
Organizational and Personal Factors That Boost Innovation: The Case of Nurses during COVID-19 Pandemic Based on Job Demands-Resources Model


Abstract
:1. Introduction
2. Literature Review
2.1. Innovative Behaviour
2.2. Innovation Outputs
2.3. Stress and Anxiety
2.4. Work Engagement
2.5. Organizational Support
2.6. Job Demands-Resources Model
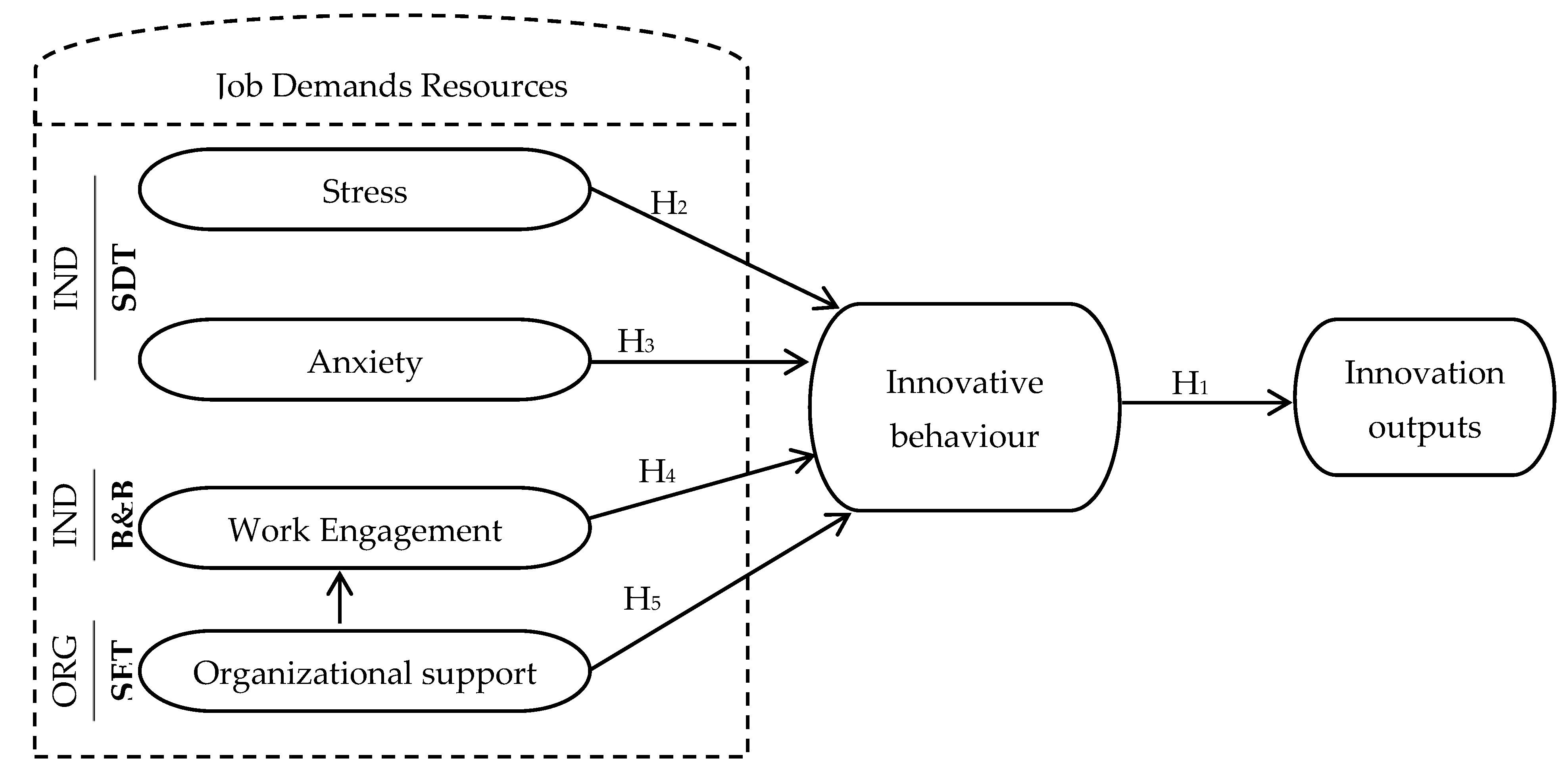
2.7. Conceptual Model
3. Methodology
3.1. Data and Sources
3.2. Methods and Techniques of Analysis
4. Presentation and Analysis of Results
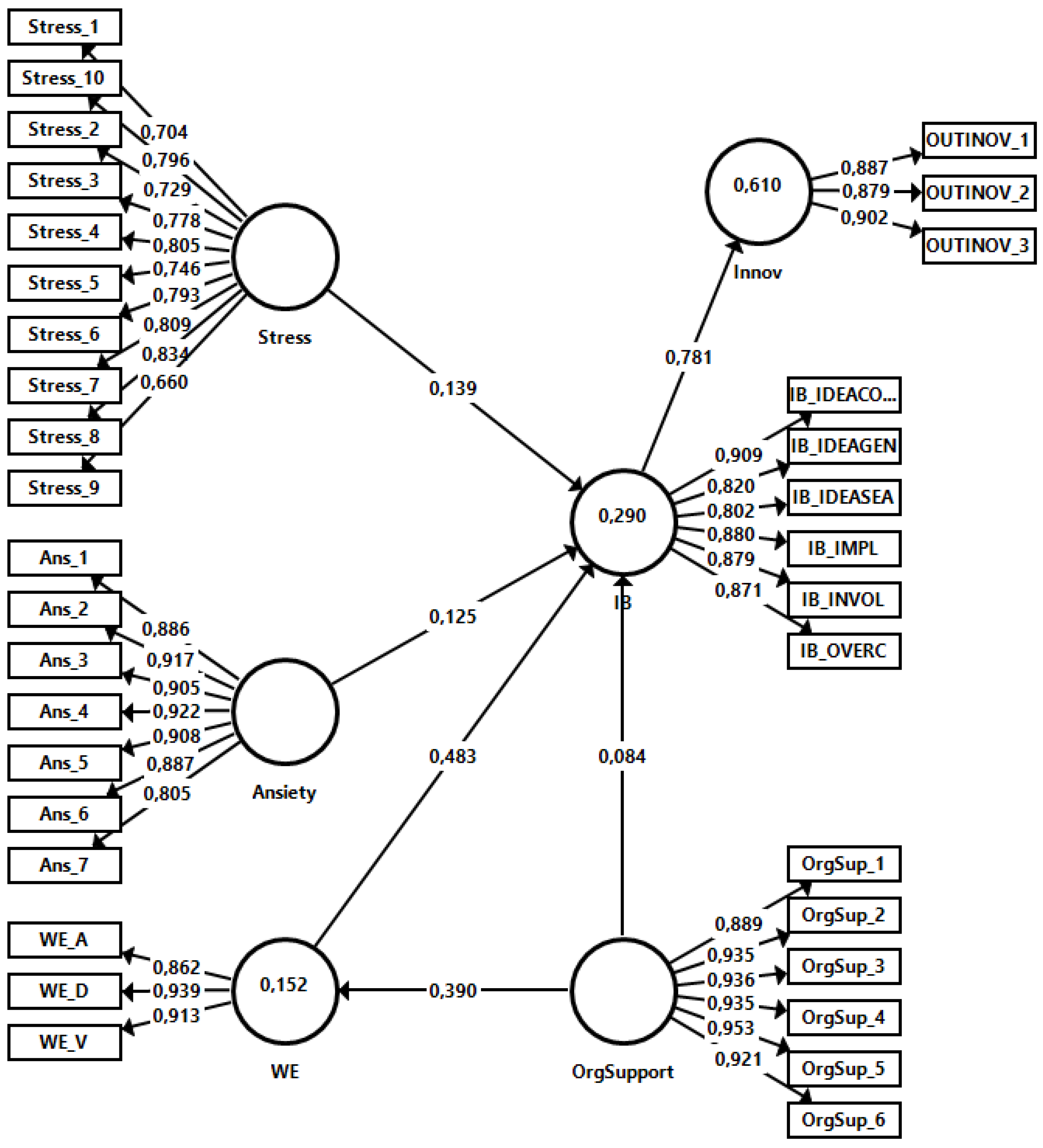
4.1. Evaluation of the Structural Equation Model
4.2. Measurement model (Outer Model)
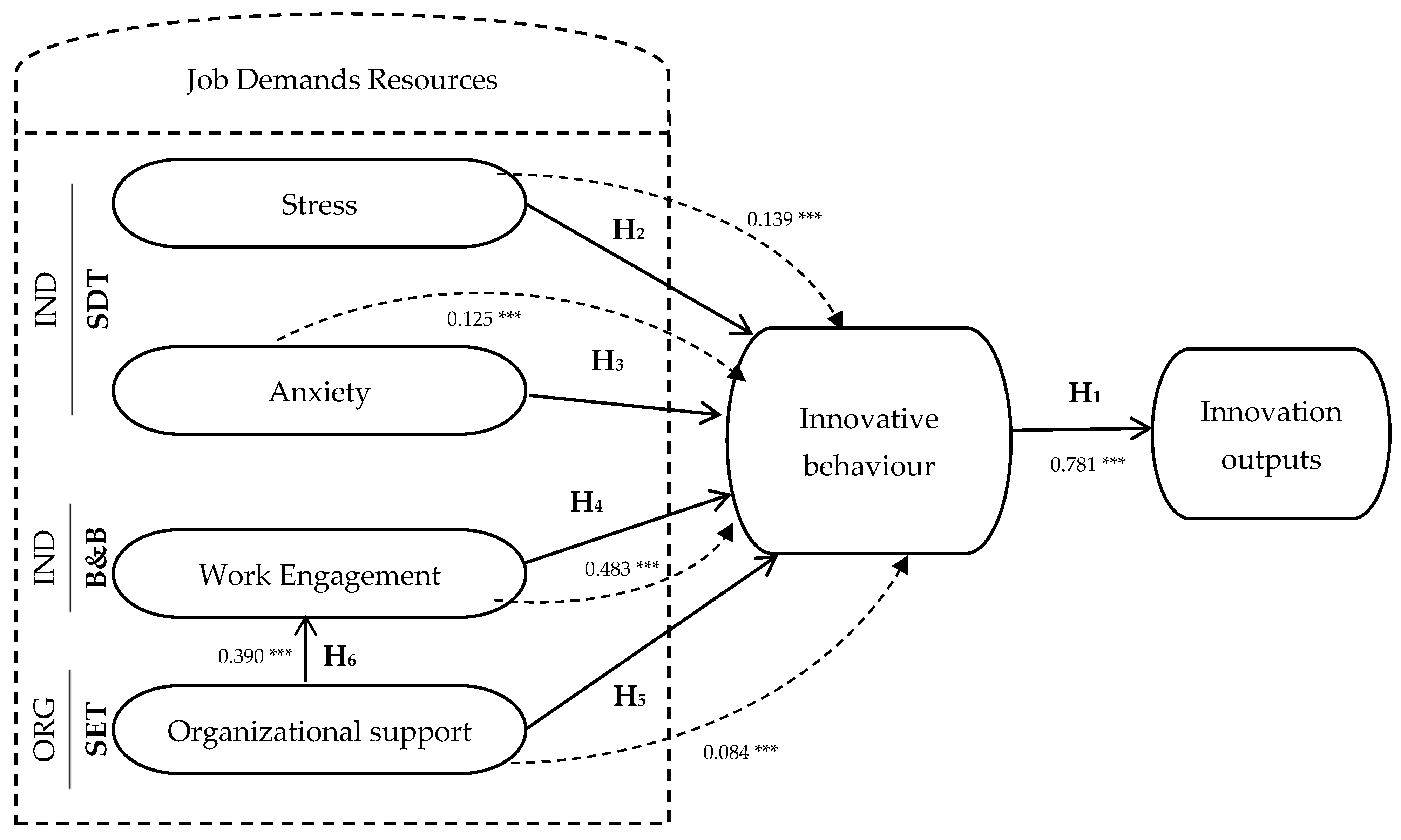
4.3. Structural Model (Inner Model)
4.4. Hypotheses and Research Questions
5. Discussion of Results
5.1. ‘Stress’ and ‘Anxiety’ Influence ‘Innovative Behaviour’ Supporting Hypotheses 2 and 3, Respectively
5.2. ‘Work Engagement’ Has a Significant Effect on ‘Innovative Behaviour’, Supporting Hypothesis 4
6. Conclusions and Future Recommendations
6.1. Conclusions
6.2. Theoretical Contributions
6.3. Practical Contributions
6.4. Implications and Limitations of the Research
6.5. Future Recommendations
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Selye, H. The Stress of Live, 2nd ed.; NK, McGraw-Hill: New York, NY, USA, 1975. [Google Scholar]
- Shen, X.; Zou, X.; Zhong, X.; Yan, J.; Li, L. Psychological stress of ICU nurses in the time of COVID-19. Crit. Care 2020, 24, 200. [Google Scholar] [CrossRef]
- Klein, R.G.; Pine, D.S. Anxiety Disorders. In Child and Adolescent Psychiatr, 4th ed.; Rutter, M., Taylor, E., Eds.; Blackwell Publishing: Oxford, UK, 2002; pp. 483–509. [Google Scholar]
- Labrague, L.J.; de los Santos, J. COVID-19 anxiety among frontline nurses: Predictive role of organizational support, personal resilience and social support. J. Nurs. Manag. 2020, 28, 1653–1661. [Google Scholar] [CrossRef]
- Porto-Martins, P.; Basso-Machado, P.; Benevides-Pereira, A. Engagement no trabalho: Uma discussão teórica. Fractal: Rev. De Psicol. 2013, 25, 629–644. [Google Scholar] [CrossRef] [Green Version]
- Miawati, T.; Tukiran, M.; Anggorodi, R. Work Engagement in Nurses during The Covid-19 Pandemic: A Literature Review. J. Ind. Eng. Manag. Res. 2021, 2, 131–137. [Google Scholar] [CrossRef]
- Amin, N.; Quek, K.F.; Oxley, J.A.; Noah, R.; Nordin, R. Emotional Distress as a Predictor of Work-Related Musculoskeletal Disorders in Malaysian Nursing Professionals. Int. J. Occup. Environ. Med. 2018, 9, 69–78. [Google Scholar] [CrossRef] [Green Version]
- Bakker, A.B.; Demerouti, E. Towards a model of work engagement. Career Dev. Int. 2007, 13, 209–223. [Google Scholar] [CrossRef] [Green Version]
- Bakker, A.B.; de Vries, J.D. Job Demands–Resources theory and self-regulation: New explanations and remedies for job burnout. Anxiety Stress Coping 2021, 34, 1–21. [Google Scholar] [CrossRef] [PubMed]
- Castro, J.; Gazetta, C.; Silva, A.; Sodré, P.; Lourenção, L. Occupational stress and engagement in oral health professionals. Rev. Bras. Em Promoção Da Saúde 2019, 32, 9157. [Google Scholar] [CrossRef]
- Xanthopoulou, D.; Bakker, A.B.; Demerouti, E.; Schaufeli, W.B. The role of personal resources in the job demands-resources model. Int. J. Stress Manag. 2007, 14, 121–141. [Google Scholar] [CrossRef] [Green Version]
- Chen, C.H.; Wang, J.; Yang, C.-S.; Fan, J.-Y. Nurse practitioner job content and stress effects on anxiety and depressive symptoms, and self-perceived health status. J. Nurs. Manag. 2016, 24, 695–704. [Google Scholar] [CrossRef]
