
Circulating IgG Levels in SARS-CoV-2 Convalescent Individuals in Cyprus

 , , , , , ,
, , , , , ,  and
and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Data Collection
2.3. Specimen Collection, Storage, and Testing for Anti-SARS-CoV-2 IgG Antibodies
2.4. Statistical Analyses
3. Results
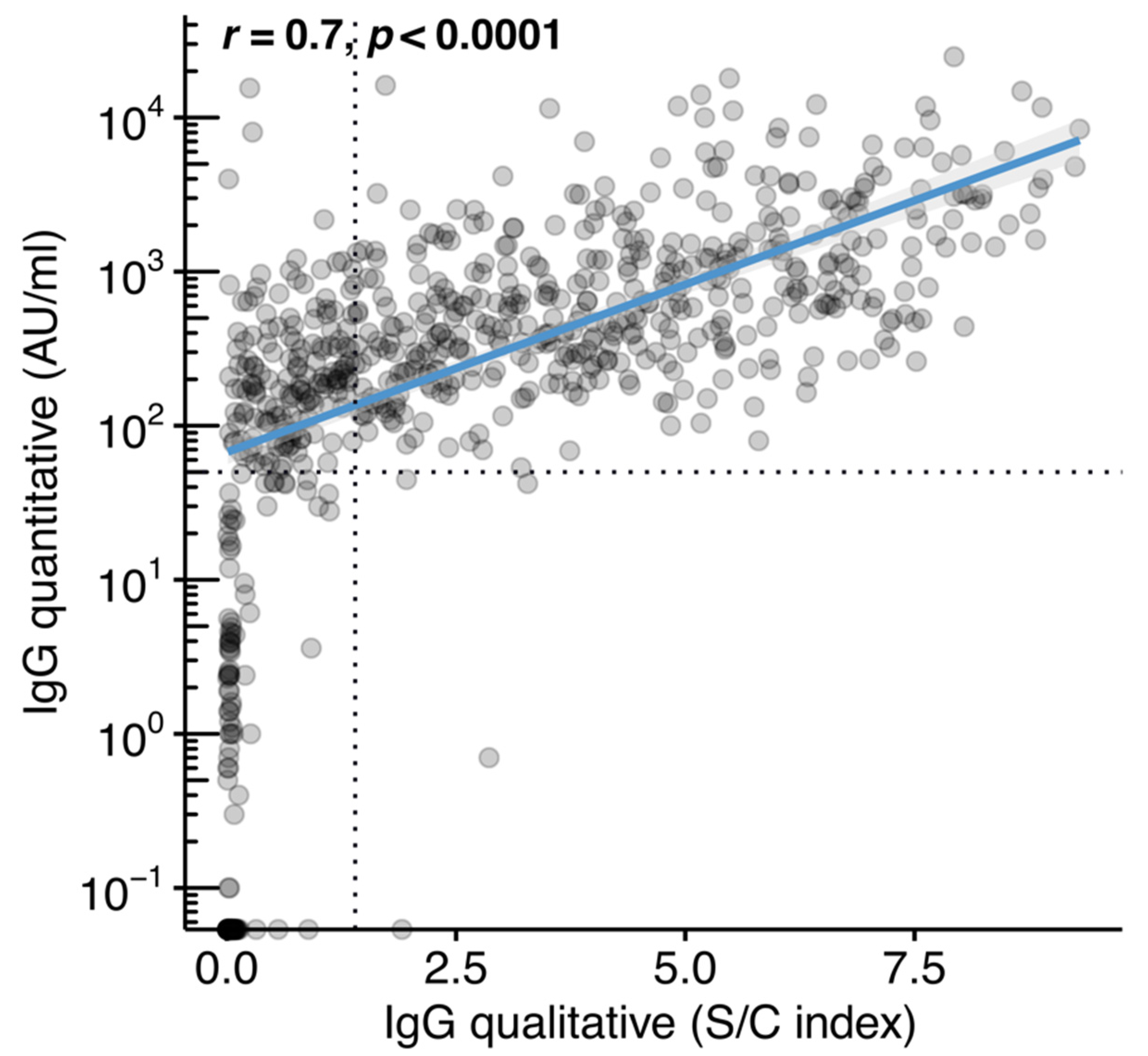
3.1. Assays Performance
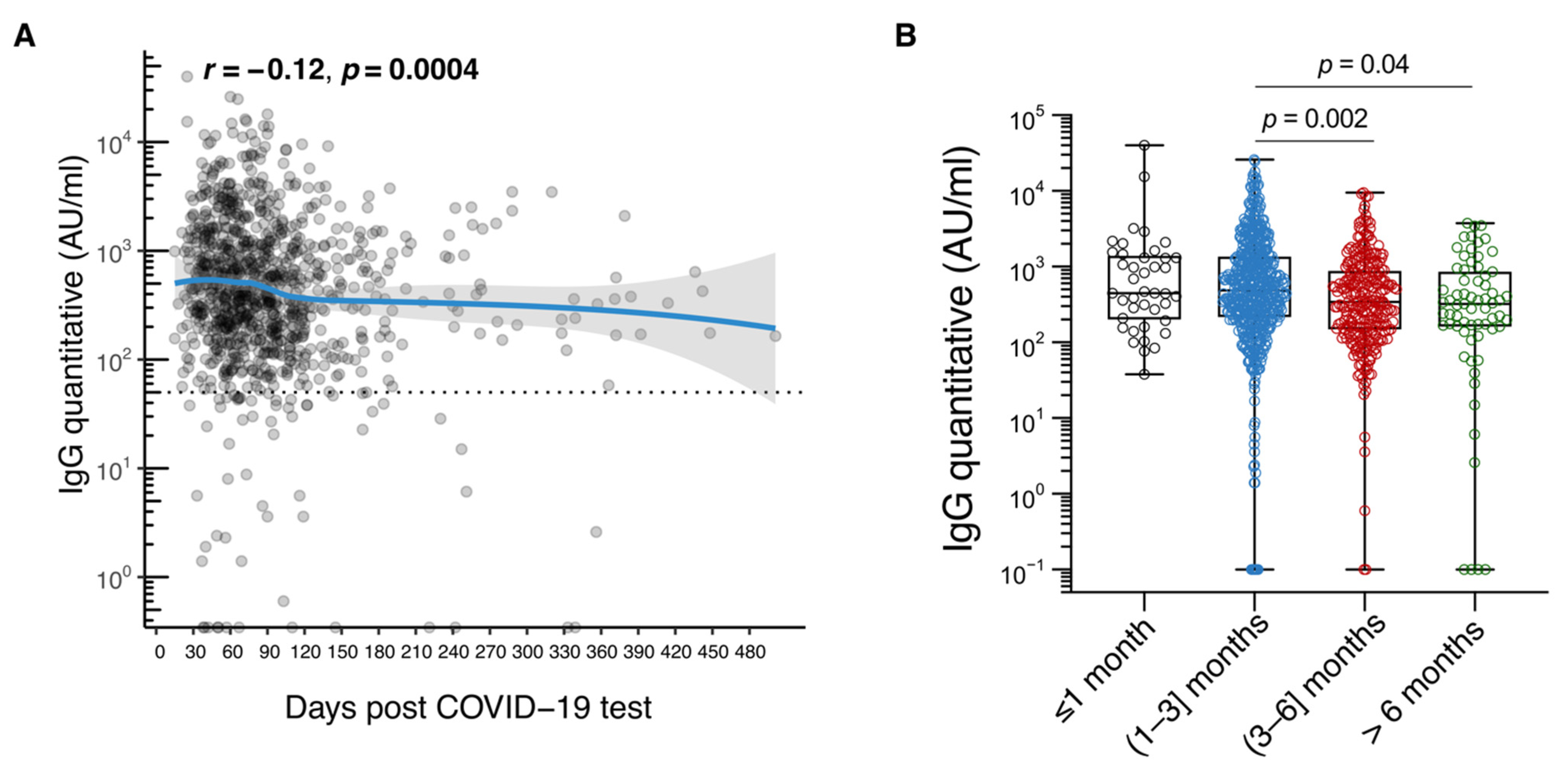
3.2. IgG Antibody Level Durability
3.3. Correlates of IgG Antibody Response
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Ke, Z.; Oton, J.; Qu, K.; Cortese, M.; Zila, V.; McKeane, L.; Nakane, T.; Zivanov, J.; Neufeldt, C.J.; Cerikan, B.; et al. Structures and distributions of SARS-CoV-2 spike proteins on intact virions. Nature 2020, 588, 498–502. [Google Scholar] [CrossRef]
- Turonova, B.; Sikora, M.; Schurmann, C.; Hagen, W.J.H.; Welsch, S.; Blanc, F.E.C.; von Bulow, S.; Gecht, M.; Bagola, K.; Horner, C.; et al. In situ structural analysis of SARS-CoV-2 spike reveals flexibility mediated by three hinges. Science 2020, 370, 203–208. [Google Scholar] [CrossRef]
- Nguyen, H.L.; Lan, P.D.; Thai, N.Q.; Nissley, D.A.; O’Brien, E.P.; Li, M.S. Does SARS-CoV-2 Bind to Human ACE2 More Strongly Than Does SARS-CoV? J. Phys. Chem. B 2020, 124, 7336–7347. [Google Scholar] [CrossRef] [PubMed]
- Chan, J.F.; Yip, C.C.; To, K.K.; Tang, T.H.; Wong, S.C.; Leung, K.H.; Fung, A.Y.; Ng, A.C.; Zou, Z.; Tsoi, H.W.; et al. Improved Molecular Diagnosis of COVID-19 by the Novel, Highly Sensitive and Specific COVID-19-RdRp/Hel Real-Time Reverse Transcription-PCR Assay Validated In Vitro and with Clinical Specimens. J. Clin. Microbiol. 2020, 58, e00310-20. [Google Scholar] [CrossRef] [Green Version]
- Wang, Z.; Muecksch, F.; Schaefer-Babajew, D.; Finkin, S.; Viant, C.; Gaebler, C.; Hoffmann, H.H.; Barnes, C.O.; Cipolla, M.; Ramos, V.; et al. Naturally enhanced neutralizing breadth against SARS-CoV-2 one year after infection. Nature 2021, 595, 426–431. [Google Scholar] [CrossRef] [PubMed]
- Van Honacker, E.; Van Vaerenbergh, K.; Boel, A.; De Beenhouwer, H.; Leroux-Roels, I.; Cattoir, L. Comparison of five SARS-CoV-2 rapid antigen detection tests in a hospital setting and performance of one antigen assay in routine practice: A useful tool to guide isolation precautions? J. Hosp. Infect. 2021, 114, 144–152. [Google Scholar] [CrossRef]
- Polack, F.P.; Thomas, S.J.; Kitchin, N.; Absalon, J.; Gurtman, A.; Lockhart, S.; Perez, J.L.; Perez Marc, G.; Moreira, E.D.; Zerbini, C.; et al. Safety and Efficacy of the BNT162b2 mRNA COVID-19 Vaccine. N. Engl. J. Med. 2020, 383, 2603–2615. [Google Scholar] [CrossRef] [PubMed]
- Heath, P.T.; Galiza, E.P.; Baxter, D.N.; Boffito, M.; Browne, D.; Burns, F.; Chadwick, D.R.; Clark, R.; Cosgrove, C.; Galloway, J.; et al. Safety and Efficacy of NVX-CoV2373 COVID-19 Vaccine. N. Engl. J. Med. 2021, 385, 1172–1183. [Google Scholar] [CrossRef] [PubMed]
