
The Influence of SARS-CoV-2 Pandemic in the Diagnosis and Treatment of Cervical Dysplasia

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
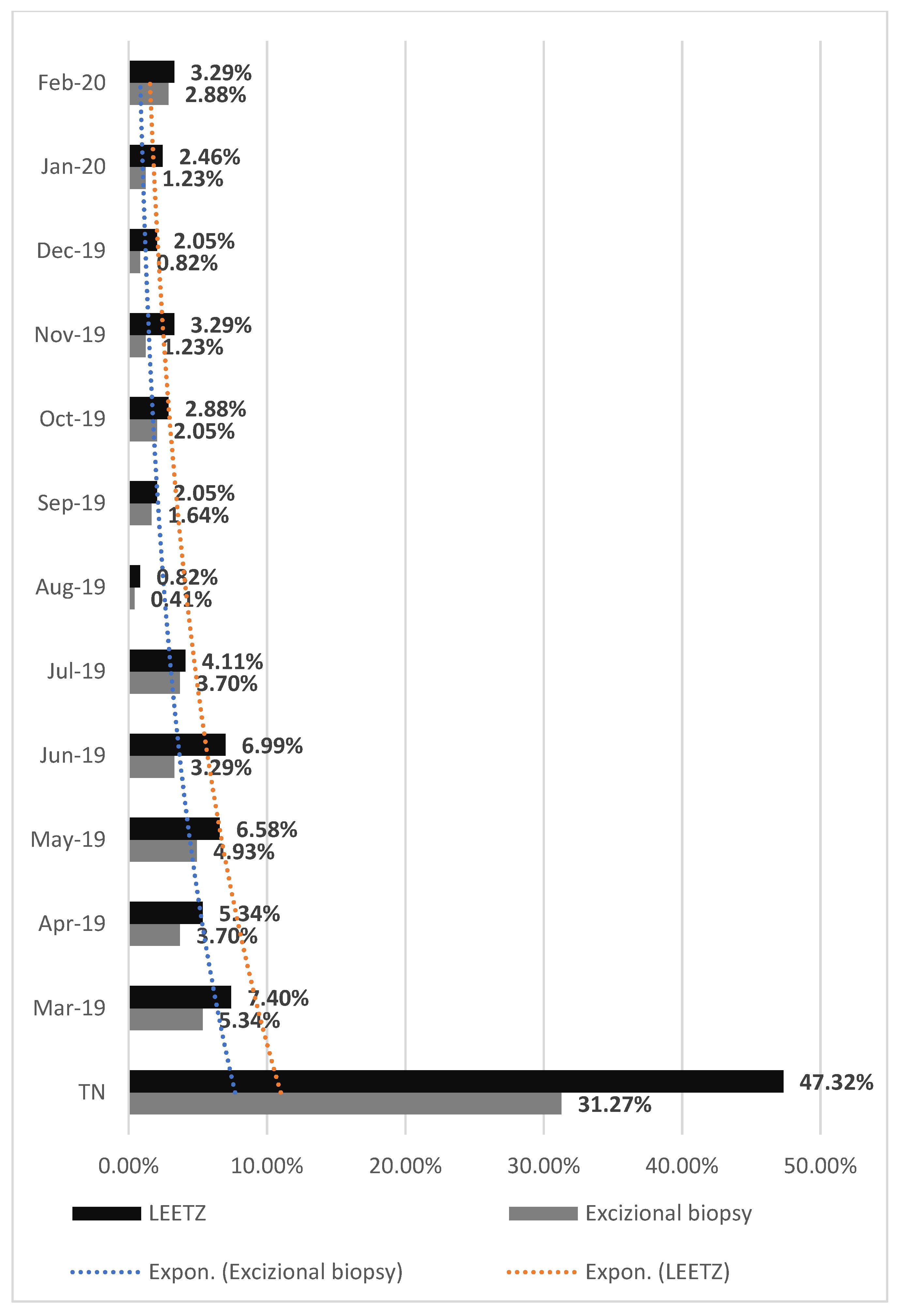
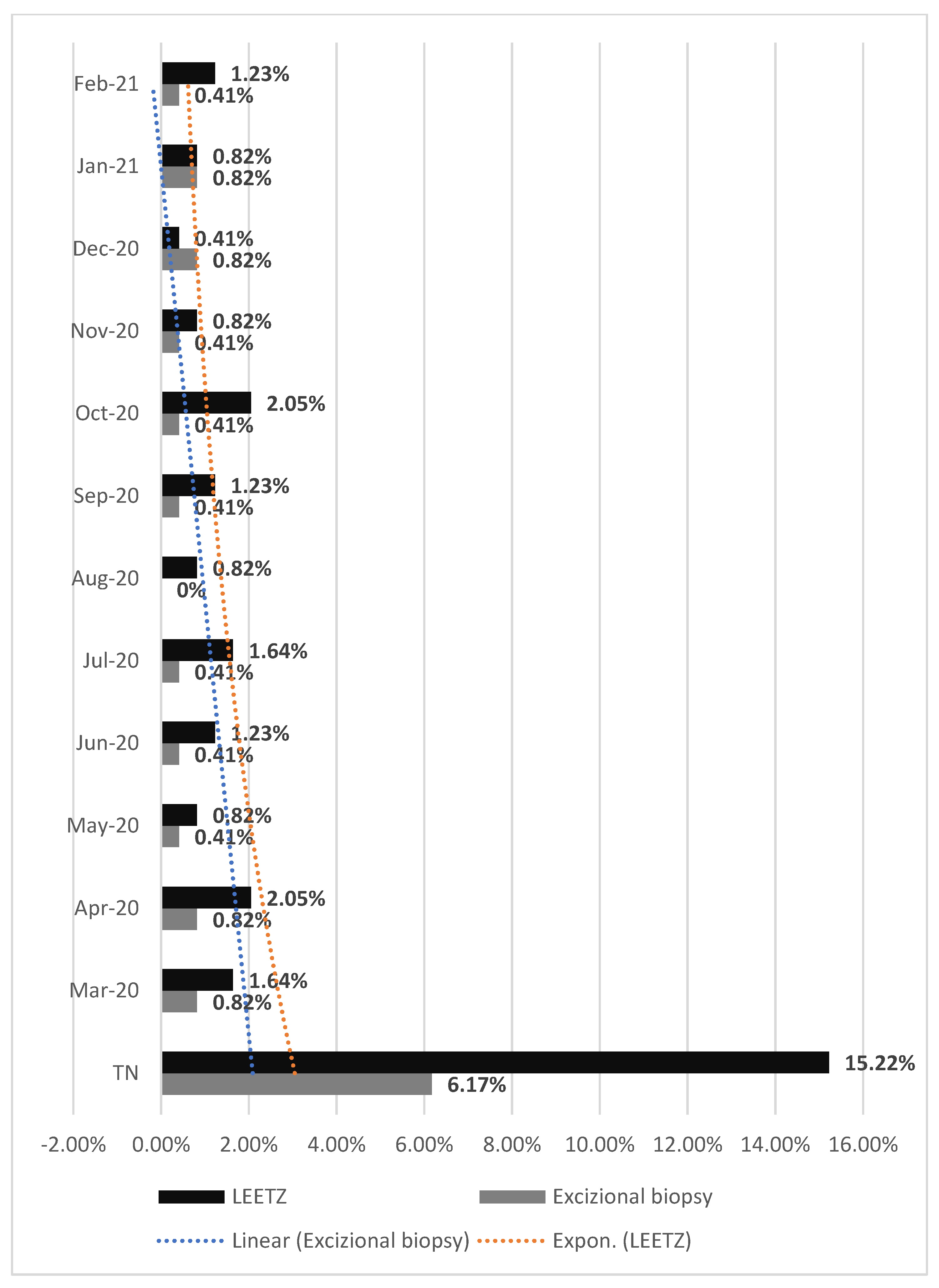
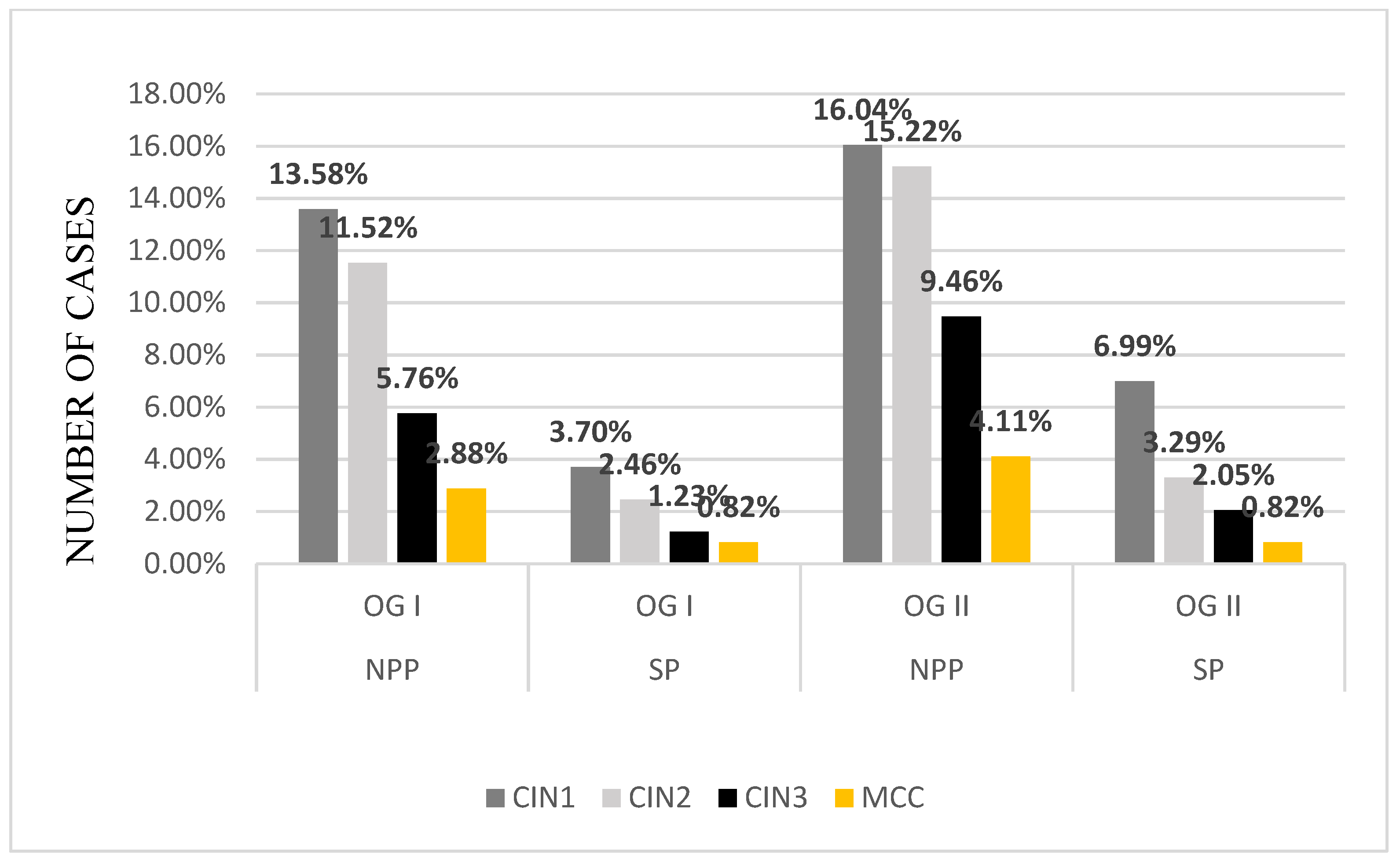
3. Results
4. Discussion
4.1. Context of the Research, Diagnosis Results Following Screening
4.2. Influence of the Pandemic Crisis
5. Conclusions
Author Contributions
Funding
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Moshkovich, O.; Lebrun-Harris, L.; Makaroff, L.; Chidambaran, P.; Chung, M.; Sripipatana, A.; Lin, S.C. Challenges and Opportunities to Improve Cervical Cancer Screening Rates in US Health Centers through Patient-Centered Medical Home Transformation. Adv. Prev. Med. 2015, 2015, 182073. [Google Scholar] [CrossRef] [Green Version]
