
Comparison of Immunogenicity and Reactogenicity of Five Primary Series of COVID-19 Vaccine Regimens against Circulating SARS-CoV-2 Variants of Concern among Healthy Thai Populations

 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Study Population
2.2. Vaccination Schedule and Vaccine Administration
2.3. Data Collection and Safety Assessment
2.4. Blood Collection
2.5. Serological Testing
2.5.1. Chemiluminescent Microparticle Immunoassay for Wild-Type SARS-CoV-2 RBD IgG Antibody
2.5.2. Surrogate Virus Neutralization Test for Wild-Type SARS-CoV-2
2.5.3. In-House Surrogate Virus Neutralization Test for SARS-CoV-2 Variants of Concern
2.6. Statistical Analysis
3. Results
3.1. Participant Characteristics
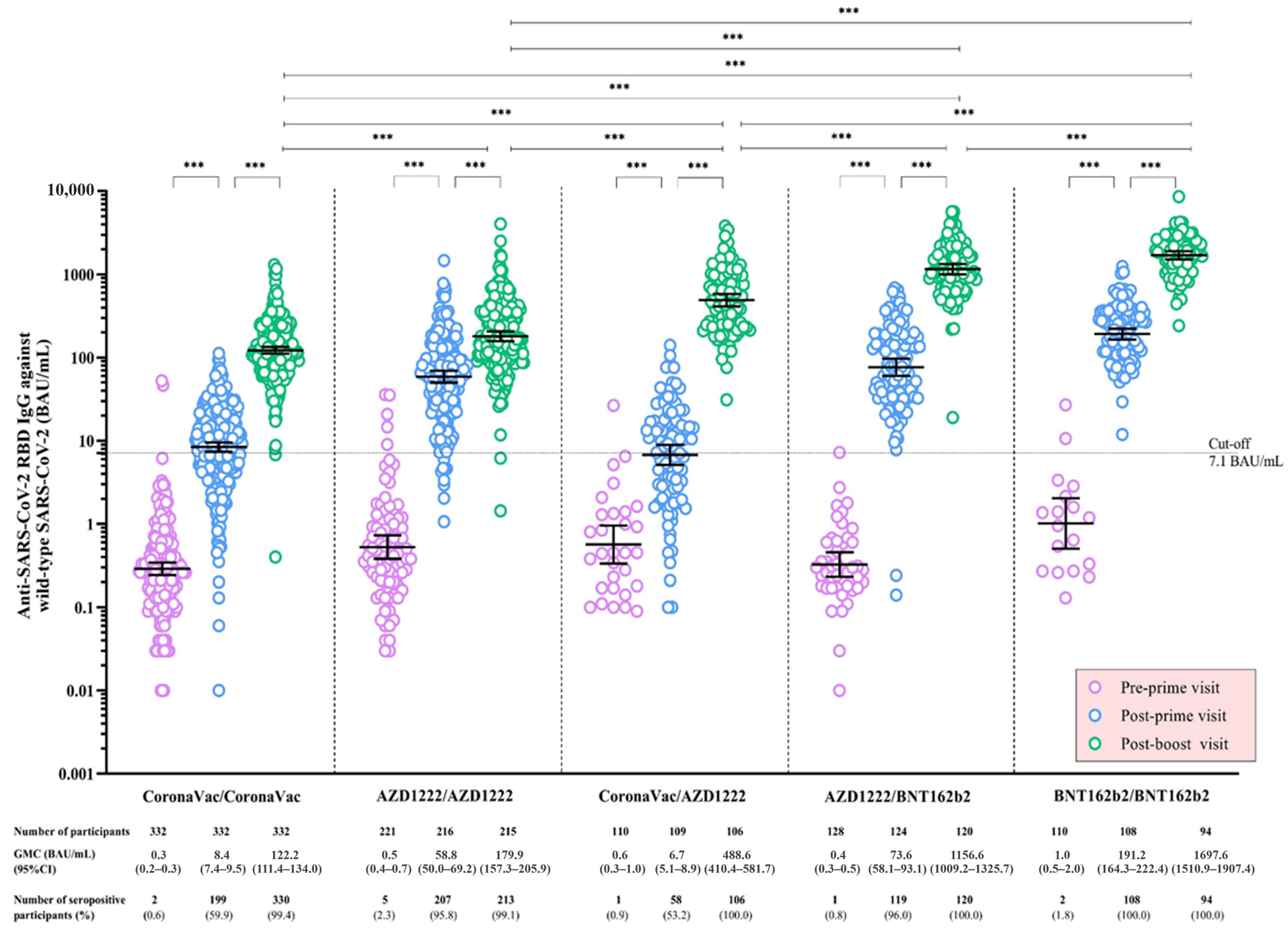
3.2. Anti-SARS-CoV-2 RBD IgG against Wild-Type SARS-CoV-2 Following a Primary Series of COVID-19 Vaccination
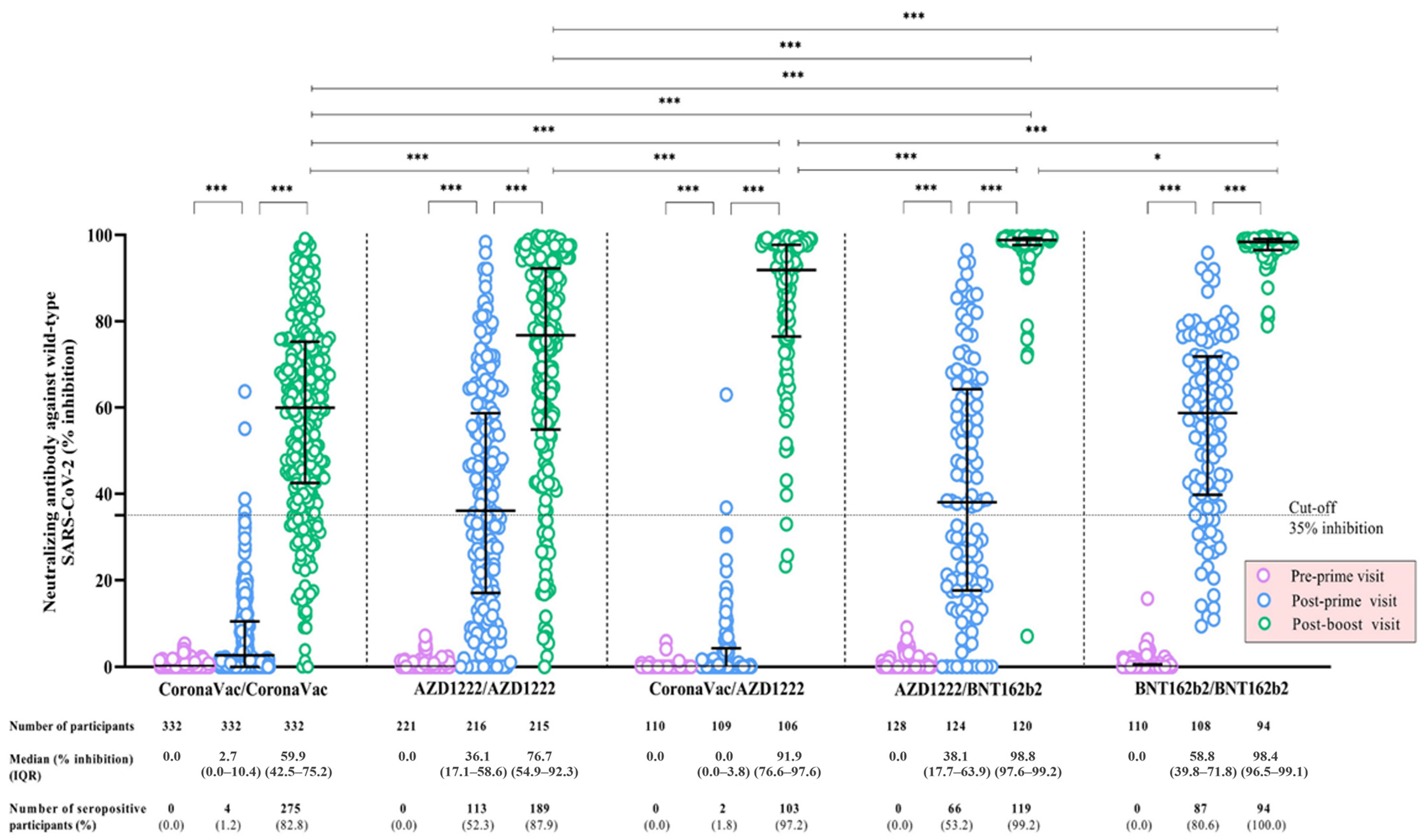
3.3. Neutralizing Antibody against Wild-Type SARS-CoV-2 Following a Primary Series of COVID-19 Vaccination
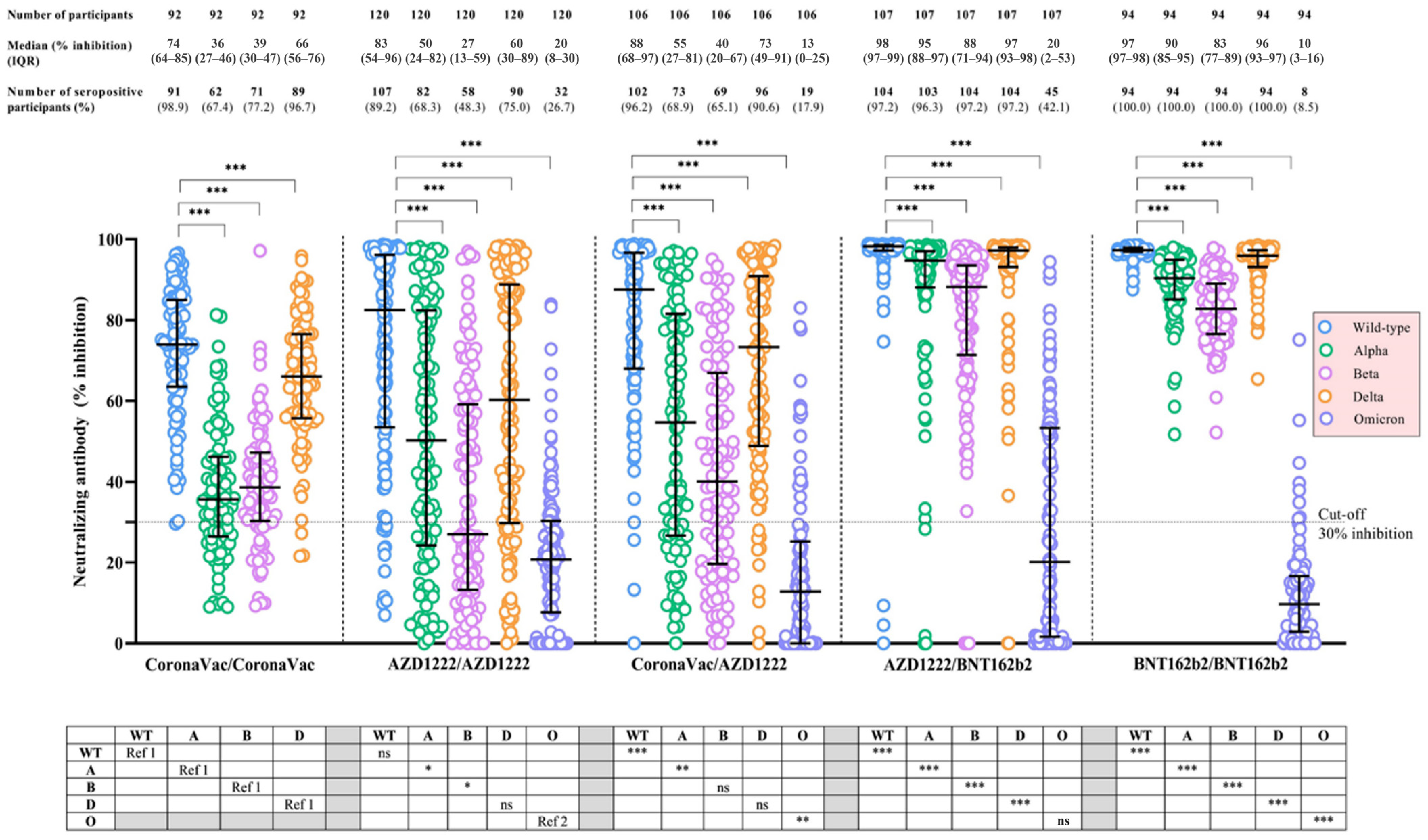
3.4. Neutralizing Antibody against SARS-CoV-2 Variants of Concern Following Completion of a Primary Series of COVID-19 Vaccination
