
Factors Influencing the Evolution of Pulmonary Hypertension in Previously Healthy Subjects Recovering from a SARS-CoV-2 Infection

 ,
,  , , and
, , and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
- Patients aged over 18 but younger than 55 years, to avoid the impact of age on pulmonary and CV structure and function;
- The existence of a SARS-CoV2 infection within 4–8 weeks before the first exam, confirmed by a positive result of real-time reverse transcriptase-polymerase chain reaction (RT-PCR) assay of nasal and pharyngeal swabs, with a mild/moderate pulmonary injury during the acute phase, confirmed by CCT either during the hospitalization or as an outpatient during a COVID-19 evaluation, including CCT and laboratory tests;
- The persistence of symptoms defining the post-acute COVID-19 syndrome;
- An initial cardiologic examination with TTE, suggesting the presence of elevated esPAP values, with or without RVD, at 4–8 weeks after the acute infection and a second CCT assessment confirming the regression of pulmonary lesions;
- The willingness to attend subsequent cardiologic examinations with TTE at 3 and 6 months after the COVID-19.
- Patients under 18 or over 55 years old;
- Individuals who did not agree to sign the informed consent or those not willing to undergo all assessments;
- Subjects already diagnosed with PH before the COVID-19, those with a pre-existing history of other significant pulmonary and/or CV diseases, those who suffered confirmed pulmonary thromboembolism/deep vein thrombosis during COVID-19, or identified during the study with significant previously unknown cardiac pathology;
- Patients without a pre-existing COVID-19 assessment, including laboratory tests and CCT describing the severity of their lung injury, and/or without a subsequent control confirming the regression of these lesions;
- Patients with severe/critical forms of COVID-19 or with pulmonary infection associated with severe respiratory insufficiency, requiring mechanical ventilation.
2.2. Evaluation Methods
- Tricuspid Regurgitation Velocity (TRV) was determined from an apical window with continuous Doppler;
- The estimated esPAP was assessed based on the peak TRV and adding the right atrial pressure (RAP), which was estimated by determining the inferior vena cava’s diameter, as well as its respiratory variations. In our study, we assumed that esPAP levels ≥35 mm Hg at rest indicates PH [24,26] with its gravity ranging from mild (35–44 mmHg) to moderate (45–60 mm Hg) and severe (>60 mm Hg) [25,26];
- Tricuspid annular plane systolic excursion (TAPSE); was determined in M-Mode, at the lateral margin of the level of the tricuspid valve annulus; levels under 17 mm, were considered suggestive for RVD dysfunction;
- Fractional area change (FAC) was determined in four chamber views; values <35% being considered pathological;
- The eccentricity index to differentiate RV volume and pressure overload by measuring two LV minor axes (one parallel to the interventricular septum and another perpendicular to it) at both end-diastole and end-systole.
2.3. Statistical Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- CDC Coronavirus Disease 2019 (COVID-19). Available online: https://www.cdc.gov/coronavirus/2019-ncov/lab/resources/antibody-tests-guidelines.html (accessed on 10 January 2021).