- González-Gancedo, J.; Fernández-Martínez, E.; Rodríguez-Borrego, M.A. Relationships among general health, job satisfaction, work engagement and job features in nurses working in a public hospital: A cross-sectional study. J. Clin. Nurs. 2019, 28, 1273–1288. [Google Scholar] [CrossRef] [PubMed]
- Hetzel-Riggin, M.; Swords, B.; Tuang, H.; Deck, J.; Spurgeon, N. Work Engagement and Resiliency Impact the Relationship Between Nursing Stress and Burnout. Psychol. Rep. 2019, 123, 1835–1853. [Google Scholar] [CrossRef] [PubMed]
- Kurtessis, J.N.; Eisenberger, R.; Ford, M.T.; Buffardi, L.C.; Stewart, K.A.; Adis, C.S. Perceived Organizational Support: A Meta-Analytic Evaluation of Organizational Support Theory. J. Manag. 2017, 43, 1854–1884. [Google Scholar] [CrossRef] [Green Version]
- Maben, J.; Bridges, J. Covid-19: Supporting nurses’ psychological and mental health. J. Clin. Nurs. 2020, 29, 2742–2750. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Scott, S.G.; Bruce, R.A. Determinants of Innovative Behavior: A Path Model of Individual Innovation in the Workplace. Acad. Manag. J. 1994, 37, 580–607. [Google Scholar] [CrossRef]
- West, M.A.; Farr, J.L. Innovation at work. In Innovation and Creativity at Work: Psychological and Organizational Strategies, 1st ed.; West, M.A., Farr, J.L., Eds.; John Wiley & Sons: Chichester, UK, 1990; pp. 3–13. [Google Scholar]
- Krause, D.E. Influence-Based Leadership as a Determinant of the Inclination to Innovate and of Innovation-Related Behaviors: An Empirical Investigation. Leadersh. Q. 2004, 15, 79–102. [Google Scholar] [CrossRef]
- Lukeš, M.; Stephan, U. Measuring employee innovation. Int. J. Entrep. Behav. Res. 2017, 23, 136–158. [Google Scholar] [CrossRef]
- Brunetto, Y.; Saheli, N.; Dick, T.; Nelson, S. Psychosocial Safety Climate, Psychological Capital, Healthcare SLBs’ Wellbeing and Innovative Behaviour During the COVID-19 Pandemic. Public Perform. Manag. Rev. 2021, 1–22. [Google Scholar] [CrossRef]
- Demerouti, E.; Bakker, A.; Nachreiner, F.; Schaufeli, W. The job demands-resources model of burnout. J. Appl. Psychol. 2001, 86, 499–512. [Google Scholar] [CrossRef] [PubMed]
- Schaufeli, W. Engaging leadership in the job demands-resources model. Career Dev. Int. 2015, 20, 446–463. [Google Scholar] [CrossRef] [Green Version]
- Eva, N.; Meacham, H.; Newman, A.; Schwarz, G.; Tham, T. Is coworker feedback more important than supervisor feedback for increasing innovative behavior? Hum. Resour. Manag. 2019, 58, 383–396. [Google Scholar] [CrossRef]
- Agarwal, U.A.; Datta, S.; Blake-Beard, S.; Bhargava, S. Linking LMX, innovative work behaviour and turnover intentions: The mediating role of work engagement. Career Dev. Int. 2019, 17, 208–230. [Google Scholar] [CrossRef]
- Axtell, C.M.; Holman, D.J.; Unsworth, K.L.; Wall, T.D.; Waterson, P.E.; Harrington, E. Shopfloor innovation: Facilitating the suggestion and implementation of ideas. J. Occup. Organ. Psychol. 2000, 73, 265–285. [Google Scholar] [CrossRef]
- Carnevale, J.B.; Huang, L.; Crede, M.; Harms, P.; Uhl-Bien, M. Leading to Stimulate Employees’ Ideas: A Quantitative Review of Leader-Member Exchange, Employee Voice, Creativity, and Innovative Behavior. Appl. Psychol. 2017, 66, 517–552. [Google Scholar] [CrossRef]