3.5. Adverse Events Following a Primary Series of COVID-19 Vaccination
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Zheng, C.; Shao, W.; Chen, X.; Zhang, B.; Wang, G.; Zhang, W. Real-world effectiveness of COVID-19 vaccines: A literature review and meta-analysis. Int. J. Infect. Dis. 2022, 114, 252–260. [Google Scholar] [CrossRef] [PubMed]
- Liu, H.; Zhang, J.; Cai, J.; Deng, X.; Peng, C.; Chen, X.; Yang, J.; Wu, Q.; Chen, X.; Chen, Z.; et al. Herd immunity induced by COVID-19 vaccination programs and suppression of epidemics caused by the SARS-CoV-2 Delta variant in China. medRxiv 2021. [Google Scholar] [CrossRef]
- MacIntyre, C.R.; Costantino, V.; Trent, M. Modelling of COVID-19 vaccination strategies and herd immunity, in scenarios of limited and full vaccine supply in NSW, Australia. Vaccine 2022, 40, 2506–2513. [Google Scholar] [CrossRef] [PubMed]
- Basta, N.E.; Moodie, E.M.M.; the VIPER (Vaccines, Infectious disease Prevention, and Epidemiology Research) Group COVID-19 Vaccine Development and Approvals Tracker Team. COVID-19 Vaccine Development and Approvals Tracker. Available online: https://covid19.trackvaccines.org/vaccines/approved/ (accessed on 5 February 2023).