- Benard, V.B.; Thomas, C.C.; King, J.; Massetti, G.M.; Doria-Rose, V.P.; Saraiya, M. Centers for Disease Control and Prevention (CDC) Vital Signs: Cervical Cancer Incidence, Mortality, and Screening—United States, 2007–2012. MMWR Morb. Mortal Wkly. Rep. 2014, 63, 1004–1009. [Google Scholar]
- Kalliala, I.; Athanasiou, A.; Veroniki, A.A.; Salanti, G.; Efthimiou, O.; Raftis, N.; Bowden, S.; Paraskevaidi, M.; Aro, K.; Arbyn, M.; et al. Incidence and Mortality from Cervical Cancer and Other Malignancies after Treatment of Cervical Intraepithelial Neoplasia: A Systematic Review and Meta-Analysis of the Literature. Ann. Oncol. 2020, 31, 213–227. [Google Scholar] [CrossRef] [Green Version]
- Rees, M.; Angioli, R.; Coleman, R.L.; Glasspool, R.; Plotti, F.; Simoncini, T.; Terranova, C. European Menopause and Andropause Society (EMAS) and International Gynecologic Cancer Society (IGCS) Position Statement on Managing the Menopause after Gynecological Cancer: Focus on Menopausal Symptoms and Osteoporosis. Maturitas 2020, 134, 56–61. [Google Scholar] [CrossRef]