- Rambaut, A.; Holmes, E.C.; O’Toole, Á.; Hill, V.; McCrone, J.T.; Ruis, C.; du Plessis, L.; Pybus, O.G. A dynamic nomenclature proposal for SARS-CoV-2 lineages to assist genomic epidemiology. Nat. Microbiol. 2020, 5, 1403–1407. [Google Scholar] [CrossRef] [PubMed]
- Aleem, A.; Akbar Samad, A.B.; Slenker, A.K. Emerging Variants of SARS-CoV-2 and Novel Therapeutics against Corona-Virus (COVID-19); StatPearls Publishing: Treasure Island, FL, USA, 2021. [Google Scholar]
- Huang, Y.; Tan, C.; Wu, J.; Chen, M.; Wang, Z.; Luo, L.; Zhou, X.; Liu, X.; Huang, X.; Yuan, S.; et al. Impact of coronavirus disease 2019 on pulmonary function in early convalescence phase. Respir. Res. 2020, 21, 163. [Google Scholar] [CrossRef] [PubMed]
- Blanco, J.-R.; Cobos-Ceballos, M.-J.; Navarro, F.; Sanjoaquin, I.; Revillas, F.A.D.L.; Bernal, E.; Buzon-Martin, L.; Viribay, M.; Romero, L.; Espejo-Perez, S.; et al. Pulmonary long-term consequences of COVID-19 infections after hospital discharge. Clin. Microbiol. Infect. 2021, 27, 892–896. [Google Scholar] [CrossRef] [PubMed]
- Bellan, M.; Soddu, D.; Balbo, P.E.; Baricich, A.; Zeppegno, P.; Avanzi, G.C.; Baldon, G.; Bartolomei, G.; Battaglia, M.; Battistini, S.; et al. Respiratory and Psychophysical Sequelae Among Patients With COVID-19 Four Months After Hospital Discharge. JAMA Netw. Open 2021, 4, e2036142. [Google Scholar] [CrossRef] [PubMed]
- Del Rio, C.; Collins, L.F.; Malani, P. Long-term Health Consequences of COVID-19. JAMA 2020, 324, 1723. [Google Scholar] [CrossRef]
- Moreno-Pérez, O.; Merino, E.; Leon-Ramirez, J.-M.; Andres, M.; Ramos, J.M.; Arenas-Jiménez, J.; Asensio, S.; Sanchez, R.; Ruiz-Torregrosa, P.; Galan, I.; et al. Post-acute COVID-19 syndrome. Incidence and risk factors: A Mediterranean cohort study. J. Infect. 2021, 82, 378–383. [Google Scholar] [CrossRef]
- Cascino, T.M.; Desai, A.A.; Kanthi, Y. At a crossroads: Coronavirus disease 2019 recovery and the risk of pulmonary vascular disease. Curr. Opin. Pulm. Med. 2021, 27, 342–349. [Google Scholar] [CrossRef]
