
Liver Injury and Elevated FIB-4 Define a High-Risk Group in Patients with COVID-19

 , ,
, ,  add
Show full author list
add
Show full author list
Abstract
:1. Introduction
Aims
2. Materials and Methods
2.1. Study Design and Participants
2.2. Baseline Evaluation
2.3. Non-Invasive Scores
2.4. Follow-Up
2.5. Ethical Considerations
2.6. Statistical Analysis
3. Results
3.1. Baseline Characteristics
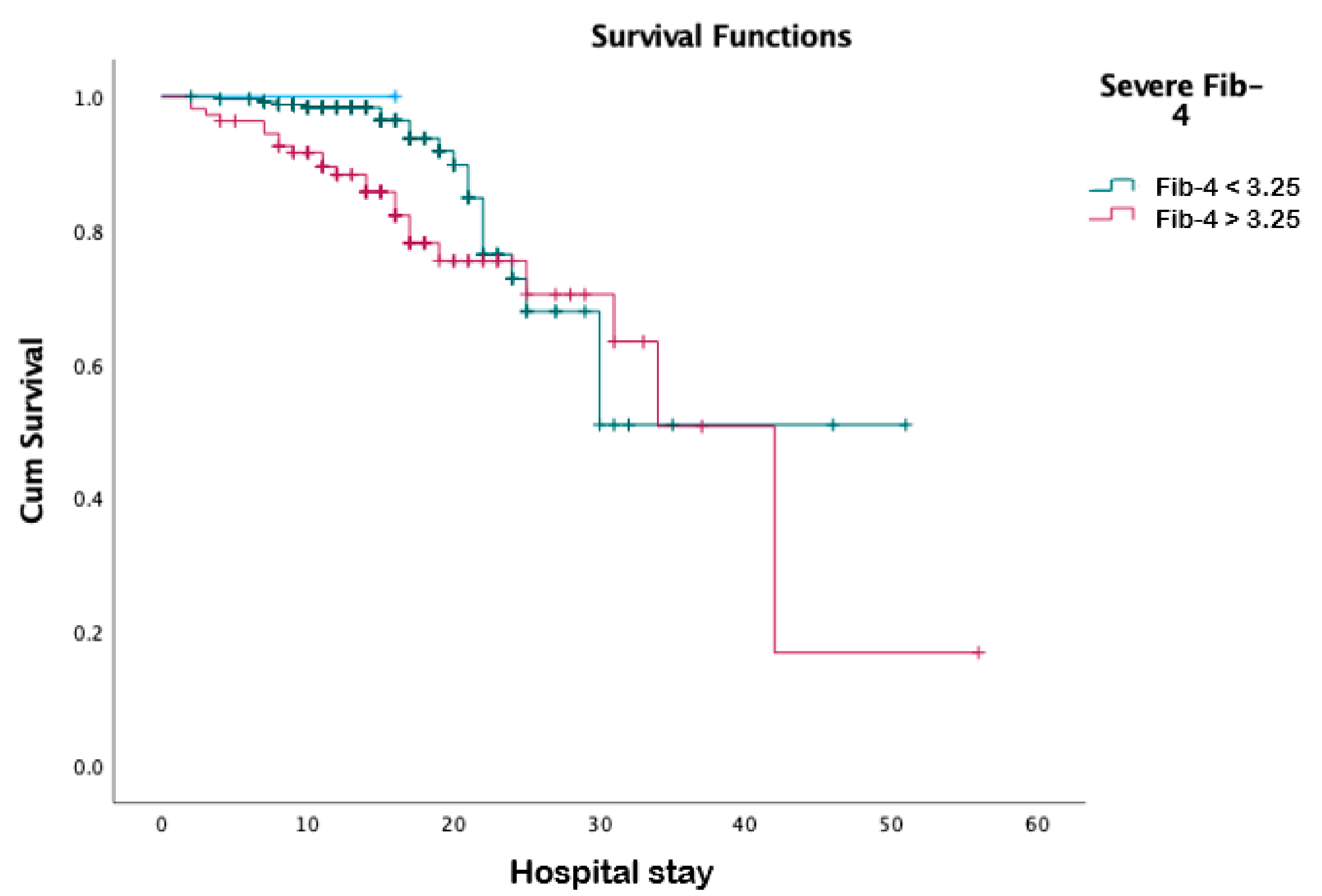
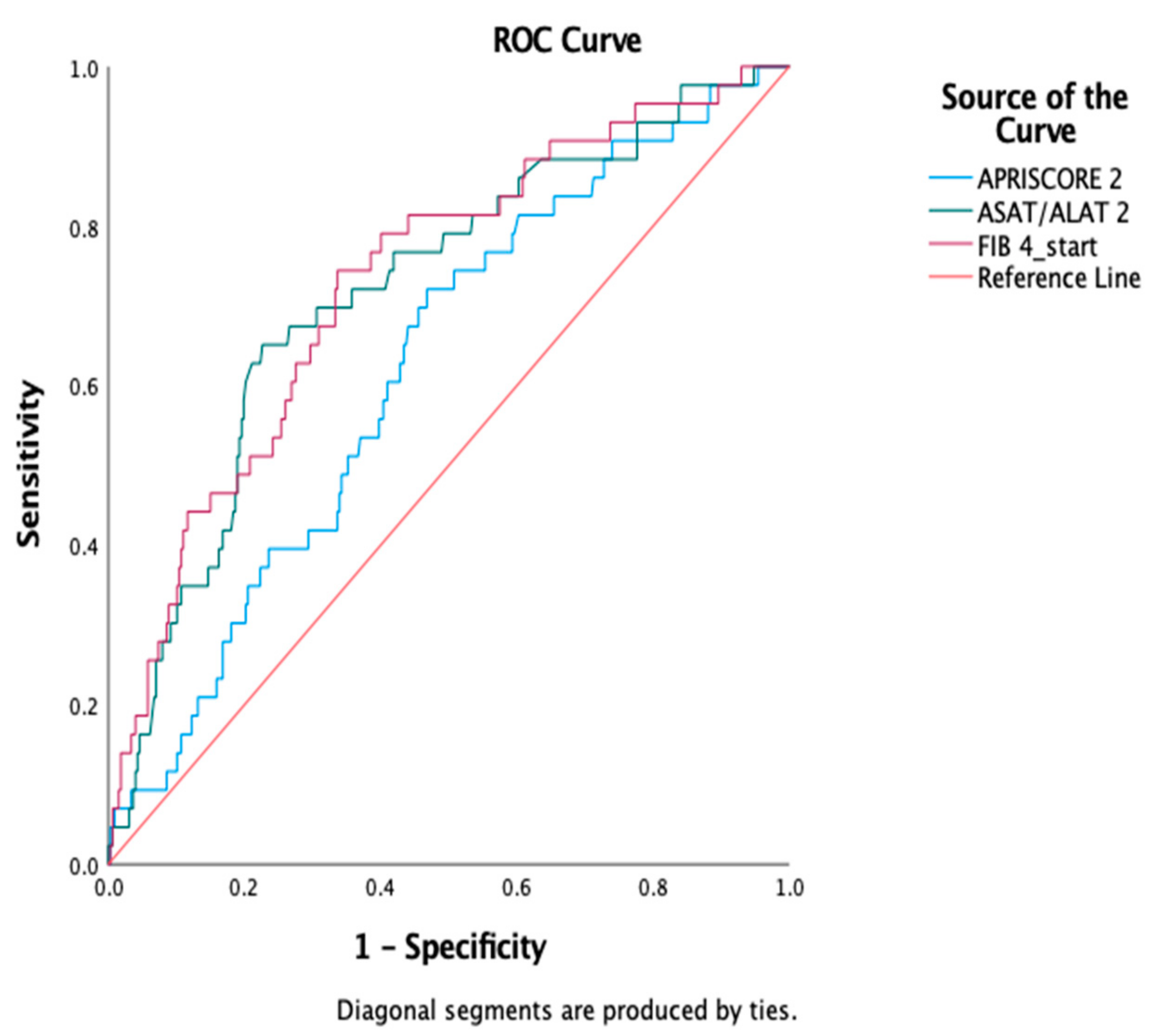
3.2. Univariate Outcome Analysis
3.3. Multivariate Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Fajgenbaum, D.C.; June, C.H. Cytokine Storm. N. Engl. J. Med. 2020, 383, 2255–2273. [Google Scholar] [CrossRef]
- Nishiga, M.; Wang, D.W.; Han, Y.; Lewis, D.B.; Wu, J.C. COVID-19 and cardiovascular disease: From basic mechanisms to clinical perspectives. Nat. Rev. Cardiol. 2020, 17, 543–558. [Google Scholar] [CrossRef] [PubMed]
- Feldman, E.L.; Savelieff, M.G.; Hayek, S.S.; Pennathur, S.; Kretzler, M.; Pop-Busui, R. COVID-19 and Diabetes: A Collision and Collusion of Two Diseases. Diabetes 2020, 69, 2549–2565. [Google Scholar] [CrossRef]
- Stefan, N.; Birkenfeld, A.L.; Schulze, M.B.; Ludwig, D.S. Obesity and impaired metabolic health in patients with COVID-19. Nat. Rev. Endocrinol. 2020, 16, 341–342. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fung, M.; Nambiar, A.; Pandey, S.; Aldrich, J.M.; Teraoka, J.; Freise, C.; Roberts, J.; Chandran, S.; Hays, S.R.; Bainbridge, E.; et al. Treatment of immunocompromised COVID-19 patients with convalescent plasma. Transpl. Infect. Dis. 2021, 23, e13477. [Google Scholar] [CrossRef] [PubMed]
- Brenner, E.J.; Ungaro, R.C.; Gearry, R.B.; Kaplan, G.G.; Kissous-Hunt, M.; Lewis, J.D.; Ng, S.C.; Rahier, J.-F.; Reinisch, W.; Ruemmele, F.M.; et al. Corticosteroids, But Not TNF Antagonists, Are Associated with Adverse COVID-19 Outcomes in Patients with Inflammatory Bowel Diseases: Results from an International Registry. Gastroenterology 2020, 159, 481–491. [Google Scholar] [CrossRef] [PubMed]
- Tian, Y.; Qiu, X.; Wang, C.; Zhao, J.; Jiang, X.; Niu, W.; Huang, J.; Zhang, F. Cancer associates with risk and severe events of COVID -19: A systematic review and meta-analysis. Int. J. Cancer 2021, 148, 363–374. [Google Scholar] [CrossRef] [PubMed]
- Jothimani, D.; Venugopal, R.; Abedin, M.F.; Kaliamoorthy, I.; Rela, M. COVID-19 and the liver. J. Hepatol. 2020, 73, 1231–1240. [Google Scholar] [CrossRef] [PubMed]
