and their data play a crucial role in pandemic preparedness and response.
- Providers—Includes physician groups, hospitals, laboratories, doctors, and other healthcare professionals and medical facilities that deliver medical care to patients. Patient data, such as electronic medical records (EMRs), are stored, organized, and managed in a large-scale centralized clinical repository. Providers contribute to clinical teams and researchers by providing health information to combat diseases.
- Payers—A payer is a company (for example, an insurance company) that pays people or bodies, other than the patient, to finance or refund the cost of the medicinal products and healthcare services. A payer is responsible for processing payments, patient eligibility, enrollment, and claims.
- Pharma—Pharmaceutical companies are the makers of vaccines prescribed by healthcare providers. They supply medicines and provide other supporting services, such as patient disease and medication management.
- Researchers—Conduct pharmaceutical and biomedical research. Digital healthcare can augment researchers’ insights by analyzing the healthcare data, clinical trials, and public health research.
- Regulators—Healthcare industries and government agencies that oversee industry standards, enforce and write regulations, and set healthcare policy.
- Government—Handles public safety and emergencies. It implements stay-at-home orders or lockdown to reorganize, rebalance resources, and protect health workers while combating COVID-19. They execute policies that encourage and support innovators to create healthcare solutions based on information technologies where information flows securely to the required parties. Involved in the management of the procurement of PPE kits, medicinal supplies, and appliances/oxygen condensers. Provides staff training on COVID-19 prevention and provision of patient counseling on medicines.
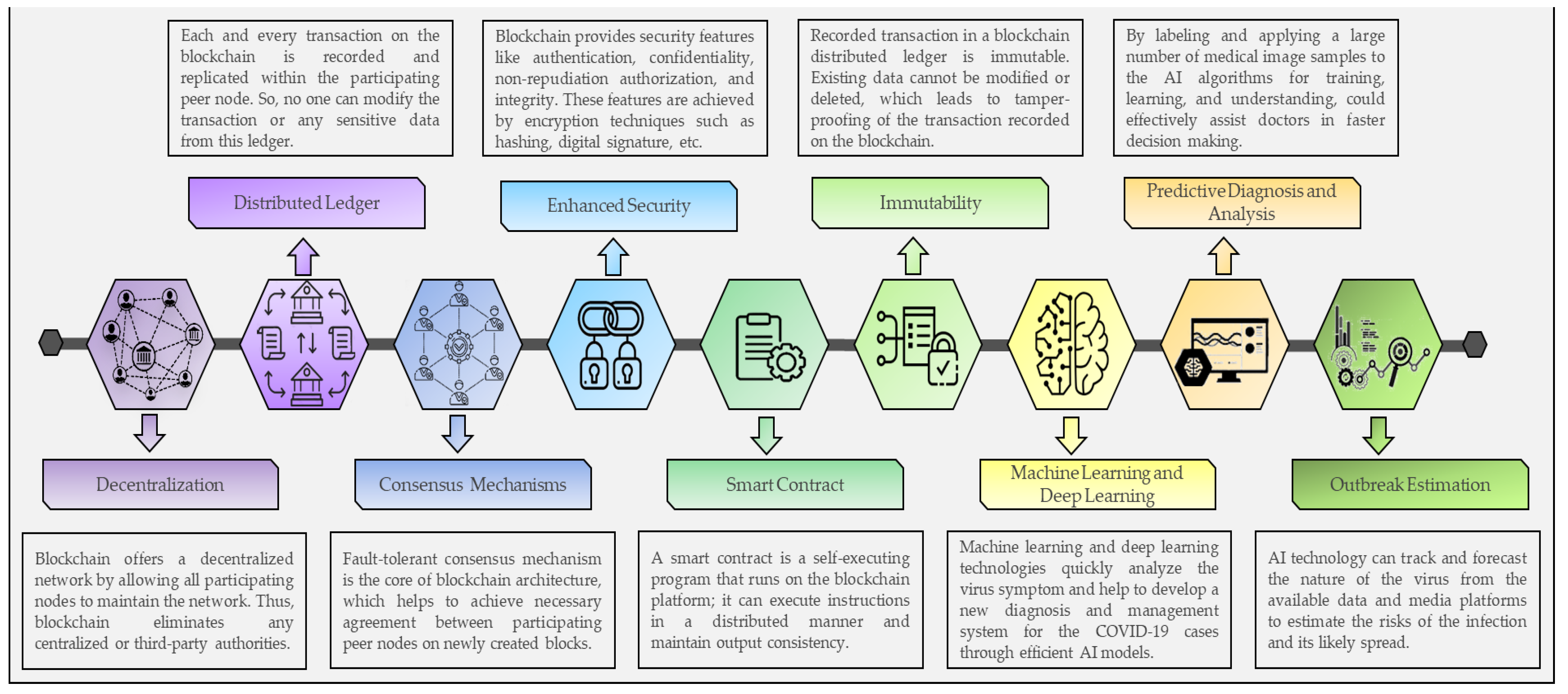
3.2. Blockchain and Artificial Intelligence Technologies
- Blockchain helps to improve interoperability among different healthcare organizational platforms, such as pharmaceutical needs, hospital databases, supply chain logistics, and insurance claims.
- Storage and management of health record data using blockchain platforms offer patients the protection of their data and provides access to their health records based upon request.
- Blockchain improves information management among stakeholders in the healthcare ecosystem.
- Blockchain reduces centralized control over patient datasets. Thus, it helps to boost medical research and treatment.
- A smart platform can be developed using AI for the automated surveillance, monitoring, detection, and prediction of the spread of this virus.
- The use of AI in reviewing and analyzing radiology images, such as CTs and X-rays, could help to increase COVID-19 detection accuracy.
