Article Text

Abstract
The COVID-19 pandemic has led to an exponential increase in SARS-CoV-2 infections and associated deaths, and represents a significant challenge to healthcare professionals and facilities. Individual countries have taken several prevention and containment actions to control the spread of infection, including measures to guarantee safety of both healthcare professionals and patients who are at increased risk of infection from COVID-19. Faecal microbiota transplantation (FMT) has a well-established role in the treatment of Clostridioides difficile infection. In the time of the pandemic, FMT centres and stool banks are required to adopt a workflow that continues to ensure reliable patient access to FMT while maintaining safety and quality of procedures. In this position paper, based on the best available evidence, worldwide FMT experts provide guidance on issues relating to the impact of COVID-19 on FMT, including patient selection, donor recruitment and selection, stool manufacturing, FMT procedures, patient follow-up and research activities.
- colonic microflora
- diarrhoeal disease
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
The outbreak of coronavirus disease 2019 (COVID-19), caused by the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), was first identified in Wuhan and, despite the drastic safety measures taken by the Chinese government, rapidly evolved into a pandemic.
Consequently, healthcare facilities have intensively decreased elective activities both to avoid potential transmission of the virus and to shift human and structural resources to the management of COVID-19. Beyond these general measures, some gastroenterological activities have been triaged according to risk and need, including endoscopic procedures, which result in aerosolisation of the virus.1 2 Therefore, several scientific societies have released recommendations to prioritise indications and implement safe working protocols of endoscopic clinical practice during the pandemic.3–5
In recent years faecal microbiota transplantation (FMT) has revolutionised the management of recurrent Clostridioides difficile infection (CDI).6 7 As CDI continues to be associated with significant morbidity and mortality,8–11 FMT should be considered among the non-postponable gastroenterological procedures during the COVID-19 pandemic, at least in high-risk patients with CDI where FMT could be life-saving and the benefits outweigh the risks. FMT has become increasingly standardised and safe, and guidance on the general organisation and the criteria required to establish a stool bank has recently been released.12 However, this pandemic has raised several issues and concerns regarding the impact and risks of FMT related to SARS-CoV-2, as the risk of a medium- to long-term cohabitation with this pandemic is inevitable. Recently, the FDA has recommended that only FMT products generated from stool donated before 1 December 2019 should be used until proper SARS-CoV-2 testing of donors and/or stool 'as feasible' and screening protocols become available,13 and some FMT centres have suspended the active recruitment of new donors until FMT protocols are able to screen donors for COVID-19 and specific stool testing is available.14
Therefore, we aim to provide guidance regarding the reorganisation of FMT services in light of the evolving COVID-19 pandemic to assure the highest level of safety for the patients and healthcare providers who perform FMT.
Methods
The main topics of this position paper were proposed by two authors (GI and GC) and reviewed and refined by the working group, who were selected as being internationally acknowledged experts in FMT and stool banking. To update and extend on previously published guidelines in light of the evolving COVID-19 pandemic,12 15 the following key topics were identified by GI and GC and approved by all authors: patient selection; donor recruitment and selection; stool manufacturing and supply; FMT procedure and follow-up of treated patients. In addition to pragmatic expert guidance, a literature review was conducted to capture best available current evidence. Recommendations from the major international medical institutions (eg, WHO, European and US Centers for Disease Prevention and Control) and from scientific societies involved in digestive disorders were also reviewed.
However, in view of the limited evidence and need for urgent guidance, a formal standard consensus methodology was not followed.12 15 The first draft of the paper was primarily written by a small task force (GC, GI, CRK, BHM and ZK), and iterative changes were made via virtual discussion among all experts, including three rounds of revision, until consensus was reached. The final position paper was approved by all experts after further virtual discussion.
Patient selection
Recipients of FMT for recurrent/refractory CDI
The COVID-19 pandemic is going to affect the placement of FMT within the treatment algorithm for patients with recurrent or refractory CDI (figure 1).