- Sterling, R.K.; Lissen, E.; Clumeck, N.; Sola, R.; Correa, M.C.; Montaner, J.; Sulkowski, M.S.; Torriani, F.J.; Dieterich, D.T.; Thomas, D.L.; et al. Development of a simple noninvasive index to predict significant fibrosis in patients with HIV/HCV coinfection. Hepatology 2006, 43, 1317–1325. [Google Scholar] [CrossRef] [PubMed]
- Vilar-Gomez, E.; Chalasani, N. Non-invasive assessment of non-alcoholic fatty liver disease: Clinical prediction rules and blood-based biomarkers. J. Hepatol. 2018, 68, 305–315. [Google Scholar] [CrossRef]
- Ibáñez-Samaniego, L.; Bighelli, F.; Usón, C.; Caravaca, C.; Carrillo, C.F.; Romero, M.; Barreales, M.; Perelló, C.; Madejón, A.; Marcos, A.C.; et al. Elevation of Liver Fibrosis Index FIB-4 Is Associated with Poor Clinical Outcomes in Patients With COVID-19. J. Infect. Dis. 2020, 222, 726–733. [Google Scholar] [CrossRef] [PubMed]
- Romero-Cristóbal, M.; Clemente-Sánchez, A.; Piñeiro, P.; Cedeño, J.; Rayón, L.; del Río, J.; Ramos, C.; Hernández, D.-A.; Cova, M.; Caballero, A.; et al. Possible unrecognised liver injury is associated with mortality in critically ill COVID-19 patients. Ther. Adv. Gastroenterol. 2021, 14, 17562848211023410. [Google Scholar] [CrossRef]
- Campos-Murguía, A.; Román-Calleja, B.M.; Toledo-Coronado, I.V.; González-Regueiro, J.A.; Solís-Ortega, A.A.; Kúsulas-Delint, D.; Cruz-Contreras, M.; Cruz-Yedra, N.; Cubero, F.J.; Nevzorova, Y.A.; et al. Liver fibrosis in patients with metabolic associated fatty liver disease is a risk factor for adverse outcomes in COVID-19. Dig. Liver Dis. 2021, 53, 525–533. [Google Scholar] [CrossRef]
- Xiang, F.; Sun, J.; Chen, P.-H.; Han, P.; Zheng, H.; Cai, S.; Kirk, G.D. Early Elevation of Fibrosis-4 Liver Fibrosis Score Is Associated with Adverse Outcomes among Patients with Coronavirus Disease 2019. Clin. Infect. Dis. 2021, 73, e594–e601. [Google Scholar] [CrossRef] [PubMed]
- Wai, C.-T.; Greenson, J.K.; Fontana, R.J.; Kalbfleisch, J.D.; Marrero, J.A.; Conjeevaram, H.S.; Lok, A.S.-F. A simple noninvasive index can predict both significant fibrosis and cirrhosis in patients with chronic hepatitis C. Hepatology 2003, 38, 518–526. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lin, Z.-H.; Xin, Y.-N.; Dong, Q.-J.; Wang, Q.; Jiang, X.-J.; Zhan, S.-H.; Sun, Y.; Xuan, S.-Y. Performance of the aspartate aminotransferase-to-platelet ratio index for the staging of hepatitis C-related fibrosis: An updated meta-analysis. Hepatology 2011, 53, 726–736. [Google Scholar] [CrossRef] [PubMed]
