
Salivary Ferritin Changes in Patients with COVID-19

 , and
, and
Abstract
:1. Introduction
2. Material and Methods
2.1. Participant and Samples
2.2. Ferritin Measurement in Saliva
2.3. Effect of Different SARS-CoV2 Inactivation Protocols in Salivary Ferritin Concentrations
2.4. Salivary Ferritin Concentrations in COVID-19 Patients
- –
- Healthy group (HG), which included individuals who did not have any clinical sign of disease for at least 4 weeks before sampling and were negative to SARS-CoV-2 infection by RT-PCR (n = 30, 16 men and 14 women, aged between 23 and 75 years old).
- –
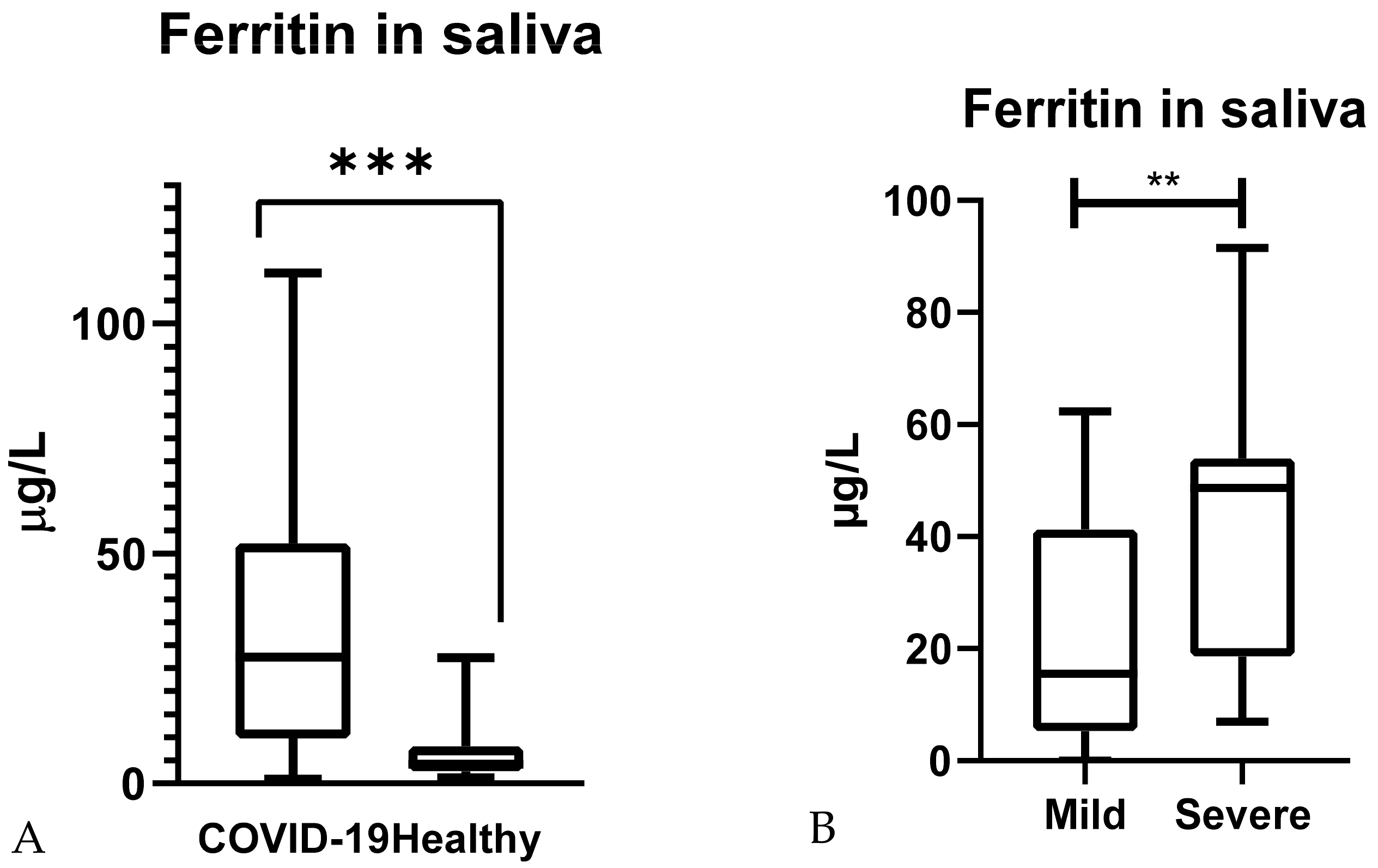
- Diseased group (DG), which included individuals with clinical signs of two levels of severity and a confirmed COVID-19 diagnosis (n = 65, 34 men and 31 women, aged between 24 and 91 years old). Patients were divided according to disease severity into mild (n = 47, no need for oxygen supplementation or conventional oxygen therapy) and severe (n = 18, requiring nasal flow oxygen or assisted respiration) [29]. In all cases, samples were taken on the day of hospital admission.