- Our World in Data. Coronavirus (COVID-19) Vaccinations. Available online: https://ourworldindata.org/covid-vaccinations (accessed on 5 February 2023).
- Borobia, A.M.; Carcas, A.J.; Pérez-Olmeda, M.; Castaño, L.; Bertran, M.J.; García-Pérez, J.; Campins, M.; Portolés, A.; González-Pérez, M.; Morales, M.T.G.; et al. Immunogenicity and reactogenicity of BNT162b2 booster in ChAdOx1-S-primed participants (CombiVacS): A multicentre, open-label, randomised, controlled, phase 2 trial. Lancet 2021, 398, 121–130. [Google Scholar] [CrossRef] [PubMed]
- Liu, X.; Shaw, R.H.; Stuart, A.S.V.; Greenland, M.; Aley, P.K.; Andrews, N.J.; Cameron, J.C.; Charlton, S.; Clutterbuck, E.A.; Collins, A.M.; et al. Safety and immunogenicity of heterologous versus homologous prime-boost schedules with an adenoviral vectored and mRNA COVID-19 vaccine (Com-COV): A single-blind, randomised, non-inferiority trial. Lancet 2021, 398, 856–869. [Google Scholar] [CrossRef] [PubMed]
- Atmar, R.L.; Lyke, K.E.; Deming, M.E.; Jackson, L.A.; Branche, A.R.; El Sahly, H.M.; Rostad, C.A.; Martin, J.M.; Johnston, C.; Rupp, R.E.; et al. Heterologous SARS-CoV-2 booster vaccinations—Preliminary report. medRxiv 2021. [Google Scholar] [CrossRef]
- Gilbert, P.B.; Montefiori, D.C.; McDermott, A.B.; Fong, Y.; Benkeser, D.; Deng, W.; Zhou, H.; Houchens, C.R.; Martins, K.; Jayashankar, L.; et al. Immune correlates analysis of the mRNA-1273 COVID-19 vaccine efficacy clinical trial. Science 2022, 375, 43–50. [Google Scholar] [CrossRef]
- Khoury, D.S.; Cromer, D.; Reynaldi, A.; Schlub, T.E.; Wheatley, A.K.; Juno, J.A.; Subbarao, K.; Kent, S.J.; Triccas, J.A.; Davenport, M.P. Neutralizing antibody levels are highly predictive of immune protection from symptomatic SARS-CoV-2 infection. Nat. Med. 2021, 27, 1205–1211. [Google Scholar] [CrossRef]
- Zhang, Z.; Mateus, J.; Coelho, C.H.; Dan, J.M.; Moderbacher, C.R.; Gálvez, R.I.; Cortes, F.H.; Grifoni, A.; Tarke, A.; Chang, J.; et al. Humoral and cellular immune memory to four COVID-19 vaccines. Cell 2022, 185, 2434–2451.e17. [Google Scholar] [CrossRef]
- Dodd, R.H.; Pickles, K.; Nickel, B.; Cvejic, E.; Ayre, J.; Batcup, C.; Bonner, C.; Copp, T.; Cornell, S.; Dakin, T.; et al. Concerns and motivations about COVID-19 vaccination. Lancet Infect. Dis. 2021, 21, 161–163. [Google Scholar] [CrossRef]
- Department of Disease Control, Ministry of Public Health. Guidelines for COVID-19 Vaccination in Thailand. Available online: https://ddc.moph.go.th/vaccine-covid19/guidelines (accessed on 5 February 2023).
- Department of Disease Control, Ministry of Public Health. Daily Report of COVID-19 Vaccine in Thailand. Available online: https://ddc.moph.go.th/vaccine-covid19/diaryReport (accessed on 5 February 2023).
- World Health Organization. WHO Coronavirus (COVID-19) Dashboard—Thailand. Available online: https://covid19.who.int/region/searo/country/th (accessed on 18 February 2023).
