
Impact of Local and Demographic Factors on Early COVID-19 Vaccine Hesitancy among Health Care Workers in New York City Public Hospitals

 , , , , ,
, , , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Settings and Survey Participants
2.2. Survey
2.3. Random Forest Analysis
2.4. Statistical Analysis
3. Results
3.1. Study Population
3.2. Vaccine Status
3.3. Demographics
3.4. Education and Hospital Role
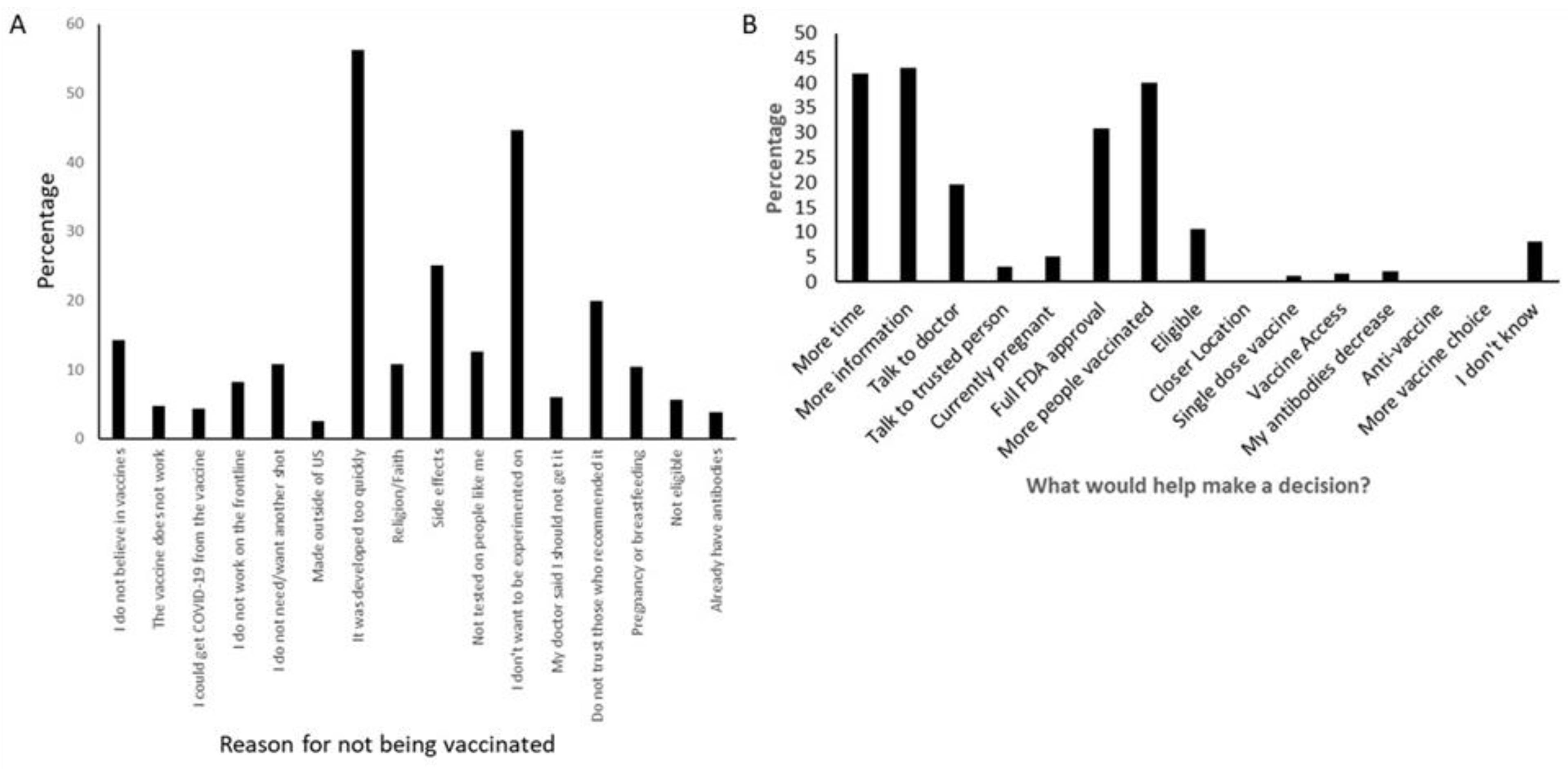
3.5. Reasons for Hesitancy towards the COVID-19 Vaccine
3.6. Machine Learning Analysis
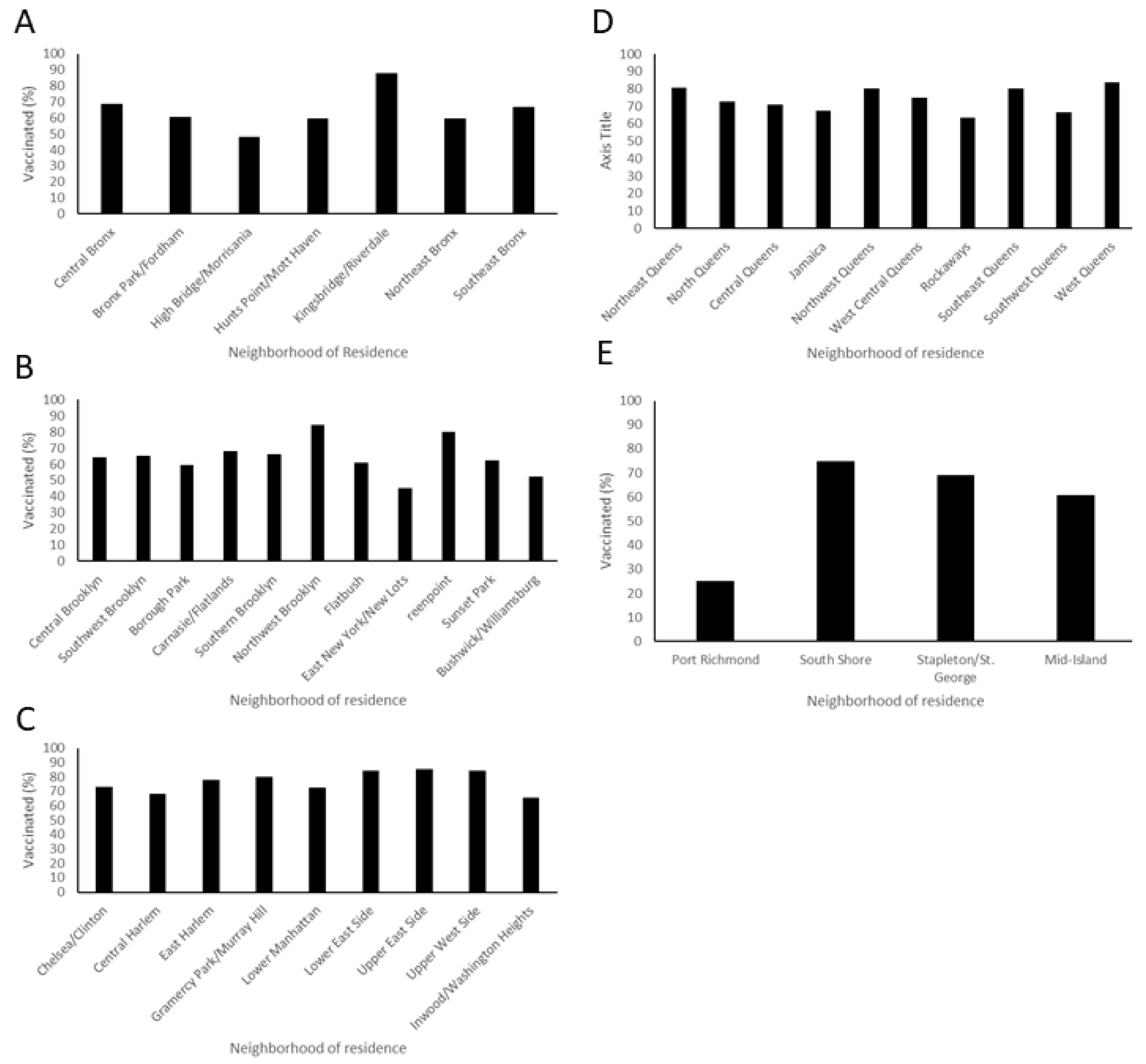
3.7. Location of Respondents
4. Discussion
4.1. Demographics and COVID-19 Vaccine Hesitancy
4.2. Location of Work and Home
4.3. First-Hand Experience with Serious COVID-19 Cases
4.4. Changing Attitudes over Time
4.5. Strategies for Intervention
4.6. Limitations
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Greenwood, B. The contribution of vaccination to global health: Past, present and future. Philos. Trans. R. Soc. B Biol. Sci. 2014, 369, 20130433. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ciardi, F.; Menon, V.; Jensen, J.L.; Shariff, M.A.; Pillai, A.; Venugopal, U.; Kasubhai, M.; Dimitrov, V.; Kanna, B.; Poole, B.D. Knowledge, Attitudes and Perceptions of COVID-19 Vaccination among Healthcare Workers of an Inner-City Hospital in New York. Vaccines 2021, 9, 516. [Google Scholar] [CrossRef] [PubMed]
- Dzieciolowska, S.; Hamel, D.; Gadio, S.; Dionne, M.; Gagnon, D.; Robitaille, L.; Cook, E.; Caron, I.; Talib, A.; Parkes, L.; et al. COVID-19 vaccine acceptance, hesitancy, and refusal among Canadian healthcare workers: A multicenter survey. Am. J. Infect. Control 2021, 49, 1152–1157. [Google Scholar] [CrossRef] [PubMed]