- Kyrgiou, M.; Arbyn, M.; Bergeron, C.; Bosch, F.X.; Dillner, J.; Jit, M.; Kim, J.; Poljak, M.; Nieminen, P.; Sasieni, P.; et al. Cervical Screening: ESGO-EFC Position Paper of the European Society of Gynaecologic Oncology (ESGO) and the European Federation of Colposcopy (EFC). Br. J. Cancer 2020, 123, 510–517. [Google Scholar] [CrossRef] [PubMed]
- Cancer Today. Available online: http://gco.iarc.fr/today/home (accessed on 30 September 2021).
- Health Profile Romania. Available online: https://www.worldlifeexpectancy.com/country-health-profile/romania (accessed on 30 September 2021).
- Andreassen, T.; Weiderpass, E.; Nicula, F.; Suteu, O.; Itu, A.; Bumbu, M.; Tincu, A.; Ursin, G.; Moen, K. Controversies about Cervical Cancer Screening: A Qualitative Study of Roma Women’s (Non)Participation in Cervical Cancer Screening in Romania. Soc. Sci. Med. 2017, 183, 48–55. [Google Scholar] [CrossRef] [PubMed]
- Arbyn, M.; Raifu, A.O.; Weiderpass, E.; Bray, F.; Anttila, A. Trends of Cervical Cancer Mortality in the Member States of the European Union. Eur. J. Cancer 2009, 45, 2640–2648. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.J.; Burger, E.A.; Regan, C.; Sy, S. Screening for Cervical Cancer in Primary Care: A Decision Analysis for the US Preventive Services Task Force. JAMA 2018, 320, 706–714. [Google Scholar] [CrossRef]
- Raţiu, A.C.; Secoşan, C.A.; Balint, O.; Sas, I.; Grigoraş, D.; Ilina, R.Ş.; Jianu, A.M.; Motoc, A.G.M.; Pirtea, L.C. The Importance of Immunocytochemistry in the Detection of High-Grade Cervical Lesions. Rom. J. Morphol. Embryol. 2017, 58, 1151–1156. [Google Scholar]
- Istvan Nyirjesym, Conization of Cervix: Background, History of the Procedure, Problem. Available online: https://emedicine.medscape.com/article/270156-overview (accessed on 30 August 2021).
