1. Introduction
The world has been going through an existential pandemic of the COVID-19 disease since December 2019, and it has affected every aspect of our lives [
1]. This pandemic has had an intense social and economic impact on most countries. COVID-19 is characterized by a high transmissibility and has a significant mortality rate [
2]. All countries have been implementing several precautionary measures to ensure the safety of their citizens. More than 200 countries and territories have been reported to become infected by this virus. As of 29 June 2021, nearly 180 million confirmed cases of COVID-19 and four million deaths have been reported globally [
3].
Coronaviruses actually belong to the family of
Coronaviridae, which is a family of enveloped single-stranded positive-sense RNA viruses [
4]. The International Committee on Taxonomy of Viruses named the current discovered novel coronavirus as ‘SARS-CoV-2′, and the disease has been termed ‘COVID-19′ [
5,
6,
7]. SARS-CoV-2 has been listed as one of the novel Betacoronaviruses that infect human beings. It has been investigated that the SARS-CoV-2 is 88% identical to the other two coronaviruses, which were also discovered in China in 2018, i.e., bat-SL-CoVZC45 and bat-SL-CoVZXC21 [
8,
9]. A study from University College London (UCL) has identified 198 recurring mutations to the virus [
10]. The most common symptoms of COVID-19 are a fever, sneezing, cough, sore throat, throat swelling, headache, weakness, malaise, and breathlessness.
The most preferred technique for the diagnosis of COVID-19 is the ‘reverse transcription-polymerase chain reaction’ (RT-PCR) test. However, other non-contact techniques, such as pulmonary X-rays, computed tomography (CT) images, and high-resolution computed tomography (HRCT) images, are also preferred by clinicians [
11]. Deep learning and artificial intelligence (AI), in this respect, play a vital role in the accurate detection of COVID-19. In the field of medical data analysis, deep neural networks and AI rapidly gained popularity because they happen to be the most suitable for big data analysis [
12]. Deep learning models, especially convolutional neural networks (CNN), are able to automatically learn multiple level of features from data in a hierarchical manner [
13]. Furthermore, the interest in the detection of COVID-19 using deep learning and convolutional neural network (CNN) is rapidly increasing.
Recently, quite a few studies have been conducted on the applications of artificial intelligence for the detection and classification of COVID-19. For example, regarding pre-trained models, five pre-trained models, i.e., ResNet-50, ResNet-101, ResNet-152, and Inception-ResNet-v2 were used in [
14]. The study uses a dataset of four classes, i.e., ‘COVID’ with 341 images, ‘normal’ with 2800 images, ‘viral pneumonia’ with 1493 images, and ‘bacterial pneumonia’ with 2772 images. However, the pre-trained models have been tested on only two classes at a time for each model, i.e., ‘COVID’ vs. ‘normal’, ‘COVID’ vs. ‘viral pneumonia’, ‘COVID’ vs. ‘bacterial pneumonia’. Similarly, Ref. [
15] presents five pre-trained models for three classes in total. The used models are VGG19, MobileNetV2, Inception, Xception, Inception, and ResNet v2. The best performance is achieved on MobileNetV2, with 96.78% accuracy. Furthermore, a computer-aided detection (CAD) was implemented on ResNet-50, Inception V3, DenseNet-201, and Xception in [
16]. This study focuses on and presents the division of a highly imbalanced training dataset into a group of small balanced datasets. The use of pre-trained models was also presented in [
17], where VGG16, Inception ResNetV2, ResNet-50, Densenet-201, VGG19, MobileNetV2, and NasNet Mobile were utilized. This research utilizes 400 CT scan images and 400 X-ray images, each containing 200 COVID and 200 normal images.
Some of the modified CNN models have also been reported. For example, in [
18], a VGG16 based modified CNN was presented, which is named ‘Corona-Net’. The presented model utilizes a three-class classification with two phases, i.e., a re-initialization phase and a classification phase for the detection of COVID-19. Similarly, another modified CNN is presented in [
19], in which several parameters have been optimized for the loss minimization purpose. In addition to a training dataset, two external datasets for validation purposes have been utilized. Likewise, VGG16 and VGG19 models have been used in [
20] as backbone networks to evaluate the layer depth of the same CNN architecture. Each backbone network has been trained and evaluated with different degrees of fine tuning. In addition to the aforementioned modified CNNs, a modified inception model is presented in [
21], where 1065 CT scan images were used. The presented accuracy is 89.5%. A multi-view fusion deep learning network based on ResNet-50 is presented in [
22]. A total of 368 COVID-19 and 127 pneumonia images were used. The idea is to train the model in multi-view images of chest CT images, which improves the efficacy of the diagnosis.
Some other methods have also been reported, and one such model is presented in [
23]. This study utilized Inception-ResNet-v2 as the based model. The presented model is named ‘CoVIR-Net’. They exhibited two approaches: CoVIR-Net with Inception-Resnet-v2 residual blocks and the CoVIR-Net feature extractor with a random forest classifier. The two approaches presented accuracies of 95.78% and 97.29%, respectively. Another method named by the authors as ‘COVID-Net’ is presented in [
24]. The presented architecture utilizes a lightweight residual PEPX (projection-expansion-projection-extension) design pattern. The presented article utilizes an open-source dataset, COVIDx. This dataset has 13,975 X-ray images that have been collected from 13,870 patient cases. The presented model reports a 93.3% test accuracy. Similarly, a ResNet-50-based model termed ‘DREnet’ is presented in [
25]. It was used for the diagnosis of CT images that were divided into three classes. The achieved accuracy is reported as 89.36%. A modified model named ‘DeCoVNet’ has been presented in [
26], which use UNet as the base model. The presented model was tested on 499 CT scan images, with an accuracy of 95.9%. In addition, a model called ‘DarkCovidNet’ is presented in [
27], in which the DarkNet model has been utilized as a classifier for the YOLO real time object selection. It exhibited a binary and multiclass accuracy of 98.08% and 87.02%, respectively. Another model, named ‘Coronet’, is presented in [
28], with the use of Xception as the base model. A total of 203 normal and 660 bacterial pneumonia images were used. The reported accuracy is 89.6%.
A comparative study was performed in [
29] using ResNet-18, ResNet-50, COVID-NET, and DenseNet-121 on Pytorch 1.4. The collection of a custom dataset was reported (named as ‘CORDA’), which consists of data of 386 patients from a hospital in Turin, Italy. Six other publicly available datasets were also utilized. In addition to the implementation of the aforementioned models, authors have also used a new convolutional neural network comprising of eight convolution layers and a fully connected layer. This new model has been named ’Conv8’. The use of this smaller architecture did not perform well in comparison to large models, such as ResNet-18, but presented acceptable results, with a BA of 0.61 and DOR of 2.38. The main constraint of the study was the lack of availability of a large dataset. The authors suggested that these models can perform quite well upon the availability of a larger dataset. In comparison, the re-search work in this paper focuses on the use of fine tuning and transfer learning by utilizing the pre-trained weights through freezing the pre-trained layers. Only the weights of the last two layers have been re-trained/updated. Furthermore, a large dataset of 7232 images has been used in this research, which improves the accuracies of the models used in this paper. Moreover, the testing dataset has been segregated from the training and validation datasets. Apart from this segregated dataset, a locally collected dataset of 450 images has also been utilized for the purpose of testing and prediction.