- AI could automatically estimate the number of positive COVID-19 cases and death cases in any region. In addition, AI helps to determine the most virus-exposed countries, regions, and people to take measures accordingly in advance.
- The application of artificial intelligence (AI) in medication development can help pharmaceutical companies streamline drug repurposing and discovery.
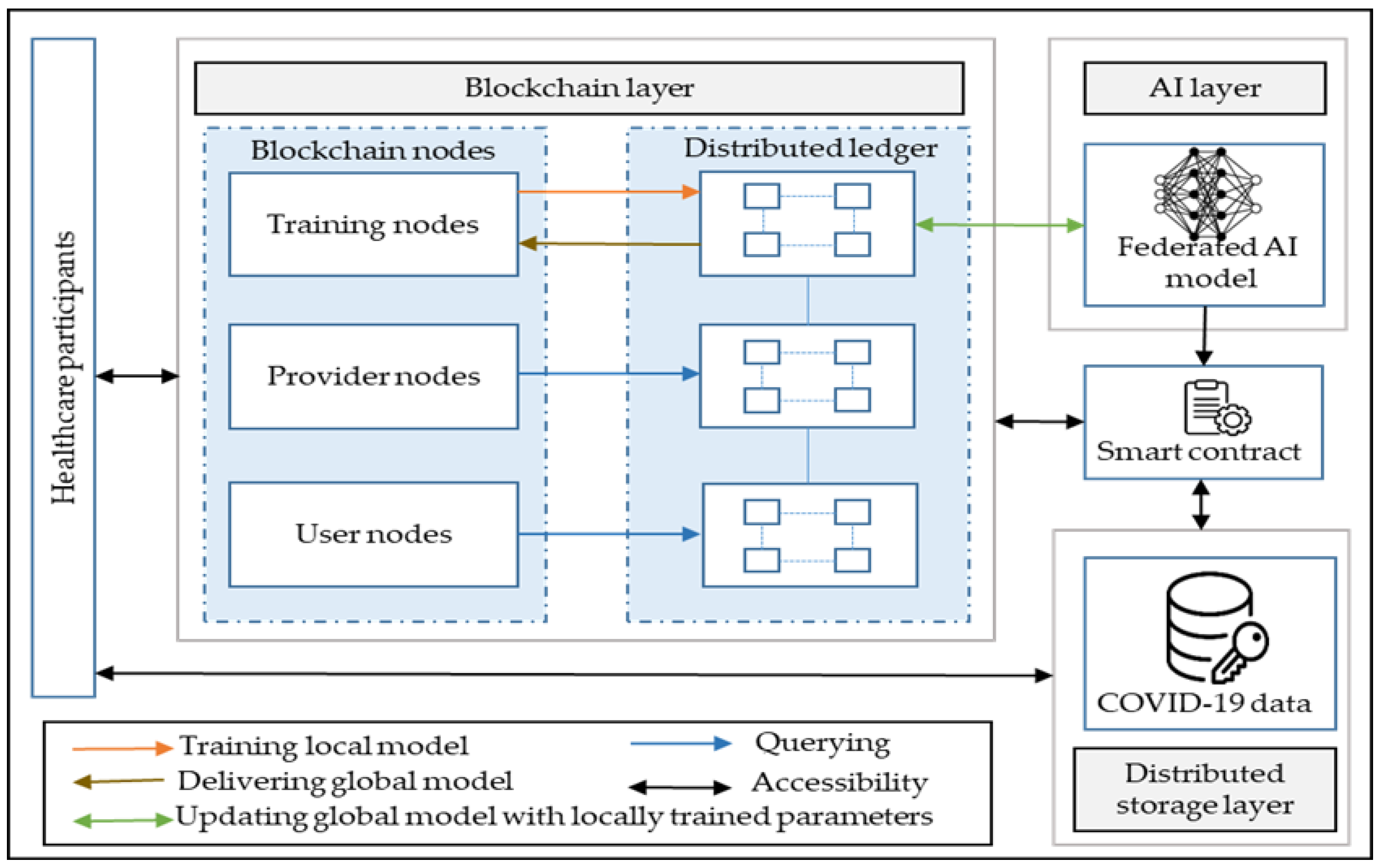
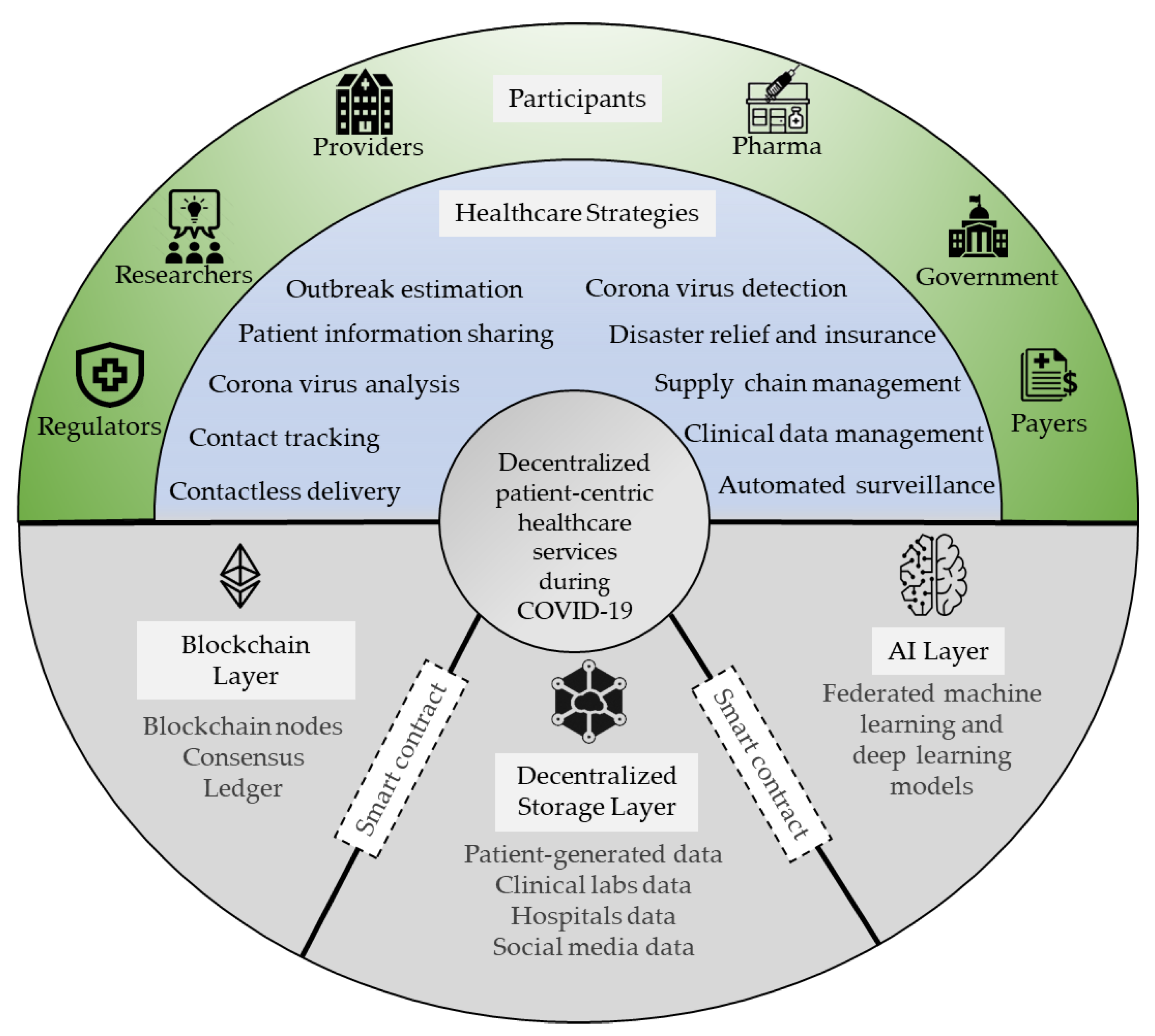
4. The Proposed Patient-Centric Framework
5. Applications for Healthcare Management and Response Strategies during COVID-19
5.1. Patient-Centric Information Sharing and Clinical Data Management
5.2. Decentralized Contact Tracing
5.3. Outbreak Estimation
5.4. Coronavirus Detection and Analysis
5.5. Disaster Relief and Insurance
5.6. Supply Chain Management
5.7. Contactless Delivery and Automated Surveillances
6. Discussions
6.1. Challenges and Solutions
6.2. Future Work
7. Conclusions
Author Contributions
Funding
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Wilder-Smith, A.; Osman, S. Public health emergencies of international concern: A historic overview. J. Travel Med. 2020, 27, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Economic Effects of Coronavirus Outbreak (COVID-19) on the World Economy. Available online: https://ssrn.com/abstract=3557504 (accessed on 5 June 2021).
- Kaye, A.D.; Okeagu, C.N.; Pham, A.D.; Silva, R.A.; Hurley, J.J.; Arron, B.L.; Sarfraz, N.; Lee, H.N.; Ghali, G.E.; Gamble, J.W.; et al. Economic impact of COVID-19 pandemic on healthcare facilities and systems: International perspectives. Best Pract. Res. Clin. Anesthesiol. 2020. [Google Scholar] [CrossRef]
- Minor, D. The Democratization of Health Care. Stanford Medicine 2018 Health Trends Report. 2018. Available online: https://med.stanford.edu/content/dam/sm/school/documents/Health-Trends-Report/Stanford-Medicine-Health-Trends-Report-2018.pdf (accessed on 5 June 2021).