- Hyams, C.; Marlow, R.; Maseko, Z.; King, J.; Ward, L.; Fox, K.; Heath, R.; Tuner, A.; Friedrich, Z.; Morrison, L.; et al. Effectiveness of BNT162b2 and ChAdOx1 nCoV-19 COVID-19 vaccination at preventing hospitalisations in people aged at least 80 years: A test-negative, case-control study. Lancet Infect. Dis. 2021, 21, 1539–1548. [Google Scholar] [CrossRef]
- El Sahly, H.M.; Baden, L.R.; Essink, B.; Doblecki-Lewis, S.; Martin, J.M.; Anderson, E.J.; Campbell, T.B.; Clark, J.; Jackson, L.A.; Fichtenbaum, C.J.; et al. Efficacy of the mRNA-1273 SARS-CoV-2 Vaccine at Completion of Blinded Phase. N. Engl. J. Med. 2021. [Google Scholar] [CrossRef]
- Thomas, S.J.; Moreira, E.D., Jr.; Kitchin, N.; Absalon, J.; Gurtman, A.; Lockhart, S.; Perez, J.L.; Perez Marc, G.; Polack, F.P.; Zerbini, C.; et al. Safety and Efficacy of the BNT162b2 mRNA COVID-19 Vaccine through 6 Months. N. Engl. J. Med. 2021. [Google Scholar] [CrossRef]
- Scourfield, D.O.; Reed, S.G.; Quastel, M.; Alderson, J.; Bart, V.M.T.; Teijeira Crespo, A.; Jones, R.; Pring, E.; Richter, F.C.; Oxford-Cardiff, C.-L.C.; et al. The role and uses of antibodies in COVID-19 infections: A living review. Oxf. Open Immunol. 2021, 2, iqab003. [Google Scholar] [CrossRef] [PubMed]
- Lou, B.; Li, T.D.; Zheng, S.F.; Su, Y.Y.; Li, Z.Y.; Liu, W.; Yu, F.; Ge, S.X.; Zou, Q.D.; Yuan, Q.; et al. Serology characteristics of SARS-CoV-2 infection after exposure and post-symptom onset. Eur. Respir. J. 2020, 56, 2000763. [Google Scholar] [CrossRef]
- Ma, H.; Zeng, W.; He, H.; Zhao, D.; Jiang, D.; Zhou, P.; Cheng, L.; Li, Y.; Ma, X.; Jin, T. Serum IgA, IgM, and IgG responses in COVID-19. Cell Mol. Immunol. 2020, 17, 773–775. [Google Scholar] [CrossRef] [PubMed]
- Isho, B.; Abe, K.T.; Zuo, M.; Jamal, A.J.; Rathod, B.; Wang, J.H.; Li, Z.; Chao, G.; Rojas, O.L.; Bang, Y.M.; et al. Persistence of serum and saliva antibody responses to SARS-CoV-2 spike antigens in COVID-19 patients. Sci. Immunol. 2020, 5. [Google Scholar] [CrossRef] [PubMed]
- Turner, J.S.; Kim, W.; Kalaidina, E.; Goss, C.W.; Rauseo, A.M.; Schmitz, A.J.; Hansen, L.; Haile, A.; Klebert, M.K.; Pusic, I.; et al. SARS-CoV-2 infection induces long-lived bone marrow plasma cells in humans. Nature 2021, 595, 421–425. [Google Scholar] [CrossRef]
- Ortega, N.; Ribes, M.; Vidal, M.; Rubio, R.; Aguilar, R.; Williams, S.; Barrios, D.; Alonso, S.; Hernandez-Luis, P.; Mitchell, R.A.; et al. Seven-month kinetics of SARS-CoV-2 antibodies and role of pre-existing antibodies to human coronaviruses. Nat. Commun. 2021, 12, 4740. [Google Scholar] [CrossRef]
- Xiao, K.; Yang, H.; Liu, B.; Pang, X.; Du, J.; Liu, M.; Liu, Y.; Jing, X.; Chen, J.; Deng, S.; et al. Antibodies Can Last for More Than 1 Year After SARS-CoV-2 Infection: A Follow-Up Study From Survivors of COVID-19. Front. Med. 2021, 8, 967. [Google Scholar] [CrossRef]