- Norderfeldt, J.; Liliequist, A.; Frostell, C.; Adding, C.; Agvald, P.; Eriksson, M.; Lönnqvist, P. Acute pulmonary hypertension and short-term outcomes in severe Covid-19 patients needing intensive care. Acta Anaesthesiol. Scand. 2021, 65, 761–769. [Google Scholar] [CrossRef]
- Pagnesi, M.; Baldetti, L.; Beneduce, A.; Calvo, F.; Gramegna, M.; Pazzanese, V.; Ingallina, G.; Napolano, A.; Finazzi, R.; Ruggeri, A.; et al. Pulmonary hypertension and right ventricular involvement in hospitalised patients with COVID-19. Heart 2020, 106, 1324–1331. [Google Scholar] [CrossRef]
- Potus, F.; Mai, V.; Lebret, M.; Malenfant, S.; Breton-Gagnon, E.; Lajoie, A.C.; Boucherat, O.; Bonnet, S.; Provencher, S. Novel insights on the pulmonary vascular consequences of COVID-19. Am. J. Physiol. Cell. Mol. Physiol. 2020, 319, L277–L288. [Google Scholar] [CrossRef]
- Wu, X.; Liu, X.; Zhou, Y.; Yu, H.; Li, R.; Zhan, Q.; Ni, F.; Fang, S.; Lu, Y.; Ding, X.; et al. 3-month, 6-month, 9-month, and 12-month respiratory outcomes in patients following COVID-19-related hospitalisation: A prospective study. Lancet Respir. Med. 2021, 9, 747–754. [Google Scholar] [CrossRef]
- You, J.; Zhang, L.; Ni-Jia-Ti, M.-Y.-D.-L.; Zhang, J.; Hu, F.; Chen, L.; Dong, Y.; Yang, K.; Zhang, B.; Zhang, S. Anormal pulmonary function and residual CT abnormalities in rehabilitating COVID-19 patients after discharge. J. Infect. 2020, 81, e150–e152. [Google Scholar] [CrossRef]
- Malik, B.; Abdelazeem, B.; Ghatol, A. Pulmonary Fibrosis After COVID-19 Pneumonia. Cureus 2021, 13. [Google Scholar] [CrossRef]
- Vrettou, A.-R.; Parissis, J.; Ikonomidis, I. The Dual Role of Echocardiography in the Diagnosis of Acute Cardiac Complications and Treatment Monitoring for Coronavirus Disease 2019 (COVID-19). Front. Cardiovasc. Med. 2020, 7, 19. [Google Scholar] [CrossRef]
- Bursi, F.; Santangelo, G.; Sansalone, D.; Valli, F.; Vella, A.M.; Toriello, F.; Barbieri, A.; Carugo, S. Prognostic utility of quantitative offline 2D-echocardiography in hospitalized patients with COVID-19 disease. Echocardiography 2020, 37, 2029–2039. [Google Scholar] [CrossRef]