- Morley, J.; Cowls, J.; Taddeo, M.; Floridi, L. Ethical guidelines for COVID-19 tracing apps. Nature 2020, 582, 29–31. [Google Scholar] [CrossRef]
- Ko, H.; Leitner, J.; Kim, E.; Jeong, J. Information technology–based tracing strategy in response to COVID-19 in South Korea—Privacy controversies. JAMA 2020, 323, 2129–2130. [Google Scholar]
- Reddy, S.; Fox, J.; Purohit, M.P. Artificial intelligence-enabled healthcare delivery. J. R. Soc. Med. 2019, 112, 22–28. [Google Scholar] [CrossRef]
- Hölbl, M.; Kompara, M.; Kamišalić, A.; Zlatolas, L.N. A systematic review of the use of blockchain in healthcare. Symmetry 2018, 10, 470. [Google Scholar] [CrossRef] [Green Version]
- Monrat, A.A.; Schelén, O.; Andersson, K. A survey of blockchain from the perspectives of applications, challenges, and opportunities. IEEE Access 2019, 7, 117134–117151. [Google Scholar] [CrossRef]
- Griggs, K.N.; Ossipova, O.; Kohlios, C.P.; Baccarini, A.N.; Howson, E.A.; Hayajneh, T. Healthcare blockchain system using smart contracts for secure automated remote patient monitoring. J. Med. Syst. 2018, 42, 1–7. [Google Scholar] [CrossRef]
- Vaishya, R.; Javaid, M.; Khan, I.H.; Haleem, A. Artificial Intelligence (AI) applications for COVID-19 pandemic. Diabetes Metab. Syndr. Clin. Res. Rev. 2020, 14, 337–339. [Google Scholar] [CrossRef]
- McMahan, H.B.; Moore, E.; Ramage, D.; Hampson, S.; Aguera y Arcas, B. Communication-efficient learning of deep networks from decentralized data. In Proceedings of the 20th International Conference on Artificial Intelligence and Statistics, AISTATS, Lauderdale, FL, USA, 20–22 April 2017; pp. 1273–1282. [Google Scholar]
- Lu, X.; Liao, Y.; Lio, P.; Hui, P. Privacy-preserving asynchronous federated learning mechanism for edge network computing. IEEE Access 2020, 8, 48970–48981. [Google Scholar] [CrossRef]
- Sharma, A.; Bahl, S.; Bagha, A.K.; Javaid, M.; Shukla, D.K.; Haleem, A. Blockchain technology and its applications to combat COVID-19 pandemic. Res. Biomed. 2020, 1–8. [Google Scholar] [CrossRef]
- Chen, H.S.; Jarrell, J.T.; Carpenter, K.A.; Cohen, D.S.; Huang, X.; Hospital, M.G. Blockchain in healthcare: A patient-centered model. Biomed. J. Sci. Tech. Res. (BJSTR) 2019, 20, 15017–15022. [Google Scholar]
- Jabarulla, M.Y.; Lee, H.-N. Blockchain-based distributed patient-centric image management system. Appl. Sci. 2020, 11, 196. [Google Scholar] [CrossRef]
- Ploug, T.; Holm, S. The four dimensions of contestable AI diagnostics—A patient-centric approach to explainable AI. Artif. Intell. Med. 2020, 107, 101901. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, D.C.; Ding, M.; Pathirana, P.N.; Seneviratne, A. Blockchain and AI-based solutions to combat Coronavirus (COVID-19)-like epidemics: A survey. Preprints 2020, 1–15. [Google Scholar] [CrossRef]
- Omar, A.; Bhuiyan, M.; Basu, A.; Kiyomoto, S.; Rahman, M. Privacy-friendly platform for healthcare data in cloud based on blockchain environment. Future Gener. Comput. Syst. 2019, 95, 511–521. [Google Scholar] [CrossRef]
- Ramani, V.; Kumar, T.; Bracken, A.; Liyanage, M.; Ylianttila, M. Secure and efficient data accessibility in blockchain based healthcare systems. In Proceedings of the IEEE Global Communications Conference (GLOBECOM), Abu Dhabi, United Arab Emirates, 9–13 December 2018; pp. 206–212. [Google Scholar]
- Abugabah, A.; Nizam, N.; Alzubi, A. Decentralized telemedicine framework for a smart healthcare ecosystem. IEEE Access 2020, 8, 166575–166588. [Google Scholar] [CrossRef]
- Patel, V. A framework for secure and decentralized sharing of medical imaging data via blockchain consensus. Health Inform. J. 2019, 25, 1398–1411. [Google Scholar] [CrossRef]
- Shah, R.; Chircu, A. IoT and AI in healthcare: A systematic literature review. Issues Inf. Syst. 2018, 19, 33–41. [Google Scholar] [CrossRef]
- Passerat-Palmbach, J.; Farnan, T.; Miller, R.; Gross., M.S.; Flannery, H.; Gleim, B. A blockchain-orchestrated Federated Learning architecture for healthcare consortia. arXiv 2019, arXiv:1910.12603. [Google Scholar]
- Kasnakova, P.; Ivanova, S. Patient-centered approach to pharmaceutical care in the recovery of patients with post-COVID syndrome. Pharmacia 2021, 68, 381–385. [Google Scholar] [CrossRef]
- James, C.; Barfield, M.; Maass, K.; Patel, S.; Anderson, M. Will patient-centric sampling become the norm for clinical trials after COVID-19? Nat. Med. 2020, 26, 1810. [Google Scholar] [CrossRef]
- Nembaware, V.; Munung, N.; Matimba, A.; Tiffin, N. Patient-centric research in the time of COVID-19: Conducting ethical COVID-19 research in Africa. BMJ Glob. Health 2020, 5, e003035. [Google Scholar] [CrossRef]
- Beaverson, M. HealthTech. July 2020. Available online: https://healthtechmagazine.net/article/2020/12/how-covid-19-has-accelerated-digital-transformation-healthcare (accessed on 16 July 2021).