- Quattrocchi, A.; Mamais, I.; Tsioutis, C.; Christaki, E.; Constantinou, C.; Koliou, M.; Pana, Z.D.; Silvestros, V.; Theophanous, F.; Haralambous, C.; et al. Extensive Testing and Public Health Interventions for the Control of COVID-19 in the Republic of Cyprus between March and May 2020. J. Clin. Med. 2020, 9, 3598. [Google Scholar] [CrossRef]
- Gountas, I.; Quattrocchi, A.; Mamais, I.; Tsioutis, C.; Christaki, E.; Fokianos, K.; Nikolopoulos, G. Effect of public health interventions during the first epidemic wave of COVID-19 in Cyprus: A modelling study. medRxiv 2021. [Google Scholar] [CrossRef]
- Narasimhan, M.; Mahimainathan, L.; Araj, E.; Clark, A.E.; Markantonis, J.; Green, A.; Xu, J.; SoRelle, J.A.; Alexis, C.; Fankhauser, K.; et al. Clinical Evaluation of the Abbott Alinity SARS-CoV-2 Spike-Specific Quantitative IgG and IgM Assays among Infected, Recovered, and Vaccinated Groups. J. Clin. Microbiol. 2021, 59, e0038821. [Google Scholar] [CrossRef]
- Padoan, A.; Bonfante, F.; Pagliari, M.; Bortolami, A.; Negrini, D.; Zuin, S.; Bozzato, D.; Cosma, C.; Sciacovelli, L.; Plebani, M. Analytical and clinical performances of five immunoassays for the detection of SARS-CoV-2 antibodies in comparison with neutralization activity. EBioMedicine 2020, 62, 103101. [Google Scholar] [CrossRef] [PubMed]
- Piccoli, L.; Park, Y.J.; Tortorici, M.A.; Czudnochowski, N.; Walls, A.C.; Beltramello, M.; Silacci-Fregni, C.; Pinto, D.; Rosen, L.E.; Bowen, J.E.; et al. Mapping Neutralizing and Immunodominant Sites on the SARS-CoV-2 Spike Receptor-Binding Domain by Structure-Guided High-Resolution Serology. Cell 2020, 183, 1024–1042.e21. [Google Scholar] [CrossRef] [PubMed]
- Castro Dopico, X.; Ols, S.; Lore, K.; Karlsson Hedestam, G.B. Immunity to SARS-CoV-2 induced by infection or vaccination. J. Intern. Med. 2021. [Google Scholar] [CrossRef] [PubMed]
- Slifka, M.K.; Antia, R.; Whitmire, J.K.; Ahmed, R. Humoral immunity due to long-lived plasma cells. Immunity 1998, 8, 363–372. [Google Scholar] [CrossRef] [Green Version]
- Slifka, M.K.; Matloubian, M.; Ahmed, R. Bone marrow is a major site of long-term antibody production after acute viral infection. J. Virol. 1995, 69, 1895–1902. [Google Scholar] [CrossRef] [Green Version]
- Haveri, A.; Ekstrom, N.; Solastie, A.; Virta, C.; Osterlund, P.; Isosaari, E.; Nohynek, H.; Palmu, A.A.; Melin, M. Persistence of neutralizing antibodies a year after SARS-CoV-2 infection in humans. Eur. J. Immunol. 2021. [Google Scholar] [CrossRef]
- Dan, J.M.; Mateus, J.; Kato, Y.; Hastie, K.M.; Yu, E.D.; Faliti, C.E.; Grifoni, A.; Ramirez, S.I.; Haupt, S.; Frazier, A.; et al. Immunological memory to SARS-CoV-2 assessed for up to 8 months after infection. Science 2021, 371, eabf4063. [Google Scholar] [CrossRef]