- Tan, C.W.; Chia, W.N.; Qin, X.; Liu, P.; Chen, M.I.C.; Tiu, C.; Hu, Z.; Chen, V.C.W.; Young, B.E.; Sia, W.R.; et al. A SARS-CoV-2 surrogate virus neutralization test based on antibody-mediated blockage of ACE2-spike protein-protein interaction. Nat. Biotechnol. 2020, 38, 1073–1078. [Google Scholar] [CrossRef]
- Barin, B.; Kasap, U.; Selçuk, F.; Volkan, E.; Uluçkan, Ö. Comparison of SARS-CoV-2 anti-spike receptor binding domain IgG antibody responses after CoronaVac, BNT162b2, ChAdOx1 COVID-19 vaccines, and a single booster dose: A prospective, longitudinal population-based study. Lancet Microbe 2022, 3, e274–e283. [Google Scholar] [CrossRef] [PubMed]
- Schmidt, T.; Klemis, V.; Schub, D.; Mihm, J.; Hielscher, F.; Marx, S.; Abu-Omar, A.; Ziegler, L.; Guckelmus, C.; Urschel, R.; et al. Immunogenicity and reactogenicity of heterologous ChAdOx1 nCoV-19/mRNA vaccination. Nat. Med. 2021, 27, 1530–1535. [Google Scholar] [CrossRef] [PubMed]
- Mahasirimongkol, S.; Khunphon, A.; Kwangsukstid, O.; Sapsutthipas, S.; Wichaidit, M.; Rojanawiwat, A.; Wichuckchinda, N.; Puangtubtim, W.; Pimpapai, W.; Soonthorncharttrawat, S.; et al. The pilot study of immunogenicity and adverse events of a COVID-19 vaccine regimen: Priming with inactivated whole SARS-CoV-2 vaccine (CoronaVac) and boosting with the adenoviral vector (ChAdOx1 nCoV-19) vaccine. Vaccines 2022, 10, 536. [Google Scholar] [CrossRef] [PubMed]
- Wanlapakorn, N.; Suntronwong, N.; Phowatthanasathian, H.; Yorsaeng, R.; Vichaiwattana, P.; Thongmee, T.; Auphimai, C.; Srimuan, D.; Thatsanatorn, T.; Assawakosri, S.; et al. Safety and immunogenicity of heterologous and homologous inactivated and adenoviral-vectored COVID-19 vaccine regimens in healthy adults: A prospective cohort study. Hum. Vaccines Immunother. 2022, 18, 2029111. [Google Scholar] [CrossRef]
- Barros-Martins, J.; Hammerschmidt, S.I.; Cossmann, A.; Odak, I.; Stankov, M.V.; Ramos, G.M.; Dopfer-Jablonka, A.; Heidemann, A.; Ritter, C.; Friedrichsen, M.; et al. Immune responses against SARS-CoV-2 variants after heterologous and homologous ChAdOx1 nCoV-19/BNT162b2 vaccination. Nat. Med. 2021, 27, 1525–1529. [Google Scholar] [CrossRef] [PubMed]
- Pozzetto, B.; Legros, V.; Djebali, S.; Barateau, V.; Guibert, N.; Villard, M.; Peyrot, L.; Allatif, O.; Fassier, J.B.; Massardier-Pilonchéry, A.; et al. Immunogenicity and efficacy of heterologous ChAdOx1-BNT162b2 vaccination. Nature 2021, 600, 701–706. [Google Scholar] [CrossRef]
- Kardani, K.; Bolhassani, A.; Shahbazi, S. Prime-boost vaccine strategy against viral infections: Mechanisms and benefits. Vaccine 2016, 34, 413–423. [Google Scholar] [CrossRef]
- Kunal, S.; Sakthivel, P.; Gupta, N.; Ish, P. Mix and match COVID-19 vaccines: Potential benefit and perspective from India. Postgrad. Med. J. 2021, 98, e99–e101. [Google Scholar] [CrossRef]
- Mistry, P.; Barmania, F.; Mellet, J.; Peta, K.; Strydom, A.; Viljoen, I.M.; James, W.; Gordon, S.; Pepper, M.S. SARS-CoV-2 Variants, Vaccines, and Host Immunity. Front. Immunol. 2022, 12, 809244. [Google Scholar] [CrossRef]
- Ao, D.; Lan, T.; He, X.; Liu, J.; Chen, L.; Baptista-Hon, D.T.; Zhang, K.; Wei, X. SARS-CoV-2 Omicron variant: Immune escape and vaccine development. MedComm 2022, 3, e126. [Google Scholar] [CrossRef] [PubMed]
- Cheng, S.M.S.; Mok, C.K.P.; Leung, Y.W.Y.; Ng, S.S.; Chan, K.C.K.; Ko, F.W.; Chen, C.; Yiu, K.; Lam, B.H.S.; Lau, E.H.Y.; et al. Neutralizing antibodies against the SARS-CoV-2 Omicron variant BA.1 following homologous and heterologous CoronaVac or BNT162b2 vaccination. Nat. Med. 2022, 28, 486–489. [Google Scholar] [CrossRef] [PubMed]
- Niyomnaitham, S.; Toh, Z.Q.; Wongprompitak, P.; Jansarikit, L.; Srisutthisamphan, K.; Sapsutthipas, S.; Jantraphakorn, Y.; Mingngamsup, N.; Licciardi, P.V.; Chokephaibulkit, K. Immunogenicity and reactogenicity against the SARS-CoV-2 variants following heterologous primary series involving CoronaVac, ChAdox1 nCov-19 and BNT162b2 plus BNT162b2 booster vaccination: An open-label randomized study in healthy Thai adults. Hum. Vaccines Immunother. 2022, 18, 2091865. [Google Scholar] [CrossRef]