- Coronavirus (COVID-19) Events as They Happen. Available online: https://www.who.int/emergencies/diseases/novel-coronavirus-2019/events-as-they-happen (accessed on 30 August 2021).
- Education: From Disruption to Recovery. Available online: https://en.unesco.org/covid19/educationresponse (accessed on 30 August 2021).
- Velavan, T.P.; Meyer, C.G. The COVID-19 Epidemic. Trop. Med. Int. Health 2020, 25, 278–280. [Google Scholar] [CrossRef] [Green Version]
- AHA Letter to Surgeon General Re: Elective Surgeries and COVID-19. Available online: https://www.aha.org/lettercomment/2020-03-15-aha-letter-surgeon-general-re-elective-surgeries-and-covid-19 (accessed on 30 August 2021).
- Stahel, P.F. How to Risk-Stratify Elective Surgery during the COVID-19 Pandemic? Patient Saf. Surg. 2020, 14, 8. [Google Scholar] [CrossRef]
- COVID-19: Guidance for Triage of Non-Emergent Surgical Procedures. Available online: http://www.facs.org/covid-19/clinical-guidance/triage (accessed on 30 August 2021).
- Coronavirus Disease (COVID-19) Situation Reports. Available online: https://www.who.int/emergencies/diseases/novel-coronavirus-2019/situation-reports (accessed on 30 August 2021).
- HealthLeaders Surgeon General Urges Providers to “Consider Stopping Elective Surgeries.” Hospitals Push Back. Available online: https://www.healthleadersmedia.com/clinical-care/surgeon-general-urges-providers-consider-stopping-elective-surgeries-hospitals-push (accessed on 30 August 2021).
- Elston, D.M. The Coronavirus (COVID-19) Epidemic and Patient Safety. J. Am. Acad Derm. 2020, 82, 819–820. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, R.; Zhang, Y.; Huang, L.; Cheng, B.-H.; Xia, Z.-Y.; Meng, Q.-T. Safety and Efficacy of Different Anesthetic Regimens for Parturients with COVID-19 Undergoing Cesarean Delivery: A Case Series of 17 Patients. Can. J. Anaesth. 2020, 67, 655–663. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lie, S.A.; Wong, S.W.; Wong, L.T.; Wong, T.G.L.; Chong, S.Y. Practical Considerations for Performing Regional Anesthesia: Lessons Learned from the COVID-19 Pandemic. Can. J. Anaesth. 2020, 67, 885–892. [Google Scholar] [CrossRef] [Green Version]
- Petrescu, A.-M.; Ruican, D.; Zorila, L.; Cernea, N.; Tudorache, S.; Iliescu, D. Modern Cervical Imaging Assessment. Review of Literature on Confocal Microscopy and Digital Automated Colposcopy. Obstet. Şi. Ginecol. 2019, 3, 5–8. [Google Scholar] [CrossRef]
- Comanescu, A.; Iliescu, D.; Comanescu, M.; Cernea, N.; Mogoanta, L.; Simionescu, C. Colposcopic Evaluation of Neoplasic and Preneoplasic Lesions of the Cervix—A Retrospective Study. Curr. Health Sci. J. 2010, 36, 63–65. [Google Scholar]
- Boicea, A.; Pătraşcu, A.; Surlin, V.; Iliescu, D.; Schenker, M.; Chiuţu, L. Correlations between Colposcopy and Histologic Results from Colposcopically Directed Biopsy in Cervical Precancerous Lesions. Rom. J. Morphol. Embryol. 2012, 53, 735–741. [Google Scholar] [PubMed]
- Ferlay, J.; Soerjomataram, I.; Ervik, M.; Dikshit, R.; Eser, S.; Mathers, C.; Rebelo, M.; Parkin, D.M.; Forman, D.; Bray, F. GLOBOCAN 2012: Estimated Cancer Incidence, Mortality and Prevalence Worldwide in 2012 v1.0; IARC CancerBase No. 11; IARC: Lion, France, 2012; ISBN 978-92-832-2447-1. [Google Scholar]