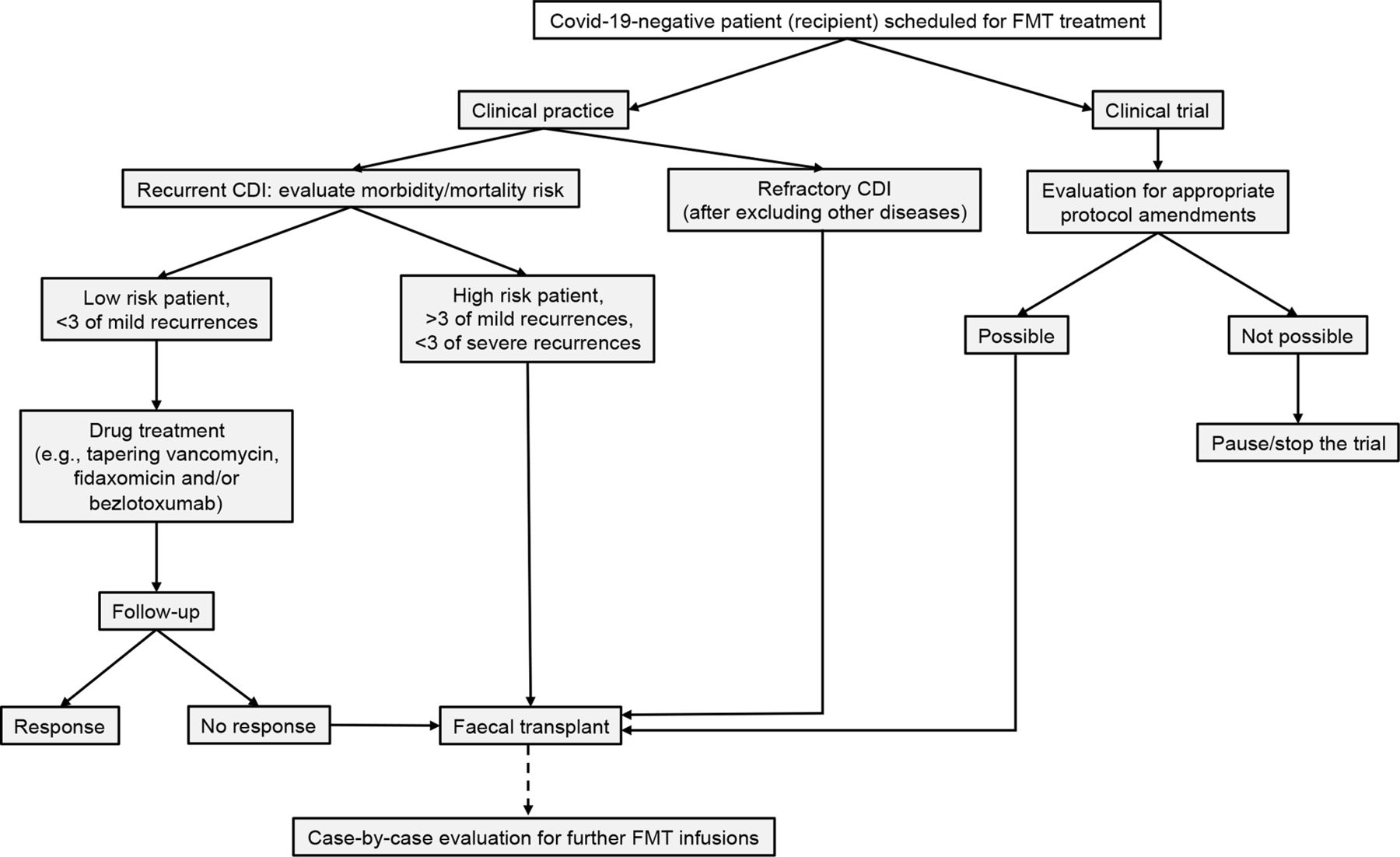
Proposed treatment algorithm for patients with recurrent or refractory Clostridioides difficile infection (CDI) during the COVID-19 pandemic. FMT, faecal microbiota transplantation.