- Janssen, M.; Heerkens, Y.; Van der Heijden, B.; Korzilius, H.; Peters, P.; Engels, J. A study protocol for a cluster randomised controlled trial on mindfulness-based stress reduction: Studying effects of mindfulness-based stress reduction and an additional organizational health intervention on mental health and work-related perceptions of teachers in Dutch secondary vocational schools. Trials 2020, 21, 1–18. [Google Scholar] [CrossRef]
- McSherry, R.; Douglas, M. Innovation in nursing practice: A means to tackling the global challenges facing nurses, midwives and nurse leaders and managers in the future. J. Nurs. Manag. 2011, 19, 165–169. [Google Scholar] [CrossRef] [PubMed]
- Hoch, J.E. Shared leadership and innovation: The role of vertical leadership and employee integrity. J. Bus. Psychol. 2013, 28, 159–174. [Google Scholar] [CrossRef] [Green Version]
- Afsar, B.; Badir, F.Y.; Saeed, B. Transformational leadership and innovative work behaviour. Ind. Manag. Data Syst. 2014, 114, 1270–1300. [Google Scholar] [CrossRef]
- Rao, J.; Weintraub, J. How Innovative Is Your Company’s Culture? MIT Sloan Manag. Rev. 2013, 54, 29–37. Available online: https://sloanreview.mit.edu/article/how-innovative-is-your-companys-culture/ (accessed on 13 April 2020).
- Rahmadani, V.; Schaufeli, W.; Stouten, J.; Zhang, Z.; Zulkarnain, Z. Engaging Leadership and Its Implication for Work Engagement and Job Outcomes at the Individual and Team Level: A Multi-Level Longitudinal Study. Int. J. Environ. Res. Public Health 2020, 17, 776. [Google Scholar] [CrossRef] [Green Version]
- Farr, F.; Ford, C. Individual innovation. In Innovation and Creativity at Work: Psychological and Organizational Strategies, 1st ed.; West, M.A., Farr, J.L., Eds.; John Wiley & Sons: Chichester, UK, 1990; pp. 63–80. [Google Scholar]
- Garg, S.; Dhar, R. Employee service innovative behavior: The roles of leader-member exchange (LMX), work engagement, and job autonomy. Int. J. Manpow. 2017, 38, 242–258. [Google Scholar] [CrossRef]
- Janssen, O.; van Yperen, N.W. Employees’ goal orientations, the quality of leader-member exchange, and the role of job performance and job satisfaction. Acad. Manag. J. 2004, 47, 368–384. [Google Scholar] [CrossRef] [Green Version]
- Tierney, P. Leadership and creativity: A Reciprocal Evolving Model. In Handbook of Organizational Creativity; Zhou, J., Shalley, C.E., Eds.; Lawrence Erlbaum Associates: Mahwah, NJ, USA, 2008; pp. 95–123. [Google Scholar]
- Bakker, A.B.; Demerouti, E.; de Boer, E.; Schaufeli, W. Job demands and job resources as predictors of absence duration and frequency. J. Vocat. Behav. 2003, 62, 341–356. [Google Scholar] [CrossRef]
- Kwon, K.; Kim, T. An integrative literature review of employee engagement and innovative behavior: Revisiting the JD-R model. Hum. Resour. Manag. Rev. 2020, 30, 100704. [Google Scholar] [CrossRef]
- Montani, F.; Vandenberghe, C.; Khedhaouria, A.; Courcy, F. Examining the inverted U-shaped relationship between workload and innovative work behavior: The role of work engagement and mindfulness. Hum. Relat. 2019, 73, 59–93. [Google Scholar] [CrossRef]
- Carlucci, D.; Mura, M.; Schiuma, G. Fostering Employees’ Innovative Work Behaviour in Healthcare Organizations. International J. Innov. Manag. 2019, 24, 2050014. [Google Scholar] [CrossRef]
- Åmo, B.W. Employee innovation behaviour in health care: The influence from management and colleagues. Int. Nurs. Rev. 2006, 53, 231–237. [Google Scholar] [CrossRef]
- Holleman, G.; Poot, E.; Mintjes-de Groot, J.; van Achterberg, T. The relevance of team characteristics and team directed strategies in the implementation of nursing innovations: A literature review. Int. J. Nurs. Stud. 2009, 46, 1256–1264. [Google Scholar] [CrossRef] [Green Version]