- Tudoran, M.; Tudoran, C.; Lazureanu, V.; Marinescu, A.; Pop, G.; Pescariu, A.; Enache, A.; Cut, T. Alterations of Left Ventricular Function Persisting during Post-Acute COVID-19 in Subjects without Previously Diagnosed Cardiovascular Pathology. J. Pers. Med. 2021, 11, 225. [Google Scholar] [CrossRef]
- Tudoran, C.; Tudoran, M.; Pop, G.; Giurgi-Oncu, C.; Cut, T.; Lazureanu, V.; Oancea, C.; Parv, F.; Ciocarlie, T.; Bende, F. Associations between the Severity of the Post-Acute COVID-19 Syndrome and Echocardiographic Abnormalities in Previously Healthy Outpatients Following Infection with SARS-CoV-2. Biology 2021, 10, 469. [Google Scholar] [CrossRef]
- Gandhi, R.T.; Lynch, J.B.; Del Rio, C. Mild or Moderate Covid-19. N. Engl. J. Med. 2020, 383, 1757–1766. [Google Scholar] [CrossRef]
- Rubin, G.D.; Ryerson, C.J.; Haramati, L.B.; Sverzellati, N.; Kanne, J.; Raoof, S.; Schluger, N.W.; Volpi, A.; Yim, J.-J.; Martin, I.B.K.; et al. The Role of Chest Imaging in Patient Management during the COVID-19 Pandemic: A Multinational Consensus Statement from the Fleischner Society. Radiology 2020, 296, 172–180. [Google Scholar] [CrossRef] [Green Version]
- Francone, M.; Iafrate, F.; Masci, G.M.; Coco, S.; Cilia, F.; Manganaro, L.; Panebianco, V.; Andreoli, C.; Colaiacomo, M.C.; Zingaropoli, M.A.; et al. Chest CT score in COVID-19 patients: Correlation with disease severity and short-term prognosis. Eur. Radiol. 2020, 30, 6808–6817. [Google Scholar] [CrossRef]
- Klok, F.A.; Boon, G.J.; Barco, S.; Endres, M.; Geelhoed, J.M.; Knauss, S.; Rezek, S.A.; Spruit, M.A.; Vehreschild, J.; Siegerink, B. The Post-COVID-19 Functional Status (PCFS) Scale: A Tool to Measure Functional Status over Time after COVID-19. Eur. Respir. J. 2020, 56, 2001494. [Google Scholar] [CrossRef]