- Giannini, E.; Risso, D.; Botta, F.; Chiarbonello, B.; Fasoli, A.; Malfatti, F.; Romagnoli, P.; Testa, E.; Ceppa, P.; Testa, R. Validity and Clinical Utility of the Aspartate Aminotransferase–Alanine Aminotransferase Ratio in Assessing Disease Severity and Prognosis in Patients with Hepatitis C Virus–Related Chronic Liver Disease. Arch. Intern. Med. 2003, 163, 218–224. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Adenote, A.; Dumic, I.; Madrid, C.; Barusya, C.; Nordstrom, C.W.; Prada, L.R. NAFLD and Infection, a Nuanced Relationship. Can. J. Gastroenterol. Hepatol. 2021, 2021, 5556354. [Google Scholar] [CrossRef]
- Pan, L.; Huang, P.; Xie, X.; Xu, J.; Guo, D.; Jiang, Y. Metabolic associated fatty liver disease increases the severity of COVID-19: A meta-analysis. Dig. Liver Dis. 2020, 53, 153–157. [Google Scholar] [CrossRef]
- Mushtaq, K.; Khan, M.U.; Iqbal, F.; Alsoub, D.H.; Chaudhry, H.S.; Ata, F.; Iqbal, P.; Elfert, K.; Balaraju, G.; Almaslamani, M.; et al. NAFLD is a predictor of liver injury in COVID-19 hospitalized patients but not of mortality, disease severity on the presentation or progression—The debate continues. J. Hepatol. 2021, 74, 482–484. [Google Scholar] [CrossRef]
- Ji, D.; Cheng, G.; Lau, G. Reply to: “NAFLD is a predictor of liver injury in COVID-19 hospitalized patients but not of mortality, disease severity on the presentation or progression—The debate continues. J. Hepatol. 2020, 74, 484–485. [Google Scholar] [CrossRef]
- Li, K.; Fang, Y.; Li, W.; Pan, C.; Qin, P.; Zhong, Y.; Liu, X.; Huang, M.; Liao, Y.; Li, S. CT image visual quantitative evaluation and clinical classification of coronavirus disease (COVID-19). Eur. Radiol. 2020, 30, 4407–4416. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McPherson, S.; Hardy, T.; Dufour, J.-F.; Petta, S.; Romero-Gómez, M.; Allison, M.; Oliveira, C.P.; Francque, S.; Van Gaal, L.; Schattenberg, J.M.; et al. Age as a Confounding Factor for the Accurate Non-Invasive Diagnosis of Advanced NAFLD Fibrosis. Am. J. Gastroenterol. 2017, 112, 740–751. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, C.; Shi, L.; Wang, F.-S. Liver injury in COVID-19: Management and challenges. Lancet Gastroenterol. Hepatol. 2020, 5, 428–430. [Google Scholar] [CrossRef]
- Alqahtani, S.; Schattenberg, J.M. Liver injury in COVID-19: The current evidence. United Eur. Gastroenterol. J. 2020, 8, 509–519. [Google Scholar] [CrossRef]
