
Increased Prevalence of Neuropsychiatric Disorders during COVID-19 Pandemic in People Needing a Non-Deferrable Neurological Evaluation



Abstract
:1. Introduction
2. Materials and Methods
3. Results
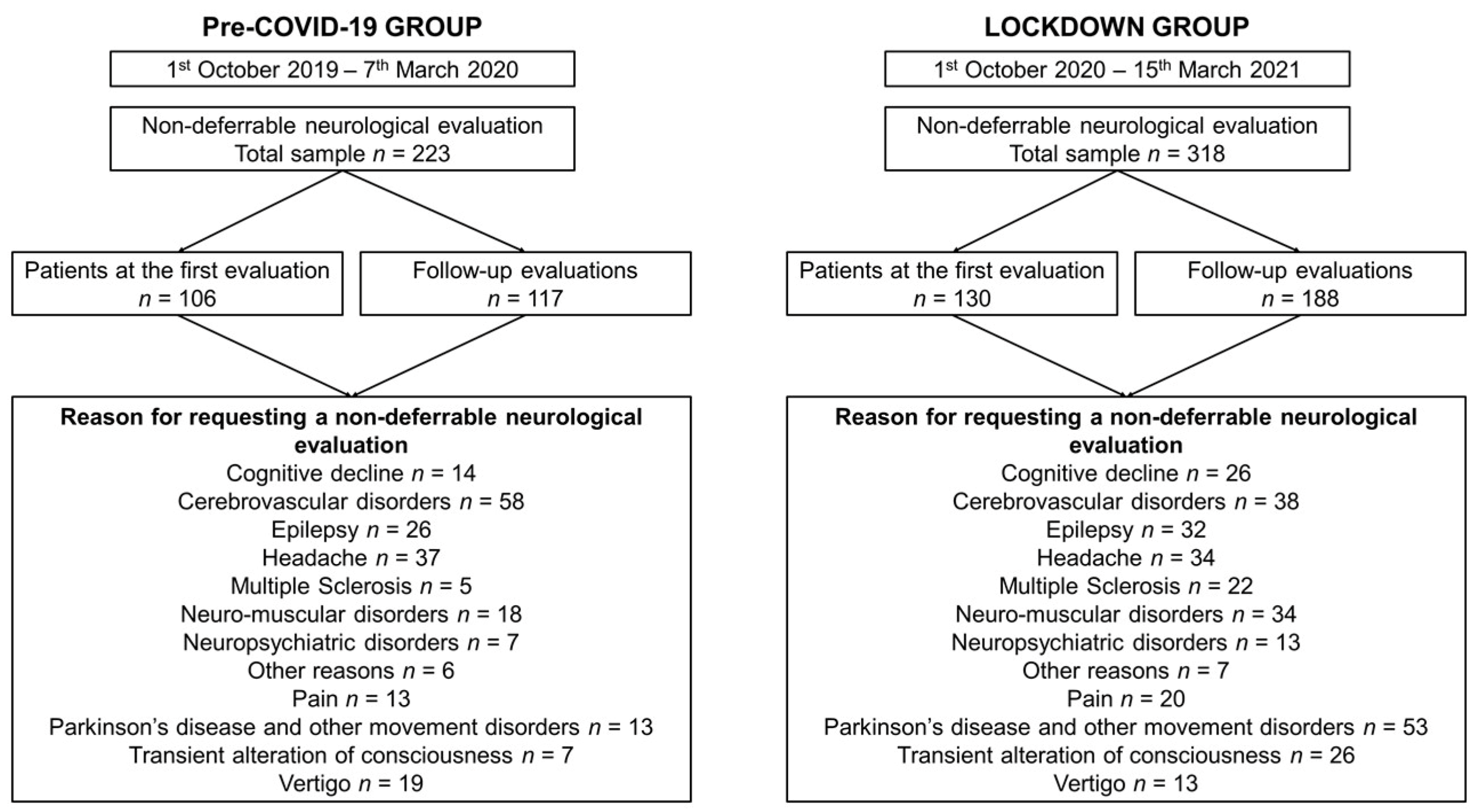
3.1. Demographics and Clinical Features
3.2. Differences in Reasons for Requesting a Non-Deferrable Neurological Evaluation
3.3. Differences in the Prevalence of Diagnoses at Discharge
3.4. Appropriateness of the Non-Deferrable Neurological Evaluations
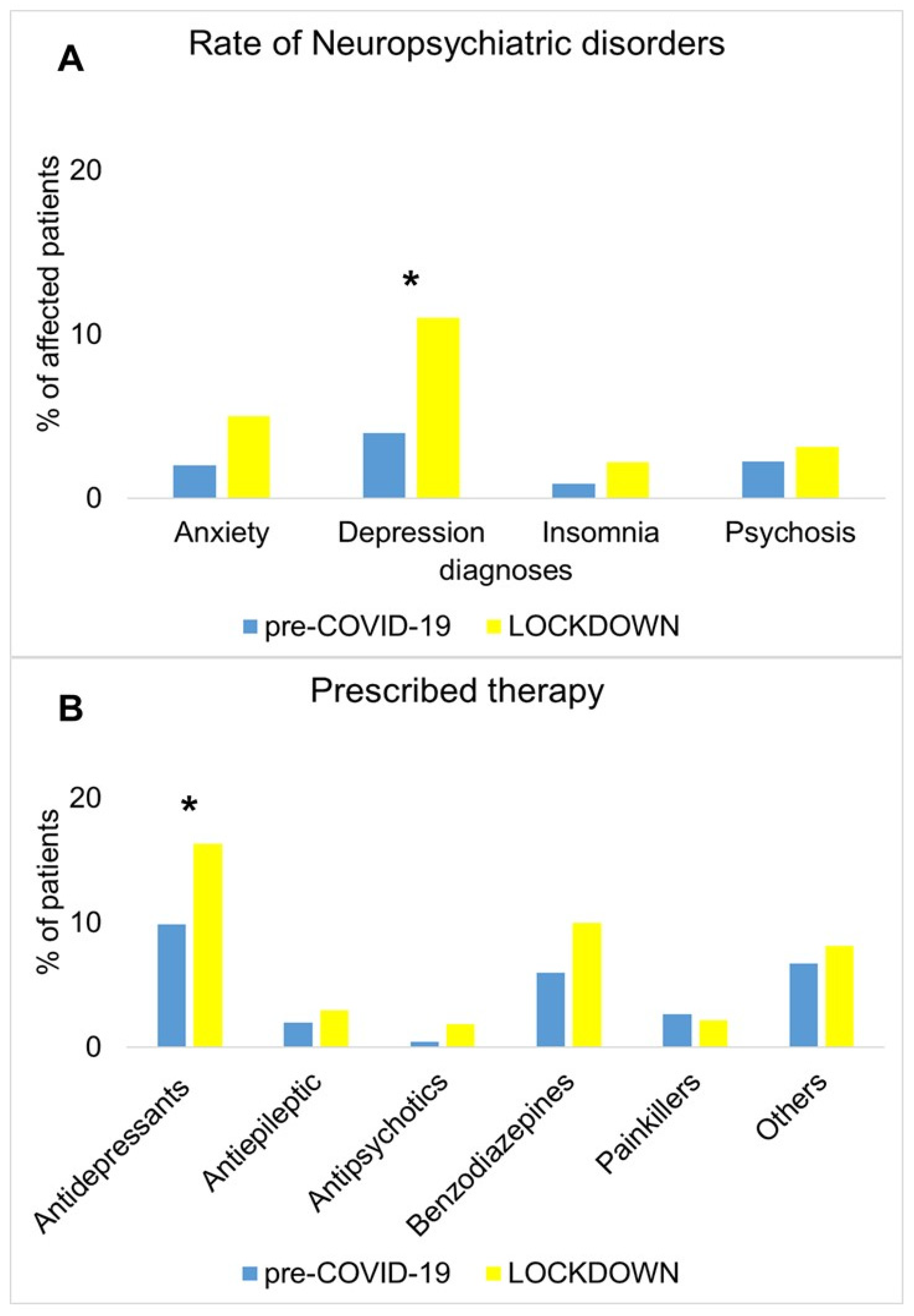
3.5. Subanalysis of NPSs and Prescribed Therapy
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Willan, J.; King, A.J.; Jeffery, K.; Bienz, N. Challenges for NHS hospitals during covid-19 epidemic. BMJ 2020, 368, m1117. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Proudfoot, A.G.; O’Brien, B.; Schilling, R.; Gould, D.W.; McGlennan, A.; Wragg, A.; Knight, C.; McAuliffe, S.; Marshall, G.; Orzechowska, I.; et al. Rapid establishment of a COVID-19 critical care unit in a convention centre: The Nightingale Hospital London experience. Intensive Care Med. 2021, 47, 349–351. [Google Scholar] [CrossRef] [PubMed]
- Prasad, S.; Holla, V.V.; Neeraja, K.; Surisetti, B.K.; Kamble, N.; Yadav, R.; Pal, P.K. Impact of Prolonged Lockdown due to COVID-19 in Patients with Parkinson’s Disease. Neurol. India 2020, 68, 792. [Google Scholar] [PubMed]