- Lang, R.M.; Bierig, M.; Devereux, R.B.; Flachskampf, F.A.; Foster, E.; Pellikka, P.A.; Picard, M.; Roman, M.J.; Seward, J.; Shanewise, J.S.; et al. Recommendations for Chamber Quantification: A Report from the American Society of Echocardiography’s Guidelines and Standards Committee and the Chamber Quantification Writing Group, Developed in Conjunction with the European Association of Echocardiography, a Branch of the European Society of Cardiology. J. Am. Soc. Echocardiogr. 2005, 18, 1440–1463. [Google Scholar] [CrossRef]
- Badano, L.P.; Kolias, T.J.; Muraru, D.; Abraham, T.P.; Aurigemma, G.; Edvardsen, T.; D’Hooge, J.; Donal, E.; Fraser, A.G.; Marwick, T.; et al. Standardization of left atrial, right ventricular, and right atrial deformation imaging using two-dimensional speckle tracking echocardiography: A consensus document of the EACVI/ASE/Industry Task Force to standardize deformation imaging. Eur. Heart J. Cardiovasc. Imaging 2018, 19, 591–600. [Google Scholar] [CrossRef]
- Galiè, N.; Humbert, M.; Vachiéry, J.-L.; Gibbs, S.; Lang, I.M.; Kaminski, K.A.; Simonneau, G.; Peacock, A.; Noordegraaf, A.V.; Beghetti, M.; et al. 2015 ESC/ERS Guidelines for the diagnosis and treatment of pulmonary hypertension: The Joint Task Force for the Diagnosis and Treatment of Pulmonary Hypertension of the European Society of Cardiology (ESC) and the European Respiratory Society (ERS): Endorsed by: Association for European Paediatric and Congenital Cardiology (AEPC), International Society for Heart and Lung Transplantation (ISHLT). Eur. Heart J. 2015, 37, 67–119. [Google Scholar] [CrossRef] [PubMed]
- Baycan, O.F.; Barman, H.A.; Atici, A.; Tatlisu, A.; Bolen, F.; Ergen, P.; Icten, S.; Gungor, B.; Caliskan, M. Evaluation of biventricular function in patients with COVID-19 using speckle tracking echocardiography. Int. J. Cardiovasc. Imaging 2021, 37, 135–144. [Google Scholar] [CrossRef] [PubMed]
- Richter, D.; Guasti, L.; Koehler, F.; Squizzato, A.; Nistri, S.; Christodorescu, R.; Dievart, F.; Gaudio, G.; Asteggiano, R.; Ferrini, M. Late phase of COVID-19 pandemic in General Cardiology. A position paper of the ESC Council for Cardiology Practice. ESC Heart Fail. 2021, 8, 3483–3494. [Google Scholar] [CrossRef] [PubMed]