CDI is present when it recurs within 8 weeks after the onset of a prior episode, provided that symptoms of the previous episode have been resolved after completion of initial treatment. Refractory disease occurs when CDI is unresponsive to the antimicrobial treatment and there is persistence of diarrhoea with positive C. difficile toxin, or of diarrhoea without toxin in the absence of other plausible causes of diarrhoea.16
The indication for FMT should be considered on a case-by-case basis, taking into account factors including: number and severity of previous CDI episodes; prior treatment modalities administered and alternative possible strategies; comorbidities; and the safety, feasibility and practicality of FMT administration, given the specific complexities presented by the COVID-19 pandemic.
At present, it may be pragmatic to consider treating many ‘typical’ recurrent CDI patients—who would have received FMT in the pre-COVID-19 era—with other approved therapies, including vancomycin, fidaxomicin and/or bezlotoxumab.16 17 Specifically, there may be a role for tapered and pulsed vancomycin regimens or extended fidaxomicin, although there is a paucity of data.17 This strategy may have the dual benefit of effectively treating a patient with recurrent CDI, while also creating a ‘window’ of time in which clinical developments may occur which could facilitate safer administration of FMT—for example, improvements in donor screening techniques or adequate organisation of the FMT centre.
However, during the COVID-19 pandemic there are still likely to be a number of patients with presumed recurrent/refractory CDI for whom FMT is thought to be the most appropriate therapy—for example, especially those with fulminant CDI who have limited therapeutic alternatives and are felt to not be surgical candidates. In all such cases, careful evaluation of diagnostic certainty of CDI causing symptoms needs to be made prior to considering FMT.
Furthermore, it would be appropriate to have a detailed discussion during the consent process with such patients to explain the complexities and uncertainties associated with FMT, and alternative treatment options during the pandemic. A further uncertainty relates to the number of FMTs that may be appropriate in a CDI treatment regimen. Specifically, protocols related to pseudomembranous colitis have reported good outcomes either through repeating FMT every 3 days until pseudomembrane resolution18 or, alternatively, giving 5 days of vancomycin in the case of FMT failure before a subsequent FMT.19 Almost all FMT studies in CDI and clinical guidelines recognise that sequential FMT has higher efficacy than a single infusion, at least in specific situations such as severe CDI or enema infusion.6 15 20 Therefore, when clinicians are committing to FMT as a treatment approach in the time of COVID-19, it seems reasonable that they are prepared to offer at least a second FMT to a patient in the event of initial FMT failure, using, if possible, aliquots from the same donor of the first infusion to reduce the risk for transmission. However, recognising the risks inherent in FMT administration at present, as well as the limited FMT stocks available for the forseeable future, stool banks and/or clinicians should consider on a case-by-case basis whether offering two or more FMTs for a patient with recurrent/refractory CDI is feasible, safe, appropriate and equitable compared with other patients who may also be in need.
When FMT is being considered in a COVID-19-positive patient with CDI, an additional consideration to the above should be whether the FMT procedure can be postponed. The treatment for recurrent/refractory CDI should be considered on a case-by-case basis, taking into account all the above discussed factors and also the COVID-19-related clinical picture. In such cases, a thorough multidisciplinary discussion among FMT experts, infectious disease physicians and intensivists/anaesthetists is mandatory.
Donor recruitment and screening
To minimise the risk of COVID-19 infection of donors and recipients, we suggest specific changes in the pathway for donor recruitment and screening, principally including the evaluation of clinical history, laboratory testing and checks on the day of donation. For hospital-based stool banks, donors should also sign an informed consent, or at least be thoroughly informed by the physicians (according to local rules) to accept the potential risk of being infected with COVID-19 when they come to the hospital for testing and donation.21
The suggestions below are similar to those already released by some regulatory institutions (eg, the US Food and Drug Administration22 and the Italian National Transplant Centre23) and differ slightly from those previously released by our group.24 Such measures should be adapted to local healthcare systems and updated accordingly with further evidence on COVID-19.
