
Joint COVID-19 Contact Tracing and Malaria Reactive Case Detection as Efficient Strategies for Disease Control
 , , , ,
, , , , {kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Key Definitions
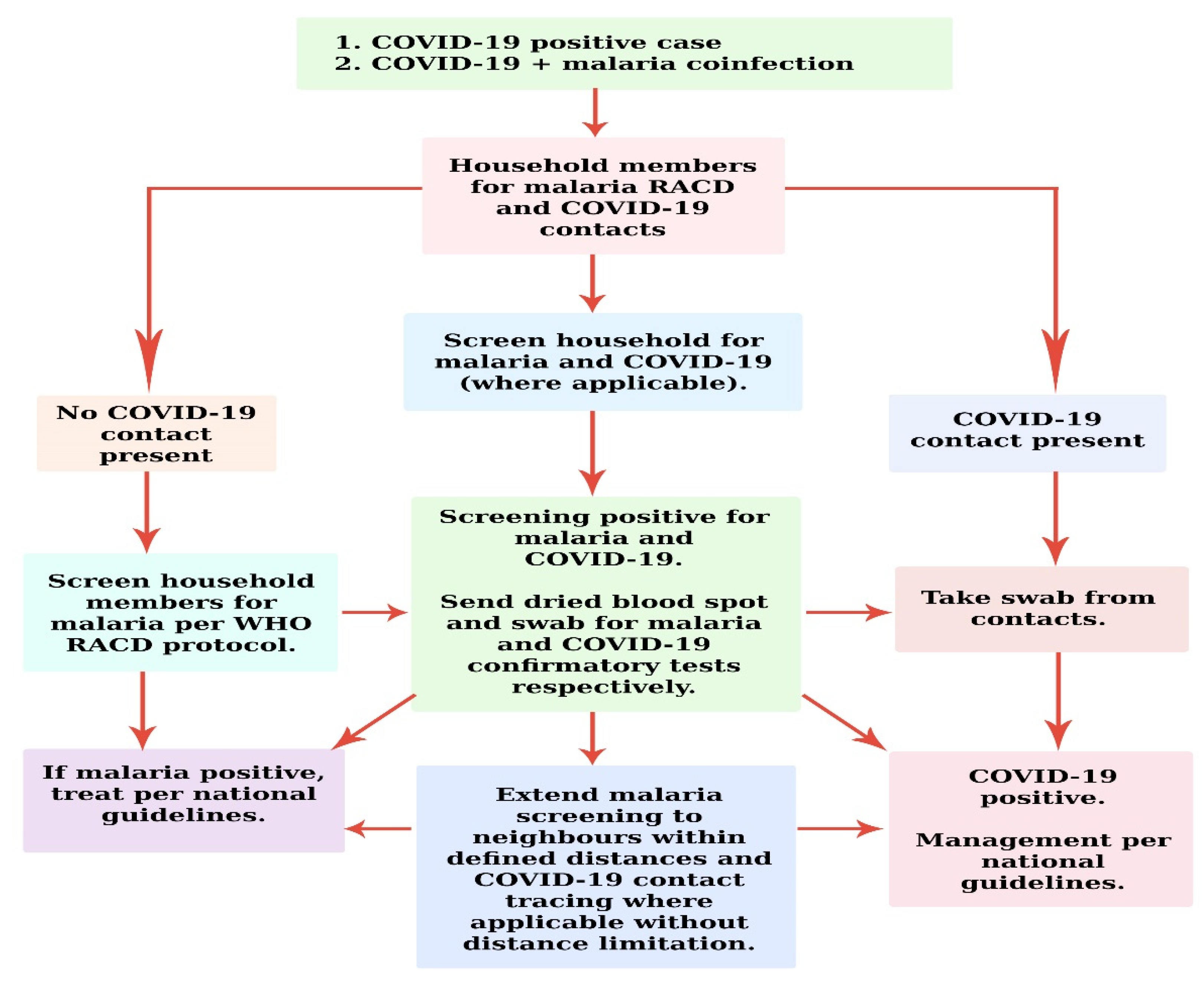
3. Two-Pronged Hybrid Proposal for COVID-19 Contact Tracing and Malaria RACD
4. Operational Commonalities between COVID-19 Contact Tracing and Malaria RACD
5. Differences
6. Challenges and Way Forward
7. Conclusions
8. Patents
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- World Health Organization. Contact Tracing in the Context of COVID-19: Interim Guidance; World Health Organization: Geneva, Switzerland, 2020.