- Lei, F.; Liu, Y.; Zhou, F.; Qin, J.; Zhang, P.; Zhu, L.; Zhang, X.; Cai, J.; Lin, L.; Ouyang, S.; et al. Longitudinal Association between Markers of Liver Injury and Mortality in COVID-19 in China. Hepatology 2020, 72, 389–398. [Google Scholar] [CrossRef] [PubMed]
- Qi, X.; Liu, Y.; Wang, J.; Fallowfield, J.A.; Wang, J.; Li, X.; Shi, J.; Pan, H.; Zou, S.; Zhang, H.; et al. Clinical course and risk factors for mortality of COVID-19 patients with pre-existing cirrhosis: A multicentre cohort study. Gut 2020, 70, 433–436. [Google Scholar] [CrossRef] [PubMed]
- Singh, S.; Khan, A. Clinical Characteristics and Outcomes of Coronavirus Disease 2019 among Patients with Preexisting Liver Disease in the United States: A Multicenter Research Network Study. Gastroenterology 2020, 159, 768–771. [Google Scholar] [CrossRef]
- Iavarone, M.; D’Ambrosio, R.; Soria, A.; Triolo, M.; Pugliese, N.; Del Poggio, P.; Perricone, G.; Massironi, S.; Spinetti, A.; Buscarini, E.; et al. High rates of 30-day mortality in patients with cirrhosis and COVID-19. J. Hepatol. 2020, 73, 1063–1071. [Google Scholar] [CrossRef]
- Gil Park, J.; Kang, M.K.; Lee, Y.R.; Song, J.E.; Kim, N.Y.; Kweon, Y.O.; Tak, W.Y.; Jang, S.Y.; Lee, C.; Kim, B.S.; et al. Fibrosis-4 index as a predictor for mortality in hospitalised patients with COVID-19: A retrospective multicentre cohort study. BMJ Open 2020, 10, e041989. [Google Scholar] [CrossRef]
- Li, Y.; Regan, J.; Fajnzylber, J.; Coxen, K.; Corry, H.; Wong, C.; Rosenthal, A.; Atyeo, C.; Fischinger, S.; Gillespie, E.; et al. Liver Fibrosis Index FIB-4 Is Associated with Mortality in COVID-19. Hepatol. Commun. 2020, 5, 2021. [Google Scholar] [CrossRef] [PubMed]
- Pranata, R.; Yonas, E.; Huang, I.; Lim, M.A.; Nasution, S.A.; Kuswardhani, R.A.T. Fibrosis-4 index and mortality in coronavirus disease 2019. Eur. J. Gastroenterol. Hepatol. 2021. [Google Scholar] [CrossRef]
- Sutandyo, N.; Kurniawati, S.A.; Jayusman, A.M.; Syafiyah, A.H.; Pranata, R.; Hanafi, A.R. Repurposing FIB-4 index as a predictor of mortality in patients with hematological malignancies and COVID-19. PLoS ONE 2021, 16, e0257775. [Google Scholar] [CrossRef]
- Younossi, Z.M.; Koenig, A.B.; Abdelatif, D.; Fazel, Y.; Henry, L.; Wymer, M. Global epidemiology of nonalcoholic fatty liver disease-Meta-analytic assessment of prevalence, incidence, and outcomes. Hepatology 2016, 64, 73–84. [Google Scholar] [CrossRef] [Green Version]