Questionnaire and clinical history
Although the initial clinical assessment and questionnaire administration are usually carried out in the FMT centres, in the COVID-19 era they can be generally implemented via telemedicine to avoid unnecessary exposure of potential donors to the hospital. The donor health questionnaire should be sent earlier to the candidate donor electronically, and the interview can be conducted through a video/phone consultation. For hospital-based stool banks, healthcare visits should be kept only on a case-to-case scenario, based on the physician's discretion (eg, clinical issues, technical obstacles, need for a cultural-linguistic mediator) or on donor desire for healthcare visit (eg, impossibility for a confidential interview in a reserved space at home).
Additional items should be included in the clinical questionnaire. First, physicians should specifically assess if the donor has been diagnosed with laboratory-confirmed SARS-CoV-2 infection or has been closely exposed to subjects with suspected or proven infection.
In addition, potential donors should be clinically assessed for COVID-19 including, as suggested by the Center for Disease Control and Prevention (CDC)25: fever, cough, dyspnoea, chills, anosmia or ageusia, sore throat, muscle pain not explainable by alternative diagnosis within the previous 30 days.26 If the potential donor has any symptoms suggestive of COVID-19, he/she should be temporarily excluded from the next stage of the laboratory screening and donation process. Moreover, healthcare workers actively involved in the management of patients should be excluded too.
Laboratory testing
All donors who pass the questionnaire should undergo laboratory examinations.12 Specific testing for the detection of SARS-CoV-2 must be added to the standard panel of donor laboratory testing,12 including at least nasopharyngeal swab and reverse transcription polymerase chain reaction (RT-PCR) assay and serology.27 Where available, validated molecular stool testing should be performed on the donated material (figure 2), and efforts from centres to include it in the donor screening are strongly advocated. All subjects who test positive must be temporarily excluded from donation, and advised of the result and to take precautionary measures against transmission, based on local protocols.

{kind=link}
{kind=link}
Proposed workflow of stool donation during the COVID-19 pandemic.
Some considerations about COVID-19 testing are necessary. First, there is no diagnostic testing so far that guarantees full accuracy of the diagnosis of COVID-19, nor can a single testing be used for all stages of the disease, so the examinations should be combined at different time points of the donor screening. Moreover, there is only limited evidence on COVID-19 diagnostics, so our suggestions could be updated once more consolidated data are available. These diagnostic limits should be discussed with the recipient.
So far, the nasopharyngeal swab is the most commonly used test for diagnosis of pulmonary COVID-19. Viral RNA in the nasopharyngeal swab is detectable from a few days before start of the symptoms, peaks within the first week of symptom onset, and starts to decline by week 3, becoming subsequently undetectable.27 Serological diagnosis is especially important to intercept subjects with few or late symptoms where the nasopharyngeal swab could be less sensitive.
IgM and IgG ELISA have been found to be positive from day 4 after symptom onset, with a peak after 2–3 weeks from the start of the infection28 29; specifically, IgM lowers at week 5 and disappears from week 7 of the illness, while IgG persists beyond week 7.30
Combined nasopharyngeal swab and IgM testing have been shown to increase diagnostic accuracy, so we recommend using them together to screen donors.31 However, the long-term persistence of antibodies remains unknown.
The screening of donor stools through a molecular test for SARS-CoV-2 has been advocated as the safest way forward to prevent the potential risk of viral transmission.14 However, although there is recent evidence that SARS-CoV-2 can be found in faeces32 and that it actively infects human gut enterocytes,33 it is not yet clear if the presence of faecal viral particles indicates infectivity, and if asymptomatic serologically positive individuals can also shed the virus that way. Moreover, several studies report on longer faecal excretion than nasopharyngeal route (table 1).28 32 34–39 Recently, local protocols for stool SARS-CoV-2 viral quantification have become available, and quantification has yielded promising results.40
Studies evaluating the presence of SARS-CoV-2 in faecal samples or anal/rectal swabs
Based on these considerations, positivity of PCR on nasopharyngeal swab/stool and/or IgM serology should be absolute criteria for exclusion from donation for at least 8 weeks; after that time frame, the potential donor could be considered again and re-tested. In case of IgG seroconversion for SARS-CoV-2, a donor should be excluded for 30 days and then re-tested with questionnaire and molecular stool testing; thereafter, if negative for stool testing and symptom-free, the donor should be allowed to donate.