- Costabile, T.; Carotenuto, A.; Lavorgna, L.; Borriello, G.; Moiola, L.; Inglese, M.; Petruzzo, M.; Trojsi, F.; Ianniello, A.; Nozzolillo, A.; et al. COVID-19 pandemic and mental distress in multiple sclerosis: Implications for clinical management. Eur. J. Neurol. 2021, 28, 3375–3383. [Google Scholar] [CrossRef] [PubMed]
- Motolese, F.; Rossi, M.; Albergo, G.; Stelitano, D.; Villanova, M.; Di Lazzaro, V.; Capone, F. The Psychological Impact of COVID-19 Pandemic on People with Multiple Sclerosis. Front. Neurol. 2020, 11, 580507. [Google Scholar] [CrossRef]
- Esselin, F.; De La Cruz, E.; Pageot, N.; Juntas-Moralès, R.; Alphandéry, S.; Camu, W. Increased worsening of amyotrophic lateral sclerosis patients during Covid-19-related lockdown in France. Amyotroph. Lateral Scler. Front. Degener. 2021, 12, 1–3. [Google Scholar] [CrossRef]
- Gobbi, S.; Płomecka, M.B.; Ashraf, Z.; Radziński, P.; Neckels, R.; Lazzeri, S.; Dedić, A.; Bakalović, A.; Hrustić, L.; Skórko, B.; et al. Worsening of Preexisting Psychiatric Conditions During the COVID-19 Pandemic. Front. Psychiatry 2020, 11, 581426. [Google Scholar] [CrossRef]
- Tondo, G.; Sarasso, B.; Serra, P.; Tesser, F.; Comi, C. The Impact of the COVID-19 Pandemic on the Cognition of People with Dementia. Int. J. Environ. Res. Public Health 2021, 18, 4285. [Google Scholar] [CrossRef]
- Delmastro, M.; Zamariola, G. Depressive symptoms in response to COVID-19 and lockdown: A cross-sectional study on the Italian population. Sci. Rep. 2020, 10, 1–10. [Google Scholar] [CrossRef]