2.5. Comparison with Serum Ferritin
2.6. Protein Measurement in Saliva
2.7. Statistical Analysis
3. Results
3.1. Effect of Different SARS-CoV2 Inactivation Protocols in Salivary Ferritin Concentrations
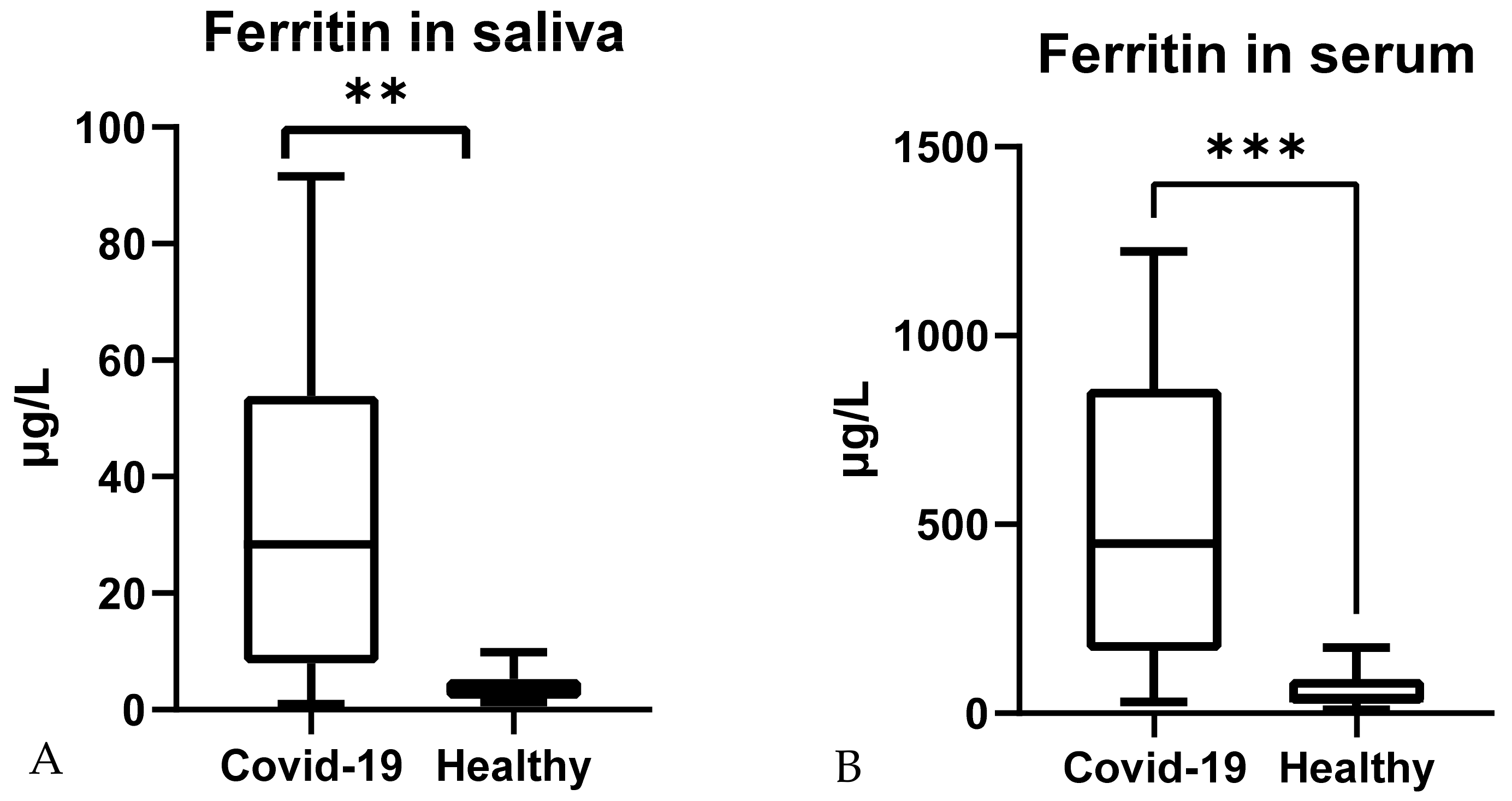
3.2. Salivary Ferritin Concentrations in COVID-19 Patients
3.3. Comparison with Serum Ferritin
3.4. Correction by Protein Content
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Huang, C.; Wang, Y.; Li, X.; Ren, L.; Zhao, J.; Hu, Y.; Zhang, L.; Fan, G.; Xu, J.; Gu, X.; et al. Clinical Features of Patients Infected with 2019 Novel Coronavirus in Wuhan, China. Lancet 2020, 395, 497–506. [Google Scholar] [CrossRef] [Green Version]
- Dahan, S.; Segal, G.; Katz, I.; Hellou, T.; Tietel, M.; Bryk, G.; Amital, H.; Shoenfeld, Y.; Dagan, A. Ferritin as a Marker of Severity in COVID-19 Patients: A Fatal Correlation. Isr. Med. Assoc. J. 2020, 22, 494–500. [Google Scholar] [PubMed]
- Kadkhoda, K. COVID-19: An Immunopathological View. mSphere 2020, 5, e00344-20. [Google Scholar] [CrossRef] [Green Version]
- Chen, G.; Wu, D.; Guo, W.; Cao, Y.; Huang, D.; Wang, H.; Wang, T.; Zhang, X.; Chen, H.; Yu, H.; et al. Clinical and immunological features of severe and moderate coronavirus disease 2019. J. Clin. Investig. 2020, 130, 2620–2629. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Qin, C.; Zhou, L.; Hu, Z.; Zhang, S.; Yang, S.; Tao, Y.; Xie, C.; Ma, K.; Shang, K.; Wang, W.; et al. Dysregulation of Immune Response in Patients with Coronavirus 2019 (COVID-19) in Wuhan, China. Clin. Infect. Dis. 2020, 71, 762–768. [Google Scholar] [CrossRef] [PubMed]
- Gómez-Pastora, J.; Weigand, M.; Kim, J.; Wu, X.; Strayer, J.; Palmer, A.F.; Zborowski, M.; Yazer, M.; Chalmers, J.J. Hyperferritinemia in critically ill COVID-19 patients—Is ferritin the product of inflammation or a pathogenic mediator? Clin. Chim. Acta 2020, 509, 249–251. [Google Scholar] [CrossRef] [PubMed]
- Zuyderhoudt, F.M.J. Ferritin in Serum. Ned. Tijdschr. Geneeskd. 1982, 126, 1733–1737. [Google Scholar]
- Sharif, K.; Vieira Borba, V.; Zandman-Goddard, G.; Shoenfeld, Y. Eppur Si Muove: Ferritin is Essential in Modulating Inflammation. Clin. Exp. Immunol. 2018, 191, 149–150. [Google Scholar] [CrossRef] [Green Version]
- Agmon-Levin, N.; Rosário, C.; Katz, B.S.P.; Zandman-Goddard, G.; Meroni, P.; Cervera, R.; Stojanovich, L.; Blank, M.; Pierangeli, S.S.; Praprotnik, S.; et al. Ferritin in the Antiphospholipid Syndrome and Its Catastrophic Variant (cAPS). Lupus 2013, 22, 1327–1335. [Google Scholar] [CrossRef] [PubMed]