- Centers for Disease Control and Prevention. Case Investigation and Contact Tracing: Part of a Multipronged Approach to Fight the COVID-19 Pandemic; Centers for Disease Control and Prevention: Atlanta, GA, USA, 2020.
- World Health Organization. Coronavirus (COVID-19) Dashboard. 2021. Available online: https://covid19.who.int/table (accessed on 14 June 2021).
- Lu, G.; Razum, O.; Jahn, A.; Zhang, Y.; Sutton, B.; Sridhar, D.; Ariyoshi, K.; von Seidlein, L.; Müller, O. COVID-19 in Germany and China: Mitigation versus elimination strategy. Glob. Health Action 2021, 14, 1875601. [Google Scholar] [CrossRef]
- Salyer, S.J.; Maeda, J.; Sembuche, S.; Kebede, Y.; Tshangela, A.; Moussif, M.; Ihekweazu, C.; Mayet, N.; Abate, E.; Ouma, A.O.; et al. The first and second waves of the COVID-19 pandemic in Africa: A cross-sectional study. Lancet 2021, 397, 1265–1275. [Google Scholar] [CrossRef]
- World Health Organization. Coronavirus (COVID-19), Africa. 2021. Available online: https://www.afro.who.int/health-topics/coronavirus-COVID-19 (accessed on 14 June 2021).
- Sturrock, H.J.; Hsiang, M.S.; Cohen, J.M.; Smith, D.L.; Greenhouse, B.; Bousema, T. Targeting asymptomatic malaria infections: Active surveillance in control and elimination. PLoS Med. 2013, 10, e1001467. [Google Scholar] [CrossRef]
- Sanders, K.; Gueye, C.S.; Phillips, A.A.; Gosling, R. Active case detection for malaria elimination: A confusion of acronyms and definitions. Malar. Chemother. Control Elimin. 2012, 1–5. [Google Scholar] [CrossRef]
- World Health Organization. Disease Surveillance for Malaria Elimination: An Operational Manual; World Health Organization: Geneva, Switzerland, 2012.
- World Health Organization. World Malaria Report 2021; World Health Organization: Geneva, Switzerland, 2021.
- Hussein, M.I.; Albashir, A.A.; Elawad, O.A.; Homeida, A. Malaria and COVID19: Unmasking their ties. Malar. J. 2020, 19, 457. [Google Scholar] [CrossRef]
- Rando, H.M.; Wellhausen, N.; Ghosh, S.; Lee, A.J.; Dattoli, A.A.; Hu, F.; Byrd, J.B.; Rafizadeh, D.N.; Lordan, R.; Qi, Y.; et al. Identification and Development of Therapeutics for COVID-19. mSystems 2021, 6, e00233-21. [Google Scholar] [CrossRef]
- Pereira, M.L.; Marinho, C.R.; Epiphanio, S. Could heme oxygenase-1 be a new target for therapeutic intervention in malaria-associated acute lung injury/acute respiratory distress syndrome? Front. Cell. Infect. Microbiol. 2018, 8, 161. [Google Scholar] [CrossRef]
- World Health Organization. Tailoring Malaria Interventions in the COVID-19 Response; World Health Organization: Geneva, Switzerland, 2020.