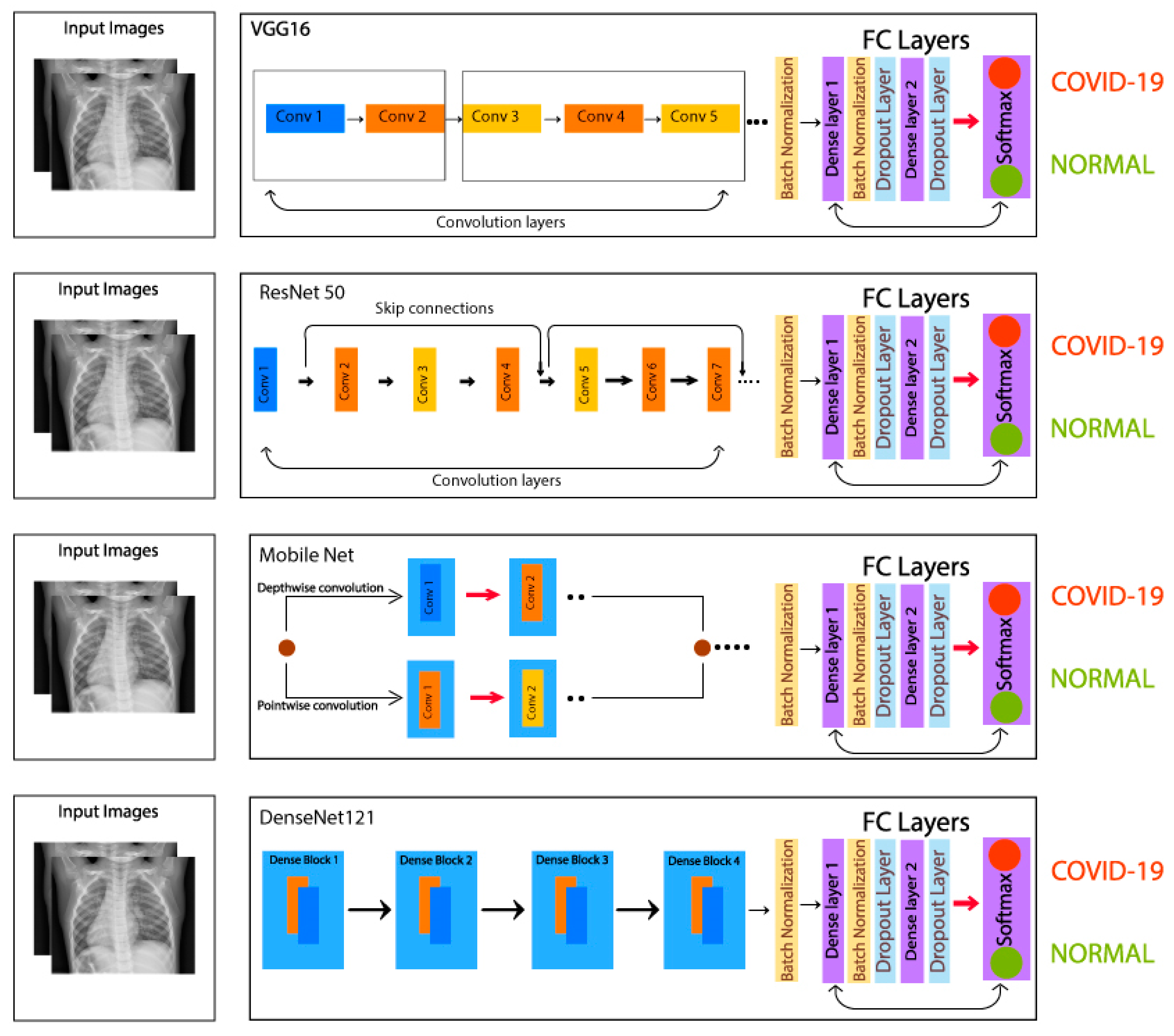
In this research, the transfer learning technique is used to detect COVID-19 from the pulmonary (chest) X-rays. For this purpose, four pre-trained CNN models, i.e., VGG16, ResNet50, MobileNet, and DenseNet-121 have been used. In order to utilize both the transfer learning technique and the fine-tuning on the aforementioned pre-trained models, batch normalization and dropout layers are added in the FC layer. Details on the implementation of transfer learning are given in
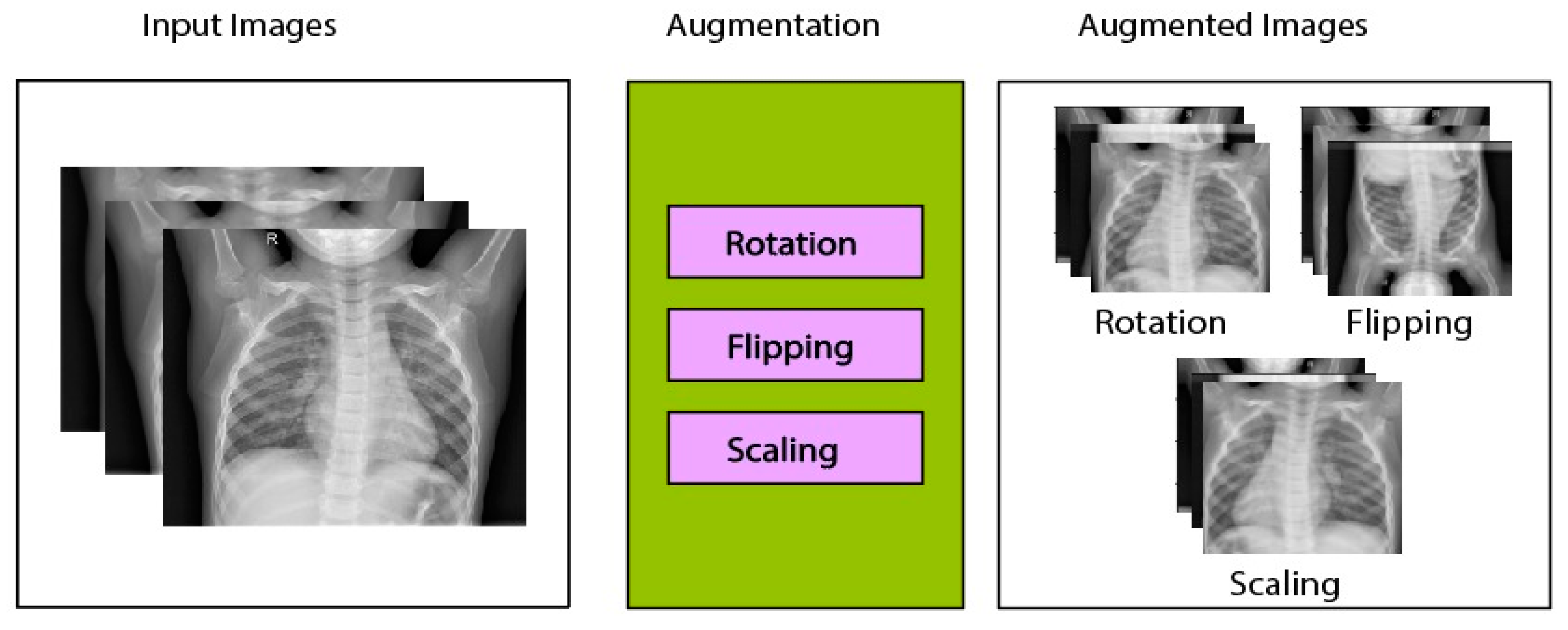