Finally, as the COVID-19 diagnostics are still evolving, these suggestions should be updated as soon as further evidence is gained and new tests (eg, those on saliva) are developed.
Donation workflow and quarantine
The donation workflow is summarised in figure 2. Potential donors who pass the questionnaire and laboratory testing described above can start providing faecal material. A dedicated toilet at the stool bank should be reserved for stool collection, and high-touch surface areas should be cleaned after each donation. If not operationally possible, stool should be collected at home with standard recommendations.12
At each donation, donors should be checked, beyond the standardised questionnaire already suggested,12 for: diagnosis of SARS-CoV-2 infection; household exposure to subjects with suspected or proven infections; clinical symptoms of COVID-19 (as described above) not explainable by alternative diagnosis, since the last donation. Donors who prove to be positive for one of these items must be excluded from donation and previously donated stool, up to 4 weeks before the occurrence of symptoms/COVID-19 diagnosis, should be discarded as initial evidence suggests that SARS-CoV-2 is able to remain in stools up to 4 weeks after infection.36
For each donor, donated stools must be either: (1) immediately manufactured into FMT preparations, frozen and stored at −80°C, and finally quarantined until that donor has passed a further donor screening (to be repeated every 8–12 weeks) at the end of a period of donation, and be available for administration to patients only after this further check; or (2) assessed directly with validated molecular stool testing for common pathogens and for SARS-CoV-2. In this case, if direct testing is negative, they can be released for use without the need for quarantine, as recommended in our previous guidelines.12
Stool manufacturing
Broadly, there are two models for preparing FMT: patient-selected fresh FMT or frozen FMT manufactured by a stool bank from healthy donors. However, due to factors related to safety, access and economics, the frozen FMT model manufactured by stool banks is widely adopted by clinicians.41 42
Although rare clinical scenarios may require the use of fresh FMT prior to COVID-19, to date the fresh FMT model should be avoided to facilitate close adherence to recommended safety measures during the COVID-19 pandemic.43 Although the infectivity of RNA-positive SARS-CoV-2 stool is unknown, preliminary data suggest that viral shedding in the stool takes approximately 2–4 weeks,36 gastrointestinal symptoms commonly precede respiratory symptoms,44 and viral shedding in stool may lag behind despite clearance in respiratory samples.32 36
These data confirm the need for best practices in the manufacturing of FMT preparations. In our previous consensus report we recommended high-quality microbiology facilities (at least biosafety level 2) with robust standard operating procedures that allow safe processing of human samples by trained staff.12 Additionally, appropriate documentation, robust quality processes, retention of donor samples for further checks and standards for release of the final product are recommended.12 13 45 46 Therefore, as high safety measures were already recommended by previous guidelines,12 no significant changes in the stool manufacturing working protocol are currently needed to deal adequately with COVID-19.
FMT procedure and follow-up
Routes of FMT delivery: which is best during COVID-19?
Endoscopic FMT routes are most commonly used worldwide. Overall, endoscopic procedures have the potential to facilitate the transmission of virus to healthcare workers and patients (due to the close distance between patients and physicians, exposure to splashes, mucus or saliva during upper endoscopy, potential oral–faecal transmission during lower endoscopy, or by creating aerosol), although early real-world data suggest that the risk of viral transmission through endoscopy may be low.47 48
For these reasons it is prudent to create a process by which risks are minimised. Professional societies have released guidelines on gastrointestinal endoscopy and the use of personal protective equiptment (PPE) for these procedures in the setting of COVID-19.3 5 When FMT is administered via colonoscopy, it is recommended that the strict procedures to minimise risk before, during and after the procedure be followed (detailed in the section below). The only method of FMT delivery which does not generate aerosol is the ingestion of encapsulated donor stool. This is the preferred method, when available, to minimise transmission risks and usage of PPE which may be in limited supply. However, we acknowledge that capsulised FMT is still not widely available for use at all centres.