- Alsamhi, S.H.; Lee, B.; Guizani, M.; Kumar, N.; Qiao, Y.; Liu, X. Blockchain for decentralized multi-drone to combat COVID-19 and future pandemics: Framework and proposed solutions. Trans. Emerg. Telecommun. Technol. 2021, e4255. [Google Scholar] [CrossRef]
- Lalmuanawma, S.; Hussain, J.; Chhakchhuak, L. Applications of machine learning and artificial intelligence for COVID-19 (SARS-CoV-2) pandemic: A review. Chaos Solitons Fractals 2020, 139, 110059. [Google Scholar] [CrossRef] [PubMed]
- Tuckson, R.; Edmunds, M.; Hodgkins, M. Telehealth. N. Engl. J. Med. 2017, 377, 1585–1592. [Google Scholar] [CrossRef]
- Rabah, K. Convergence of AI, IoT, big data and blockchain: A review. Lake Inst. J. 2018, 1, 1–18. [Google Scholar]
- Ye, J. The Role of Health Technology and Informatics in a Global Public Health Emergency: Practices and Implications from the COVID-19 Pandemic. JMIR Med. Inform. 2020, 8, e19866. [Google Scholar] [CrossRef]
- Flannery, D.; Jarrin, R. Building A Regulatory and Payment Framework Flexible Enough to Withstand Technological Progress. Health Aff. 2018, 37, 2052–2059. [Google Scholar] [CrossRef] [PubMed]
- Mahmood, S.; Hasan, K.; Carras, M.C.; Labrique, A. Global Preparedness Against COVID-19: We Must Leverage the Power of Digital Health. JMIR Public Health Surveill. 2020, 6, e18980. [Google Scholar] [CrossRef] [Green Version]
- Bahl, S.; Singh, R.; Javaid, M.; Khan, I.; Vaishya, R.; Suman, R. Telemedicine technologies for confronting COVID-19 pandemic: A review. J. Ind. Integr. Manag. Innov. Entrep. 2020, 5, 547–561. [Google Scholar] [CrossRef]
- Ghosh, A.; Gupta, R.; Misra, A. Telemedicine for diabetes care in India during COVID19 pandemic and national lockdown period: Guidelines for physicians. Diabetes Metab. Syndr. Clin. Res. Rev. 2020, 14, 273–276. [Google Scholar] [CrossRef]
- Bahl, S.; Javaid, M.; Bagha, A.; Singh, R.; Haleem, A.; Vaishya, R.; Suman, R. Biosensors applications in fighting COVID-19 pandemic. Apollo Med. 2020, 17, 221–223. [Google Scholar] [CrossRef]
- Javaid, M.; Haleem, A.; Vaishya, R.; Bahl, S.; Suman, R.; Vaish, A. Industry 4.0 technologies and their applications in fighting COVID-19 pandemic. Diabetes Metab. Syndr. Clin. Res. Rev. 2020, 14, 419–422. [Google Scholar] [CrossRef] [PubMed]
- Whitelaw, S.; Mamas, M.A.; Topol, E.; Van Spall, H.G.C. Applications of digital technology in COVID-19 pandemic planning and response. Lancet Digit. Health 2020, 2, e435–e440. [Google Scholar] [CrossRef]
- Ferretti, L.; Wymant, C.; Kendall, M.; Zhao, L.; Nurtay, A.; Abeler-Dörner, L.; Parker, M.; Bonsall, D.; Fraser, C. Quantifying SARS-CoV-2 transmission suggests epidemic control with digital contact tracing. Science 2020, 368, eabb6936. [Google Scholar] [CrossRef] [Green Version]
- Gagliardi, A.; Lemieux-Charless, L.; Brown, A.; Sullivan, T.; Goel, V. Barriers to patient involvement in health service planning and evaluation: An exploratory study. Patient Educ. Couns. 2008, 70, 234–241. [Google Scholar] [CrossRef] [PubMed]
- Mead, N.; Bower, P. Patient-centredness: A conceptual framework and review of the empirical literature. Soc. Sci. Med. 2000, 51, 1087–1110. [Google Scholar] [CrossRef]
- Crawford, M.; Rutter, D.; Manley, C.; Weaver, T.; Bhui, K.; Fulop, N.; Tyrer, P. Systematic review of involving patients in the planning and development of health care. BMJ 2002, 325, 1263. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gordon, W.J.; Catalini, C. Blockchain Technology for Healthcare: Facilitating the Transition to Patient-Driven Interoperability. Comput. Struct. Biotechnol. J. 2018, 16, 224–230. [Google Scholar] [CrossRef]
- Nakamoto, S. Bitcoin: A Peer-to-Peer Electronic Cash System. 2008. Available online: https://bitcoin.org/bitcoin.pdf. (accessed on 5 June 2021).
- Wood, G. ETHEREUM: A Secure Decentralised Generalised Transaction Ledger. 2014. Available online: https://gavwood.com/paper.pdf (accessed on 5 June 2021).
- Agboo, C.; Mahmoud, Q.; Eklund, J. Blockchain technology in healthcare: A systematic review. Healthcare 2019, 7, 56. [Google Scholar] [CrossRef] [Green Version]
- Zhang, R.; Xue, R.; Liu, L. Security and Privacy on Blockchain. ACM Comput. Surv. 2019, 52, 1–34. [Google Scholar] [CrossRef] [Green Version]
- Jang, J.; Lee, H.N. Profitable Double-Spending Attacks. Appl. Sci. 2020, 10, 8477. [Google Scholar] [CrossRef]
- Khatoon, A. A Blockchain-Based Smart Contract System for Healthcare Management. Electronics 2020, 9, 94. [Google Scholar] [CrossRef] [Green Version]
- Niya, S.R.; Schüpfer, F.; Bocek, T.; Stiller, B. A Peer-to-Peer Purchase and Rental Smart Contract-based Application. Inf. Technol. 2018, 60, 307–320. [Google Scholar]
- Novikov, S.; Kazakov, O.; Kulagina, N.; Azarenko, N. Blockchain and smart contracts in a decentralized health infrastructure. In Proceedings of the IEEE International Conference Quality Management, Transport and Information Security, Information Technologies (IT&QM&IS), St. Petersburg, Russia, 24 September 2018; pp. 697–703. [Google Scholar]
- Nguyen, D.; Pathirana, P.; Ding, M.; Seneviratne, A. Blockchain for secure EHRs sharing of mobile cloud based e-health systems. IEEE Access 2019, 7, 66792–66806. [Google Scholar] [CrossRef]
- Zheng, X.; Mukkamala, R.; Vatrapu, R.; Ordieres-Mere, J. Blockchain-based personal health data sharing system using cloud storage. In Proceedings of the IEEE 20th International Conference on e-Health Networking, Applications and Services (Healthcom), Ostrava, Czech Republic, 17–20 September 2018; pp. 1–6. [Google Scholar]
- Hasselgren, A.; Kralevska, K.; Gilgoroski, D.; Pedersen, S.; Faxvaag, A. Blockchain in healthcare and health sciences–A scoping review. Int. J. Med. Inform. 2019, 134, 104040. [Google Scholar] [CrossRef]
- Christiansen, P. Artificial Intelligence: Healthcare’s New Nervous System. 2017. Available online: https://www.accenture.com/_acnmedia/PDF-49/Accenture-Health-Artificial-Intelligence.pdf (accessed on 5 June 2021).