- Trogen, B.; Pirofski, L.A. Understanding vaccine hesitancy in COVID-19. Medcine 2021, 2, 498–501. [Google Scholar] [CrossRef] [PubMed]
- ECDC. Coronavirus Disease 2019 (COVID-19) in the EU/EEA and the UK; European Center for Disease Prevention and Control: Stockholm, Switzerland, 2020. [Google Scholar]
- Heyerdahl, L.W.; Dielen, S.; Nguyen, T.; Van Riet, C.; Kattumana, T.; Simas, C.; Vandaele, N.; Vandamme, A.M.; Vandermeulen, C.; Giles-Vernick, T.; et al. Doubt at the core: Unspoken vaccine hesitancy among healthcare workers. Lancet Reg. Health Eur. 2021, 12, 100289. [Google Scholar] [CrossRef] [PubMed]
- Azarpanah, H.; Farhadloo, M.; Vahidov, R.; Pilote, L. Vaccine hesitancy: Evidence from an adverse events following immunization database, and the role of cognitive biases. BMC Public Health 2021, 21, 1686. [Google Scholar] [CrossRef] [PubMed]
- Paris, C.; Bénézit, F.; Geslin, M.; Polard, E.; Baldeyrou, M.; Turmel, V.; Tadié, É.; Garlantezec, R.; Tattevin, P. COVID-19 vaccine hesitancy among healthcare workers. Infect. Dis. Now. 2021, 51, 484–487. [Google Scholar] [CrossRef]
- Di Gennaro, F.; Murri, R.; Segala, F.V.; Cerruti, L.; Abdulle, A.; Saracino, A.; Bavaro, D.F.; Fantoni, M. Attitudes towards Anti-SARS-CoV2 Vaccination among Healthcare Workers: Results from a National Survey in Italy. Viruses 2021, 13, 371. [Google Scholar] [CrossRef]
- Neumann-Böhme, S.; Varghese, N.E.; Sabat, I.; Barros, P.P.; Brouwer, W.; Van Exel, J.; Schreyögg, J.; Stargardt, T. Once we have it, will we use it? A European survey on willingness to be vaccinated against COVID-19. Eur. J. Health Econ. 2020, 21, 977–982. [Google Scholar] [CrossRef]