- Pascuale, C.A.; Varese, A.; Ojeda, D.S.; Pasinovich, M.E.; Lopez, L.; Rossi, A.H.; Rodriguez, P.E.; Miglietta, E.A.; Group, L.S.; Mazzitelli, I.; et al. Immunogenicity and reactogenicity of heterologous immunization against SARS CoV-2 using Sputnik V, ChAdOx1-S, BBIBP-CorV, Ad5-nCoV, and mRNA-1273. Cell Rep. Med. 2022, 3, 100706. [Google Scholar] [CrossRef]
- Chalkias, S.; Harper, C.; Vrbicky, K.; Walsh, S.R.; Essink, B.; Brosz, A.; McGhee, N.; Tomassini, J.E.; Chen, X.; Chang, Y.; et al. A bivalent Omicron-containing booster vaccine against Covid-19. N. Engl. J. Med. 2022, 387, 1279–1291. [Google Scholar] [CrossRef] [PubMed]
- Asano, M.; Okada, H.; Itoh, Y.; Hirata, H.; Ishikawa, K.; Yoshida, E.; Matsui, A.; Kelly, E.J.; Shoemaker, K.; Olsson, U.; et al. Immunogenicity and safety of AZD1222 (ChAdOx1 nCoV-19) against SARS-CoV-2 in Japan: A double-blind, randomized controlled phase 1/2 trial. Int. J. Infect. Dis. 2022, 114, 165–174. [Google Scholar] [CrossRef]
- Müller, L.; Andrée, M.; Moskorz, W.; Drexler, I.; Walotka, L.; Grothmann, R.; Ptok, J.; Hillebrandt, J.; Ritchie, A.; Rabl, D.; et al. Age-dependent immune response to the Biontech/Pfizer BNT162b2 coronavirus disease 2019 vaccination. Clin. Infect. Dis. 2021, 73, 2065–2072. [Google Scholar] [CrossRef]
- Kang, Y.M.; Minn, D.; Lim, J.; Lee, K.D.; Jo, D.H.; Choe, K.W.; Kim, M.J.; Kim, J.M.; Kim, K.N. Comparison of antibody response elicited by ChAdOx1 and BNT162b2 COVID-19 vaccine. J. Korean Med. Sci. 2021, 36, e311. [Google Scholar] [CrossRef] [PubMed]
- Gruver, A.L.; Hudson, L.L.; Sempowski, G.D. Immunosenescence of ageing. J. Pathol. 2007, 211, 144–156. [Google Scholar] [CrossRef]
- Kadali, R.A.K.; Janagama, R.; Peruru, S.; Malayala, S.V. Side effects of BNT162b2 mRNA COVID-19 vaccine: A randomized, cross-sectional study with detailed self-reported symptoms from healthcare workers. Int. J. Infect. Dis. 2021, 106, 376–381. [Google Scholar] [CrossRef]
- Folegatti, P.M.; Ewer, K.J.; Aley, P.K.; Angus, B.; Becker, S.; Belij-Rammerstorfer, S.; Bellamy, D.; Bibi, S.; Bittaye, M.; Clutterbuck, E.A.; et al. Safety and immunogenicity of the ChAdOx1 nCoV-19 vaccine against SARS-CoV-2: A preliminary report of a phase 1/2, single-blind, randomised controlled trial. Lancet 2020, 396, 467–478. [Google Scholar] [CrossRef] [PubMed]
- Tomita, K.; Okada, S.; Sugihara, S.; Ikeuchi, T.; Touge, H.; Hasegawa, J.; Yamasaki, A. Physical characteristics of injection site pain after COVID-19 mRNA BNT162b2 vaccination. Yonago Acta Med. 2021, 64, 339–444. [Google Scholar] [CrossRef] [PubMed]
- Hervé, C.; Laupèze, B.; Giudice, G.D.; Didierlaurent, A.M.; Silva, F.T.D. The how’s and what’s of vaccine reactogenicity. NPJ Vaccines 2019, 4, 39. [Google Scholar] [CrossRef] [PubMed] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Characteristics a | CoronaVac/ CoronaVac | AZD1222/ AZD1222 | CoronaVac/ AZD1222 | AZD1222/ BNT162b2 | BNT162b2/ BNT162b2 | P b |
|---|---|---|---|---|---|---|
| Number of enrolled participants | 332 | 221 | 110 | 128 | 110 | |
| Age, years | 39.0 (30.0–48.0) | 62.6 (52.3–68.3) | 59.8 (44.0–65.2) | 52.3 (30.7–67.5) | 28.7 (22.8–36.9) | <0.001 |
| Age category | <0.001 | |||||
| <60 years | 332 (100) | 73 (33.0) | 55 (50.0) | 73 (57.0) | 110 (100) | |
| ≥60 years | 0 (0) | 148 (67.0) | 55 (50.0) | 55 (43.0) | 0 (0) | |
| Sex | 0.003 | |||||
| Male | 90 (27.1) | 81 (36.7) | 48 (43.6) | 44 (34.4) | 27 (24.6) | |
| Female | 242 (72.9) | 140 (63.3) | 62 (56.4) | 84 (65.6) | 83 (75.4) | |
| Body mass index, kg/m2 | 23.1 (20.9–26.0) | 24.7 (22.0–27.3) | 27.4 (23.7–35.0) | 23.2 (20.3–26.2) | 22.5 (19.8–26.6) | <0.001 |
| Body mass index category | <0.001 | |||||
| Underweight | 20 (6.0) | 10 (4.5) | 2 (1.8) | 8 (6.3) | 14 (12.7) | |
| Normal weight | 201 (60.6) | 108 (48.9) | 40 (36.4) | 78 (60.9) | 56 (50.9) | |
| Overweight | 80 (24.1) | 75 (33.9) | 36 (32.7) | 34 (26.6) | 28 (25.5) | |
| Obese | 31 (9.3) | 28 (12.7) | 32 (29.1) | 8 (6.2) | 12 (10.9) | |
| Cigarette smoking | <0.001 | |||||
| Never smoked | 326 (98.2) | 197 (89.1) | 88 (80.0) | 120 (93.8) | 103 (93.6) | |