- Wang, W.; Knovich, M.A.; Coffman, L.G.; Torti, F.M.; Torti, S.V. Serum Ferritin: Past, Present and Future. Biochim. Biophys. Acta-Gen. Subj. 2010, 1800, 760–769. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rosário, C.; Zandman-Goddard, G.; Meyron-Holtz, E.G.; D’Cruz, D.P.; Shoenfeld, Y. The Hyperferritinemic Syndrome: Macrophage Activation Syndrome, Still’s Disease, Septic Shock and Catastrophic Antiphospholipid Syndrome. BMC Med. 2013, 11, 185. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shafer, W. (Ed.) Antimicrobial Peptides and Human Disease; Springer: Berlin/Heidelberg, Germany, 2006; ISBN 978-3540299158. [Google Scholar]
- Zandman-Goddard, G.; Shoenfeld, Y. Ferritin in Autoimmune Diseases. Autoimmun. Rev. 2007, 6, 457–463. [Google Scholar] [CrossRef]
- Orbach, H.; Zandman-Goddard, G.; Amital, H.; Barak, V.; Szekanecz, Z.; Szucs, G.; Danko, K.; Nagy, E.; Csepany, T.; Carvalho, J.F.; et al. Novel Biomarkers in Autoimmune Diseases: Prolactin, Ferritin, Vitamin D, and TPA Levels in Autoimmune Diseases. Ann. N. Y. Acad. Sci. 2007, 1109, 385–400. [Google Scholar] [CrossRef] [PubMed]
- Manesh, M.S.; Kheiri, S.; Abasi, F.; Momeni, A. Serum Ferritin Has Correlation with HbA1c in type 2 Diabetic Patients. Adv. Biomed. Res. 2015, 4, 74. [Google Scholar] [CrossRef]
- Son, N.E. Influence of Ferritin Levels and Inflammatory Markers on HbA1c in the Type 2 Diabetes Mellitus Patients. Pak. J. Med. Sci. 2019, 35, 1030–1035. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vargas-Vargas, M.; Cortés-Rojo, C. Ferritin Levels and COVID-19. Rev. Panam. Salud Publica/Pan Am. J. Public Health 2020, 44, e72. [Google Scholar] [CrossRef] [PubMed]
- Trottestam, H.; Horne, A.C.; Aricò, M.; Egeler, R.M.; Filipovich, A.H.; Gadner, H.; Imashuku, S.; Ladisch, S.; Webb, D.; Janka, G.; et al. Chemoimmunotherapy for Hemophagocytic Lymphohistiocytosis: Long-Term Results of the HLH-94 Treatment Protocol. Blood 2011, 118, 4577–4584. [Google Scholar] [CrossRef] [PubMed]
- Velavan, T.P.; Meyer, C.G. Mild Versus Severe COVID-19: Laboratory Markers. Int. J. Infect. Dis. 2020, 95, 304–307. [Google Scholar] [CrossRef]
- Giamarellos-Bourboulis, E.J.; Netea, M.G.; Rovina, N.; Akinosoglou, K.; Antoniadou, A.; Antonakos, N.; Damoraki, G.; Gkavogianni, T.; Adami, M.E.; Katsaounou, P.; et al. Complex Immune Dysregulation in COVID-19 Patients with Severe Respiratory Failure. Cell Host Microbe 2020, 27, 992–1000.e3. [Google Scholar] [CrossRef] [PubMed]