- Lazarus, J.V.; Ratzan, S.C.; Palayew, A.; Gostin, L.O.; Larson, H.J.; Rabin, K.; Kimball, S.; El-Mohandes, A. A global survey of potential acceptance of a COVID-19 vaccine. Nat. Med. 2020, 20, 1–4. [Google Scholar] [CrossRef]
- Gallè, F.; Sabella, E.A.; Roma, P.; Da Molin, G.; Diella, G.; Montagna, M.T.; Ferracuti, S.; Liguori, G.; Orsi, G.B.; Napoli, C. Acceptance of COVID-19 Vaccination in the Elderly: A Cross-Sectional Study in Southern Italy. Vaccines 2021, 9, 1222. [Google Scholar] [CrossRef]
- Lin, C.; Tu, P.; Beitsch, L.M. Confidence and Receptivity for COVID-19 Vaccines: A Rapid Systematic Review. Vaccines 2021, 9, 16. [Google Scholar] [CrossRef] [PubMed]
- El-Mohandes, A.; White, T.M.; Wyka, K.; Rauh, L.; Rabin, K.; Kimball, S.H.; Ratzan, S.C.; Lazarus, J.V. COVID-19 vaccine acceptance among adults in four major US metropolitan areas and nationwide. Sci. Rep. 2021, 11, 21844. [Google Scholar] [CrossRef] [PubMed]
- Des Jarlais, D.C.; Cooper, H.L.F.; Arasteh, K.; Feelemyer, J.; McKnight, C.; Ross, Z. Potential geographic "hotspots" for drug-injection related transmission of HIV and HCV and for initiation into injecting drug use in New York City, 2011–2015, with implications for the current opioid epidemic in the US. PLoS ONE 2018, 13, e0194799. [Google Scholar] [CrossRef]
- Sullivan, G.M.; Feinn, R. Using Effect Size-or Why the P Value Is Not Enough. J. Grad. Med. Educ. 2012, 4, 279–282. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Carrieri, V.; Lagravinese, R.; Resce, G. Predicting vaccine hesitancy from area-level indicators: A machine learning approach. Health Econ. 2021, 30, 3248–3256. [Google Scholar] [CrossRef] [PubMed]