| Ever smoked (current and former) | 6 (1.8) | 24 (10.9) | 22 (20.0) | 8 (6.2) | 7 (6.4) | |
| Alcohol consumption | <0.001 | |||||
| Never drunk | 287 (86.5) | 168 (76.0) | 71 (64.6) | 100 (78.1) | 87 (79.1) | |
| Ever drunk (current and former) | 45 (13.5) | 53 (24.0) | 39 (35.4) | 28 (21.9) | 23 (20.9) |
| Study Participant and Study Visit | CoronaVac/CoronaVac | AZD1222/AZD1222 | CoronaVac/AZD1222 | AZD1222/BNT162b2 | BNT162b2/BNT162b2 | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| GMC of Anti- RBD-WT IgG (95% CI, BAU/mL) | GMR a (95% CI) | P a | GMC of Anti- RBD-WT IgG (95% CI, BAU/mL) | GMR a (95% CI) | P a | GMC of Anti- RBD-WT IgG (95% CI, BAU/mL) | GMR a (95% CI) | P a | GMC of Anti- RBD-WT IgG (95% CI, BAU/mL) | GMR a (95% CI) | P a | GMC of Anti- RBD-WT IgG (95% CI, BAU/mL) | GMR a (95% CI) | P a | |
| All participants | |||||||||||||||
| Pre-prime visit | 0.3 (0.2–0.3) | 0.5 (0.4–0.7) | 0.6 (0.3–1.0) | 0.4 (0.3–0.5) | 1.0 (0.5–2.0) | ||||||||||
| Post-prime visit | 8.4 (7.4–9.5) | 29.1 (23.9–35.4) | <0.001 | 58.8 (50.0–69.2) | 114.1 (82.9–157.1) | <0.001 | 6.7 (5.1–8.9) | 12.5 (7.6–20.6) | <0.001 | 73.6 (58.1–93.1) | 211.0 (138.0–322.6) | <0.001 | 191.2 (164.3–222.4) | 193.9 (122.7–306.4) | <0.001 |
| Post-boost visit | 122.2 (111.4–134.0) | 14.7 (13.1–16.6) | <0.001 | 179.9 * (157.3–205.9) | 3.0 (2.6–3.6) | <0.001 | 488.6 * (410.4–581.7) | 74.8 (61.3–91.3) | <0.001 | 1156.6 * (1009.2–1325.7) | 15.9 (13.2–19.1) | <0.001 | 1697.6 * (1510.9–1907.4) | 9.0 (8.1–10.1) | <0.001 |
| Adults aged < 60 years old | |||||||||||||||
| Pre-prime visit | 0.3 (0.2–0.3) | 0.6 (0.3–1.0) | 0.8 (0.4–1.8) | 0.3 (0.2–0.4) | 1.0 (0.5–2.0) | ||||||||||
| Post-prime visit | 8.4 (7.4–9.5) | 29.1 (23.9–35.4) | <0.001 | 72.6 (54.6–96.5) | 131.3 (80.5–214.2) | <0.001 | 9.7 (6.9–13.7) | 11.7 (5.5–24.9) | <0.001 | 100.3 (79.9–125.9) | 330.0 (224.5–485.1) | <0.001 | 191.2 (164.3–222.4) | 193.9 (122.7–306.4) | <0.001 |
| Post-boost visit | 122.2 (111.4–134.0) | 14.7 (13.1–16.6) | <0.001 | 258.3 * (207.2–321.8) | 3.5 (2.6–4.8) | <0.001 | 566.4 * (435.0–737.6) | 58.5 (46.4–73.8) | <0.001 | 1279.1 * (1111.8–1471.5) | 12.8 (83.4–15.4) | <0.001 | 1697.6 * (1510.9–1907.4) | 9.0 (8.1–10.1) | <0.001 |
| Elderly aged ≥ 60 years old | |||||||||||||||
| Pre-prime visit | - | - | - | 0.5 (0.3–0.7) | 0.4 (0.2–0.9) | 1.1 (0.4–3.2) | - | - | - | ||||||
| Post-prime visit | - | - | - | 53.0 (43.5–64.5) | 109.5 (72.3–165.8) | <0.001 | 4.6 (3.0–7.1) | 10.0 (5.5–18.3) | <0.001 | 46.6 (29.3–73.4) | 90.7 (35.6–231.1) | <0.001 | - | - | - |
| Post-boost visit | - | - | - | 150.0 (127.4–176.6) | 2.8 (2.3–3.4) | <0.001 | 421.4 † (335.0–530.1) | 96.6 (80.9–131.6) | <0.001 | 989.3 † (752.6–1300.5) | 22.4 (15.7–31.9) | <0.001 | - | - | - |
| Study Participant and Study Visit | CoronaVac/CoronaVac | AZD1222/AZD1222 | CoronaVac/AZD1222 | AZD1222/BNT162b2 | BNT162b2/BNT162b2 | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Median of NAb-WT (IQR, % Inhibition) | Median Difference a (IQR, % Inhibition) | P a | Median of NAb-WT (IQR, % Inhibition) | Median Difference a (IQR, % Inhibition) | P a | Median of NAb-WT (IQR, % Inhibition) | Median Difference a (IQR, % Inhibition) | P a | Median of NAb-WT (IQR, % Inhibition) | Median Difference a (IQR, % Inhibition) | P a | Median of NAb-WT (IQR, % Inhibition) | Median Difference a (IQR, % Inhibition) | P a | |
| All participants | |||||||||||||||
| Pre-prime visit | 0 | 0 | 0 | 0 | 0 | ||||||||||
| Post-prime visit | 2.7 (0–10.4) | 2.4 (0–10.3) | <0.001 | 36.1 (16.6–58.6) | 36.1 (36.1–58.2) | <0.001 | 0 (0.0–3.8) | 0 (0–3.8) | <0.001 | 38.1 (17.7–63.9) | 37.6 (17.4–62.8) | <0.001 | 58.8 (39.8–71.8) | 58.8 (37.5–71.8) | <0.001 |
| Post-boost visit | 59.9 (42.5–75.2) | 51.6 (35.6–68.3) | <0.001 | 76.7 * (54.9–92.3) | 31.7 (9.5–53.3) | <0.001 | 91.9 * (76.6–97.6) | 85.9 (72.3–93.4) | <0.001 | 98.8 * (97.6–99.2) | 59.4 (33.4–77.1) | <0.001 | 98.4 * (96.5–99.1) | 40.5 (26.8–58.4) | <0.001 |
| Adults aged < 60 years old | |||||||||||||||
| Pre-prime visit | 0 | 0 | 0 | 0 | 0 | ||||||||||