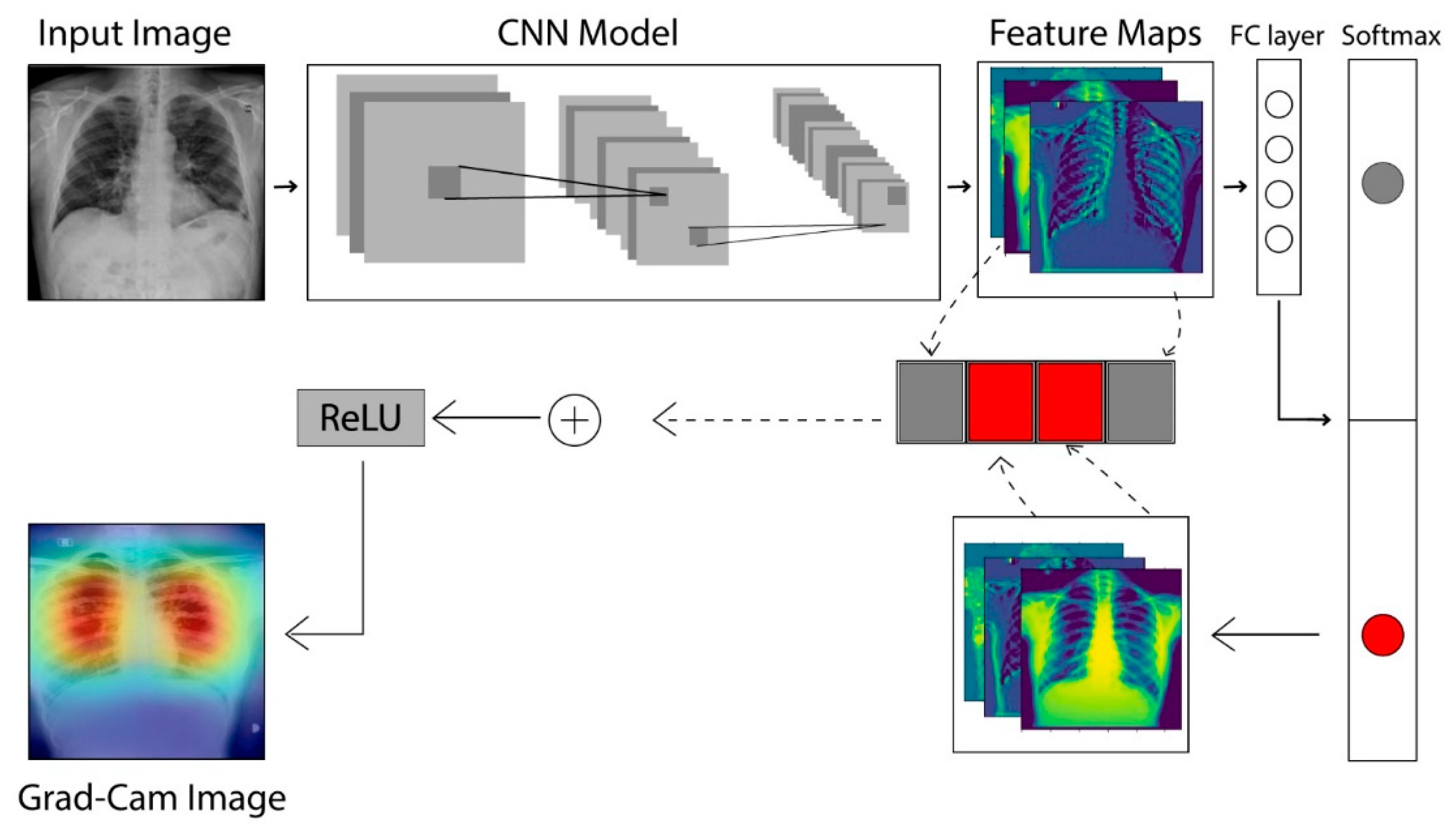
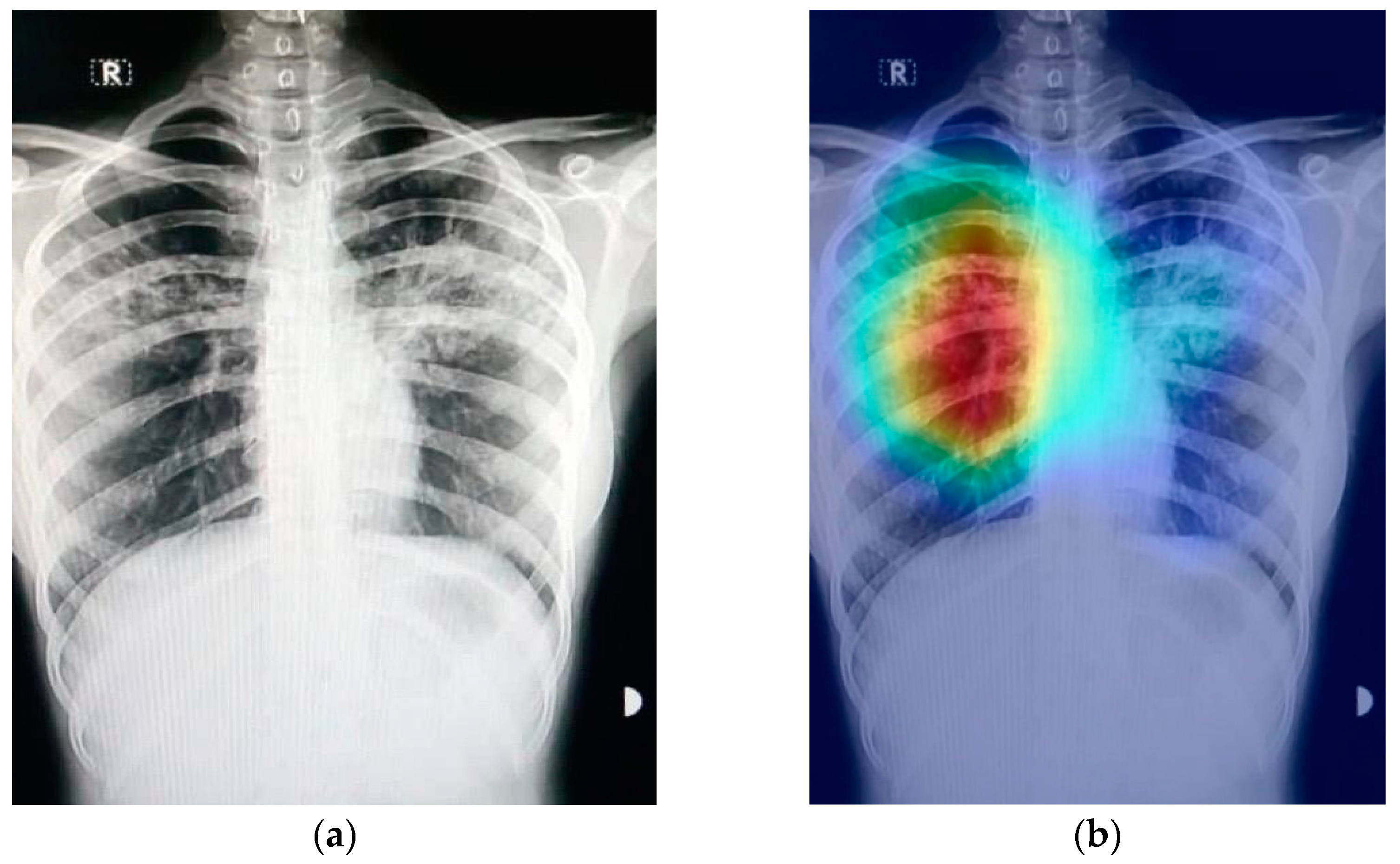
Section 2.3. The models under study have been compared on the basis of important parameters, such as the number of epochs, batch size, learning rate, etc. Suggestions have been made on the basis of comparison and critical analysis. The models have been tested on 450 indigenously collected X-ray images of Pakistani patients. Finally, the Grad-CAM technique has been applied in order to create class-specific heatmap images to highlight the features