Delivery by retention enema would be less likely to be aerosol generating and can be performed by a single healthcare provider, minimising their exposure and PPE utilisation, but efficacy appears lower than endoscopic administration6 and patients may need multiple treatment courses, which would increase their exposure to the healthcare environment. FMT via nasoenteric or colonic transendoscopic enteral tube is used widely in some centres, particularly in elderly hospitalised patients. The otolaryngology literature considers procedures of the head and neck to be high risk in patients with confirmed or suspected COVID-19.49 The nose and nasopharyx have been shown to be reservoirs of high concentrations of the SARS-CoV-2 virus,50 and placement of the tube through the nasopharynx could cause particles to become aerosolised. Adequate topical analgesia to make the procedure comfortable for the patient and minimise coughing, gagging and sneezing is recommended. Furthermore, staff numbers present should be minimised. Those present should wear full PPE, including N95 masks and face shields/goggles, gloves, hair nets, and dedicated operating room or procedural areas, ideally with negative pressure, are advised.
Generally, it is advisable that FMT centres determine preferred routes of delivery on a case-by-case basis and according to their expertise in one or another route.
Endoscopic procedures
Several scientific societies have issued recommendations for healthcare facilities providing elective procedures.4 5 51 Restrictions will vary based on country or state, and local considerations should be identified and followed. When FMT is being performed in an endoscopy unit, the following procedures are advisable to minimise risk to staff and other patients.
Patient triage: Patients scheduled for outpatient elective endoscopic FMT should have temperature checked and be questioned about symptoms including fever, cough, dyspnoea, chills, anosmia or ageusia, sore throat and muscle pain on arrival for the procedure and prior to entering the facility. In patients who are suspected of, or have a known diagnosis of COVID-19, the physician should assess if the procedure is postponable based on the clinical picture of the patient and, in case, he/she should be instructed to perform a nasopharyngeal swab and to resume oral vancomycin to prevent recurrence.
The outcome of these checks must be tracked in an appropriate register.
Patients who present with symptoms suggestive of COVID-19 should be asked to contact their primary care provider for further evaluation. Patients should be given a cloth or surgical facemask to wear on arrival at the facility and strict social distancing should be maintained in waiting room areas, with chairs at least 2 metres apart. Visitors/family members should be prohibited from remaining on site and can be telephoned afterwards to meet the patient at the door at time of discharge.
PPE: It is recommended that all patients, healthcare providers and staff wear surgical facemasks at all times. FMT procedures involving mucous membranes including nasoenteric tube insertion, upper endoscopy or colonoscopy require N95 masks and face shields to be worn by proceduralists and any members of the healthcare team present. Staff should be educated on the proper methods for donning and removing PPE.
Recovery room: Patients should ideally recover in the room in which the procedure is conducted, which can then be terminally cleaned before being used for the next patient. If space does not permit, then the patient should be recovered in an area in which social distancing can be maintained (at least 2 metres between patients). There is no sound basis for asking patients to retain donor material for longer than is necessary to recover from sedation.
Follow-up
Patients should be called 24 hours after the procedure to assess any short-term adverse events or procedural complications. Follow-up appointments should be conducted using telemedicine as per institutional protocols, when possible. Follow-up evaluations at different time points (between 1 and 8 weeks) are advisable to discuss post-FMT symptoms, assess for signs of recurrence and enquire about symptoms of infection.43 52 Patients should be instructed to contact the provider immediately if symptoms of infection develop or if they are diagnosed with COVID-19 within 28 days of the procedure so that contact tracing and monitoring of exposed staff can be performed, as well as 'look-back' testing of retained donor stool samples. If patients develop diarrhoea suggestive of CDI recurrence, they can be triaged by telephone to determine whether they need to seek care at the hospital or whether they can submit stool for testing and/or start empiric anti-CDI therapy at home. Those whose prior CDI episodes have been severe or who report diarrhoea suggestive of CDI recurrence together with high fevers, severe abdominal pain or vomiting should be evaluated in an emergency room or physician's office. If the conditions and indication exist, further treatment with FMT may be considered.