- Premkumar, L.; Segovia-Chumbez, B.; Jadi, R.; Martinez, D.R.; Raut, R.; Markmann, A.; Cornaby, C.; Bartelt, L.; Weiss, S.; Park, Y.; et al. The receptor binding domain of the viral spike protein is an immunodominant and highly specific target of antibodies in SARS-CoV-2 patients. Sci. Immunol. 2020, 5, eabc8413. [Google Scholar] [CrossRef]
- Suthar, M.S.; Zimmerman, M.G.; Kauffman, R.C.; Mantus, G.; Linderman, S.L.; Hudson, W.H.; Vanderheiden, A.; Nyhoff, L.; Davis, C.W.; Adekunle, O.; et al. Rapid Generation of Neutralizing Antibody Responses in COVID-19 Patients. Cell Rep. Med. 2020, 1, 100040. [Google Scholar] [CrossRef]
- Iyer, A.S.; Jones, F.K.; Nodoushani, A.; Kelly, M.; Becker, M.; Slater, D.; Mills, R.; Teng, E.; Kamruzzaman, M.; Garcia-Beltran, W.F.; et al. Persistence and decay of human antibody responses to the receptor binding domain of SARS-CoV-2 spike protein in COVID-19 patients. Sci. Immunol. 2020, 5, eabe0367. [Google Scholar] [CrossRef]
- Roltgen, K.; Powell, A.E.; Wirz, O.F.; Stevens, B.A.; Hogan, C.A.; Najeeb, J.; Hunter, M.; Wang, H.; Sahoo, M.K.; Huang, C.; et al. Defining the features and duration of antibody responses to SARS-CoV-2 infection associated with disease severity and outcome. Sci. Immunol. 2020, 5, eabe0240. [Google Scholar] [CrossRef]
- Li, K.; Huang, B.; Wu, M.; Zhong, A.; Li, L.; Cai, Y.; Wang, Z.; Wu, L.; Zhu, M.; Li, J.; et al. Dynamic changes in anti-SARS-CoV-2 antibodies during SARS-CoV-2 infection and recovery from COVID-19. Nat. Commun. 2020, 11, 6044. [Google Scholar] [CrossRef]
- Wang, X.; Guo, X.; Xin, Q.; Pan, Y.; Hu, Y.; Li, J.; Chu, Y.; Feng, Y.; Wang, Q. Neutralizing Antibody Responses to Severe Acute Respiratory Syndrome Coronavirus 2 in Coronavirus Disease 2019 Inpatients and Convalescent Patients. Clin. Infect. Dis. 2020, 71, 2688–2694. [Google Scholar] [CrossRef]
- Robbiani, D.F.; Gaebler, C.; Muecksch, F.; Lorenzi, J.C.C.; Wang, Z.; Cho, A.; Agudelo, M.; Barnes, C.O.; Gazumyan, A.; Finkin, S.; et al. Convergent antibody responses to SARS-CoV-2 in convalescent individuals. Nature 2020, 584, 437–442. [Google Scholar] [CrossRef] [PubMed]
- Zeng, F.; Dai, C.; Cai, P.; Wang, J.; Xu, L.; Li, J.; Hu, G.; Wang, Z.; Zheng, F.; Wang, L. A comparison study of SARS-CoV-2 IgG antibody between male and female COVID-19 patients: A possible reason underlying different outcome between sex. J. Med. Virol. 2020, 92, 2050–2054. [Google Scholar] [CrossRef]
- Ye, X.Y.; Angelo, L.S.; Nicholson, E.G.; Iwuchukwu, O.P.; de Rezende, W.C.; Rajan, A.; Aideyan, L.O.; McBride, T.J.; Bond, N.; Santarcangelo, P.; et al. Serum IgG anti-SARS-CoV-2 Binding Antibody Level Is Strongly Associated With IgA and Functional Antibody Levels in Adults Infected With SARS-CoV-2. Front. Immunol. 2021, 12. [Google Scholar] [CrossRef] [PubMed]