- Mehta, P.; McAuley, D.F.; Brown, M.; Sanchez, E.; Tattersall, R.S.; Manson, J.J. COVID-19: Consider cytokine storm syndromes and immunosuppression. Lancet 2020, 395, 1033–1034. [Google Scholar] [CrossRef]
- Tvarijonaviciute, A.; Martínez-Subiela, S.; López-Jornet, P.; Lamy, E. The Future of Saliva as an Analytical Sample. In Saliva in Health and Disease; Springer International Publishing: Berlin/Heidelberg, Germany, 2020; pp. 321–326. [Google Scholar]
- Ceron, J.; Lamy, E.; Martinez-Subiela, S.; Lopez-Jornet, P.; Capela-Silva, F.; Eckersall, P.; Tvarijonaviciute, A. Use of Saliva for Diagnosis and Monitoring the SARS-CoV-2: A General Perspective. J. Clin. Med. 2020, 9, 1491. [Google Scholar] [CrossRef] [PubMed]
- Franco-Martínez, L.; Tecles, F.; Torres-Cantero, A.; Bernal, E.; San Lázaro, I.; Alcaraz, M.J.; Vicente-Romero, M.R.; Lamy, E.; Sánchez-Resalt, C.; Rubio, C.P.; et al. Analytical validation of an automated assay for the measurement of adenosine deaminase (ADA) and its isoenzymes in saliva and a pilot evaluation of their changes in patients with SARS-CoV-2 infection. Clin. Chem. Lab. Med. 2021, 59, 1592–1599. [Google Scholar] [CrossRef]
- Dolores Contreras-Aguilar, M.; Escribano, D.; Martínez-subiela, S.; Martínez-Miró, S.; Rubio, M.; Tvarijonaviciute, A.; Tecles, F.; Ceró, J.J.; Contreras-Aguilar, M.D.; Escribano, D.; et al. Influence of the Way of Reporting Alpha-Amylase Values in Saliva in Different Naturalistic Situations: A pilot study. PLoS ONE 2017, 12, e0180100. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Franco-Martínez, L.; Tvarijonaviciute, A.; Martínez-Subiela, S.; Márquez, G.; Martínez Díaz, N.; Cugat, R.; Cerón, J.J.; Jiménez-Reyes, P. Changes in lactate, ferritin, and uric acid in saliva after repeated explosive effort sequences. J. Sports Med. Phys. Fit. 2019, 59, 902–909. [Google Scholar] [CrossRef] [PubMed]
- Patterson, E.I.; Prince, T.; Anderson, E.R.; Casas-Sanchez, A.; Smith, S.L.; Cansado-Utrilla, C.; Turtle, L.; Hughes, G.L. Methods of inactivation of SARS-CoV-2 for downstream biological assays. bioRxiv 2020. [Google Scholar] [CrossRef]
- Pastorino, B.; Touret, F.; Gilles, M.; de Lamballerie, X.; Charrel, R.N. Evaluation of heating and chemical protocols for inactivating SARS-CoV-2. bioRxiv 2020. [Google Scholar] [CrossRef]
- Ahmed, S.; Ansar Ahmed, Z.; Siddiqui, I.; Haroon Rashid, N.; Mansoor, M.; Jafri, L. Evaluation of serum ferritin for prediction of severity and mortality in COVID-19—A cross sectional study. Ann. Med. Surg. 2021, 63, 102163. [Google Scholar] [CrossRef]