Research activities
The enormous potential impact of COVID-19 on many facets of research (including the undertaking of clinical trials) has already been recognised.53 54 This clearly applies to the very active field of FMT clinical trials. Specifically, prior to the COVID-19 pandemic there were >300 trials involving FMT registered on www.clinicaltrials.gov, involving a myriad of indications from autism to ulcerative colitis.55–57 In the months leading up to the current pandemic there were two important safety alerts from the USA relating to the possible transfer of pathogens to patients via FMT, resulting in one death and five hospitalisations.13 58 Before those undertaking FMT research were able to fully respond to the last alert, the COVID-19 pandemic struck and FMT trial activity has been currently paused in most regions.
However, as the most realistic scenario is the medium to longer cohabitation with COVID-19, FMT-related research should take adequate security measures rather than being suspended, despite potential complexity.
To guarantee the best possible safety based on current evidence, ongoing trials should adapt their protocols according to the changing status of COVID-19, and upcoming trials should be designed taking into account the same security measures proposed in this document for clinical practice.
For specific patient populations, including those with inflammatory bowel disease (IBD) treated with immunosuppressive medication or cancer patients on chemotherapy, exposure to a healthcare facility for FMT administration may be difficult. For example, patients with IBD living in high prevalence areas for COVID-19 have been recommended to ‘shield’ from public activity by government-mandated advice and professional guidelines59 60 to minimise the risk of infection.
Additionally, the panel discussed solutions to keep a smooth patient recruitment in FMT clinical trials. To avoid enrolment hurdles and to safely perform follow-up, virtual visits (especially those after treatment) should be considered rather than in-person assessments.59 61 Moreover, where possible, potentially eligible candidates should be provided with specific documentation (eg, the ticket of the scheduled visit) to be able to reach the hospital without being stopped by authorities if unnecessary movements are not allowed during the lockdown phase.
Furthermore, for FMT trials there should be a pragmatic ongoing dialogue between trial investigators and the ethical, funding and administrative bodies overseeing the study to ensure that studies can still proceed safely and effectively, although with potential adaptations; this may require flexibility in study protocols, review of appropriate and achievable endpoints (eg, length of participant follow-up) and consideration of unblinding if required. To ensure the safety of patients, also taking into account recent FMT-related adverse events in the context of clinical trials,58 it is recommended that donor recruitment protocols and workflows follow international guidelines.12 The use of multi-donor FMT could potentially increase the risk of COVID-19 transmission and should only be considered within a FMT trial if there is strict adherence to proposed security measures. The development of a reliable stool assay for SARS-CoV2 is also advocated to make the implementation of clinical trials faster and safer and, when available, such diagnostic tools should be included in the screening protocols.
As suggested for clinical practice, the use of frozen stools is preferred over fresh material, although SARS-CoV-2 can probably survive the storage conditions. The manipulation of faecal aliquots and the storage of stool samples before and after FMT should be done in a highly safe environment (at least biosafety level 2). Additionally, members of the FMT staff who are in charge of sample handling should undergo, in the COVID-19 era, a more rigorous safety training as there is a potential risk of being exposed to SARS-CoV-2.
The use of registers and the application of the same strict traceability protocols that have been recommended for clinical practice are also recommended for research protocols.12
Finally, these principles for assessing SARS-CoV-2, designed for standard FMT, are also recommended to be applied to trials investigating next-generation microbiome drugs which are directly derived from human faeces (while it is not necessary for synthetically derived ones).