- Salmon, A.; Dudley, M.Z.; Glanz, J.M.; Omer, S.B. Vaccine hesitancy: Causes, consequences, and a call to action. Vaccine 2015, 33 (Suppl. S4), D66–D71. [Google Scholar] [CrossRef] [PubMed]
- Leask, J.; Kinnersley, P.; Jackson, C.; Cheater, F.; Bedford, H.; Rowles, G. Communicating with parents about vaccination: A framework for health professionals. BMC Pediatr. 2012, 12, 154. [Google Scholar] [CrossRef]
- McClure, C.C.; Cataldi, J.R.; O’Leary, S.T. Vaccine hesitancy: Where We are and where we are going. Clin. Ther. 2018, 39, 1550–1562. [Google Scholar] [CrossRef] [Green Version]
- Beleche, T.; Ruhter, J.; Kolbe, A.; Marus, J.; Bush, L.; Sommers, B. Available online: https://aspe.hhs.gov/sites/default/files/private/pdf/265341/aspe-ib-vaccine-hesitancy.pdf (accessed on 6 January 2022).
- Vaux, S.; Fonteneau, L.; Gautier, A. Ouverture vaccinale antigrippale chez les professionnels de santé. Bull. Sante Publique 2019, 10, 8. [Google Scholar]
- Available online: https://www1.nyc.gov/site/doh/covid/covid-19-data-vaccines.page#people (accessed on 2 January 2022).
- Giambi, C.; Fabiani, M.; D’Ancona, F.; Ferrara, L.; Fiacchini, D.; Gallo, T.; Martinelli, D.; Pascucci, M.G.; Prato, R.; Filia, A.; et al. Parental vaccine hesitancy in Italy_results from a national survey. Vaccine 2018, 36, 779–787. [Google Scholar] [CrossRef] [PubMed]
- Available online: https://aspe.hhs.gov/sites/default/files/2021-08/unvaccinated-but-willing-ib.pdf (accessed on 2 January 2022).