- Zheng, K.; Gao, F.; Wang, X.-B.; Sun, Q.-F.; Pan, K.-H.; Wang, T.-Y.; Ma, H.-L.; Chen, Y.-P.; Liu, W.-Y.; George, J.; et al. Letter to the Editor: Obesity as a risk factor for greater severity of COVID-19 in patients with metabolic associated fatty liver disease. Metabolism 2020, 108, 154244. [Google Scholar] [CrossRef]
- Zhou, Y.; Zheng, K.I.; Wang, X.; Sun, Q.; Pan, K.; Wang, T.; Ma, H.; Chen, Y.; George, J.; Zheng, M. Metabolic-associated fatty liver disease is associated with severity of COVID-19. Liver Int. 2020, 40, 2160–2163. [Google Scholar] [CrossRef]
- Ji, D.; Qin, E.; Xu, J.; Zhang, D.; Cheng, G.; Wang, Y.; Lau, G. Non-alcoholic fatty liver diseases in patients with COVID-19: A retrospective study. J. Hepatol. 2020, 73, 451–453. [Google Scholar] [CrossRef]
- Narayanan, S.; Surette, F.A.; Hahn, Y.S. The Immune Landscape in Nonalcoholic Steatohepatitis. Immune Netw. 2016, 16, 147–158. [Google Scholar] [CrossRef] [Green Version]
- Sharma, P.; Kumar, A. Metabolic dysfunction associated fatty liver disease increases risk of severe COVID-19. Diabetes Metab. Syndr. Clin. Res. Rev. 2020, 14, 825–827. [Google Scholar] [CrossRef]
- Targher, G.; Mantovani, A.; Byrne, C.D.; Wang, X.-B.; Yan, H.-D.; Sun, Q.-F.; Pan, K.-H.; Zheng, K.I.; Chen, Y.-P.; Eslam, M.; et al. Risk of severe illness from COVID-19 in patients with metabolic dysfunction-associated fatty liver disease and increased fibrosis scores. Gut 2020, 69, 1545–1547. [Google Scholar] [CrossRef]
- Foschi, F.G.; Domenicali, M.; Giacomoni, P.; Dall’Aglio, A.C.; Conti, F.; Borghi, A.; Bevilacqua, V.; Napoli, L.; Mirici, F.; Cucchetti, A.; et al. Is there an association between commonly employed biomarkers of liver fibrosis and liver stiffness in the general population? Ann. Hepatol. 2020, 19, 380–387. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Non-Invasive Score | As Originally Described in: | Formula | Cut-Off Values for High Risk of Advanced Fibrosis |
|---|---|---|---|
| FIB-4 | Sterling R. et al. [9] | Age (years) × AST (IU/L)/platelet count (×109/L) × √ALT (IU/L) | 3.25 if age < 65 2.0 if age ≥ 65 |
| AST/ALT ratio | Giannini E. et al. [17] | AST/ALT | 0.8 |
| Forns score | Wai C. et al. [15] | 7.811 − 3.131 × ln (platelet count) + 0.781 × ln (GGT) + 3.467 × ln (age) − 0.014 × (total cholesterol) | 6.9 |
| APRI score | Lin Z. et al. [16] | AST/upper limit of normal)/platelet count (expressed as platelets × 109/L) × 100 | 1 |
| Variable | Median (Confidence Interval)/No (%) |
|---|---|
| Age (years) | 65.5 (58.11–69.3) |
| Gender (M, %) | 220 (59.45%) |
| Biological parameters | |
| Hemoglobin (g/dL) | 13.05 (11.54–13.96) |