- Weng, R.-H.; Huang, C.-Y.; Huang, J.-A.; Wang, M.-H. The cross-level impact of patient safety climate on nursing innovation: A cross-sectional questionnaire survey. J. Clin. Nurs. 2012, 21, 2262–2274. [Google Scholar] [CrossRef] [PubMed]
- Fan, Y.; Zheng, Q.; Liu, S.; Li, Q. Construction of a new model of job engagement, psychological empowerment and perceived work environment among Chinese registered nurses at four large university hospitals: Implications for nurse managers seeking to enhance nursing retention and quality of care. J. Nurs. Manag. 2016, 24, 646–655. [Google Scholar] [CrossRef]
- De Jong, J.; Den Hartog, D. Measuring innovative work behaviour. Creat. Innov. Manag. 2010, 19, 23–36. [Google Scholar] [CrossRef]
- Ahmed, A.; Ramzan, M. Effects of Job Stress on Employees Job Performance A Study on Banking Sector of Pakistan. IOSR J. Bus. Manag. 2013, 11, 61–68. [Google Scholar] [CrossRef]
- Wolor, C.W.; Dalimunthe, S.; Febrilia, I.; Martono, S. How to Manage Stress Experienced by Employees When Working from Home Due to the Covid-19 Virus Outbreak. Int. J. Adv. Sci. Technol. 2020, 29, 8359–8364. [Google Scholar]
- Malik, T. Culturally Imprinted Anxiety and the Itinerary of Clinical Trial Projects for Its Management. Cross-Cultural Research 2020, 55, 148–178. [Google Scholar] [CrossRef]
- Smith, C.; Lazarus, R.S. Emotion and adaptation. In Handbook of Personality: Theory and Research; Pervin, L.A., Ed.; The Guilford Press: New York, NY, USA, 1991; pp. 609–637. [Google Scholar]
- Vargas, D.; Dias, A. Depression prevalence in Intensive Care Unit nursing workers: A study at hospitals in a northwestern city of São Paulo State. Rev. Lat. -Am. Enferm. 2011, 19, 1114–1121. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Welsh, D. Predictors of Depressive Symptoms in Female Medical-Surgical Hospital Nurses. Issues Ment. Health Nurs. 2009, 30, 320–326. [Google Scholar] [CrossRef]
- Alhakami, I.Y.; Baker, O.G. Work motivation and self-rated anxiety: Nurses’ perspectives. Clin. Nurs. Stud. 2018, 6, 69–79. [Google Scholar] [CrossRef] [Green Version]
- Polat, Ş.; Kutlu, L.; Ay, F.; Purisa, S.; Erkan, H.A. Decision-making styles, anxiety levels, and critical thinking levels of nurses. Jpn. J. Nurs. Sci. 2018, 16, 309–321. [Google Scholar] [CrossRef]
- Trifiletti, E.; Pedrazza, M.; Berlanda, S.; Pyszczynski, T. Burnout disrupts anxiety buffer functioning among nurses: A three-way interaction model. Front. Psychol. 2017, 8, 1–10. [Google Scholar] [CrossRef]
- LePine, J.A.; Podsakoff, N.P.; LePine, M.A. A meta-analytic test of the challenge stressor-hindrance stressor framework: An explanation for inconsistent relationships among stressors and performance. Acad. Manag. J. 2005, 48, 764–775. [Google Scholar] [CrossRef] [Green Version]
- Deci, E.L.; Ryan, R.M. Self-determination theory: A macrotheory of human motivation, development, and health. Can. Psychol. /Psychol. Can. 2008, 49, 182–185. [Google Scholar] [CrossRef] [Green Version]
- Schaufeli, W.; Bakker, A.B.; Salanova, M. The measurement of work engagement with a short questionnaire: A cross-national study. Educ. Psychol. Meas. 2006, 66, 701–716. [Google Scholar] [CrossRef]
- Zhang, X.; Bartol, K.M. Linking empowering leadership and employee creativity: The influence of psychological empowerment, intrinsic motivation, and creative process engagement. Acad. Manag. J. 2010, 53, 107–128. [Google Scholar] [CrossRef] [Green Version]