- Erickson, B.J.; Korfiatis, P.; Akkus, Z.; Kline, T.L. Machine learning for medical imaging. Radiographics 2017, 37, 505–515. [Google Scholar] [CrossRef] [PubMed]
- Amin, S.; Hossain, M.; Muhammad, G.; Alhussein, M.; Rahman, M. Cognitive smart healthcare for pathology detection and monitoring. IEEE Access 2019, 7, 10745–10753. [Google Scholar] [CrossRef]
- Pouyanfar, S.; Sadiq, S.; Yan, Y.; Tian, H.; Tao, Y.; Reyes, M.; Shyu, L.; Chen, S..; Iyengar, S. A survey on deep learning: Algorithms, techniques, and applications. ACM Comput. Surv. (CSUR) 2018, 51, 1–36. [Google Scholar] [CrossRef]
- Taulli, T. AI (Artificial Intelligence) Companies That Are Combating the COVID-19 Pandemic. 2020. Available online: https://www.forbes.com/sites/tomtaulli/2020/03/28/ai-artificial-intelligence-companies-that-are-combating-the-covid-19-pandemic/ (accessed on 5 June 2021).
- Ye, D.; Yu, R.; Pan, M.; Han, Z. Federated learning in vehicular edge computing: A selective model aggregation approach. IEEE Access 2020, 8, 23920–23935. [Google Scholar] [CrossRef]
- Kumar, R.; Khan, A.A.; Zhang, S.; Kumar, J.; Yang, T.; Golilarz, N.A.; Zakria; Ikram, A.; Shafiq, S.; Wang, W. Blockchain-Federated-Learning and Deep Learning Models for COVID-19 detection using CT Imaging. arXiv 2020, arXiv:2007.06537. [Google Scholar]
- Lu, Y.; Huang, X.; Zhang, K.; Maharjan, S.; Zhang, Y. Blockchain Empowered Asynchronous Federated Learning for Secure Data Sharing in Internet of Vehicles. IEEE Trans. Veh. Technol. 2020, 69, 4298–4311. [Google Scholar] [CrossRef]
- Hua, G.; Zhu, L.; Wu, J.; Shen, C.; Zhou, L.; Lin, Q. Blockchain-Based Federated Learning for Intelligent Control in Heavy Haul Railway. IEEE Access 2020, 8, 176830–176839. [Google Scholar] [CrossRef]
- Harris, J.D. Analysis of models for decentralized and collaborative AI on blockchain. In Proceedings of the The 2020 International Conference on Blockchain, Rhodes Island, Greece, 2–6 November 2020. [Google Scholar]
- Lewko, A.; Waters, B. Decentralizing Attribute-Based Encryption. In Proceedings of the Annual International Conference on the Theory and Applications of Cryptographic Techniques, Tallinn, Estonia, 15–19 May 2011; pp. 568–588. [Google Scholar]
- Li, D.; Du, R.; Fu, Y.; Ho Au, M. Meta-Key: A secure data-sharing protocol under blockchain-based decentralized storage architecture. IEEE Netw. Lett. 2019, 1, 30–33. [Google Scholar] [CrossRef]
- Zahed Benisi, N.; Aminian, M.; Javadi, B. Blockchain-based decentralized storage networks: A survey. J. Netw. Comput. Appl. 2020, 162, 102656. [Google Scholar] [CrossRef]
- Benet, J. IPFS—Content Addressed, Versioned, P2P File System. arXiv 2014, arXiv:1407.3561. [Google Scholar]
- Miyachi, K.; Mackey, T.K. hOCBS: A privacy-preserving blockchain framework for healthcare data leveraging an on-chain and off-chain system design. Inf. Process. Manag. 2021, 58, 102535. [Google Scholar] [CrossRef]
- Drungilas, V.; Vaičiukynas, E.; Jurgelaitis, M.; Butkiene, R. Towards blockchain-based federated machine learning: Smart contract for model inference. Appl. Sci. 2021, 11, 1010. [Google Scholar] [CrossRef]
- Puri, V.; Kataria, A.; Sharma, V. Artificial intelligence-powered decentralized framework for internet of things in healthcare 4.0. Trans. Emerg. Telecommun. Technol. 2021, e4245. [Google Scholar] [CrossRef]
- Edemekong, P.F.; Haydel, M.J. Health Insurance Portability and Accountability Act (HIPAA); StatPearls Publishing: Treasure Island, FL, USA, 2018. [Google Scholar]
- Truong, N.; Sun, K.; Lee, G.; Guo, Y. GDPR-compliant personal data management: A BlockchainBased Solution. IEEE Trans. Inf. Forensics Secur. 2019, 15, 1746–1761. [Google Scholar] [CrossRef] [Green Version]
- Shen, B.; Guo, J.; Yang, Y. MedChain: Efficient healthcare data sharing via blockchain. Appl. Sci. 2019, 9, 1207. [Google Scholar] [CrossRef] [Green Version]
- Dietsche, E. Health Wizz Leverages Blockchain Technology to Give Patients Power over Their Data. MedCity News. 2017. Available online: https://medcitynews.com/2017/12/health-wizz/ (accessed on 5 June 2021).