- Grzelak, L.; Velay, A.; Madec, Y.; Gallais, F.; Staropoli, I.; Schmidt-Mutter, C.; Wendling, M.J.; Meyer, N.; Planchais, C.; Rey, D.; et al. Sex Differences in the Evolution of Neutralizing Antibodies to Severe Acute Respiratory Syndrome Coronavirus 2. J. Infect. Dis. 2021, 224, 983–988. [Google Scholar] [CrossRef] [PubMed]
- Sette, A.; Crotty, S. Adaptive immunity to SARS-CoV-2 and COVID-19. Cell 2021, 184, 861–880. [Google Scholar] [CrossRef]
- Kennedy, N.A.; Goodhand, J.R.; Bewshea, C.; Nice, R.; Chee, D.; Lin, S.; Chanchlani, N.; Butterworth, J.; Cooney, R.; Croft, N.M.; et al. Anti-SARS-CoV-2 antibody responses are attenuated in patients with IBD treated with infliximab. Gut 2021, 70, 865–875. [Google Scholar] [CrossRef]
- Kaplan, G.G.; Ma, C.; Charlton, C.; Kanji, J.N.; Tipples, G.; Sharifi, N.; Herauf, M.; Coward, S.; Ingram, R.J.M.; Hracs, L.; et al. Antibody response to SARS-CoV-2 among individuals with IBD diminishes over time: A serosurveillance cohort study. Gut 2021. [Google Scholar] [CrossRef]
- Chavarot, N.; Leruez-Ville, M.; Scemla, A.; Burger, C.; Amrouche, L.; Rouzaud, C.; Lebreton, X.; Martinez, F.; Sberro-Soussan, R.; Legendre, C.; et al. Decline and loss of anti-SARS-CoV-2 antibodies in kidney transplant recipients in the 6 months following SARS-CoV-2 infection. Kidney Int. 2021, 99, 486–488. [Google Scholar] [CrossRef] [PubMed]
- Jordan, S.C. Innate and adaptive immune responses to SARS-CoV-2 in humans: Relevance to acquired immunity and vaccine responses. Clin. Exp. Immunol. 2021, 204, 310–320. [Google Scholar] [CrossRef] [PubMed]
- Lawandi, A.; Warner, S.; Sun, J.; Demirkale, C.Y.; Danner, R.L.; Klompas, M.; Gundlapalli, A.; Datta, D.; Harris, A.M.; Morris, S.B.; et al. Suspected SARS-CoV-2 Reinfections: Incidence, Predictors, and Healthcare Use among Patients at 238 U.S. Healthcare Facilities, June 1, 2020- February 28, 2021. Clin. Infect. Dis. 2021. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| All (n = 1898) | Reported Past SARS-CoV-2 Infection n (%) 1112 (58.6%) | No History of SARS-CoV-2 Infection n(%) 786 (41.4%) | p-Value | |
|---|---|---|---|---|
| Age in years | ||||
| Median (IQR) | 46.0 (35.0–57.0) | 45.0 (33.0–55.0) | 47.0 (37.0–58.0) | <0.001 ‡ |
| Gender, n (%) | ||||
| Female | 770 (40.6) | 670 (60.2) | 456 (58.0) | 0.607 ¥ |
| Male | 1126 (59.3) | 441 (39.7) | 329 (41.9) | |
| Not Reported | 2 (0.1) | 1 (0.1) | 1 (0.1) | |
| Place of residence, n (%) | ||||
| Abroad | 78 (4.1) | 35 (3.2) | 43 (5.5) | |
| Ammochostos | 55 (2.9) | 31 (2.8) | 24 (3.1) | |
| Nicosia | 1413 (74.5) | 800 (71.9) | 613 (77.9) | <0.001 ¥ |
| Larnaca | 140 (7.4) | 79 (7.1) | 61 (7.8) | |
| Limassol | 150 (7.9) | 125 (11.2) | 25 (3.2) | |
| Paphos | 61 (3.1) | 41 (3.7) | 20 (2.5) | |
| Not Reported | 1 (0.1) | 1 (0.1) | 0 (0.0) | |
| Nationality, n (%) | ||||