- Peng, K.Z.; Ngo, H.Y.; Shi, J.; Wong, C.S. Gender differences in the work commitment of Chinese workers: An investigation of two alternative explanations. J. World Bus. 2009, 44, 323–335. [Google Scholar] [CrossRef]
- Fredrickson, B.L. The broaden-and-build theory of positive emotions. Philos. Trans. R. Soc. London. Ser. B Biol. Sci. 2004, 359, 1367–1378. [Google Scholar] [CrossRef]
- Luthans, F. The need for and meaning of positive organizational behavior. J. Organ. Behav. 2002, 23, 695–706. [Google Scholar] [CrossRef] [Green Version]
- Yeh, C.W. Relationships among service climate, psychological contract, work engagement and service performance. J. Air Transp. Manag. 2012, 25, 67–70. [Google Scholar] [CrossRef]
- Bakker, A.B.; Leiter, M.P. Where to go from here: Integration and future research on work engagement. In Work Engagement: A Handbook of Essential Theory and Research, 1st ed.; Bakker, A.B., Leiter, M.P., Eds.; Psychology Press: East Sussex, UK, 2010; pp. 181–196. [Google Scholar]
- Jenaro, C.; Flores, N.; Orgaz, M.B.; Cruz, M. Vigour and dedication in nursing professionals: Towards a better understanding of work engagement. J. Adv. Nurs. 2011, 67, 865–875. [Google Scholar] [CrossRef] [PubMed]
- Vander Elst, T.; Cavents, C.; Daneels, K.; Johannik, K.; Baillien, E.; Van den Broeck, A.; Godderis, L. Job demands–resources predicting burnout and work engagement among Belgian home health care nurses: A cross-sectional study. Nurs. Outlook 2016, 64, 542–556. [Google Scholar] [CrossRef] [PubMed]
- Tims, M.; Bakker, A.B.; Xanthopoulou, D. Do transformational leaders enhance their followers’ daily work engagement? Leadersh. Q. 2011, 22, 121–131. [Google Scholar] [CrossRef] [Green Version]
- Wefald, A.J.; Downey, R.G. Construct dimensionality of engagement and its relation with satisfaction. J. Psychol. 2009, 143, 91–112. [Google Scholar] [CrossRef]
- Leiter, M.P.; Bakker, A.B. Work engagement: Introduction. In Work Engagement: A Handbook of Essential Theory and Research, 1st ed.; Bakker, A.B., Leiter, M.P., Eds.; Psychology Press: London, UK, 2010; pp. 1–9. [Google Scholar] [CrossRef]
- Eisenberger, R.; Huntington, R.; Hutchison, S.; Sowa, D. Perceived organizational support. J. Appl. Psychol. 1986, 71, 500–507. [Google Scholar] [CrossRef]
- Eisenberger, R.; Armeli, S.; Rexwinkel, B.; Lynch, P.; Rhoades, L. Reciprocation of perceived organizational support. J. Appl. Psychol. 2001, 86, 42–51. [Google Scholar] [CrossRef]
- Siqueira, M.; Gomide, S. Vínculos do indivíduo com o trabalho e com a organização. In Psicologia, Organizações e Trabalho No Brasil; Zanelli, J.C., Borges-Andrade, J.E., Bastos, A.V.B., Eds.; Artmed: Porto Alegre, Brazil, 2004; pp. 300–328. [Google Scholar]
- Cropanzano, R.; Mitchell, M.S. Social Exchange Theory: An Interdisciplinary Review. J. Manag. 2005, 31, 874–900. [Google Scholar] [CrossRef] [Green Version]
- Vazquez, A.C.S.; Magnan, E.S.; Pacico, J.C.; Hutz, C.S.; Schaufeli, W.B. Adaptation and Validation of the Brazilian Version of the Utrecht Work Engagement Scale. Psico-USF 2015, 20, 207–217. [Google Scholar] [CrossRef] [Green Version]
- Saks, A.M. Antecedents and consequences of employee engagement. J. Manag. Psychol. 2006, 21, 600–619. [Google Scholar] [CrossRef] [Green Version]
- Eisenberger, R.; Stinglhamber, F. Perceived Organizational Support: Fostering Enthusiastic and Productive Employees. Am. Psychol. Assoc. 2011. [Google Scholar] [CrossRef]