- Bhatt, S.; Weiss, D.J.; Cameron, E.; Bisanzio, D.; Mappin, B.; Dalrymple, U.; Battle, K.E.; Moyes, C.L.; Henry, A.; Eckhoff, P.A.; et al. The effect of malaria control on Plasmodium falciparum in Africa between 2000 and 2015. Nature 2015, 526, 207–211. [Google Scholar] [CrossRef]
- Dittrich, S.; Lamy, M.; Acharya, S.; Thu, H.K.; Datta, R.; Blacksell, S.D.; Hein, P.S.; Mercado, C.E.; Ding, X.C.; Chebbi, A. Diagnosing malaria and other febrile illnesses during the COVID-19 pandemic. Lancet Glob. Health 2020, 8, e879–e880. [Google Scholar] [CrossRef]
- Quaglio, G.L.; Preiser, W.; Putoto, G. COVID-19 in Africa. Public Health 2020, 185, 60. [Google Scholar] [CrossRef]
- Moonen, B.; Cohen, J.M.; Snow, R.W.; Slutsker, L.; Drakeley, C.; Smith, D.L.; Abeyasinghe, R.R.; Rodriguez, M.H.; Maharaj, R.; Tanner, M.; et al. Operational strategies to achieve and maintain malaria elimination. Lancet 2010, 376, 1592–1603. [Google Scholar] [CrossRef]
- Cotter, C.; Sturrock, H.J.; Hsiang, M.S.; Liu, J.; Phillips, A.A.; Hwang, J.; Gueye, C.S.; Fullman, N.; Gosling, R.D.; Feachem, R.G. The changing epidemiology of malaria elimination: New strategies for new challenges. Lancet 2013, 382, 900–911. [Google Scholar] [CrossRef]
- Fox, M. We Need an Army: Hiring of Coronavirus Trackers Seen as Key to Curbing Disease Spread; STAT: Boston, MA, USA, 2020. [Google Scholar]
- Fair, E.; Miller, C.R.; Ottmani, S.E.; Fox, G.J.; Hopewell, P.C. Tuberculosis contact investigation in low-and middle-income countries: Standardized definitions and indicators. Int. J. Tuberc. Lung Dis. 2015, 19, 269–272. [Google Scholar] [CrossRef] [PubMed]
- Swanson, K.C.; Altare, C.; Wesseh, C.S.; Nyenswah, T.; Ahmed, T.; Eyal, N.; Hamblion, E.L.; Lessler, J.; Peters, D.H.; Altmann, M. Contact tracing performance during the Ebola epidemic in Liberia, 2014–2015. PLoS Negl. Trop. Dis. 2018, 12, e0006762. [Google Scholar] [CrossRef]
- Bergmans, B.J.; Reusken, C.B.; van Oudheusden, A.J.; Godeke, G.-J.; Marinović, A.A.B.; de Vries, E.; Hingh, Y.C.K.-D.; Vingerhoets, R.; Berrevoets, M.A.; Verweij, J.J.; et al. Test, trace, isolate: Evidence for declining SARS-CoV-2 PCR sensitivity in a clinical cohort. Diagn. Microbiol. Infect. Dis. 2021, 101, 115392. [Google Scholar] [CrossRef]
- USAID. Stop TB Partnership: COVID-19 Contact Tracing and TB Contact Investigation: An Integrated Implementation Approach; USAID: Washington, DC, USA, 2021. [Google Scholar]
- Pampana, E. A Textbook of Malaria Eradication, 2nd ed.; Oxford University Press: London, UK, 1969; p. xiv + 593. [Google Scholar]
- Hellewell, J.; Abbott, S.; Gimma, A.; Bosse, N.I.; Jarvis, C.I.; Russell, T.W.; Munday, J.D.; Kucharski, A.J.; Edmunds, W.J.; Funk, S.; et al. Feasibility of controlling COVID-19 outbreaks by isolation of cases and contacts. Lancet Glob. Health 2020, 8, e488–e496. [Google Scholar] [CrossRef]
- He, X.; Lau, E.H.Y.; Wu, P.; Deng, X.; Wang, J.; Hao, X.; Lau, Y.C.; Wong, J.Y.; Guan, Y.; Tan, X.; et al. Temporal dynamics in viral shedding and transmissibility of COVID-19. Nat. Med. 2020, 26, 672–675. [Google Scholar] [CrossRef]