that are extracted from the X-ray images. Various optimizers, i.e., Adam, the stochastic gradient descent (SGD), Adadelta, and RMSprop from Keras version 2.6.0 have been used for error minimization purpose. It is noteworthy to mention here that the pretrained models had originally been trained on the Imagenet dataset, which consisted of millions of images with multiple classes. Whereas, in this research, these models have been retrained on 5062 images assessed through the Kaggle website for two classes only. By utilizing transfer learning and fine tuning, a higher accuracy is achieved for each model. Tensorflow and Keras API is used for the processing of these models. This study was performed on a 12 GB NVIDIA Tesla K80 GPU that was provided online by Google Colab, a product of Google Research headquartered at Mountain View, CA, United States.
4. Conclusions
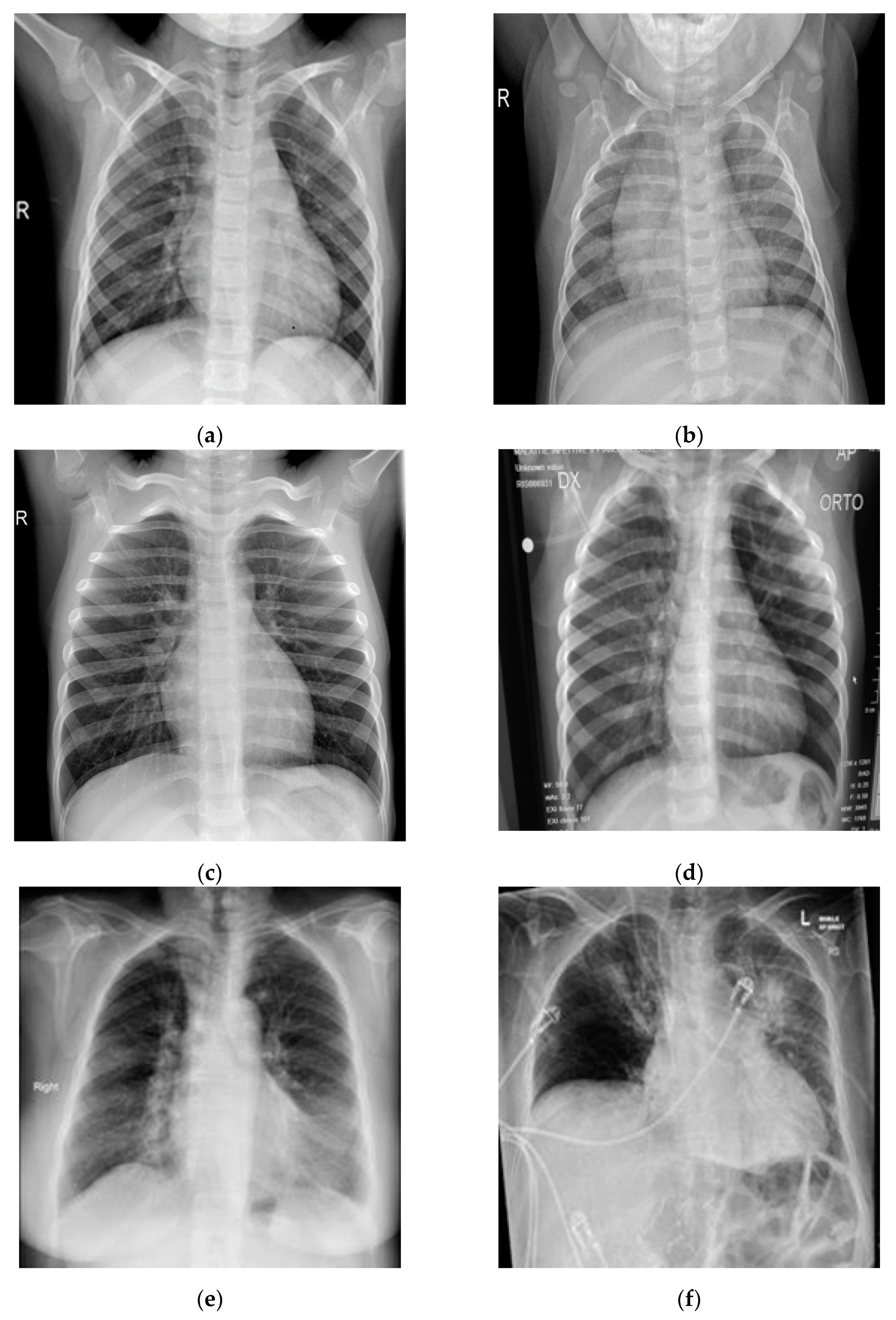
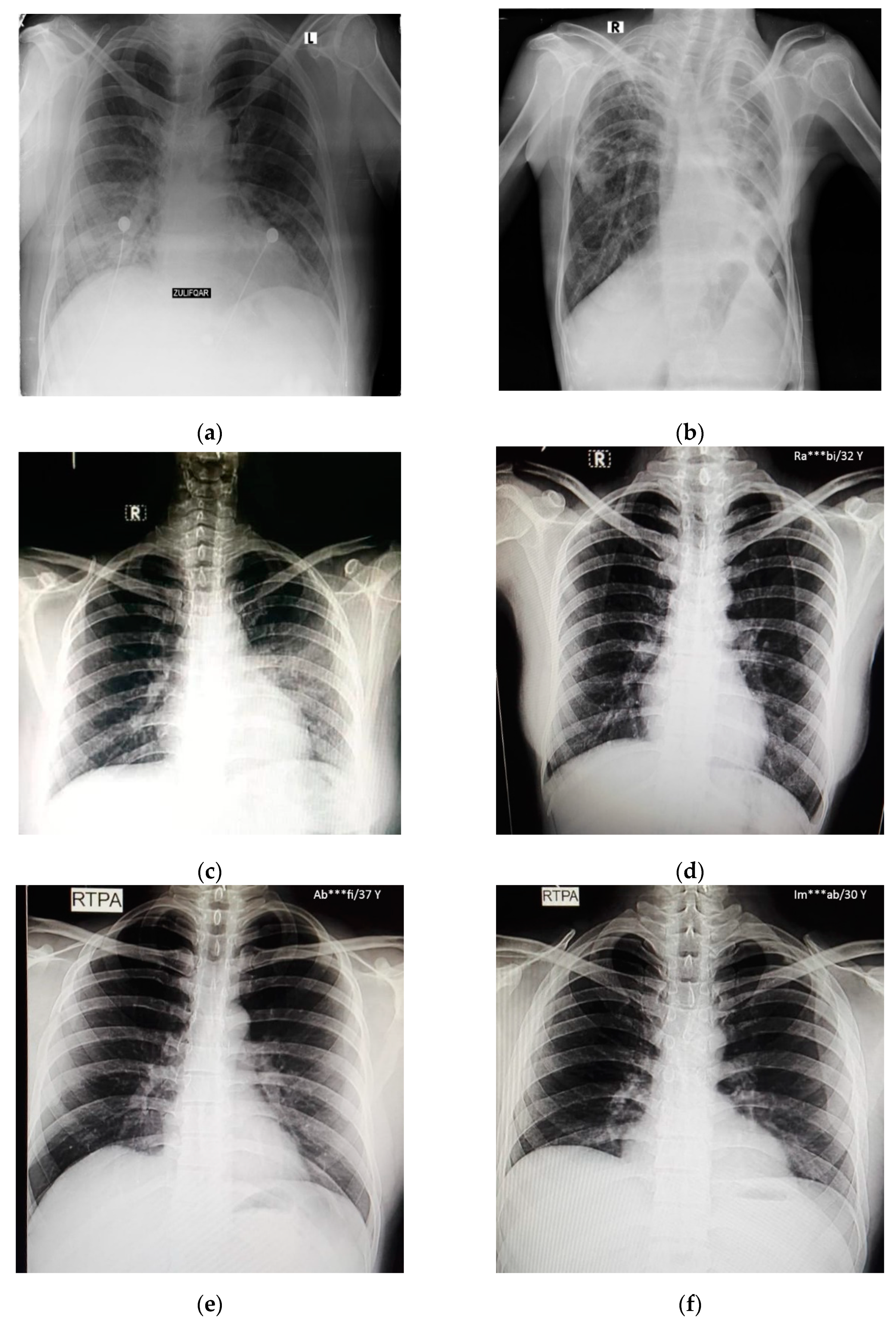
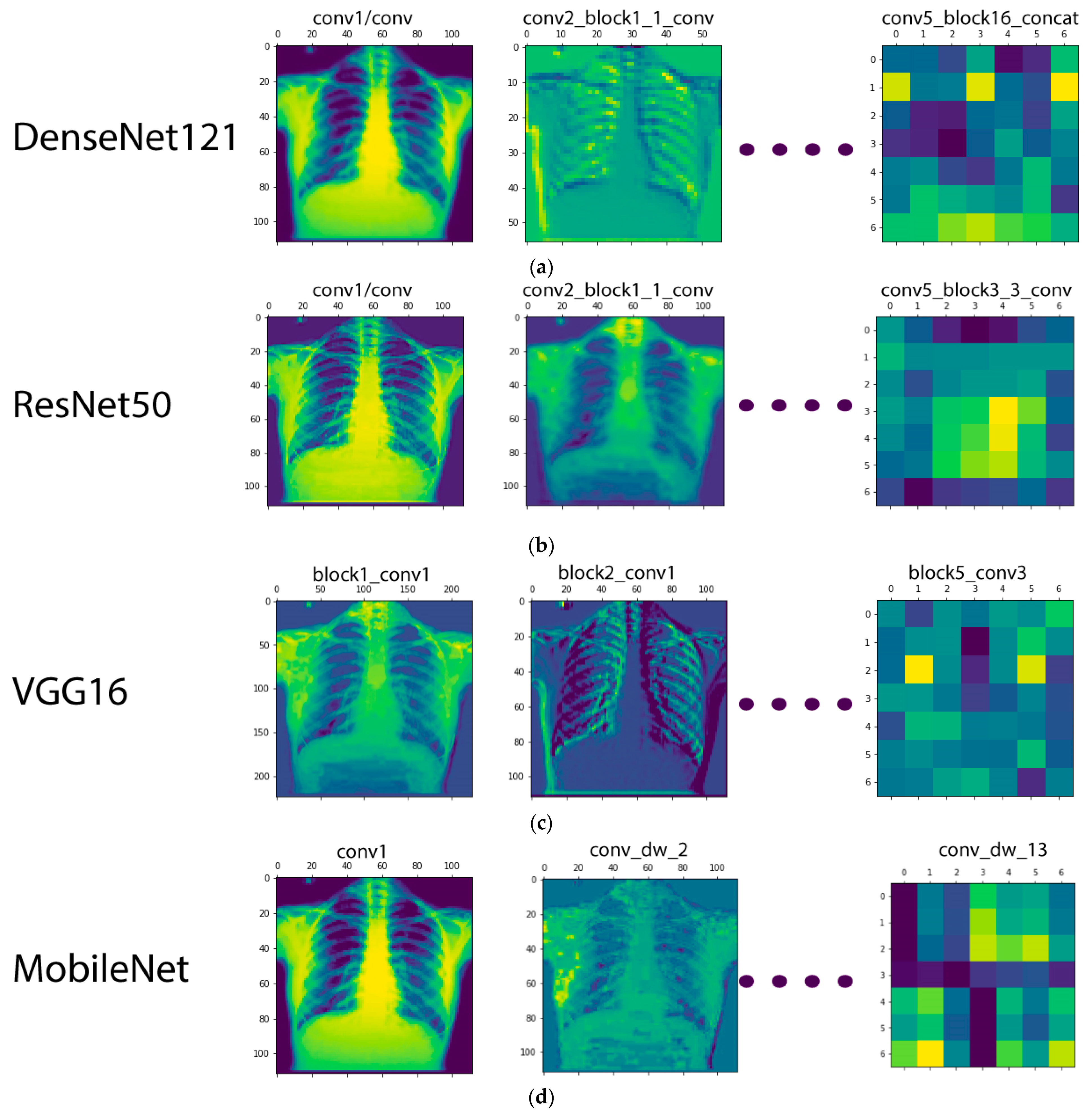
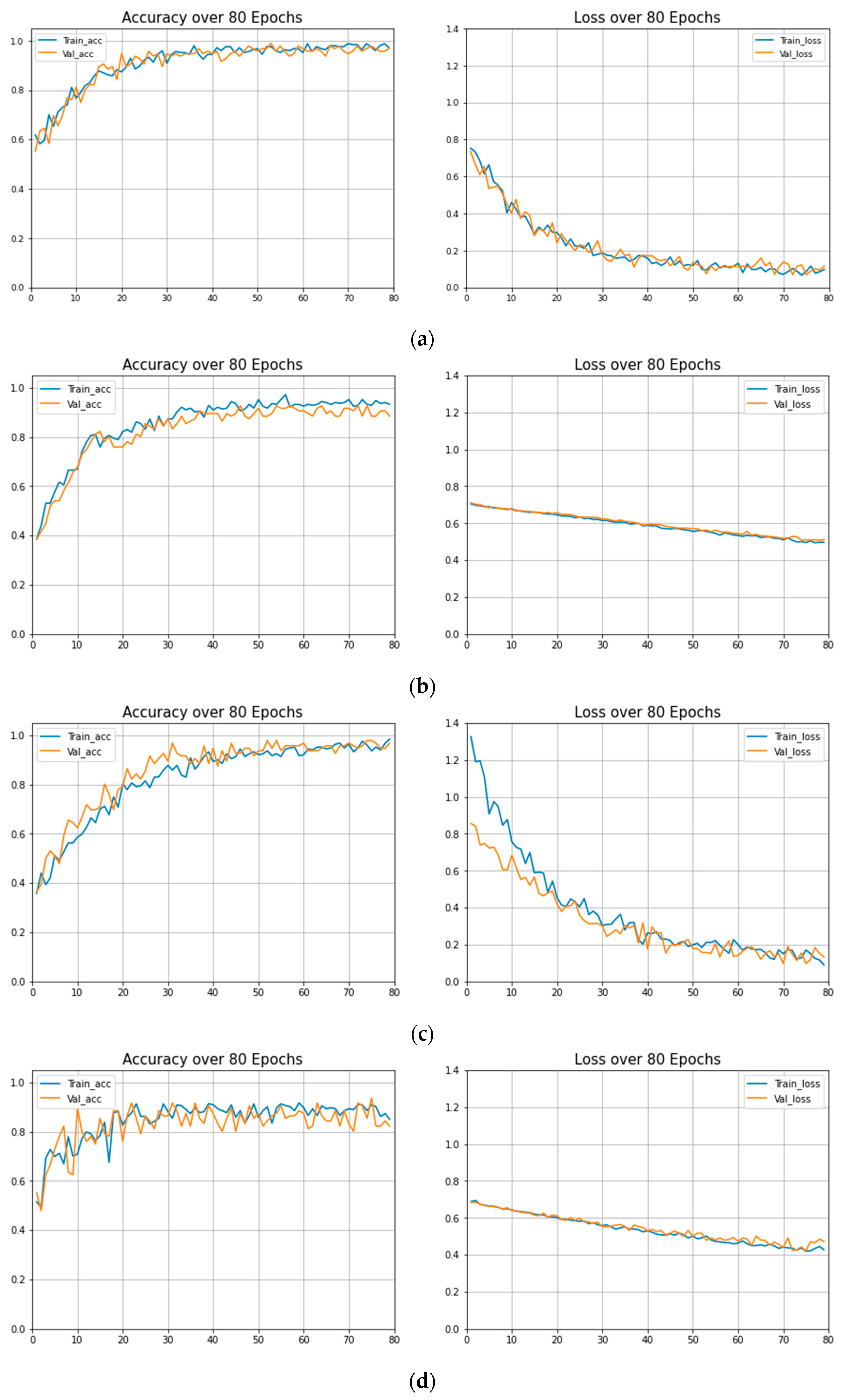
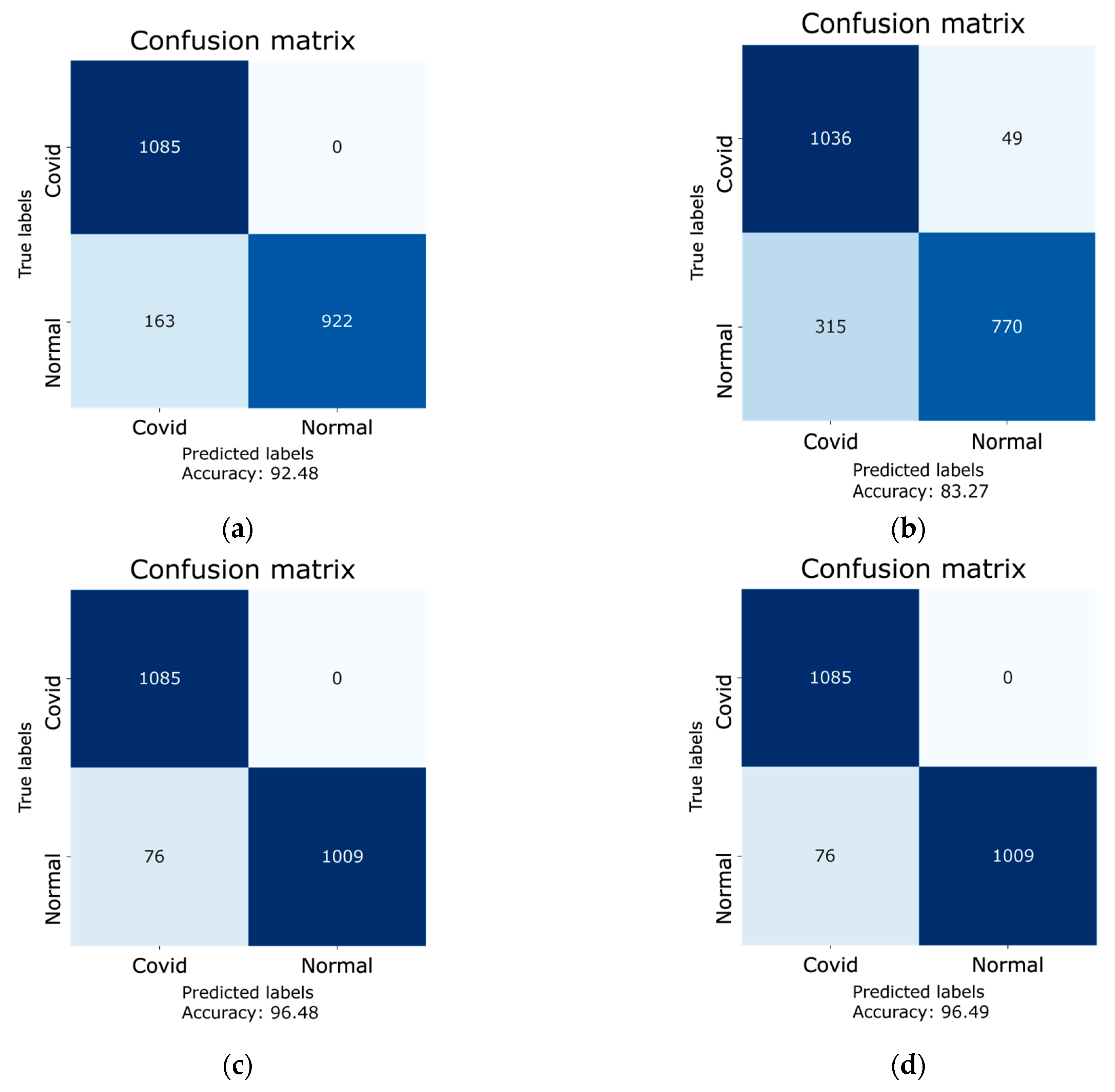