- Liang, L.; Yang, B.; Jiang, N.; Fu, W.; He, X.; Zhou, Y.; Ma, W.-L.; Wang, X. Three-Month Follow-Up Study of Survivors of Coronavirus Disease 2019 after Discharge. J. Korean Med. Sci. 2020, 35, e418. [Google Scholar] [CrossRef] [PubMed]
- Szekely, Y.; Lichter, Y.; Taieb, P.; Banai, A.; Hochstadt, A.; Merdler, I.; Oz, A.G.; Rothschild, E.; Baruch, G.; Peri, Y.; et al. Spectrum of Cardiac Manifestations in COVID-19: A Systematic Echocardiographic Study. Circulation 2020, 142, 342–353. [Google Scholar] [CrossRef]
- Nalbandian, A.; Sehgal, K.; Gupta, A.; Madhavan, M.V.; McGroder, C.; Stevens, J.S.; Cook, J.R.; Nordvig, A.S.; Shalev, D.; Sehrawat, T.S.; et al. Post-acute COVID-19 syndrome. Nat. Med. 2021, 27, 601–615. [Google Scholar] [CrossRef]
- Suzuki, Y.J.; Nikolaienko, S.I.; Shults, N.V.; Gychka, S.G. COVID-19 patients may become predisposed to pulmonary arterial hypertension. Med. Hypotheses 2021, 147, 110483. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
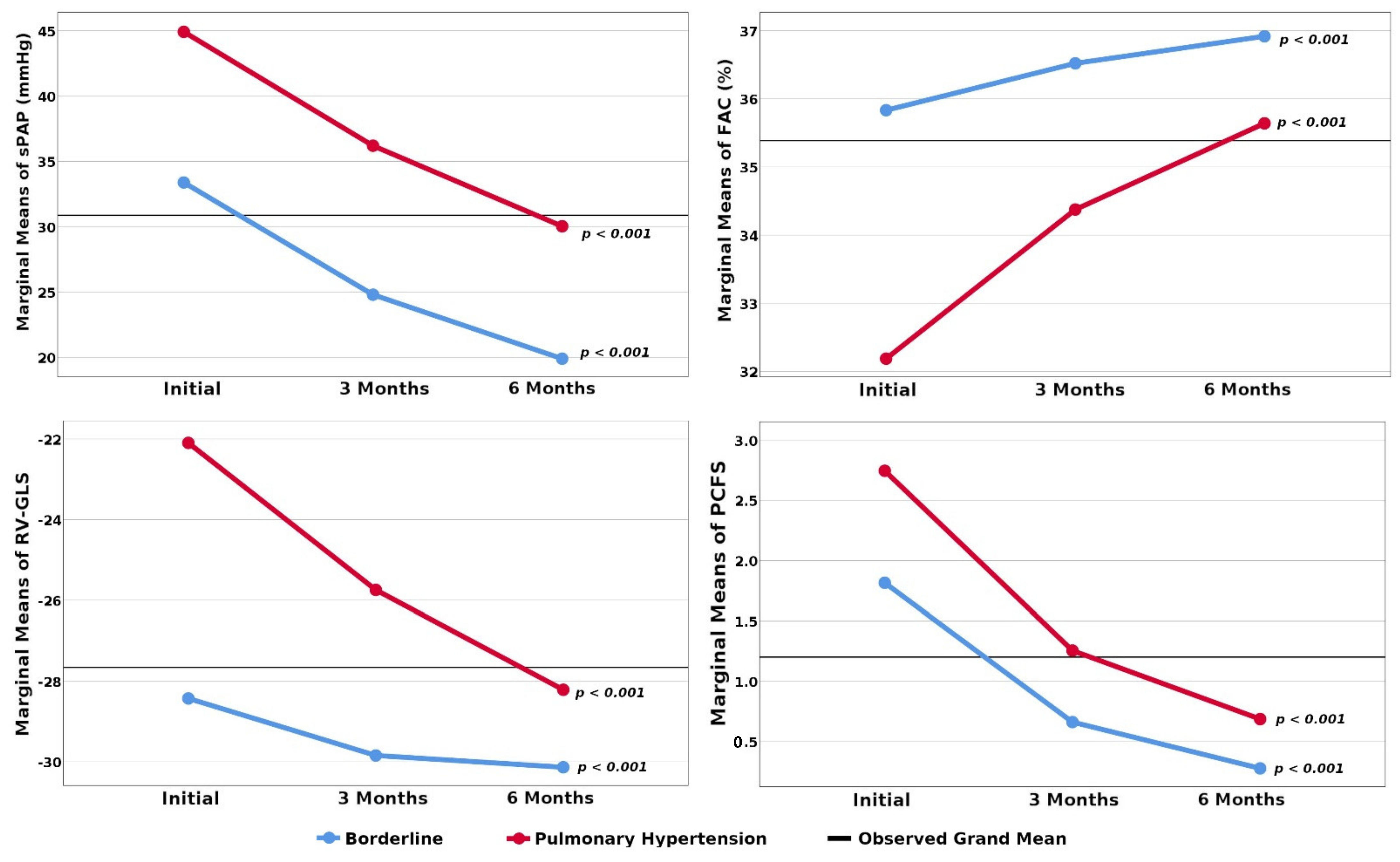
| Patients’ Characteristics at the First Evaluation | 51 Patients with PH | 65 Patients with Borderline Values | p |
|---|---|---|---|
| Age (years) | 52 (45–54) | 46 (42.5–50) | 0.001 a |
| Gender: -male -female | 28 (54.9%) 23 (45.09%) | 29 (44.61%) 36 (55.38%) | 0.271 b |
| BMI (Kg/m2) | 30.5 (27.47–31.80) | 27.45 (25.09–30.31) | 0.008 a |
| Initial pulmonary injury on CCT: -Mild: ˂30% -Moderate: 30–60% | 35 (31–40) 12 (23.52%) 39 (76.47%) | 15 (6–27.50) 52 (80%) 13 (20%) | ˂0.001 a ˂0.001 b |
| Initial CRP (mg/dL) | 43.57 (39.12–50.80) | 30.28 (26.58–37.52) | ˂0.001 a |
| PCFS scale | 3 (2–3) | 2 (2–2) | ˂0.001 a |
| Echocardiographic parameters | |||
| LAVI (mL/m2) | 29.7 (21.59–34.85) | 25.43 (18.46–33.39) | ˂0.001 a |
| LVEF (%) | 43 (40–50) | 55 (50–60) | ˂0.001 a |
| RA diameter (mm) | 38 (37–40) | 34 (33–35) | ˂0.001 a |
| RA area (cm2) | 14.44 (13.69–16) | 11.56 (10.89–12.25) | ˂0.001 a |
| RV diameter (mm) | 33 (32–35) | 28 (27–29) | ˂0.001 a |
| TRVmax: (m/s) | 3.15 (2.98–3.30) | 2.69 (2.61–2.70) | ˂0.001 a |