- Artiga, S.; Rae, M.; Pham, O.; Hamel, L.; Muñana, C. Available online: https://www.kff.org/racial-equity-and-health-policy/issue-brief/covid-19-risks-impacts-health-care-workers-race-ethnicity/ (accessed on 2 January 2022).
- Kwok, K.O.; Li, K.K.; Wei, W.I.; Tang, A.; Wong, S.Y.S.; Lee, S.S. Editor’s Choice: Influenza vaccine uptake, COVID-19 vaccination intention and vaccine hesitancy among nurses: A survey. Int. J. Nurs. Stud. 2021, 114, 103854. [Google Scholar] [CrossRef]
- Wainstock, T.; Yoles, I.; Sergienko, R.; Sheiner, E. Prenatal maternal COVID-19 vaccination and pregnancy outcomes. Vaccine 2021, 39, 6037–6040. [Google Scholar] [CrossRef] [PubMed]
- Wainstock, T.; Yoles, I.; Sergienko, R.; Sheiner, E.; CDC v-safe COVID-19 Pregnancy Registry Team. Preliminary findings of mRNA COVID-19 vaccine safety in pregnant persons. N. Engl. J. Med. 2021, 384, 2273–2282. [Google Scholar] [CrossRef] [PubMed]
- Anita Sreedhar and Anand Gopal. Available online: https://www.nytimes.com/2021/12/03/opinion/vaccine-hesitancy-covid.html (accessed on 6 January 2022).
- de Beaumont Foundation. Poll: The Language of Vaccine Acceptance. Available online: https://debeaumont.org/changing-the-covid-conversation/vaccineacceptance/ (accessed on 6 February 2022).
- Carrión, D.; Colicino, E.; Pedretti, N.F.A.; Arfur, K.B.; Rush, J.; DeFelice, N.; Just, A.C. Neighborhood-level disparities and subway utilization during the COVID-19 pandemic in New York City. Nat. Commun. 2021, 12, 3692. [Google Scholar] [CrossRef] [PubMed]
- COVID-19 Data Totals: NYC Public Health. Available online: https://www1.nyc.gov/site/doh/covid/covid-19-data-totals.page#boro (accessed on 10 August 2021).
- Pogue, K.; Jensen, J.L.; Stancil, C.K.; Ferguson, D.G.; Hughes, S.J.; Mello, E.J.; Burgess, R.; Berges, B.K.; Quaye, A.; Poole, B.D. Influences on Attitudes Regarding Potential COVID-19 Vaccination in the United States. Vaccines 2020, 8, 582. [Google Scholar] [CrossRef]
- AXIOS. Axios-Ipsos Poll: Americans Say J&J Pause Was the Right Call. Available online: https://www.axios.com/axios-ipsos-poll-johnson-and-johnson-vaccine-pause-a4eefe38-6aca-4a7e-b1d1-02e1b01a3480.html (accessed on 22 April 2021).
- Hamel, L.; Lopes, L.; Sparks, G.; Stokes, M.; Brodie, M. KFF COVID-19 Vaccine Monitor: April 2021. The Kaiser Family Foundation, 30 March 2021. Available online: https://www.kff.org/coronavirus-covid-19/poll-finding/kff-covid-19-vaccine-monitor-april-2021/ (accessed on 19 May 2021).
- Centers for Disease Control and Prevention. Vaccinate with Confidence. CDC’s Strategy to Reinforce Confidence in COVID-19 Vaccines, 12 December 2020. Available online: https://www.cdc.gov/vaccines/covid-19/downloads/vaccinate-with-confidence.pdf (accessed on 22 April 2021).