- Lavezzo, E.; Franchin, E.; Ciavarella, C.; Cuomo-Dannenburg, G.; Barzon, L.; Del Vecchio, C.; Rossi, L.; Manganelli, R.; Loregian, A.; Navarin, N.; et al. Suppression of a SARS-CoV-2 outbreak in the Italian municipality of Vo’. Nature 2020, 584, 425. [Google Scholar] [CrossRef]
- Harris, I.; Sharrock, W.W.; Bain, L.M.; Gray, K.-A.; Bobogare, A.; Boaz, L.; Lilley, K.; Krause, D.; Vallely, A.; Johnson, M.-L.; et al. A large proportion of asymptomatic Plasmodium infections with low and sub-microscopic parasite densities in the low transmission setting of Temotu Province, Solomon Islands: Challenges for malaria diagnostics in an elimination setting. Malar. J. 2010, 9, 254. [Google Scholar] [CrossRef]
- Clark, E.; Chiao, E.Y.; Amirian, E.S. Why contact tracing efforts have failed to curb coronavirus disease 2019 (COVID-19) transmission in much of the united states. Clin. Infect. Dis. 2021, 72, e415–e419. [Google Scholar] [CrossRef] [PubMed]
- Keeling, M.J.; Hollingsworth, T.D.; Read, J.M. Efficacy of contact tracing for the containment of the 2019 novel coronavirus (COVID-19). J. Epidemiol. Community Health 2020, 74, 861–866. [Google Scholar] [CrossRef] [PubMed]
- Kretzschmar, M.E.; Rozhnova, G.; Bootsma, M.C.; van Boven, M.; van de Wijgert, J.H.; Bonten, M.J. Impact of delays on effectiveness of contact tracing strategies for COVID-19: A modelling study. Lancet Glob. Health 2020, 5, e452–e459. [Google Scholar] [CrossRef]
- Service Mike. Life cycle of Anopheles. In Medical Entomology for Students, 2nd ed.; Cambridge University Press: Cambridge, UK, 2000; pp. 34–36. [Google Scholar]
- Yaro, A.S.; Dao, A.; Adamou, A.; Crawford, J.E.; MC Ribeiro, J.; Gwadz, R.; Traoré, S.F.; Lehmann, T. The distribution of hatching time in Anopheles gambiae. Malar. J. 2006, 5, 19. [Google Scholar] [CrossRef]
- Available online: http://www3.niaid.nih.gov/topics/Malaria/lifecycle.htm (accessed on 10 August 2022).
- Silvie, O.; Mota, M.M.; Matuschewski, K.; Prudêncio, M. Interactions of the malaria parasite and its mammalian host. Curr. Opin. Microbiol. 2008, 11, 352–359. [Google Scholar] [CrossRef] [PubMed]
- Greenwood, B.M.; Fidock, D.; Kyle, D.; Kappe, S.H.; Alonso, P.L.; Collins, F.H.; Duffy, P.E. Malaria: Progress, perils, and prospects for eradication. J. Clin. Investig. 2008, 118, 1266. [Google Scholar] [CrossRef]
- Cressman, G.; McKay, M.; Al-Mafazy, A.-W.; Ramsan, M.M.; Ali, A.S.; Garimo, I.A.; Mkali, H.; Ngondi, J.J. Using mobile technology to facilitate reactive case detection of malaria. Online J. Public Health Inform. 2017, 9, e068. [Google Scholar] [CrossRef]
- Perera, R.; Caldera, A.; Wickremasinghe, A.R. Reactive Case Detection (RACD) and foci investigation strategies in malaria control and elimination: A review. Malar. J. 2020, 19, 401. [Google Scholar] [CrossRef]
- Ferretti, L.; Wymant, C.; Kendall, M.; Zhao, L.; Nurtay, A.; Abeler-Dörner, L.; Parker, M.; Bonsall, D.G.; Fraser, C. Quantifying SARS-CoV-2 transmission suggests epidemic control with digital contact tracing. Science 2020, 368, eabb6936. [Google Scholar] [CrossRef]