| White blood cells (×109/L) | 7.05 (6.96–9.43) |
| Lymphocytes (×109/L) | 1.09 (0.93–1.36) |
| Neutrophils (×109/L) | 5.42 (5.52–7.57) |
| Platelets (×109/L) | 207.5 (193.04–266.21) |
| Random blood glucose (on admission, mg/dL) | 126 (119.94–172.64) |
| C–reactive protein (mg/L) | 139.5 (104.68–169.61) |
| Procalcitonin (ng/mL) | 0.14 (−0.22–1.47) |
| Fibrinogen (mg/dL) | 715.65 (682.69–941.94) |
| D-dimers (mg/dL) | 529.45 (489.79–1333.77) |
| Ferritin (mg/dL) | 824.1 (763.21–1808.79) |
| Lactate dehydrogenase (U/L) | 697.5 (515.86–840.3) |
| Total cholesterol (mg/dL) | 155.5 (142.65–177.42) |
| Triglycerides (mg/dL) | 144 (130.79–198.37) |
| HDL-cholesterol (mg/dL) | 32.5 (31.1–41.4) |
| Creatinine (mg/dL) | 1.02 (0.76–2.33) |
| Urea (mg/dL) | 43 (39.04–64.99) |
| Na (mmol/L) | 139 (136.36–139.73) |
| K (mmol/L) | 4.31 (4.23–4.69) |
| Creatinine clearance (MDRD) (mL/min/1.73 m2) | 64.47 (52.26–78.74) |
| INR | 1.07 (1–1.59) |
| Prothrombin Time (s) | 17.85 (16.05–24.7) |
| Liver tests | |
| AST (U/L) | 47.5 (47.26–93.33) |
| ALT (U/L) | 38 (33.24–77.17) |
| AST and ALT elevations (N, %) | 289 (72.94%) |
| ALP (U/L) | 67.5 (63.17–92.24) |
| GGT (U/L) | 91 (71.18–134.9) |
| ALP and GGT elevations (N, %) | 165 (50.92%) |
| Bilirubin (mg/dL) | 0.45 (0.41–0.66) |
| Fibrosis scores | |
| AST/ALT value | 1.51 (1.26–1.84) |
| Severe AST/ALT | 163 (44.1%) |
| APRI value | 0.42 (0.4–1.13) |
| Severe APRI | 88 (23.8%) |
| FIB-4 value | 2.6 (2.1–4.71) |
| Severe FIB-4 | 109 (29.5%) |
| Age adjusted severe FIB-4 | 156 (42.2%) |
| Forns value | 6.61 (5.78–7.11) |
| Severe Forns | 199 (53.8%) |
| Disease severity and personal history | |
| TSS start | 11.5 (10.44–13.31) |
| TSS maxim | 11.5 (10.58–13.75) |
| Severe COVID * | 191 (51.6%) |
| Liver steatosis on CT | 146 (39.5%) |
| Arterial hypertension | 217 (58.6%) |
| Ischemic heart disease | 62 (16.8%) |
| Atrial fibrillation | 38 (10.3%) |
| Heart failure | 42 (11.4%) |
| Chronic obstructive pulmonary disease | 34 (9.2%) |
| Stroke | 25 (6.8%) |
| Chronic kidney disease | 44 (11.9%) |
| Type 2 diabetes mellitus | 90 (24.3%) |
| Neoplasia | 27 (7.3%) |
| Variable | Survivors (n = 327, 88.4%) | Non-Survivors (n = 43, 11.6%) | p |
|---|---|---|---|
| Age (years) | 62 (55.4–67.5) | 73 (60.53–89.47) | <0.001 |
| Gender (M, %) | 190 (86.36%) | 30 (69.76%) | 0.096 |
| Biological parameters | |||
| Hemoglobin (g/dL) | 13.05 (11.24–14.04) | 13 (9.5–17.09) | 0.006 |
| White blood cells (×109/L) | 7.45 (6.96–9.74) | 6.22 (2.59–12.35) | 0.23 |