| esPAP (mmHg) | 44.69 (40.52–48.56) | 33.94 (32.24–34.16) | ˂0.001 a |
| TAPSE (mm) | 16 (15–17) | 20 (19–21.5) | ˂0.001 a |
| FAC (%) | 33.11 (30.24–34.02) | 35.85 (35.17–36.62) | ˂0.001 a |
| RV-GLS (%) | −22 (−25–−19) | −28 (−29–−28) | ˂0.001 a |
| EccI: End-diastole | 1.4 (1.2–1.6) | 1.1 (1–1.2) | ˂0.001 a |
| End-systole | 1.4 (1.1–1.6) | 1.1 (1–1.1) | ˂0.001 a |
| Parameter | esPAP at the Initial Evaluation | esPAP after 6 Months | ||||
|---|---|---|---|---|---|---|
| r | 95%CI | p | r | 95%CI | p | |
| Initial pulmonary injury | 0.821 | 0.736; 0.881 | ˂0.001 | 0.746 | 0.640; 0.815 | ˂0.001 |
| Initial CRP | 0.837 | 0.743; 0.899 | ˂0.001 | 0.725 | 0.602; 0.821 | ˂0.001 |
| PCFS | 0.713 | 0.604; 0.796 | ˂0.001 | 0.601 | 0.465; 0.705 | ˂0.001 |
| TAPSE | −0.889 | −0.929; −0.823 | ˂0.001 | −0.782 | −0.862; −0.671 | ˂0.001 |
| FAC | −0.894 | −0.929; −0.844 | ˂0.001 | −0.745 | −0.829; −0.633 | ˂0.001 |
| RV-GLS | 0.925 | 0.878; 0.957 | ˂0.001 | 0.783 | 0.680; 0.862 | ˂0.001 |
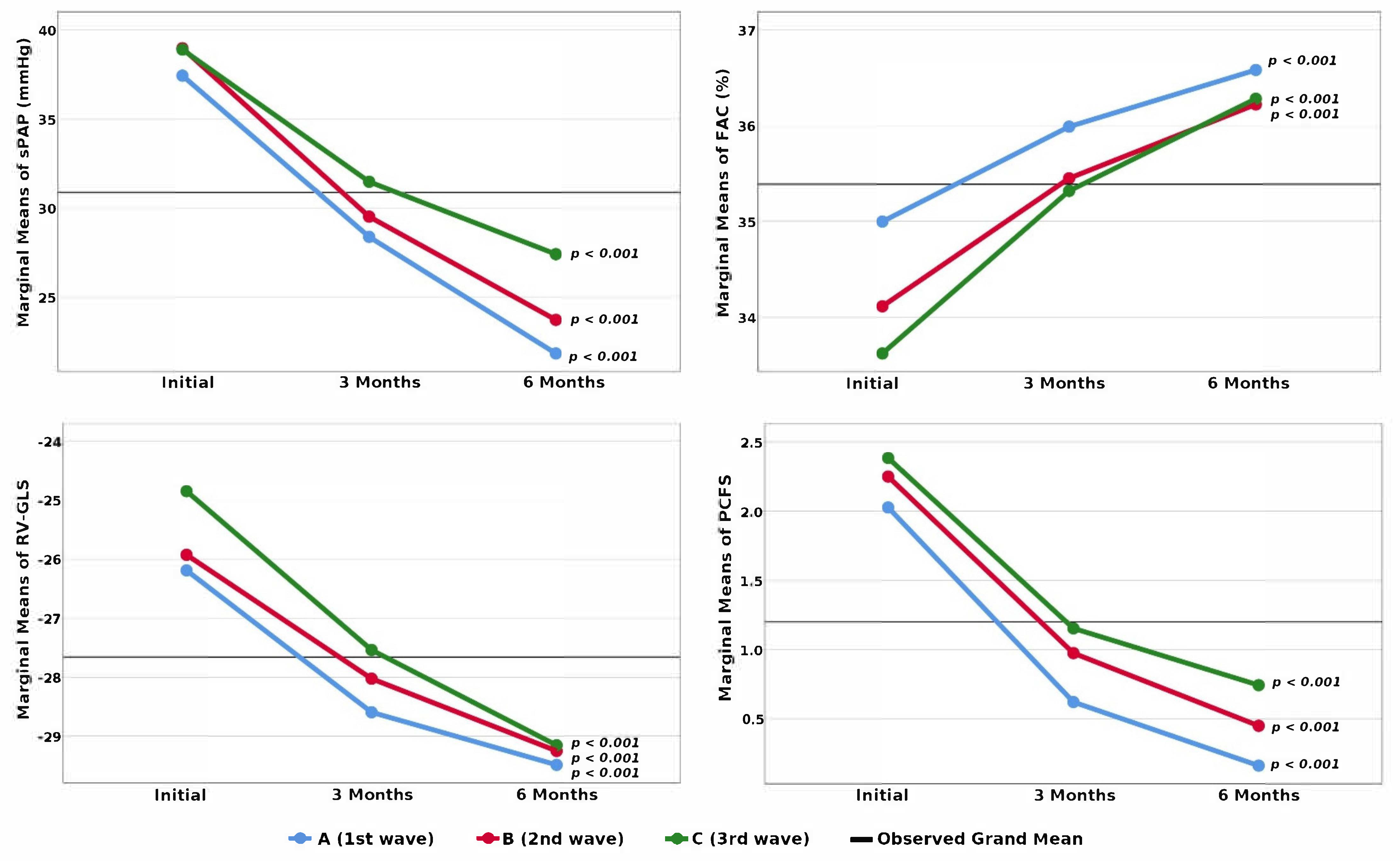
| Patients’ Characteristics at the First Evaluation | Group A 37 Patients | Group B 40 Patients | Group C 39 Patients | p |
|---|---|---|---|---|
| Patients with PH ± RVD | 15 (12% of 125) | 19 (12.66% of 150) | 17 (15.70% of 108) | 0.826 b |
| Borderline PH/RVD | 22 (17.6% of 125) | 21 (14% of 150) | 22 (20.37% of 108) | |
| Age (years) | 49 (45–54) | 50 (46–53) | 44 (40–47) | ˂0.001 a |
| Gender: male female | 22 (59.45%) 15 (40.54%) | 18 (45%) 22 (55%) | 17 (43.58%) 22 (56.41%) | 0.311 b |
| BMI | 27.72 (24.48–31.22) | 30.12 (27.54–32.67) | 27.73 (26.12–31.45) | 0.067 a |
| Initial pulmonary injury on TCT Mild: ˂30% Moderate: 30–60% | 20 (5–35) 22 (59.45%) 15 (40.54%) | 26.5 (15–35) 22 (55%) 18 (45%) | 30 (25–38) 16 (41.02%) 23 (58.97%) | 0.045 a 0.240 b |
| Initial CRP | 34.5 (25.62–41.95) | 38.06 (30.30–43.29) | 39.11 (29.67–41.82) | 0.198 a |
| PCFS | 3 (2–3) | 3 (2–3) | 3 (2–3) | 0.115 a |
| Echocardiographic parameters | ||||
| TRVmax: PH ± RVD borderline PH/RVD | 3.1 (2.95–3.29) 2.64 (2.60–2.70) | 3.15 (2.97–3.30) 2.69 (2.64–2.70) | 3.19 (3.03–3.40) 2.7 (2.60–2.71) | 0.443 a 0.181 a |