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef]
- Anton, G.; Peltecu, G.; Socolov, D.; Cornitescu, F.; Bleotu, C.; Sgarbura, Z.; Teleman, S.; Iliescu, D.; Botezatu, A.; Goia, C.D.; et al. Type-Specific Human Papillomavirus Detection in Cervical Smears in Romania. APMIS 2011, 119, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Eniu, A.; Dumitraşcu, D.; Geanta, M. Romania, Attempting to Catch up the European Standards of Care for Cancer Patients. In Cancer Care in Countries and Societies in Transition; Springer: Cham, Switzerland, 2016; pp. 361–374. ISBN 978-3-319-22911-9. [Google Scholar]
- Calfa, G.; Popa, E.; Pletea, D.; Grigore, M.; Pavaleanu, I. O Analiza SWOT a Rezultatelor Screeningului de Cancer de Col Uterin (2012–2016). SNMF Congress: Iași, Romania, 2016. [Google Scholar]
- The Impact of Episodic Screening Interruption: COVID-19 and Population-Based Cancer Screening in Canada—PubMed. Available online: https://pubmed.ncbi.nlm.nih.gov/33241760/ (accessed on 30 August 2021).
- Dinmohamed, A.G.; Cellamare, M.; Visser, O.; de Munck, L.; Elferink, M.A.G.; Westenend, P.J.; Wesseling, J.; Broeders, M.J.M.; Kuipers, E.J.; Merkx, M.A.W.; et al. The Impact of the Temporary Suspension of National Cancer Screening Programmes Due to the COVID-19 Epidemic on the Diagnosis of Breast and Colorectal Cancer in the Netherlands. J. Hematol. Oncol. 2020, 13, 147. [Google Scholar] [CrossRef]
- Maringe, C.; Spicer, J.; Morris, M.; Purushotham, A.; Nolte, E.; Sullivan, R.; Rachet, B.; Aggarwal, A. The Impact of the COVID-19 Pandemic on Cancer Deaths Due to Delays in Diagnosis in England, UK: A National, Population-Based, Modelling Study. Lancet Oncol. 2020, 21, 1023–1034. [Google Scholar] [CrossRef]
- de Jonge, L.; Worthington, J.; van Wifferen, F.; Iragorri, N.; Peterse, E.F.P.; Lew, J.-B.; Greuter, M.J.E.; Smith, H.A.; Feletto, E.; Yong, J.H.E.; et al. Impact of the COVID-19 Pandemic on Faecal Immunochemical Test-Based Colorectal Cancer Screening Programmes in Australia, Canada, and the Netherlands: A Comparative Modelling Study. Lancet Gastroenterol. Hepatol. 2021, 6, 304–314. [Google Scholar] [CrossRef]
- Khanna, D.; Khargekar, N.C.; Khanna, A.K. Implementation of Early Detection Services for Cancer in India During COVID-19 Pandemic. Cancer Control. 2020, 27, 1073274820960471. [Google Scholar] [CrossRef]
- Cancino, R.S.; Su, Z.; Mesa, R.; Tomlinson, G.E.; Wang, J. The Impact of COVID-19 on Cancer Screening: Challenges and Opportunities. JMIR Cancer 2020, 6, e21697. [Google Scholar] [CrossRef] [PubMed]
- Castanon, A.; Rebolj, M.; Pesola, F.; Sasieni, P. Recovery Strategies Following COVID-19 Disruption to Cervical Cancer Screening and Their Impact on Excess Diagnoses. Br. J. Cancer 2021, 124, 1361–1365. [Google Scholar] [CrossRef]
- Long Term Predictive Values of Cytology and Human Papillomavirus Testing in Cervical Cancer Screening: Joint European Cohort Study—The BMJ. Available online: https://www.bmj.com/content/337/bmj.a1754 (accessed on 30 August 2021).