| Lymphocytes (×109/L) | 1.09 (0.94–1.40) | 0.85 (0.00–2.05) | <0.001 |
| Neutrophils (×109/L) | 5.57 (5.47–7.79) | 5.42 (2.19–10) | 0.017 |
| Platelets (×109/L) | 231 (206–285) | 153.5 (72.98–227.52) | 0.035 |
| Random blood sugar (on admission, mg/dL) | 125 (116.01–178.69) | 128 (81.31–200.69) | 0.026 |
| C reactive protein (mg/L) | 132.29 (92.6–169.65) | 169.5 (118.35–216.14) | <0.001 |
| Procalcitonin (ng/mL) | 0.13 (0.01–1.68) | 0.25 (0.01–1.3) | 0.001 |
| Fibrinogen (mg/dL) | 746.2 (677.67–989.72) | 710.15 (677.65–733.19) | 0.015 |
| D-dimers (mg/dL) | 529.45 (461.6–934.43) | 1871.15 (−1285.41–5246.66) | 0.04 |
| LDH (U/L) | 627 (481.46–874.93) | 698.5 (500.33–854.66) | <0.001 |
| Ferritin (mg/dL) | 742.75 (696.38–1956.5) | 1073.5 (358.78–1808.81) | 0.008 |
| Cholesterol (mg/dL) | 159.5 (142.76–184.04) | 140.5 (119.17–167.32) | 0.001 |
| TG (mg/dL) | 144 (128.5–208.69) | 140.5 (74–215) | 0.557 |
| HDL (mg/dL) | 31.5 (29.23–40.87) | 38.5 (26.06–58.44) | 0.881 |
| LDL (mg/dL) | 100 (83.74–121.96) | 71 (58.54–85.96) | 0.014 |
| Creatinine (mg/dL) | 0.96 (0.53–2.36) | 1.75 (0.07–4.23) | <0.001 |
| Urea (mg/dL) | 38.5 (34.76–51.98) | 90.5 (22.21–168.28) | <0.001 |
| Na (mmol/L) | 139 (135.93–139.77) | 138.5 (133.05–144.95) | 0.115 |
| K (mmol/L) | 4.41 (4.25–4.72) | 3.95 (3.01–5.67) | 0.008 |
| Creatinine clearance (MDRD) (mL/min/1.73 m2) | 67.62 (55.16–83.85) | 40.39 (3.38–94.37) | <0.001 |
| INR | 1.07 (0.96–1.68) | 1.14 (0.92–1.37) | 0.004 |
| Prothrombin Time (s) | 17.85 (15.18–25.58) | 18.75 (12.73–27.96) | 0.008 |
| Liver tests | |||
| AST (U/L) | 51.02 (46.97–55.07) | 64.55 (49.76–79.35) | 0.04 |
| ALT (U/L) | 50.45 (45.05–55.86) | 38.95 (27.58–50.31) | 0.13 |
| ALP (U/L) | 71.5 (65.64–87.76) | 52.5 (−35.33–200.83) | 0.212 |
| GGT (U/L) | 91 (70.62–141.78) | 78 (−42.55–217.05) | 0.201 |
| Bilirubin (mg/dL) | 0.44 (0.38–0.67) | 0.63 (0.18–1.02) | 0.082 |
| Peak AST (U/L) | 69.89 (63.56–76.21) | 186.24 (71.84–300.64) | <0.001 |
| Peak ALT (U/L) | 118.85 (103.86–133.85) | 153.13 (87.82–218.44) | 0.91 |
| Fibrosis scores | |||
| AST/ALT | 1.21 (1.12–1.30) | 1.97 (1.41–2.53) | <0.001 |
| Severe fibrosis depending on AST/ALT (n, %) | 255 (78.7%) | 36 (94.7%) | 0.02 |
| APRI | 0.61 (0.51–0.71) | 0.90 (0.51–1.29) | 0.01 |
| Severe fibrosis depending on APRI (n, %) | 34 (10.5%) | 7 (18.4%) | 0.14 |
| FIB-4 | 2.60 (2.29–2.90) | 5.38 (3.32–7.44) | <0.001 |
| Severe fibrosis depending on FIB-4 (n, %) | 162 (50.2%) | 30 (78.9%) | 0.001 |