- Dewhurst, E.C.; Crawford, E.; Cue, S.; Dodkin, S.; German, A.J.; Papasouliotis, K. Analysis of canine and feline haemograms using the VetScan HMT analyser. J. Small Anim. Pract. 2003, 44, 443–448. [Google Scholar] [CrossRef] [PubMed]
- Rosner, B. Fundamentals of Biostatistics; Brooks: Boston, MA, USA, 2011. [Google Scholar]
- Banchini, F.; Cattaneo, G.M.; Capelli, P. Serum ferritin levels in inflammation: A retrospective comparative analysis between COVID-19 and emergency surgical non-COVID-19 patients. World J. Emerg. Surg. 2021, 16, 9. [Google Scholar] [CrossRef] [PubMed]
- Mishra, O.P.; Agarwal, K.N.; Agarwal, R.M.D. Salivary Iron Status in Children with Iron Deficiency and Iron Overload. J. Trop. Pediatr. 1992, 38, 64–67. [Google Scholar] [CrossRef]
- Haji-Sattari, F.; Zarabadipour, M.; Hajmanoochehri, F.; Mirzadeh, M. Salivary and Serum Ferritin Levels: Is There a Correlation? J. Islam. Dent. Assoc. IRAN 2019, 31, 214–217. [Google Scholar] [CrossRef]
- Guo, L.N.; Yang, Y.Z.; Feng, Y.Z. Serum and salivary ferritin and Hepcidin levels in patients with chronic periodontitis and type 2 diabetes mellitus. BMC Oral Health 2018, 18, 63. [Google Scholar] [CrossRef] [PubMed]
- Taneri, P.E.; Gómez-Ochoa, S.A.; Llanaj, E.; Raguindin, P.F.; Rojas, L.Z.; Roa-Díaz, Z.M.; Salvador, D.; Groothof, D.; Minder, B.; Kopp-Heim, D.; et al. Anemia and Iron Metabolism in COVID-19: A Systematic Review and Meta-Analysis. Eur. J. Epidemiol. 2020, 35, 763–773. [Google Scholar] [CrossRef] [PubMed]
- Feld, J.; Tremblay, D.; Thibaud, S.; Kessler, A.; Naymagon, L. Ferritin Levels in Patients with COVID-19: A Poor Predictor of Mortality and Hemophagocytic Lymphohistiocytosis. Int. J. Lab. Hematol. 2020, 42, 773–779. [Google Scholar] [CrossRef] [PubMed]
- Henry, B.M.; De Oliveira, M.H.S.; Benoit, S.; Plebani, M.; Lippi, G. Hematologic, Biochemical and Immune Biomarker Abnormalities Associated with Severe Illness and Mortality in Coronavirus Disease 2019 (COVID-19): A Meta-Analysis. Clin. Chem. Lab. Med. 2020, 58, 1021–1028. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Martinez-Cuazitl, A.; Vazquez-Zapien, G.J.; Sanchez-Brito, M.; Limon-Pacheco, J.H.; Guerrero-Ruiz, M.; Garibay-Gonzalez, F.; Delgado-Macuil, R.J.; de Jesus, M.G.G.; Corona-Perezgrovas, M.A.; Pereyra-Talamantes, A.; et al. ATR-FTIR spectrum analysis of saliva samples from COVID-19 positive patients. Sci. Rep. 2021, 11, 19980. [Google Scholar] [CrossRef]
- Hanff, T.C.; Mohareb, A.M.; Giri, J.; Cohen, J.B.; Chirinos, J.A. Thrombosis in COVID-19. Am. J. Hematol. 2020, 95, 1578–1589. [Google Scholar] [CrossRef] [PubMed]