- Aidoo, E.K.; Afrane, Y.; Machani, M.G.; Chebore, W.; Lawson, B.W.; Atieli, H.; Kariuki, S.; Lee, M.-C.; Koepfli, C.; Zhou, G.; et al. Reactive case detection of Plasmodium falciparum in western Kenya highlands: Effective in identifying additional cases, yet limited effect on transmission. Malar. J. 2018, 17, 111. [Google Scholar] [CrossRef]
- European Centre for Disease Prevention and Control. Resource Estimation for Contact Tracing, Quarantine and Monitoring Activities for COVID-19 Cases in the EU/EEA; ECDC: Stockholm, Sweden, 2020. [Google Scholar]
- Parker, D.M.; Landier, J.; Von Seidlein, L.; Dondorp, A.; White, L.; Hanboonkunupakarn, B.; Maude, R.J.; Nosten, F.H. Limitations of malaria reactive case detection in an area of low and unstable transmission on the Myanmar–Thailand border. Malar. J. 2016, 15, 571. [Google Scholar] [CrossRef] [Green Version]
- Nachega, J.B.; Atteh, R.; Ihekweazu, C.; Sam-Agudu, N.A.; Adejumo, P.; Nsanzimana, S.; Rwagasore, E.; Condo, J.; Paleker, M.; Mahomed, H.; et al. Contact tracing and the COVID-19 response in Africa: Best practices, key challenges, and lessons learned from Nigeria, Rwanda, South Africa, and Uganda. Am. J. Trop. Med. Hyg. 2021, 104, 1179. [Google Scholar] [CrossRef] [PubMed]
- Mastrandrea, R.; Fournet, J.; Barrat, A. Contact patterns in a high school: A comparison between data collected using wearable sensors, contact diaries and friendship surveys. PLoS ONE 2015, 10, e0136497. [Google Scholar] [CrossRef]
- Lochlainn, M.N.; Lee, K.A.; Sudre, C.H.; Varsavsky, T.; Cardoso, M.J.; Menni, C.; Bowyer, R.C.; Nguyen, L.H.; Drew, D.A.; Ganesh, S.; et al. Key predictors of attending hospital with COVID19: An association study from the COVID symptom Tracker APP in 2,618,948 individuals. medRxiv 2020. [Google Scholar] [CrossRef]
- Kind, C. Exit through the app store? Patterns 2020, 1, 100054. [Google Scholar] [CrossRef]
- Klenk, M.; Duijf, H. Ethics of digital contact tracing and COVID-19: Who is (not) free to go? Ethics Inf. Technol. 2021, 23, 69–77. [Google Scholar] [CrossRef] [PubMed]



Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Aidoo, E.K.; Squire, D.S.; Atuahene, O.O.-D.; Badu, K.; Botchway, F.A.; Osei-Adjei, G.; Sakyi, S.A.; Amoah, L.; Appiah, M.; Duku-Takyi, R.; et al. Joint COVID-19 Contact Tracing and Malaria Reactive Case Detection as Efficient Strategies for Disease Control. COVID 2022, 2, 1244-1252. https://doi.org/10.3390/covid2090091
Aidoo EK, Squire DS, Atuahene OO-D, Badu K, Botchway FA, Osei-Adjei G, Sakyi SA, Amoah L, Appiah M, Duku-Takyi R, et al. Joint COVID-19 Contact Tracing and Malaria Reactive Case Detection as Efficient Strategies for Disease Control. COVID. 2022; 2(9):1244-1252. https://doi.org/10.3390/covid2090091
Chicago/Turabian StyleAidoo, Ebenezer Krampah, Daniel Sai Squire, Obed Ohene-Djan Atuahene, Kingsley Badu, Felix Abekah Botchway, George Osei-Adjei, Samuel Asamoah Sakyi, Linda Amoah, Michael Appiah, Ruth Duku-Takyi, and et al. 2022. "Joint COVID-19 Contact Tracing and Malaria Reactive Case Detection as Efficient Strategies for Disease Control" COVID 2, no. 9: 1244-1252. https://doi.org/10.3390/covid2090091