- Sherman, S.M.; Smith, L.E.; Sim, J.; Amlôt, R.; Cutts, M.; Dasch, H.; Rubin, G.J.; Sevdalis, N. COVID-19 vaccination intention in the UK: Results from the COVID-19 vaccination acceptability study (CoVAccS), a nationally representative cross-sectional survey. Hum. Vaccin. Immunother. 2021, 17, 1612–1621. [Google Scholar] [CrossRef]
- Raude, J. Vaccine hesitancy: Some insights from social and psychological sciences. Bull. Acad. Natl. Med. 2016, 200, 199–209. [Google Scholar]
- Vanni, G.; Materazzo, M.; Santori, F.; Pellicciaro, M.; Costesta, M.; Orsaria, P.; Cattadori, F.; Pistolese, C.A.; Perretta, T.; Chiocchi, M.; et al. The Effect of Coronavirus (COVID-19) on Breast Cancer Teamwork: A Multicentric Survey. In Vivo 2020, 34 (Suppl. S3), 1685–1694. [Google Scholar] [CrossRef]
- Coppeta, L.; Ferrari, C.; Somma, G.; Mazza, A.; D’Ancona, U.; Marcuccilli, F.; Grelli, S.; Aurilio, M.T.; Pietroiusti, A.; Magrini, A.; et al. Reduced Titers of Circulating Anti-SARS-CoV-2 Antibodies and Risk of COVID-19 Infection in Healthcare Workers during the Nine Months after Immunization with the BNT162b2 mRNA Vaccine. Vaccines 2022, 10, 141. [Google Scholar] [CrossRef]
- Menon, V.; Shariff, M.A.; Perez Gutierrez, V.; Carreño, J.M.; Yu, B.; Jawed, M.; Gossai, M.; Valdez, E.; Pillai, A.; Venugopal, U.; et al. Longitudinal humoral antibody response to SARS-CoV-2 infection among healthcare workers in a New York City hospital. BMJ Open 2021, 11, e051045. [Google Scholar] [CrossRef] [PubMed]
- Ricci, M.J.; Amorim, F. Ethical and Practical Considerations Surrounding Mandatory Vaccination. Infect. Control Today 2021, 25, 8. [Google Scholar]
- Gerretsen, P.; Kim, J.; Caravaggio, F.; Quilty, L.; Sanches, M.; Wells, S.; Brown, E.E.; Agic, B.; Pollock, B.G.; Graff-Guerrero, A. Individual determinants of COVID-19 vaccine hesitancy. PLoS ONE 2021, 16, e0258462. [Google Scholar] [CrossRef] [PubMed]
- Poyiadji, N.; Tassopoulos, A.; Myers, D.T.; Wolf, L.; Griffith, B. COVID-19 Vaccine Mandates: Impact on Radiology Department Operations and Mitigation Strategies. J. Am. Coll. Radiol. 2021, 21, 916–919. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Data | n | % |
|---|---|---|
| Age (n = 3493) | ||
| 18–24 | 77 | 2.2% |
| 25–34 | 692 | 19.8% |
| 35–44 | 746 | 21.4% |
| 45–54 | 817 | 23.4% |
| 55–54 | 880 | 25.2% |
| 65+ | 281 | 8.0% |
| Gender (n = 3491) | ||
| Female | 2491 | 71.4% |
| Male | 918 | 25.3% |
| Non-binary/third gender | 19 | 0.5% |
| Prefer not to answer | 63 | 1.8% |
| Ethnicity (n = 3474) | ||
| Hispanic or Latino/a/x | 698 | 20.1% |
| Non-Hispanic | 2776 | 79.9% |
| Race (n = 3632) | ||
| American Indian | 61 | 1.8% |
| Asian | 680 | 18.7% |
| Black or African | 942 | 25.9% |
| Hispanic, Latino | 257 | 7.1% |
| Pacific Islander or Native Hawaiian | 31 | 0.9% |