| Post-prime visit | 2.7 (0–10.4) | 2.4 (0–10.3) | <0.001 | 45.6 (19.9–64.7) | 43.8 (17.2–64.7) | <0.001 | 0 (0–4.9) | 0 (0–4.9) | <0.001 | 47.0 (27.5–68.2) | 45.8 (26.8–68.2) | <0.001 | 58.8 (39.8–71.8) | 58.8 (37.5–71.8) | <0.001 |
| Post-boost visit | 59.9 (42.5–75.2) | 51.6 (35.6–68.3) | <0.001 | 85.4 * (67.0–94.7) | 33.1 (12.7–60.5) | <0.001 | 94.0 * (83.5–98.6) | 86.4 (77.9–94.0) | <0.001 | 99.1 * (98.4–99.4) | 51.6 (30.9–69.0) | <0.001 | 98.4 * (96.5–99.1) | 40.5 (26.8–58.4) | <0.001 |
| Elderly aged ≥ 60 years old | |||||||||||||||
| Pre-prime visit | - | - | - | 0 | 0 | 0 | - | - | - | ||||||
| Post-prime visit | - | - | - | 34.7 (15.5–53.7) | 34.4 (15.5–53.5) | <0.001 | 0 (0.0–3.8) | 0 (0–3.8) | <0.001 | 19.9 (5.4–52.0) | 19.9 (5.4–52.0) | <0.001 | - | - | - |
| Post-boost visit | - | - | - | 73.3 (47.2–89.9) | 31.0 (9.1–52.5) | <0.001 | 89.9 † (70.2–95.0) | 81.2 (65.1–91.9) | <0.001 | 98.0 † (94.9–99.0) | 72.0 (39.2–80.8) | <0.001 | - | - | - |
| Study Participant and SARS-CoV-2 Variant | CoronaVac/CoronaVac | AZD1222/AZD1222 | CoronaVac/AZD1222 | AZD1222/BNT162b2 | BNT162b2/BNT162b2 | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Median of NAb-VoC (IQR, % Inhibition) | Median Difference a (IQR, % Inhibition) | P a | Median of NAb-VoC (IQR, % Inhibition) | Median Difference a (IQR, % Inhibition) | P a | Median of NAb-VoC (IQR, % Inhibition) | Median Difference a (IQR, % Inhibition) | P a | Median of NAb-VoC (IQR, % Inhibition) | Median Difference a (IQR, % Inhibition) | P a | Median of NAb-VoC (IQR, % Inhibition) | Median Difference a (IQR, % Inhibition) | P a | |
| All participants | |||||||||||||||
| Wild-type | 74.0 (63.6–85.0) | Ref | Ref | 82.5 (53.7–96.0) | Ref | Ref | 87.5 * (68.2–96.7) | Ref | Ref | 98.3 * (97.3–98.5) | Ref | Ref | 97.3 * (96.9–97.9) | Ref | Ref |
| Alpha | 35.6 (26.6–46.1) | −35.4 (−39.8 to –31.1) | <0.001 | 50.3 * (24.3–82.3) | -19.8 (−32.0 to –9.6) | <0.001 | 54.6 * (26.7–81.4) | −25.0 (−41.6 to–12.6) | <0.001 | 94.7 * (88.1–97.1) | −3.2 (−7.9 to –1.4) | <0.001 | 90.4 * (85.2–94.9) | −6.8 (−11.8 to –3.2) | <0.001 |
| Beta | 38.6 (30.4–47.0) | −34.2 (−41.2 to –24.7) | <0.001 | 27.0 * (13.4–58.8) | −35.5 (−47.9 to –22.5) | <0.001 | 40.1 (19.6–66.5) | −38.4 (−49.1 to 22.0) | <0.001 | 88.2* (71.4–93.5) | −9.8 (−22.9 to –4.5) | <0.001 | 82.8 * (76.6–88.8) | −14.1 (−20.4 to –8.6) | <0.001 |
| Delta | 66.1 (55.8–76.4) | −7.5 (−11.3 to –3.2) | <0.001 | 60.2 (29.9–88.5) | −11.4 (−23.9 to –3.9) | <0.001 | 73.3 (48.9–90.9) | −8.1 (−19.1 to –2.8) | <0.001 | 97.3 * (93.1–98.0) | −1.0 (−4.2 to –0.5) | <0.001 | 96.0 * (93.2–97.3) | −1.5 (−3.8 to –0.4) | <0.001 |
| Omicron | - | - | - | 20.4 (7.9–30.3) | −54.3 (−72.0 to –33.0) | <0.001 | 12.8 † (0–24.8) | −64.3 (−80.2 to –51.2) | <0.001 | 20.4 (1.6–53.3) | −74.7 (−92.9 to –44.0) | <0.001 | 9.7 † (3.0–16.3) | −86.4 (−94.0 to –80.7) | <0.001 |
| Adults aged < 60 years old | |||||||||||||||
| Wild-type | 74.0 (63.6–85.0) | −35.4 (−39.8 to –31.1) | <0.001 | 90.7 * (63.8–97.5) | Ref | Ref | 93.8 * (69.3–97.9) | Ref | Ref | 98.5 * (98.2–98.6) | Ref | Ref | 97.3 * (96.9–97.9) | Ref | Ref |
| Alpha | 35.6 (26.6–46.1) | −34.2 (−−41.2 to –24.7) | <0.001 | 68.6 * (27.9–87.2) | −17.2 (−30.1 to –8.2) | <0.001 | 66.6 * (33.8–90.3) | −16.4 (−34.6 to –7.1) | <0.001 | 96.9 * (93.4–97.6) | −1.8 (−4.1 to –1.02) | <0.001 | 90.4 * (85.2–94.9) | −6.8 (−11.8 to –3.2) | <0.001 |
| Beta | 38.6 (30.4–47.0) | −7.5 (−11.3 to –3.2) | <0.001 | 48.5 (20.7–70.8) | −32.0 (−41.8 to –20.4) | <0.001 | 46.6 (27.1–70.9) | −32.2 (−49.0 to –16.0) | <0.001 | 91.5 * (82.1–95.5) | −6.6 (−12.7 to –3.2) | <0.001 | 82.8 * (76.6–88.8) | −14.1 (−20.4 to –8.6) | <0.001 |
| Delta | 66.1 (55.8–76.4) | −35.4 (−39.8 to –31.1) | <0.001 | 80.2 * (38.5–93.2) | −7.8 (−23.4 to –3.1) | <0.001 | 83.6 * (56.0–95.0) | −4.9 (−10.4 to –1.4) | <0.001 | 97.7 * (96.3–98.1) | −0.9 (−1.8 to –5.4) | <0.001 | 96.0 * (93.2–97.3) | −1.5 (−3.8 to –0.4) | <0.001 |
| Omicron | - | - | - | 21.1 (0.2–30.2) | −57.0 (−81.0 to –37.8) | <0.001 | 9.7 (0–26.3) | −65.4 (−82.3 to –51.9) | <0.001 | 51.5 † (25.1–61.6) | −45.8 (−69.2 to –34.7) | <0.001 | 9.7 † (3.0–16.3) | −86.4 (−94.0 to –80.7) | <0.001 |
| Elderly aged ≥ 60 years old | |||||||||||||||