- Colafrancesco, S.; Alessandri, C.; Conti, F.; Priori, R. COVID-19 gone bad: A new character in the spectrum of the hyperferritinemic syndrome? Autoimmun. Rev. 2020, 19, 102573. [Google Scholar] [CrossRef] [PubMed]
- MacKinnon, L.T.; Jenkins, D.G. Decreased salivary immunoglobulins after intense interval exercise before and after training. Med. Sci. Sports Exerc. 1993, 25, 678–683. [Google Scholar] [CrossRef]
- Traeger Mackinnon, L.; Ginn, E.; Seymour, G.J. Decreased Salivary Immunoglobulin A Secretion Rate after Intense Interval Exercise in Elite Kayakers. Eur. J. Appl. Physiol. Occup. Physiol. 1993, 67, 180–184. [Google Scholar] [CrossRef]
- Walsh, N.P. The effects of high-intensity intermittent exercise on saliva IgA, total protein and alpha-amylase. J. Sports Sci. 1999, 17, 129–134. [Google Scholar] [CrossRef]
- Ceron, J.J.; Pardo-Marin, L.; Caldin, M.; Furlanello, T.; Solano-Gallego, L.; Tecles, F.; Bernal, L.; Baneth, G.; Martinez-Subiela, S. Use of Acute Phase Proteins for the Clinical Assessment and Management of Canine Leishmaniosis: General Recommendations. BMC Vet. Res. 2018, 14, 196. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| NT | H65 | H92 | SDS | NP | TX100 | |
|---|---|---|---|---|---|---|
| Ferritin (%) | 100 | 101 (98.4–114) | 91.9 (90–105) | 111 (111–121) * | 107 (106–115) | 115 (107–117) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Franco-Martínez, L.; Cerón, J.J.; Vicente-Romero, M.R.; Bernal, E.; Torres Cantero, A.; Tecles, F.; Sánchez Resalt, C.; Martínez, M.; Tvarijonaviciute, A.; Martínez-Subiela, S. Salivary Ferritin Changes in Patients with COVID-19. Int. J. Environ. Res. Public Health 2022, 19, 41. https://doi.org/10.3390/ijerph19010041
Franco-Martínez L, Cerón JJ, Vicente-Romero MR, Bernal E, Torres Cantero A, Tecles F, Sánchez Resalt C, Martínez M, Tvarijonaviciute A, Martínez-Subiela S. Salivary Ferritin Changes in Patients with COVID-19. International Journal of Environmental Research and Public Health. 2022; 19(1):41. https://doi.org/10.3390/ijerph19010041
Chicago/Turabian StyleFranco-Martínez, Lorena, José J. Cerón, María R. Vicente-Romero, Enrique Bernal, Alberto Torres Cantero, Fernando Tecles, Cristina Sánchez Resalt, Mónica Martínez, Asta Tvarijonaviciute, and Silvia Martínez-Subiela. 2022. "Salivary Ferritin Changes in Patients with COVID-19" International Journal of Environmental Research and Public Health 19, no. 1: 41. https://doi.org/10.3390/ijerph19010041