| White | 1492 | 41.0% |
| Mixed Race | 125 | 3.4% |
| Other | 19 | 0.5% |
| Prefer not to answer | 27 | 0.7% |
| Number of Children (n = 3421) | ||
| 0 | 1327 | 38.7% |
| 1 | 621 | 18.1% |
| 2 | 899 | 26.2% |
| More then 2 | 584 | 17.0% |
| Education (n = 3465) | ||
| Some secondary school | 6 | 0.2% |
| GED | 38 | 1.1% |
| High school diploma | 119 | 3.4% |
| Some college | 289 | 8.3% |
| Associate’s degree | 284 | 8.2% |
| Bachelor’s degree | 903 | 26.1% |
| Some graduate school | 137 | 4.0% |
| Master’s degree | 862 | 24.9% |
| Doctoral level | 820 | 23.7% |
| Other | 7 | 0.2% |
| Primary Role (n = 3287) | n | % |
|---|---|---|
| Physician/Attending | 562 | 17.1% |
| Administrative Support Staff | 507 | 15.4% |
| Central Office Administration | 222 | 6.8% |
| Hospital Police | 162 | 4.9% |
| Patient Care Associate | 160 | 4.9% |
| Nurse Practitioner | 91 | 2.8% |
| Nurse | 580 | 17.6% |
| Resident | 79 | 2.4% |
| Physician Assistant | 76 | 2.3% |
| Social Worker | 59 | 1.8% |
| Information Technology | 46 | 1.4% |
| Maintenance Staff | 25 | 0.8% |
| Environmental services | 25 | 0.8% |
| Hospital Administration | 23 | 0.7% |
| Medical Student | 20 | 0.6% |
| Dietary Services/Nutritionist | 10 | 0.3% |
| Other | 640 | 19.5% |
| Demographic Variable | Vaccinated | Hesitant | p Value | Refuser | p Value | Hesitant Effect Size (IQ) |
|---|---|---|---|---|---|---|
| Age group | <0.001 | <0.001 | ||||
| 18–24 | 34 (1%) | 14 (3%) | 12 (5%) | 2.91 | ||
| 25–34 | 471 (18%) | 99 (20%) | 51 (22%) | 0.36 | ||
| 35–44 | 509 (19%) | 101 (21%) | 78 (34%) | 0.36 | ||
| 45–54 | 592 (22%) | 107 (22%) | 42 (83%) | −0.36 | ||
| 55–64 | 664 (25%) | 103 (21%) | 23 (10%) | −0.73 | ||
| >65 | 235 (9%) | 19 (4%) | 5 (2%) | −2.91 | ||
| Race | <0.001 | <0.001 | ||||
| Native American | 19 (0.8%) | 7 (1.6%) | 3 (1%) | 0.45 | ||
| Asian | 547 (22%) | 40 (9.2%) | 7 (3%) | −1.25 | ||
| Black | 486 (20%) | 188 (43%) | 103 (49%) | 0.45 | ||
| Hispanic | 174 (7%) | 34(8%) | 22 (11%) | −0.45 | ||
| Native Hawaiian | 17 (1%) | 5 (1%) | 2 (1%) | 0.15 | ||
| White | 1167 (47%) | 145 (33%) | 60 (29%) | −0.85 | ||
| Mixed | 47 (2%) | 11 (2%) | 4 (2%) | −0.15 | ||
| Other | 10 (0.4%) | 4 (1%) | 2 (1%) | 0.55 | ||
| Gender | <0.001 | <0.001 | ||||
| Female | 1723 (64%) | 348 (71%) | 166 (72%) | −0.35 | ||
| Male | 735 (27%) | 73 (15%) | 36 (16%) | −0.90 | ||
| Non binary | 10 (0.4%) | 6 (1%) | 2 (1%) | 0.98 | ||
| prefer not to answer | 36 (1%) | 15 (3%) | 10 (4%) | 0.35 |
| Vaccinated | Hesitant | p Value | Refused | p Value | Hesitant Effect Size | |
|---|---|---|---|---|---|---|
| Education | <0.001 | <0.001 | ||||
| Some high school | 5 (0.2%) | 1 (0.2%) | 0 | −0.17 | ||
| GED | 19 (1%) | 10 (2%) | 5 (2.2%) | 1.04 | ||
| High school diploma | 70 (3%) | 24 (5%) | 7 (3%) | 1.04 | ||