- Nugent, T.; Upton, D.; Cimpoesu, M. Improving data transparency in clinical trials using blockchain smart contracts. F1000Research 2016, 5, 2541. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Timberg, C.; Harwell, D. Government Efforts to Track Virus through Phone Location Data Complicated by Privacy Concerns. Washington Post. 2020. Available online: https://www.washingtonpost.com/technology/2020/03/19/privacy-coronavirus-phone-data/ (accessed on 5 June 2021).
- Jones, M.; Johnson, M.; Shervey, M.; Dudley, J.; Zimmerman, N. Privacy-Preserving Methods for Feature Engineering Using Blockchain: Review, Evaluation, and Proof of Concept. J. Med. Internet Res. 2019, 21, e13600. [Google Scholar] [CrossRef] [Green Version]
- Hylock, R.; Zeng, X. A Blockchain framework for patient-centered health records and exchange (HealthChain): Evaluation and proof-of-concept study. J. Med. Internet Res. 2019, 21, e13592. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wistrom, B. How Blockchain and Immunization Passports Could Help Us Re-Open. 2020. Available online: https://www.americaninno.com/austin/inno-insights/how-blockchain-and-immunization-passports-could-help-us-re-open/ (accessed on 5 June 2021).
- Degrasse, M. The Role of Wireless Tech in Fighting the New Coronavirus. 2020. Available online: https://www.lightreading.com/4g-3g-wifi/the-role-of-wireless-tech-in-fighting-the-new-coronavirus/d/d-id/757634 (accessed on 5 June 2021).
- Sarker, I.; Kayes, A.; Watters, P. Effectiveness analysis of machine learning classification models for predicting personalized context-aware smartphone usage. J. Big Data 2019, 6, 1–28. [Google Scholar] [CrossRef]
- Shen, J.; Shafiq, M. Learning mobile application usage-a deep learning approach. In Proceedings of the 2019 18th IEEE International Conference on Machine Learning and Applications (ICMLA), Boca Raton, FL, USA, 16–19 December 2019; pp. 287–292. [Google Scholar]
- Wang, Z.; Wang, G.; Huang, H.; Xiong, Z.; Hong, Q.; Wu, H.; Yi, P.; Jiang, K.; Wang, N.; Pei, Y.; et al. Masked Face Recognition Dataset and Application. arXiv 2020, arXiv:2003.09093. [Google Scholar]
- Gozes, O.; Frid-Adar, M.; Greenspan, H.; Browning, P.; Zhang, H.; Ji, W.; Bernheim, A.; Siegel, E. Rapid AI Development Cycle for The Coronavirus (COVID-19) Pandemic: Initial Results for Automated Detection & Patient Monitoring Using Deep Learning CT Image Analysis. arXiv 2020, arXiv:2003.05037. [Google Scholar]
- Xu, X.; Jiang, X.; Ma, C.; Du, P.; Li, X.; Lv, S.; Yu, L.; Chen, Y.; Su, J.; Lang, G.; et al. Deep learning system to screen coronavirus disease 2019 pneumonia. arXiv 2020, arXiv:2002.09334. [Google Scholar] [CrossRef]
- Narin, A.; Kaya, C.; Pamuk, Z. Automatic detection of coronavirus disease (COVID-19) using x-ray images and deep convolutional neural networks. Pattern Anal. Appl. 2021, 24, 1207–1220. [Google Scholar] [CrossRef]
- Plunk, A. Patient Consumerism and the Need for a Patient-Centric Revenue Model. 2018. Available online: https://www.beckershospitalreview.com/finance/patient-consumerism-and-the-need-for-a-patient-centric-revenue-model.html (accessed on 5 June 2021).
- Degnarain, N. Five Ways Blockchain Can Unblock the Coronavirus Medical Supply Chain. Forbes 2020. Available online: Forbes.com/sites/nishandegnarain/2020/03/22/5-ways-blockchaincan-%0Aunblock-the-coronavirus-medical-supply-chain/ (accessed on 5 June 2021).
- Lee, S.; Lee, D. “Untact”: A new customer service strategy in the digital age. Serv. Bus. 2020, 14, 1–22. [Google Scholar] [CrossRef]
- Scarlato, M.; Perra, C.; Jabarulla, M.Y.; Jung, G.; Lee, H.N. A blockchain for the collision avoidance and the recovery of crashed UAVS. In Proceedings of the Korean Institute of Electronics Engineers Conference, Jeju, Korea, 27–31 May 2019; pp. 463–467. [Google Scholar]
- Kapitonov, A.; Lonshakov, S.; Berman, I.; Ferrer Castello, E.; Bonsignorio, F.; Bulatov, V.; Svistov, A. Robotic services for new paradigm smartcities based on decentralized technologies. Ledger 2019, 56–66. [Google Scholar] [CrossRef]
- Yu, G.; Wang, K.; Ni, W.; Zhang, J.; Liu, R. Survey: Sharding in blockchains. IEEE Access 2020, 8, 14155–14181. [Google Scholar] [CrossRef]
- Bernabe, J.B.; Canovas, J.; Hermandez-Ramos, L.; Moreno, R.; Skarmeta, A. Privacy-preserving solutions for blockchain: Review and challenges. IEEE Access 2019, 7, 164908–164940. [Google Scholar] [CrossRef]
- Line, Q.; Yan, H.; Huang, Z.; Chen, W.; Shen, J.; Tang, Y. An ID-based linearly homomorphic signature scheme and its application in blockchain. IEEE Access 2018, 6, 20632–20640. [Google Scholar] [CrossRef]
- Kakavand, H.; Kost De Sevres, N.; Chilton, B. The Blockchain Revolution: An Analysis of Regulation and Technology Related to Distributed Ledger Technologies. Soc. Sci. Res. Netw. (SSRN) 2017, 1–27. [Google Scholar] [CrossRef] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Strategies | Functions | Digital Technologies | Challenges |
|---|---|---|---|
| Contact Tracking | Identifies and monitors individuals that come into contact with an infected person within a specific duration of time. | Bluetooth Low Energy technology, mobile phone applications, wearables, and IoT devices. | Security and privacy issues, since individuals’ data are analyzed and stored in a centralized cloud system. |
| Quarantine and Self-Isolation | In quarantine, individuals are requested to stay in a place (i.e., home or government facilities) for 14 days after being exposed to a COVID-19-infected person. In self-isolation, an infected person isolates within a house or other location to prevent contacting uninfected persons. | AI, a global positioning system, cameras, and recorders. | Breaches civil liberties, restricted access to essential services, and fails to track the individual who runs away from a quarantine facility without their device, like a mobile phone. |