| Cypriot | 1789 (94.3) | 1050 (94.4) | 739 (94.0) | 0.686 ¥ |
| Other | 104 (5.5) | 60 (5.4) | 44 (5.6) | |
| Not Reported | 5 (0.2) | 2 (0.2) | 3 (0.4) | |
| HCW, n (%) | ||||
| Yes | 314 (16.5) | 123 (11.1) | 191 (24.3) | <0.001 ¥ |
| No | 1584 (83.5) | 989 (88.9) | 595 (75.7) | |
| Smoking, n (%) | ||||
| Yes | 317 (16.7) | 158 (14.2) | 159 (20.2) | |
| No | 1571 (82.8) | 944 (84.9) | 627 (79.8) | <0.001 ¥ |
| No Answer | 10 (0.5) | 10 (0.9) | 0 (0.0) | |
| All (n = 1898) | Reported Past SARS-CoV-2 Infection n (%) 1112 (58.6%) | Without Reported History of SARS-CoV-2 Infection n (%) 786 (41.4) | p-Value | |
|---|---|---|---|---|
| Vaccination against COVID-19-1 dose, n (%) | ||||
| Yes 761 (40.1) | 143 (12.9) | 618 (78.6) | <0.001 ¥ | |
| No 1137 (59.1) | 969 (87.1) | 168 (21.4) | ||
| Vaccination against COVID-19-2 doses, n (%) | ||||
| Yes 687 (36.2) | 87 (7.8) | 600 (76.3) | <0.001 ¥ | |
| No 1211 (63.8) | 1025 (92.2) | 186 (23.7) | ||
| IgG test-Qualitative (S/C index)-n = 734 * | n = 622 | n = 112 | ||
| ≥1.4 | 436 (59.4) | 431 (69.3) | 5 (4.5) | <0.001 ¥ |
| <1.4 | 298 (40.6) | 191 (30.7) | 107 (95.5) | |
| IgG test-Qualitative (S/C index)-n = 734 * | n = 622 | n = 112 | ||
| Median (IQR) | 2.2 (0.5–4.8) | 2.9 (1.1–5.2) | 0.03 (0.02–0.07) | <0.001 ‡ |
| IgG test Quantitative (AU/mL)-n = 1132 * | n = 969 | n = 163 | ||
| ≥50 | 930 (82.2) | 909 (93.8) | 21 (12.9) | <0.001 ¥ |
| <50 | 202 (17.8) | 60 (6.2) | 142 (87.1) | |
| IgG test Quantitative (AU/mL)-n = 1132 * | n = 969 | n = 163 | ||
| Median (IQR) | 340.9 (105.2–994.2) | 432.1 (182.4–1147.3) | 0.0 (0.0–0.9) | <0.001 ‡ |
| IgG Test–Qualitative (S/C Index) (No History of Vaccination against COVID-19) | IgG Test–Quantitative (AU/mL) (No History of Vaccination against COVID-19) | |||||
|---|---|---|---|---|---|---|
| n = 622 | n = 969 | |||||
| ≥1.4 | <1.4 | p Value ¥ | OR (95% CI) | Median (IQR) | p Value ‡ | |
| Age | ||||||
| 0–19 | 10 (2.3) | 17 (8.7) | Ref | 425.4 (205.8–788.2) | ||
| 20–59 | 317 (73.6) | 159 (83.3) | 3.4 (1.5–7.6) | 353.3 (157.8–869.2) | ||
| ≥60 | 104 (24.1) | 15 (7.8) | <0.001 | 11.8 (4.6–30.5) | 1413.7 (567.4–3267.5) | <0.001 |
| Gender | ||||||
| Female | 242 (56.2) | 125 (65.5) | Ref | 368.3 (166.0–909.7) | ||
| Male | 189 (43.9) | 66 (34.5) | 0.030 | 1.5 (1.1–2.1) | 529.8 (206.8–1655.9) | <0.001 |
| Symptoms | ||||||
| Yes | 417 (96.8) | 170 (89.0) | 3.7 (1.8–7.4) | 441.8 (187.1–1165.6) | ||
| No | 14 (3.3) | 21 (11.0) | <0.001 | Ref | 264.2 (46.9–636.5) | 0.001 |
| Fever | ||||||
| Yes | 160 (37.1) | 51 (26.7) | 1.6 (1.1–2.4) | 577.5 (216.7–1866.8) | ||
| No | 271 (62.9) | 140 (73.3) | 0.011 | Ref | 374.5 (161.0–970.8) | <0.001 |
| Cough | ||||||
| Yes | 224 (52.0) | 66 | 2.0 (1.4–2.9) | 578.2 (223.3–1591.0) | ||
| (34.6) | ||||||
| No | 207 (48.0) | 125 (65.5) | <0.001 | Ref | 349.9 (153.6–829.8) | <0.001 |