- Fredrickson, B.L. The role of positive emotions in positive psychology: The broaden-and-build theory of positive emotions. Am. Psychol. 2006, 56, 218–226. [Google Scholar] [CrossRef]
- Fredrickson, B.L. What good are positive emotions? Rev. Gen. Psychol. 1998, 2, 300–319. [Google Scholar] [CrossRef] [PubMed]
- Fredrickson, B.L. Why positive emotions matter in organizations: Lessons from the broaden-and-build model. Psychol. Manag. J. 2000, 4, 131–142. [Google Scholar] [CrossRef]
- Chughtai, A.A. Linking affective commitment to supervisor to work outcomes. J. Manag. Psychol. 2013, 28, 606–627. [Google Scholar] [CrossRef]
- Salanova, M.; Agut, S.; Peiro, J.M. Linking organizational resources and work engagement to employee performance and customer loyalty: The mediation of service climate. J. Appl. Psychol. 2005, 90, 1217–1227. [Google Scholar] [CrossRef]
- Aryee, S.; Walumbwa, F.O.; Zhou, Q.; Hartnell, C.A. Transformational Leadership, Innovative Behavior, and Task Performance: Test of Mediation and Moderation Processes. Hum. Perform. 2012, 25, 1–25. [Google Scholar] [CrossRef]
- Kuratko, D.F.; Hornsby, J.S.; Covin, J.G. Diagnosing a firm’s internal environment for corporate entrepreneurship. Bus. Horiz. 2014, 57, 37–47. [Google Scholar] [CrossRef]
- Amirkhan, J.H. A Brief Stress Diagnostic Tool: The Short Stress Overload Scale. Assessment 2018, 25, 1001–1013. [Google Scholar] [CrossRef] [PubMed]
- Spitzer, R.L.; Kroenke, K.; Williams, J.B.W.; Löwe, B. A Brief Measure for Assessing Generalized Anxiety Disorder: The GAD-7. Arch. Intern. Med. 2006, 166, 1092–1097. [Google Scholar] [CrossRef] [Green Version]
- Ringle, C.M.; Wende, S.; Becker, J.-M. SmartPLS 3 [Software]; SmartPLS: Bönningstedt, Germany, 2015. [Google Scholar]
- Hair, J.F.; Sarstedt, M.; Pieper, T.M.; Ringle, C.M. The use of partial least squares structural equation modeling in strategic management research: A review of past practices and recommendations for future applications. Long Range Plan. 2012, 45, 320–340. [Google Scholar] [CrossRef]
- Hair, J.F.; Hult, G.T.M.; Ringle, C.M.; Sarstedt, M. A Primer on Partial Least Squares Structural Equation Modeling (PLS-SEM), 2nd ed.; Sage Publications: Thousand Oaks, CA, USA, 2017. [Google Scholar]
- Becker, J.-M.; Klein, K.; Wetzels, M. Hierarchical latent variable models in PLSSEM: Guidelines for using reflective–formative type models. Long Range Plan. 2012, 45, 359–394. [Google Scholar] [CrossRef]
- Jöreskog, K.G. Simultaneous factor analysis in several populations. Psychometrika 1971, 36, 409–426. [Google Scholar] [CrossRef]
- Bagozzi, R.P.; Yi, Y. On the evaluation of structural equation models. J. Acad. Mark. Sci. 1988, 16, 74–94. [Google Scholar] [CrossRef]
- Henseler, J.; Ringle, C.M.; Sarstedt, M. A new criterion for assessing discriminant validity in variance-based structural equation modeling. J. Acad. Mark. Sci. 2015, 43, 115–135. Available online: https://link.springer.com/article/10.1007/s11747-014-0403-8 (accessed on 23 May 2021). [CrossRef] [Green Version]
- Chin, W.W.; Marcoulides, G. The partial least squares approach to structural equation modeling. Adv. Hosp. Leis. 1998, 8, 295–336. [Google Scholar]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences, 2nd ed.; Lawrence Erlbaum Associates: New York, NY, USA, 1988. [Google Scholar]
- Falk, R.F.; Miller, N.B. A Primer for Soft Modelling, 1st ed.; University of Akron Press: Akron, OH, USA, 1992. [Google Scholar]
- Tenenhaus, M.; Vinzi, V.E.; Chatelin, Y.M.; Lauro, C. PLS path modeling. Comput. Stat. Data Anal. 2005, 48, 159–205. [Google Scholar] [CrossRef]