| Wild-type | - | - | - | 74.9 (45.3–92.9) | Ref | Ref | 79.7 (67.2–93.6) | Ref | Ref | 98.0 † (96.3–98.3) | Ref | Ref | - | - | - |
| Alpha | - | - | - | 42.3 (14.8–66.9) | −24.8 (−32.7 to –11.6) | <0.001 | 38.6 (26.6–70.1) | −28.2 (−41.8 to –21.4) | <0.001 | 90.3 † (68.7–94.7) | −7.6 (−24.8 to –3.2) | <0.001 | - | - | - |
| Beta | - | - | - | 18.0 (7.9–44.0) | –39.6 (−54.2 to –29.0) | <0.001 | 34.3† (19.6–54.4) | −42.6 (−49.1 to –25.4) | <0.001 | 78.8 † (58.3–90.9) | −16.2 (−33.7 to –6.7) | <0.001 | - | - | - |
| Delta | - | - | - | 44.8 (28.2–83.9) | −13.9 (−25.7 to –6.2) | <0.001 | 59.8 (44.0–85.8) | −13.0 (−22.2 to –5.5) | <0.001 | 93.9 † (77.0–97.7) | −2.9 (−14.7 to –0.5) | <0.001 | - | - | - |
| Omicron | - | - | - | 20.6 (14.2–30.3) | −50.3 (−62.7 to –28.4) | <0.001 | 13.3 † (1.1–23.0) | −59.1 (−76.6 to –50.4) | <0.001 | 1.8 † (0–7.7) | −92.9 (−96.3 to –83.0) | <0.001 | - | - | - |
| Adverse Events a | CoronaVac/ CoronaVac | AZD1222/ AZD1222 | CoronaVac/ AZD1222 | AZD1222/ BNT162b2 | BNT162b2/ BNT162b2 | P b |
|---|---|---|---|---|---|---|
| First dose of vaccine | (n = 286) | (n = 221) | (n = 109) | (n = 100) | (n = 83) | |
| Overall adverse events | 164 (57.3) | 179 (81.0) | 62 (56.9) | 90 (90.0) | 78 (94.0) | <0.001 |
| Local adverse events | ||||||
| Pain | 116 (40.6) | 132 (59.7) | 28 (25.7) | 74 (74.0) | 77 (92.8) | <0.001 |
| Swelling | 6 (2.1) | 29 (13.1) | 3 (2.8) | 11 (11.0) | 18 (21.7) | <0.001 |
| Erythema | 4 (1.4) | 14 (6.3) | 5 (4.6) | 10 (10.0) | 4 (4.8) | 0.002 |
| Systemic adverse events | ||||||
| Fatigue | 87 (30.4) | 94 (42.5) | 41 (37.6) | 61 (61.0) | 33 (39.8) | <0.001 |
| Headache | 50 (17.5) | 72 (32.6) | 20 (18.4) | 43 (43.0) | 16 (19.3) | <0.001 |
| Fever | 11 (3.9) | 64 (29.0) | 13 (11.9) | 52 (52.0) | 14 (16.9) | <0.001 |
| Paresthesia | 10 (3.5) | 12 (5.4) | 6 (5.5) | 3 (3.0) | 2 (2.4) | 0.65 |
| Dizziness | 5 (1.8) | 7 (3.2) | 4 (3.7) | 5 (5.0) | 0 (0) | 0.16 |
| Second dose of vaccine | (n = 286) | (n = 209) | (n = 100) | (n = 120) | (n = 76) | |
| Overall adverse events | 164 (57.3) | 149 (71.3) | 76 (76.0) | 82 (68.3) | 73 (96.1) | <0.001 |
| Local adverse events | ||||||
| Pain | 139 (48.6) | 100 (47.9) | 60 (60.0) | 74 (61.7) | 71 (93.4) | <0.001 |
| Swelling | 7 (2.5) | 20 (9.6) | 14 (14.0) | 21 (17.5) | 27 (35.5) | <0.001 |
| Erythema | 4 (1.4) | 19 (9.1) | 5 (5.0) | 11 (9.2) | 11 (14.5) | <0.001 |
| Systemic adverse events | ||||||
| Fatigue | 77 (26.9) | 61 (29.2) | 45 (45.0) | 49 (40.8) | 32 (42.1) | 0.001 |
| Headache | 41 (14.3) | 53 (25.4) | 42 (42.0) | 27 (22.5) | 33 (43.4) | <0.001 |
| Fever | 11 (3.9) | 32 (15.3) | 41 (41.0) | 32 (26.7) | 24 (31.6) | <0.001 |
| Paresthesia | 12 (4.2) | 5 (2.4) | 8 (8.0) | 5 (4.2) | 2 (2.6) | 0.24 |
| Dizziness | 3 (1.1) | 6 (2.9) | 4 (4.0) | 1 (0.8) | 3 (4.0) | 0.14 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sudjaritruk, T.; Mueangmo, O.; Saheng, J.; Winichakoon, P.; Salee, P.; Wongjak, W.; Chaito, T.; Praparattanapan, J.; Nuket, K.; Solai, N.; et al. Comparison of Immunogenicity and Reactogenicity of Five Primary Series of COVID-19 Vaccine Regimens against Circulating SARS-CoV-2 Variants of Concern among Healthy Thai Populations. Vaccines 2023, 11, 564. https://doi.org/10.3390/vaccines11030564
Sudjaritruk T, Mueangmo O, Saheng J, Winichakoon P, Salee P, Wongjak W, Chaito T, Praparattanapan J, Nuket K, Solai N, et al. Comparison of Immunogenicity and Reactogenicity of Five Primary Series of COVID-19 Vaccine Regimens against Circulating SARS-CoV-2 Variants of Concern among Healthy Thai Populations. Vaccines. 2023; 11(3):564. https://doi.org/10.3390/vaccines11030564
Chicago/Turabian StyleSudjaritruk, Tavitiya, Oramai Mueangmo, Jutamad Saheng, Poramed Winichakoon, Parichat Salee, Worawan Wongjak, Tanachot Chaito, Jutarat Praparattanapan, Khanuengnit Nuket, Nuttarika Solai, and et al. 2023. "Comparison of Immunogenicity and Reactogenicity of Five Primary Series of COVID-19 Vaccine Regimens against Circulating SARS-CoV-2 Variants of Concern among Healthy Thai Populations" Vaccines 11, no. 3: 564. https://doi.org/10.3390/vaccines11030564