| Shortness of breath | ||||||
| Yes | 121 (28.1) | 45 (23.6) | 1.3 (0.9–1.9) | 621.1 (216.7–1912.3) | ||
| No | 310 (71.9) | 146 (76.4) | 0.240 | Ref | 383.2 (166.0–966.7) | <0.001 |
| Muscle aches | ||||||
| Yes | 228 (52.9) | 89 (46.6) | 1.3 (0.9–1.8) | 418.8 (189.6–1164.9) | ||
| No | 203 (47.1) | 102 (53.4) | 0.147 | Ref | 443.4 (167.6–1122.0) | 0.862 |
| Sore throat | ||||||
| Yes | 133 (30.9) | 52 (27.2) | 1.2 (0.8–1.7) | 397.9 (186.5–1148.9) | ||
| No | 298 (69.1) | 139 (72.8) | 0.361 | Ref | 442.9 (178.4–1145.7) | 0.694 |
| Loss of taste | ||||||
| Yes | 222 (51.5) | 89 (46.6) | 1.2 (0.9–1.7) | 415.8 (184.7–1108.1) | ||
| No | 209 (48.5) | 102 (53.4) | 0.258 | Ref | 440.9 (175.4–1205.1) | 0.816 |
| Loss of smell | ||||||
| Yes | 244 (56.6) | 96 (50.3) | 1.3 (0.9–1.8) | 381.9 (170.7–1064.8) | ||
| No | 187 (43.4) | 95 (49.7) | 0.142 | Ref | 471.0 (194.8–1321.9) | 0.135 |
| Headache | ||||||
| Yes | 237 (55.0) | 97 (50.8) | 1.2 (0.8–1.7) | 427.1 (180.7–1144.6) | ||
| No | 194 (45.0) | 94 (49.2) | 0.332 | Ref | 439.7 (182.4–1204.7) | 0.877 |
| Fatigue | ||||||
| Yes | 284 (65.9) | 115 (60.2) | 1.3 (0.9–1.8) | 438.1 (186.5–1246.7) | ||
| No | 147 (34.1) | 76 (39.8) | 0.173 | Ref | 406.7 (170.4–1036.6) | 0.100 |
| Red feet toes | ||||||
| Yes | 3 (0.7) | 1 (0.5) | 1.3 (0.1–12.9) | 415.0 (236.0–814.4) | ||
| No | 428 (99.3) | 190 (99.5) | 0.639 | Ref | 432.1 (180.7–1148.9) | 0.947 |
| Nausea and Vomiting | ||||||
| Yes | 64 (14.9) | 17 (8.9) | 1.8 (1.2–3.1) | 460.9 (212.4–1538.8) | ||
| No | 367 (85.1) | 174 (91.1) | 0.042 | Ref | 425.4 (173.8–1108.1) | 0.109 |
| Diarrhea | ||||||
| Yes | 95 (22.0) | 35 (18.3) | 1.3 (0.8–1.9) | 666.8 (270.0–1602.2) | ||
| No | 336 (78.0) | 156 (81.7) | 0.293 | Ref | 384.7 (163.1–1038.3) | <0.001 |
| More than two Symptoms | ||||||
| Yes | 389 (89.4) | 152 (79.6) | 2.4 (1.5–3.8) | 443.4 (187.3–12,608.5) | ||
| No | 42 (10.6) | 39 (20.4) | <0.001 | Ref | 354.1 (115.1–758.0) | <0.001 |
| HCW | ||||||
| Yes | 52 (12.1) | 30 (15.7) | 0.7 (0.5–1.2) | 331.8 (136.7–850.9) | ||
| No | 379 (87.9) | 161 (84.3) | 0.216 | Ref | 441.8 (186.5–1166.7) | 0.048 |
| Hospital Admission | ||||||
| Yes | 34 (7.9) | 6 (3.1) | 2.6 (1.1–6.4) | 2832.2 (1325.5–4165.4) | ||
| No | 397 (92.1) | 185 (96.9) | 0.026 | Ref | 388.1 (171.8–989.0) | <0.001 |
| Difference between dates of reported 1st SARS-CoV-2 diagnostic test and IgG test | ||||||
| ≤1 month | 29 (6.7) | 7 (3.7) | 4.5 (1.6–12.5) | 447.9 (194.2–1318.2) | ||
| (1–3) months | 312 (72.6) | 97 (50.8) | 3.5 (1.9–6.6) | 488.5 (216.2–1365.5) | ||
| (3–6) months | 68 (15.8) | 64 (33.5) | 1.2 (0.6–2.3) | 341.6 (149.4–856.2) | ||
| >6 months | 21 (4.9) | 23 (12.0) | <0.001 | Ref | 327.3 (163.6–874.8) | <0.001 |
| Difference between dates of symptom onset and IgG test | ||||||
| ≤1 month | 30 (7.0) | 7 (3.7) | 5.5 (2.1–14.3) | 447.5 (207.6–1363.9) | ||