- Schaufeli, W.; De Witte, H. Work Engagement: Real or Redundant? Burn. Res. 2017, 5, 1–2. [Google Scholar] [CrossRef]
- Fink, G. Stress: Concepts, Definition and History. In Reference Module in Neuroscience and Biobehavioral Psychology; Elsevier: Melbourne, Australia, 2017; pp. 1–9. [Google Scholar] [CrossRef]
- Kim, J.J.; Diamond, D.M. The stressed hippocampus, synaptic plasticity and lost memories. Nat. Rev. Neurosci. 2002, 3, 453–462. [Google Scholar] [CrossRef] [PubMed]
- WHO–World Health Organization. Q&A Detail. 2020. Available online: https://www.who.int/news-room/q-a-detail/ccupational-health-stress-at-the-workplace (accessed on 22 June 2020).
- Wang, Y.X.; Yang, Y.J.; Wang, Y.; Su, D.; Li, S.W.; Zhang, T.; Li, H.P. The mediating role of inclusive leadership: Work engagement and innovative behaviour among Chinese head nurses. J. Nurs. Manag. 2019, 27, 688–696. [Google Scholar] [CrossRef] [PubMed]
- Hu, M.; Horng, J.; Sun, Y. Hospitality teams: Knowledge sharing and service innovation performance. Tour. Manag. 2009, 30, 41–50. [Google Scholar] [CrossRef]
- Kim, T.T.; Lee, G. Hospitality employee knowledge-sharing behaviors in the relationship between goal orientations and service innovative behavior. Int. J. Hosp. Manag. 2013, 34, 324–337. [Google Scholar] [CrossRef]
- Mitchell, M.S.; Ambrose, M.L. Abusive supervision and workplace deviance and the moderating effects of negative reciprocity beliefs. J. Appl. Psychol. 2007, 92, 1159–1168. [Google Scholar] [CrossRef]
- Ortiz-Hunt, A.; Hunt, R.; Lerner, D. Sustainable Human Healthcare: The Centrality of Intrapreneurial Nurses. Acad. Manag. Proc. 2019, 2019, 12403. [Google Scholar] [CrossRef]
- Radaelli, G.; Lettieri, E.; Mura, M.; Spiller, N. Knowledge Sharing and Innovative Work Behaviour in Healthcare: A Micro-Level Investigation of Direct and Indirect Effects. Creat. Innov. Manag. 2014, 23, 400–414. [Google Scholar] [CrossRef]
- Birdi, K.; Leach, D.; Magadley, W. The relationship of individual capabilities and environmental support with different facets of designers’ innovative behavior. J. Prod. Innov. Manag. 2016, 33, 19–35. [Google Scholar] [CrossRef]
- Afsar, B.; Cheema, S.; Bin Saeed, B. Do nurses display innovative work behavior when their values match with hospitals’ values? Eur. J. Innov. Manag. 2018, 21, 157–171. [Google Scholar] [CrossRef]
- Kroes, B. The Relationship Between Transformational Leadership and Innovative Work Behavior: The Role of Self-Efficacy and The Effect of Perceived Organizational Support on Innovative Work Behavior. Master’s Thesis, Tilburg University, Tilburg, The Netherlands, 2015. [Google Scholar]
- Park, Y.K.; Song, J.H.; Yoon, S.W.; Kim, J. Learning Organization and Innovative Behavior: The Mediating Effect of Work Engagement. Eur. J. Train. Dev. 2013, 38, 75–94. [Google Scholar] [CrossRef]
- Zhong, L.; Wayne, S.; Liden, R. Job engagement, perceived organizational support, high-performance human resource practices, and cultural value orientations: A cross-level investigation. J. Organ. Behav. 2016, 37, 823–844. [Google Scholar] [CrossRef]
- Basso, C. O Impacto do Suporte Organizacional e do Suporte à Aprendizagem no Engajamento no Trabalho e nos Danos Físicos e Psicossociais Relacionados ao Trabalho: O Caso de uma Instituição Federal de Ensino Superior. Master’s Thesis, Federal University Rio Grande do Sul, Porto Alegre, Brazil, 2020. Available online: http://hdl.handle.net/10183/212223 (accessed on 4 May 2020).