| Forns | 7.86 (7.57–8.15) | 9.29 (8.60–9.98) | <0.001 |
| Severe fibrosis depending on Forns (n, %) | 130 (66.7%) | 30 (96.8%) | <0.001 |
| Disease severity and personal history | |||
| Liver steatosis on CT | 126 (38.53%) | 20 (46.51%) | 0.314 |
| TSS start | 11 (10.15–13.35) | 12.5 (6.62–18.38) | 0.004 |
| TSS maxim | 11 (10.28–13.72) | 12.5 (5.77–20.23) | <0.001 |
| Arterial hypertension | 183 (56.5%) | 28 (73.7%) | 0.04 |
| Ischemic heart disease | 45 (13.9%) | 12 (31.6%) | 0.005 |
| Atrial fibrillation | 30 (9.3%) | 6 (15.8%) | 0.20 |
| Chronic heart failure | 31 (9.6%) | 10 (26.3%) | 0.002 |
| Chronic obstructive pulmonary disease | 23 (7.1%) | 10 (26.3%) | <0.001 |
| Stroke | 22 (6.8%) | 3 (7.9%) | 0.79 |
| Chronic kidney disease | 30 (9.3%) | 12 (31.6%) | <0.001 |
| Type 2 diabetes mellitus | 75 (23.1%) | 13 (34.2%) | 0.13 |
| Neoplasia | 21 (6.5%) | 5 (13.2%) | 0.13 |
| Fibrosis Scores | Associations | p |
|---|---|---|
| Severe FIB-4 | Steatosis | 0.721 |
| ALT > 50 | 0.196 | |
| AST > 50 | <0.001 | |
| Severe FIB-4 > 65 | Steatosis | 0.012 |
| ALT > 50 | <0.001 | |
| AST > 50 | 0.008 | |
| Severe Forns | Steatosis | 0.001 |
| ALT > 50 | 0.001 | |
| AST > 50 | 0.001 | |
| Severe APRI | Steatosis | 0.031 |
| AST/ALT | Steatosis | 0.029 |
| Fibrosis Scores | OR | Std Error | p |
|---|---|---|---|
| FIB-4 | 1.353 | 0.151 | 0.046 |
| AST > 50 | 1.02 | 0.009 | 0.037 |
| AST/ALT | 1.46 | 0.262 | 0.144 |
| APRI | 0.21 | 0.985 | 0.119 |
| Forns | 1.131 | 0.144 | 0.391 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Crisan, D.; Avram, L.; Grapa, C.; Dragan, A.; Radulescu, D.; Crisan, S.; Grosu, A.; Militaru, V.; Buzdugan, E.; Stoicescu, L.; et al. Liver Injury and Elevated FIB-4 Define a High-Risk Group in Patients with COVID-19. J. Clin. Med. 2022, 11, 153. https://doi.org/10.3390/jcm11010153
Crisan D, Avram L, Grapa C, Dragan A, Radulescu D, Crisan S, Grosu A, Militaru V, Buzdugan E, Stoicescu L, et al. Liver Injury and Elevated FIB-4 Define a High-Risk Group in Patients with COVID-19. Journal of Clinical Medicine. 2022; 11(1):153. https://doi.org/10.3390/jcm11010153
Chicago/Turabian StyleCrisan, Dana, Lucretia Avram, Cristiana Grapa, Alexandra Dragan, Dan Radulescu, Sorin Crisan, Alin Grosu, Valentin Militaru, Elena Buzdugan, Laurentiu Stoicescu, and et al. 2022. "Liver Injury and Elevated FIB-4 Define a High-Risk Group in Patients with COVID-19" Journal of Clinical Medicine 11, no. 1: 153. https://doi.org/10.3390/jcm11010153