| esPAP: PH ± RVD borderline PH/RVD | 44.18 (39.80–48.29) 33.3 (32.04–34.16) | 44.69 (40.28–48.56) 33.94 (32.98–34.26) | 46.73 (41.70–49.62) 34.16 (32.04–34.37) | 0.443 a 0.181 a |
| TAPSE: PH ± RVD borderline PH/RVD | 16.63 (15.10–17.50)22 (20–22) | 16 (13.67–17)20 (19–21) | 15.37 (12.25–16.50)19 (18.75–20) | 0.087 a 0.001 a |
| FAC: PH ± RVD borderline PH/RVD | 33.56 (31.57–34.56) 36.1 (35.59–37) | 33.11 (30–34) 35.85 (35.10–36.61) | 32.87 (29.89–33.67) 35.39 (34.78–35.89) | 0.159 a 0.005 a |
| RV-GLS: PH ± RVD borderline PH/RVD | −23 (−25–−19) −29 (−29–−28) | −22 (−26–−20) −29 (−29–−28) | −20 (−24–−17.50) −28 (−29–−27) | 0.127 a 0.075 a |
| Variable | β | Standard Error | p | 95% CI for β |
|---|---|---|---|---|
| Wave | 1.763 | 0.472 | <0.001 | 0.827; 2.700 |
| Initial Pulmonary Injury | 0.127 | 0.046 | 0.007 | 0.036; 0.218 |
| esPAP (initial) | 0.702 | 0.084 | <0.001 | 0.535; 0.868 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tudoran, C.; Tudoran, M.; Lazureanu, V.E.; Marinescu, A.R.; Cut, T.G.; Oancea, C.; Pescariu, S.A.; Pop, G.N. Factors Influencing the Evolution of Pulmonary Hypertension in Previously Healthy Subjects Recovering from a SARS-CoV-2 Infection. J. Clin. Med. 2021, 10, 5272. https://doi.org/10.3390/jcm10225272
Tudoran C, Tudoran M, Lazureanu VE, Marinescu AR, Cut TG, Oancea C, Pescariu SA, Pop GN. Factors Influencing the Evolution of Pulmonary Hypertension in Previously Healthy Subjects Recovering from a SARS-CoV-2 Infection. Journal of Clinical Medicine. 2021; 10(22):5272. https://doi.org/10.3390/jcm10225272
Chicago/Turabian StyleTudoran, Cristina, Mariana Tudoran, Voichita Elena Lazureanu, Adelina Raluca Marinescu, Talida Georgiana Cut, Cristian Oancea, Silvius Alexandru Pescariu, and Gheorghe Nicusor Pop. 2021. "Factors Influencing the Evolution of Pulmonary Hypertension in Previously Healthy Subjects Recovering from a SARS-CoV-2 Infection" Journal of Clinical Medicine 10, no. 22: 5272. https://doi.org/10.3390/jcm10225272