- Castanon, A.; Rebolj, M.; Burger, E.A.; de Kok, I.M.C.M.; Smith, M.A.; Hanley, S.J.B.; Carozzi, F.M.; Peacock, S.; O’Mahony, J.F. Cervical Screening during the COVID-19 Pandemic: Optimising Recovery Strategies. Lancet Public Health 2021, 6, e522–e527. [Google Scholar] [CrossRef]
- De Pelsemaeker, M.-C.; Guiot, Y.; Vanderveken, J.; Galant, C.; Van Bockstal, M.R. The Impact of the COVID-19 Pandemic and the Associated Belgian Governmental Measures on Cancer Screening, Surgical Pathology and Cytopathology. Pathobiology 2021, 88, 46–55. [Google Scholar] [CrossRef]
- EHRN Delayed Cancer Screenings. Available online: https://ehrn.org/articles/delays-in-preventive-cancer-screenings-during-covid-19-pandemic (accessed on 30 August 2021).
- Tsai, H.-J.; Chang, Y.-L.; Chen, F.-M. The Feasibility and Necessity of Cancer Screening Events in the Community during the COVID-19 Pandemic in Taiwan. J. Med. Screen 2021, 28, 55–56. [Google Scholar] [CrossRef] [PubMed]
- Routine Chronic Disease Screenings and Oncology Biomarker Tests Plummet During COVID-19. Available online: https://www.komodohealth.com/insights/2020/04/routine-chronic-disease-screenings-and-oncology-biomarker-tests-plummet-during-covid-19 (accessed on 30 August 2021).
- Vigliar, E.; Iaccarino, A.; Bruzzese, D.; Malapelle, U.; Bellevicine, C.; Troncone, G. Cytology in the Time of Coronavirus Disease (COVID-19): An Italian Perspective. J. Clin. Pathol. 2021, 74, 261–263. [Google Scholar] [CrossRef] [Green Version]












{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Anti-Ki67 1 |
| Dako |
| MIB-1 |
| Ethylenediaminetetraacetic acid (EDTA), pH9 |
| Monoclonal mouse anti-human Ki67 |
| 1:50 |
| Cells in the division in G1, S, G2 and M phase |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Istrate-Ofițeru, A.-M.; Berbecaru, E.-I.-A.; Ruican, D.; Nagy, R.D.; Rămescu, C.; Roșu, G.-C.; Iovan, L.; Dîră, L.M.; Zorilă, G.-L.; Țieranu, M.-L.; et al. The Influence of SARS-CoV-2 Pandemic in the Diagnosis and Treatment of Cervical Dysplasia. Medicina 2021, 57, 1101. https://doi.org/10.3390/medicina57101101
Istrate-Ofițeru A-M, Berbecaru E-I-A, Ruican D, Nagy RD, Rămescu C, Roșu G-C, Iovan L, Dîră LM, Zorilă G-L, Țieranu M-L, et al. The Influence of SARS-CoV-2 Pandemic in the Diagnosis and Treatment of Cervical Dysplasia. Medicina. 2021; 57(10):1101. https://doi.org/10.3390/medicina57101101
Chicago/Turabian StyleIstrate-Ofițeru, Anca-Maria, Elena-Iuliana-Anamaria Berbecaru, Dan Ruican, Rodica Daniela Nagy, Cătălina Rămescu, Gabriela-Camelia Roșu, Larisa Iovan, Laurențiu Mihai Dîră, George-Lucian Zorilă, Maria-Loredana Țieranu, and et al. 2021. "The Influence of SARS-CoV-2 Pandemic in the Diagnosis and Treatment of Cervical Dysplasia" Medicina 57, no. 10: 1101. https://doi.org/10.3390/medicina57101101