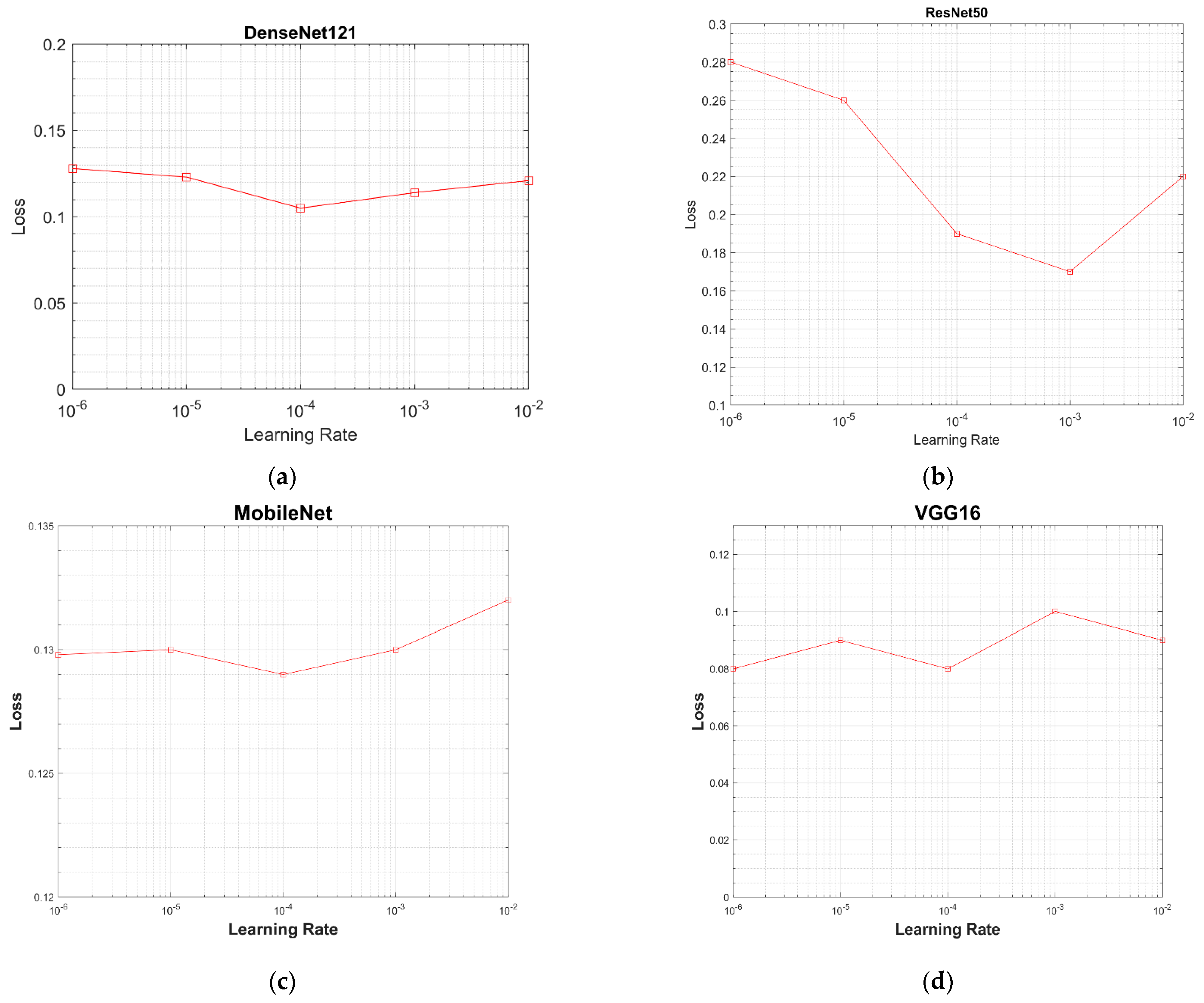
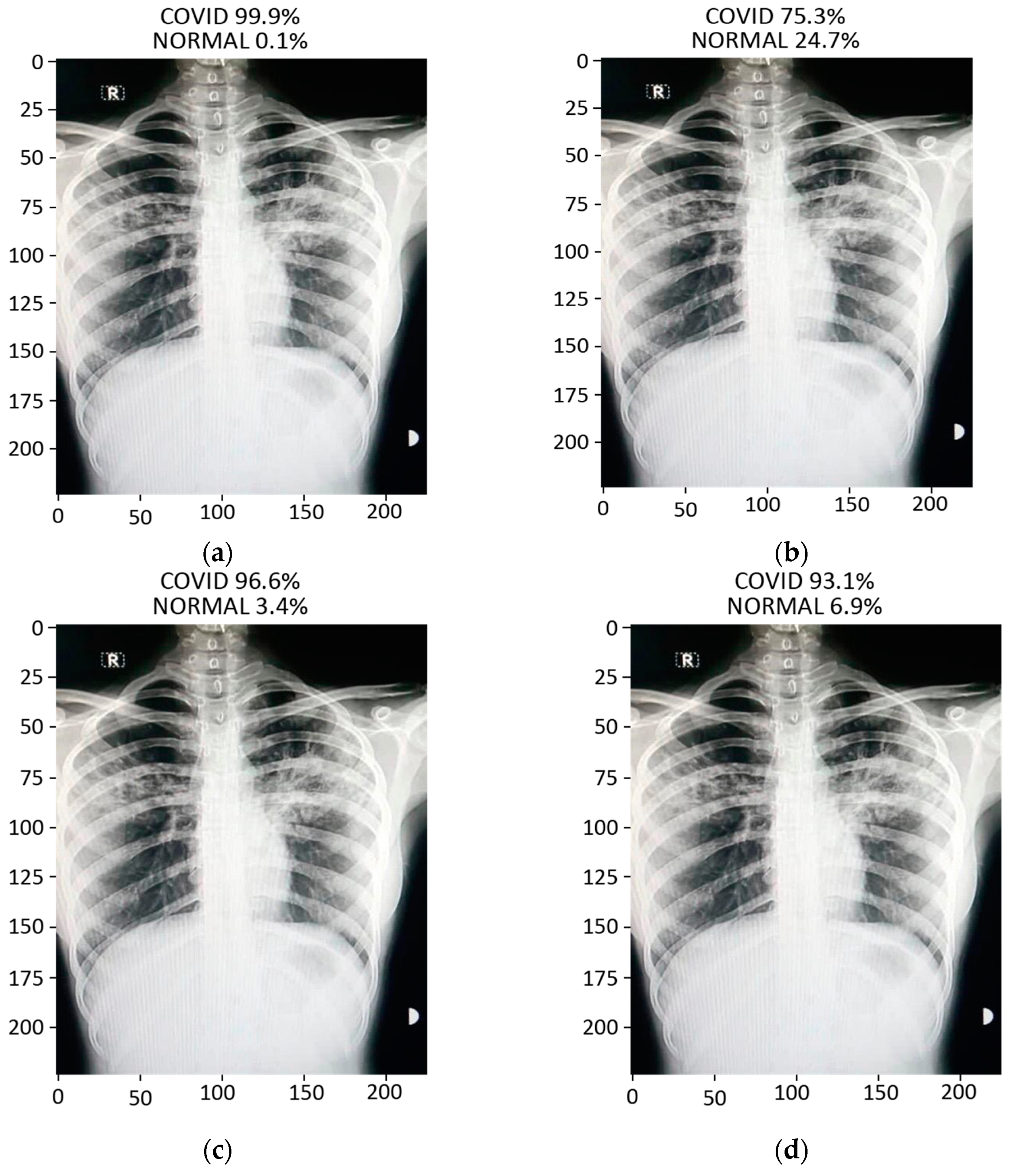
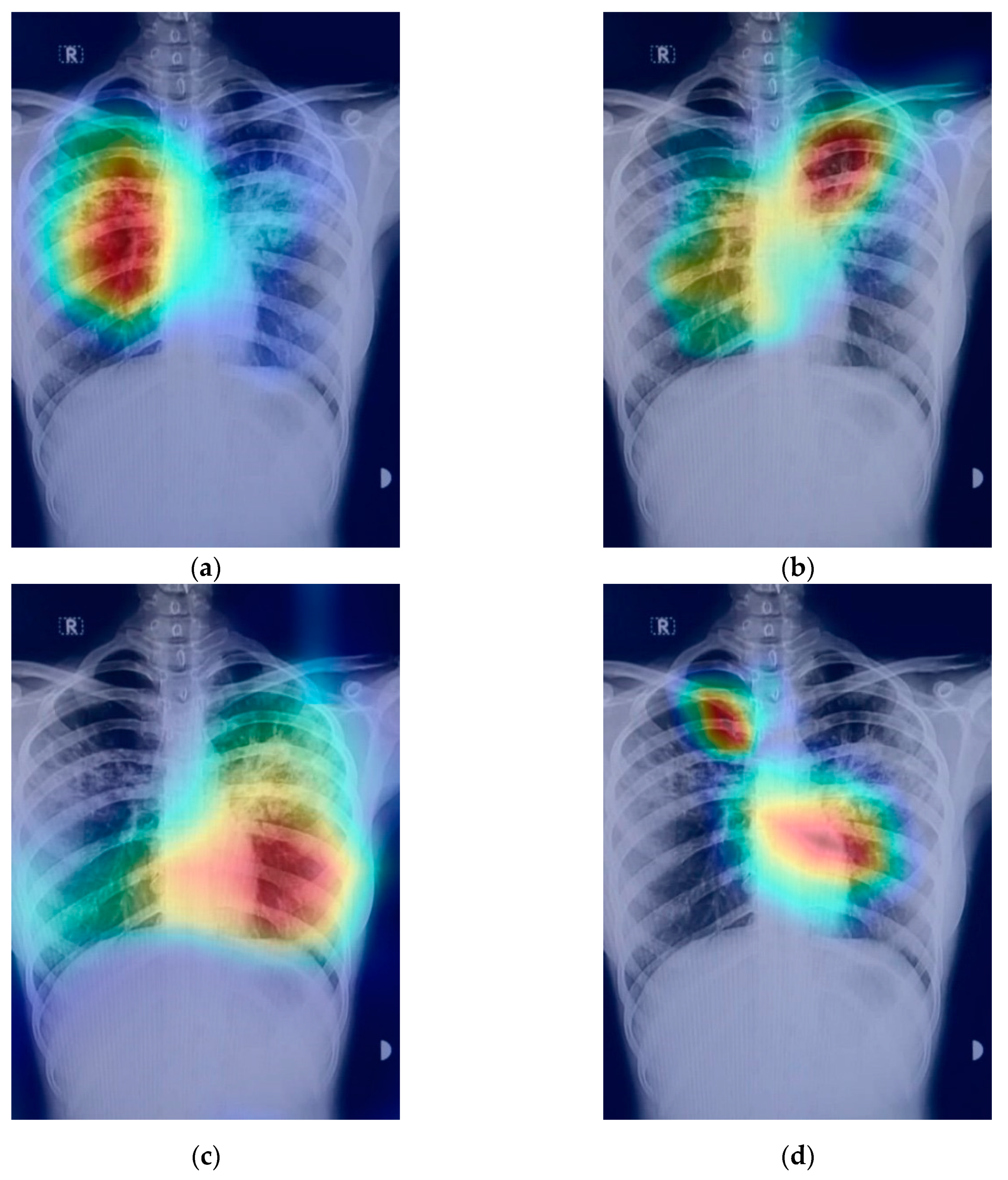
In this paper, we applied transfer learning technique with fine tuning on the four pre-trained models (VGG16, ResNet-50, MobileNet, and DenseNet-121) in order to detect COVID-19 using chest X-ray images acquired from a hospital in Pakistan. The models under study were trained using the dataset of more than 3600 COVID-19 and normal chest X-ray images, whereas an indigenously collected dataset of 450 X-ray images of Pakistani patients were used for testing and prediction purposes. Various important parameters, e.g., recall, specificity, F1-score, precision, loss graphs, and confusion matrices were used to validate the accuracy of the models. The VGG16 model exhibited the least accurate performance in classifying the COVID-19 and normal chest X-ray images; however, the DenseNet-121 displayed promising results in the classification of the COVID-19 and normal images. The achieved accuracies of VGG16, ResNet-50, DenseNet-121, and MobileNet are 83.27%, 92.48%, 96.49%, and 96.48%, respectively. Furthermore, in order to highlight the area where the model is paying the most attention during feature extraction, the Grad-CAM technique was also applied to create class-specific heatmap images. Various optimizers were tested, and among all of the optimizers under study, the ‘RMSprop’ optimizer exhibited the best performance and hence was applied for the error minimization and better optimization in the training procedure.


 ,
, 


















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}