{kind=link}
{kind=link}
{kind=link}
| Items | λ | CR | α Cronb. | AVE |
|---|---|---|---|---|
| Anxiety (over the last 2 weeks, how often have you been bothered by the following problems) | ||||
| Ans_1-Feeling nervous, anxious or on edge | 0.886 *** | 0.964 | 0.958 | 0.793 |
| Ans_2-Not being able to stop or control worrying | 0.917 *** | |||
| Ans_3-Worrying too much about different things | 0.905 *** | |||
| Ans_4-Trouble relaxing | 0.922 *** | |||
| Ans_5-Being so restless that it is hard to sit still | 0.908 *** | |||
| Ans_6-Becoming easily annoyed or irritable | 0.887 *** | |||
| Ans_7-Feeling afraid as if something awful might happen | 0.805 *** | |||
| Stress | ||||
| Stress_1-In the past week, have you felt inadequate? | 0.704 *** | 0.934 | 0.929 | 0.588 |
| Stress_2-In the past week, have you felt swamped by your responsibilities? | 0.729 *** | |||
| Stress_3-In the past week, have you felt that the odds were against you? | 0.778 *** | |||
| Stress_4-In the past week, have you felt that there wasn’t enough time to get to everything? | 0.805 *** | |||
| Stress_5-In the past week, have you felt like nothing was going right? | 0.746 *** | |||
| Stress_6-In the past week, have you felt like you were rushed? | 0.793 *** | |||
| Stress_7-In the past week, have you felt like there was no escape? | 0.809 *** | |||
| Stress_8-In the past week, have you felt like things kept piling up? | 0.834 *** | |||
| Stress_9-In the past week, have you felt like just giving up? | 0.660 *** | |||
| Stress_10-In the past week, have you felt like you were carrying a heavy load? | 0.796 *** | |||
| Work Engagement | ||||
| WE_A–Absorption | 0.862 *** | 0.932 | 0.889 | 0.820 |
| WE_D–Dedication | 0.939 *** | |||
| WE_V–Vigour | 0.913 *** | |||
| Organizational Support | ||||
| OrgSup_1-The way of rewarding in my organization motivates employees to come up with new ideas and procedures | 0.889 *** | 0.974 | 0.968 | 0.862 |
| OrgSup_2-My organization encourages employees who have innovative ideas | 0.935 *** | |||
| OrgSup_3-My organization has ensured sufficient resources to support the implementation of new ideas | 0.936 *** | |||
| OrgSup_4-My organization provides time for employees to put their ideas and innovations into practice | 0.935 *** | |||
| OrgSup_5-My organization often recognizes employees who take individual risks for their willingness to defend new projects, whether they are successful or not | 0.953 *** | |||
| OrgSup_6-My organization encourages employees to talk to colleagues in other departments about ideas for new projects | 0.921 *** | |||
| Innovative Behaviour | ||||
| IDEAGEN-Generation of ideas | 0.820 *** | 0.945 | 0.930 | 0.741 |
| IDEASEA–Search for ideas | 0.802 *** | |||
| IDEACOM–Communication of ideas | 0.909 *** | |||
| IMPL–Start of implementation | 0.880 *** | |||
| INVOL–Involvement of colleagues | 0.879 *** | |||
| OVERC–Overcoming obstacles | 0.871 *** | |||
| Innovation Outputs | ||||
| OUT_01-I am often successful at work when I put my ideas into practice | 0.887 *** | 0.919 | 0.868 | 0.791 |
| OUT_02-Many things created by me are used in our organization | 0.879 *** | |||
| OUT_03-I have always implemented improvements in the places where I worked | 0.902 *** | |||
| (1) | (2) | (3) | (4) | (5) | (6) | |
|---|---|---|---|---|---|---|
| (1) Anxiety | ||||||
| (2) Stress | 0.773 | |||||
| (3) Work Engagement | 0.246 | 0.228 | ||||
| (4) Organizational Support | 0.057 | 0.057 | 0.420 | |||
| (5) Innovative Behaviour | 0.107 | 0.147 | 0.524 | 0.273 | ||
| (6) Innovation Outputs | 0.112 | 0.153 | 0.458 | 0.341 | 0.861 |
| Path | R2 | f 2 | f 2 Effect |
|---|---|---|---|
| Innovative Behaviour → Innovation outputs | 0.610 | 1.562 | Large |
| Stress → Innovative Behaviour | 0.290 | 0.014 | - |
| Anxiety → Innovative Behaviour | 0.290 | 0.011 | - |
| Work Engagement → Innovative Behaviour | 0.290 | 0.266 | Medium |
| Organizational Support → Innovative Behaviour | 0.290 | 0.008 | - |
| Organizational Support → Work Engagement | 0.152 | 0.179 | Medium |
| Path Direct Effect | Regression Coefficient (β) | p | Is the Hypothesis Supported? |
|---|---|---|---|
| H1: Innovative Behaviour → Innovation | 0.781 *** | <0.001 | Yes |
| H2: Stress → Innovative Behaviour | 0.139 ** | 0.002 | Yes |
| H3: Anxiety → Innovative Behaviour | 0.125 ** | 0.004 | Yes |
| H4: Work Engagement → Innovative Behaviour | 0.483 *** | <0.001 | Yes |
| H5: Organizational Support → Innovative Behaviour | 0.084 * | 0.014 | Yes |
| H6: Organizational Support → Work Engagement | 0.390 *** | <0.001 | Yes |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Moreno Cunha, A.; Marques, C.S.; Santos, G. Organizational and Personal Factors That Boost Innovation: The Case of Nurses during COVID-19 Pandemic Based on Job Demands-Resources Model. Sustainability 2022, 14, 458. https://doi.org/10.3390/su14010458
Moreno Cunha A, Marques CS, Santos G. Organizational and Personal Factors That Boost Innovation: The Case of Nurses during COVID-19 Pandemic Based on Job Demands-Resources Model. Sustainability. 2022; 14(1):458. https://doi.org/10.3390/su14010458
Chicago/Turabian StyleMoreno Cunha, Ariana, Carla Susana Marques, and Gina Santos. 2022. "Organizational and Personal Factors That Boost Innovation: The Case of Nurses during COVID-19 Pandemic Based on Job Demands-Resources Model" Sustainability 14, no. 1: 458. https://doi.org/10.3390/su14010458