| Automated Surveillance | To identify and monitor individuals without facemasks, social distancing, and accidental touching in public gathering places. Detects symptoms, such as breathing difficulties, coughing, and fever, using self-tracking digital technologies. | Facial recognition, digital thermometers, surveillance cameras, and thermal cameras. | Security attacks, operational cost. |
| Clinical Data Management | Used to diagnose infected individuals and provides the capacity for telemedicine services and virtual care, prediction of clinical outcomes, and monitoring of clinical status by clinicians. | Picture archiving and communications system (PACS). | Not cost efficient, privacy breaches may occur, failure in diagnosis. |
| Patient Information Sharing | Patient health and medical information sharing could decrease the possibility of duplicate testing and avoid medication errors. Furthermore, sharing patient data among the global research community plays an essential role in coronavirus research by formulating powerful raw data sets. | AI, web-based toolkits, and PACS. | Satisfying Health Insurance Portability and Accountability Act (HIPAA) compliances, lack of anonymity, security, privacy, and data management issues. |
| Contactless Delivery | During the lockdown, contactless delivery of essential supplies, such as medicine, food, and sanitizers, prevents direct interactions with people, since doorstep delivery might not be safe during a high transmission rate. | Robots and drones. | Security attacks, operational costs, and legal issues in the case of an accident. |
| Supply Chain Management | Identify and secure logistics capacity based on the type of goods, such as medical equipment and vaccines/drugs or other pharmaceutical medicines. | Mobile platforms, data analytics, cloud, and IoT. | Procuring medical equipment, pharmaceutical medicines, and household essentials are difficult due to the surge in demand. |
| Disaster Relief and Insurance | Financial organizations and governments have to help the public by providing unemployment insurance relief, loans to protect their business losses, and health insurance that covers treatment costs during the COVID-19 outbreak. | Web-based toolkits and mobile applications. | Time-consuming and ineffective due to paper-based procedures and centralized authority. |
| Aspects | Standard Healthcare System | Proposed Healthcare Platform |
|---|---|---|
| Source Data Storage | The COVID-19 data are stored in a centralized cloud-based storage system, like PACS. | The COVID-19 data are stored in decentralized storage systems, such as IPFS. |
| Database Sharing Mechanism and Integrity | Depends on a cloud-based mechanism and EHR databases managed by a third-party clearinghouse. Thus, there are possibilities of data tampering. | Depends on a blockchain-based sharing mechanism and EHR databases managed by the participants of the healthcare ecosystem. Thus, databases are immutable. |
| Administration Performance and Scalability | More transactions are processed per second and enable great scalability. | Process minimal transactions per second, and there are scalability issues since the framework is at its developing stage. |
| Implementation Cost | Easy to implement and maintain due to its large-scale adoption. | Uncertainty in the operating costs. |
| Incentive Mechanism for Sharing Data | Not available. | The patient can receive an incentive for sharing their medical data for research purposes. |
| Data Accessibility | Depend on healthcare entities. | Patients have complete access to and control over their data. |
| Anonymity | High risk of privacy leakage and identity theft. | The identity of the patients and the transactions between healthcare participants remain anonymous since blockchain public addresses do not link to anyone’s identity. |
| Data Auditability | Always depends on administrators to audit the data. | The moment the blockchain reaches a predetermined state, any node in the blockchain network can track and trace the data right from its origin based on cryptography technology. |
| Computational Performance of AI | Computationally expensive for training large datasets acquired from different sources in a centralized server. | The federated learning approach reduces the computational power by enabling collaborations between several healthcare organizations to train the distributed global AI models without relying on any centralized server. |
| Decision Making | Human involvement. | Human involvement, AI, and a smart contract. |
| Fault Tolerance | Risk of a single point of failure. | A distributed blockchain ledger is highly fault-tolerant because of the consensus mechanism. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jabarulla, M.Y.; Lee, H.-N. A Blockchain and Artificial Intelligence-Based, Patient-Centric Healthcare System for Combating the COVID-19 Pandemic: Opportunities and Applications. Healthcare 2021, 9, 1019. https://doi.org/10.3390/healthcare9081019
Jabarulla MY, Lee H-N. A Blockchain and Artificial Intelligence-Based, Patient-Centric Healthcare System for Combating the COVID-19 Pandemic: Opportunities and Applications. Healthcare. 2021; 9(8):1019. https://doi.org/10.3390/healthcare9081019
Chicago/Turabian StyleJabarulla, Mohamed Yaseen, and Heung-No Lee. 2021. "A Blockchain and Artificial Intelligence-Based, Patient-Centric Healthcare System for Combating the COVID-19 Pandemic: Opportunities and Applications" Healthcare 9, no. 8: 1019. https://doi.org/10.3390/healthcare9081019