| Some college | 174 (6%) | 49 (10%) | 36 (16%) | 0.17 | ||
| Associates degree | 177 (7%) | 49 (10%) | 27 (12%) | 0.17 | ||
| Bachelor’s degree | 600 (22%) | 137 (28%) | 67 (29%) | −0.17 | ||
| Some graduate school | 91 (3%) | 20 (4%) | 9 (4%) | −0.17 | ||
| Master’s degree | 605 (23%) | 113 (23%) | 41 (18%) | −0.52 | ||
| Doctoral degree | 744 (28%) | 30 (6%) | 14 (6%) | −2.43 | ||
| Other | 3 (0.1%) | 2 (0.4%) | 2.9 (1%) | 1.22 | ||
| Primary Role | Vaccinated | Hesitant | p < 0.001 | Refused | p < 0.001 | |
| Medical staff | 820 (31%) | 30 (6%) | 16 (7%) | −0.76 | ||
| Nursing and support staff | 502 (19%) | 110 (22%) | 56 (24%) | 0 | ||
| Maintenance/Environmental staff | 32 (1%) | 6 (1%) | 5 (2.2%) | −0.12 | ||
| Hospital Administrative staff | 662 (25%) | 203 (41%) | 83 (36%) | 0.29 | ||
| Clinical support staff | 348 (13%) | 36 (7%) | 23 (10%) | −0.41 | ||
| Hosp Police | 9 (0.3%) | 6 (1%) | 8 (3%) | 0.59 | ||
| Community Outreach tracers | 38 (1%) | 19 (4%) | 2 (1%) | 0.94 | ||
| Pharmacy | 38 (1%) | 4 (1%) | 3 (1.3%) | −0.41 | ||
| Other | 0 | 2 (1%) | 2 (1%) | 2 |
| Question | Mean Decrease Gini |
|---|---|
| How has your experience with COVID-19 changed your overall opinion on vaccinations? | 8.2 |
| Which best describes your primary role at work? | 7.97 |
| What is your age group? | 5.86 |
| What is your highest level of formal education? | 4.58 |
| Based on your overall experience how serious is COVID-19? | 2.72 |
| Where do you work? | 2.35 |
| How many children do you have? | 2.16 |
| What is your gender? | 1.41 |
| I worry that I cannot pay for the vaccine now or in the future | 1.16 |
| Are you Hispanic or Latino? | 0.71 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Afzal, A.; Shariff, M.A.; Perez-Gutierrez, V.; Khalid, A.; Pili, C.; Pillai, A.; Venugopal, U.; Kasubhai, M.; Kanna, B.; Poole, B.D.; et al. Impact of Local and Demographic Factors on Early COVID-19 Vaccine Hesitancy among Health Care Workers in New York City Public Hospitals. Vaccines 2022, 10, 273. https://doi.org/10.3390/vaccines10020273
Afzal A, Shariff MA, Perez-Gutierrez V, Khalid A, Pili C, Pillai A, Venugopal U, Kasubhai M, Kanna B, Poole BD, et al. Impact of Local and Demographic Factors on Early COVID-19 Vaccine Hesitancy among Health Care Workers in New York City Public Hospitals. Vaccines. 2022; 10(2):273. https://doi.org/10.3390/vaccines10020273
Chicago/Turabian StyleAfzal, Afsheen, Masood A. Shariff, Victor Perez-Gutierrez, Amnah Khalid, Christina Pili, Anjana Pillai, Usha Venugopal, Moiz Kasubhai, Balavenkatesh Kanna, Brian D. Poole, and et al. 2022. "Impact of Local and Demographic Factors on Early COVID-19 Vaccine Hesitancy among Health Care Workers in New York City Public Hospitals" Vaccines 10, no. 2: 273. https://doi.org/10.3390/vaccines10020273