| (1–3) months | 303 (70.5) | 89 (46.6) | 4.4 (2.6–7.4) | 495.0 (222.6–1407.0) | ||
| (3–6) months | 66 (15.3) | 55 (28.8) | 1.5 (0.9–2.8) | 354.0 (153.6–894.4) | ||
| >6 months | 31 (7.2) | 40 (20.9) | <0.001 | Ref | 300.8 (120.8–890.0) | <0.001 |
| (1) | (2) | (3) | (4) | |
|---|---|---|---|---|
| Variables | Model 1– Characteristics of Participants | Model 2–Symptoms | Model 3–Hospital Admission | Model 4–Overall |
| Fever (Yes) | 0.149 *** | 0.100 ** | ||
| (0.044) | (0.042) | |||
| Cough (Yes) | 0.143 *** | 0.109 *** | ||
| (0.043) | (0.040) | |||
| Shortness of breath (Yes) | 0.112 ** | 0.028 | ||
| (0.048) | (0.046) | |||
| Diarrhea (Yes) | 0.132 *** | 0.075 | ||
| (0.050) | (0.047) | |||
| Symptoms Duration (in days) | 0.002 ** | 0.001 | ||
| (0.001) | (0.001) | |||
| At Least two Symptoms (Yes) | −0.029 | 0.116 * | ||
| (0.081) | (0.068) | |||
| Time difference between date of symptoms and date of antibody test | −0.0011 *** | |||
| (0.000) | ||||
| Age (in Years) | 0.011 *** | 0.020 *** | ||
| (0.001) | (0.001) | |||
| Gender (Female) | −0.134 *** | −0.102 ** | ||
| (0.040) | (0.040) | |||
| BMI (kg/m2) | 0.019 *** | 0.015 *** | ||
| (0.004) | (0.004) | |||
| Smoking Status (Yes) | −0.238 *** | −0.201 *** | ||
| (0.054) | (0.055) | |||
| Health Care Workers (Yes) | −0.107 * | −0.064 | ||
| (0.062) | (0.061) | |||
| Time difference between date of first diagnostic test for SARS-CoV-2 (antigen-based or molecular) and date of antibody test | −0.001 *** | −0.001 *** | ||
| (0.000) | (0.000) | |||
| Hospital Admission (Yes) | 0.734 *** | 0.415 *** | ||
| (0.080) | (0.082) | |||
| Constant | 1.891 *** | 2.591 *** | 2.613 *** | 1.793 *** |
| (0.112) | (0.081) | (0.020) | (0.125) | |
| Observations | 930 | 833 | 956 | 844 |
| R-squared | 0.170 | 0.080 | 0.081 | 0.251 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mamais, I.; Malatras, A.; Papagregoriou, G.; Giallourou, N.; Kakouri, A.C.; Karayiannis, P.; Koliou, M.; Christaki, E.; Nikolopoulos, G.K.; Deltas, C. Circulating IgG Levels in SARS-CoV-2 Convalescent Individuals in Cyprus. J. Clin. Med. 2021, 10, 5882. https://doi.org/10.3390/jcm10245882
Mamais I, Malatras A, Papagregoriou G, Giallourou N, Kakouri AC, Karayiannis P, Koliou M, Christaki E, Nikolopoulos GK, Deltas C. Circulating IgG Levels in SARS-CoV-2 Convalescent Individuals in Cyprus. Journal of Clinical Medicine. 2021; 10(24):5882. https://doi.org/10.3390/jcm10245882
Chicago/Turabian StyleMamais, Ioannis, Apostolos Malatras, Gregory Papagregoriou, Natasa Giallourou, Andrea C. Kakouri, Peter Karayiannis, Maria Koliou, Eirini Christaki, Georgios K. Nikolopoulos, and Constantinos Deltas. 2021. "Circulating IgG Levels in SARS-CoV-2 Convalescent Individuals in Cyprus" Journal of Clinical Medicine 10, no. 24: 5882. https://doi.org/10.3390/jcm10245882