Conclusions
The COVID-19 pandemic is challenging the healthcare systems of individual countries worldwide, and it is reasonable to assume that it will be present also in the near future, forcing us to adapt overall clinical-procedural standards. Therefore, we have learnt to rationalise medical care services with criteria dictated first by the emergency and then by reasoned planning, with varying degrees of difficulty in different clinical scenarios.
In that context, FMT finds its place as a life-saving procedure for a considerable number of patients with CDI which, despite COVID-19, will continue to be numerous in clinical practice.
The general workflow of a FMT service, as recommended before the diffusion of COVID-19,12 already allows guaranteeing high levels of safety, both for physicians and for patients. Due to their robust organisation, FMT services can adapt to the pandemic-related scenario, and a few feasible security measures, which are described in this position paper (table 2) are advocated to assure a safe cohabitation with COVID-19 in the near future. However, we recognise that certain recommendations here represent expert opinion rather than clear evidence-based practice and that, given the rapid developments occurring in evidence related to COVID-19 pathophysiology, they may need updating in the future to maintain the highest safety levels for FMT services.
Summary of recommendations
Acknowledgments
GC, GI and LM received grants in the field of faecal microbiota transplantation from the Italian Ministry of Health. BHM is the recipient of a National Institute of Health Research (NIHR) Academic Clinical Lectureship. The Division of Digestive Diseases at Imperial College London received financial and infrastructure support from the NIHR Imperial Biomedical Research Centre (BRC) based at Imperial College Healthcare NHS Trust and Imperial College London.
References
Footnotes
Twitter @gianluca1aniro, @jonathansegal1985, @GiovanniCammar9
Contributors GC conceived the idea of the project. GC and GI organised and designed the project, selected the expert panel and established the main topics. GC, GI, CRK, BHM and ZK wrote the initial draft of the manuscript. All panel members read and revised the manuscript for important intellectual content and approved the final manuscript.
Funding The project was in part funded by the Catholic University of Rome, Line D-1 research funding.
Competing interests AG reports personal fees for consultancy from Eisai Srl, 3PSolutions, Real Time Meeting, Fondazione Istituto Danone, Sinergie Srl, Board MRGE and Sanofi SpA personal fees for acting as a speaker for Takeda SpA, AbbVie and Sandoz SpA and personal fees for acting on advisory boards for VSL3 and Eisai. BHM reports personal fees from Finch Therapeutics Group. CRK has served as a clinical advisor, with no financial compensation, for OpenBiome since 2013; she is a local principal investigator for the PRISM-3 clinical trial, for which her institution receives some salary support for a research coordinator and compensation from Finch Therapeutics Group for each patient enrolled. FZ reports grants from the non-profit China Microbiota Transplantation System (fmtBank) and has a patent for GenFMTer for separating microbiota issued to FMT medical. GC has received personal fees for acting as advisor for Ferring Therapeutics. GI has received personal fees for acting as speaker from Biocodex, Danone, Metagenics, and for acting as consultant/advisor from Ferring Therapeutics, Giuliani, Metagenics. HS reports personal fees from Danone, Enterome, Takeda, AbbVie, Roche, Amgen, Danone, BiomX, Ferring, BMS, Astellas, MSD, Novartis, Tillotts Pharma, and Biose, and grants from Biocodex, Danone and BiomX, and is a co-founder of Exeliom Biosciences. JJK and EJK report grants from Vedanta Biosciences. JRA reports personal fees from Finch Therapeutics and has a non-financial relationship with OpenBiome as a scientific advisor. MF reports personal fees from Finch Therapeutics Group, Rebiotix, Takeda, AbbVie and Janssen. SCN reports grants from Ferring and personal fees from Takeda, AbbVie, Janssen and Tillotts. SPC reports non-financial support from Janssen and personal fees from Shire, Ferring, Microbiotica and Pfizer. ZK is an employee and shareholder of Finch Therapeutics and is an unpaid special advisor for OpenBiome.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement There are no data in this work.