- Berardi, C.; Antonini, M.; Genie, M.G.; Cotugno, G.; Lanteri, A.; Melia, A.; Paolucci, F. The COVID-19 pandemic in Italy: Policy and technology impact on health and non-health outcomes. Health Policy Technol. 2020, 9, 454–487. [Google Scholar] [CrossRef]
- Chirico, F.; Sacco, A.; Nucera, G.; Magnavita, N. Coronavirus disease 2019: The second wave in Italy. J. Health Res. 2021, 35, 359–363. [Google Scholar] [CrossRef]
- Kutlu, Ö.; Güneş, R.; Coerdt, K.; Metin, A.; Khachemoune, A. The effect of the “stay-at-home” policy on requests for dermatology outpatient clinic visits after the COVID-19 outbreak. Dermatol. Ther. 2020, 33, e13581. [Google Scholar] [CrossRef] [PubMed]
- Onesti, C.E.; Rugo, H.S.; Generali, D.; Peeters, M.; Zaman, K.; Wildiers, H.; Harbeck, N.; Martin, M.; Cristofanilli, M.; Cortes, J.; et al. Oncological care organisation during COVID-19 outbreak. ESMO Open 2020, 5, e000853. [Google Scholar] [CrossRef]
- Allevi, F.; Dionisio, A.; Baciliero, U.; Balercia, P.; Beltramini, G.A.; Bertossi, D.; Bozzetti, A.; Califano, L.; Cascone, P.; Colombo, L.; et al. Impact of COVID-19 epidemic on maxillofacial surgery in Italy. Br. J. Oral Maxillofac. Surg. 2020, 58, 692–697. [Google Scholar] [CrossRef] [PubMed]
- Ziadé, N.; Hmamouchi, I.; El Kibbi, L.; Abdulateef, N.; Halabi, H.; Abutiban, F.; Hamdi, W.; El Rakawi, M.; Eissa, M.; Masri, B. The impact of COVID-19 pandemic on rheumatology practice: A cross-sectional multinational study. Clin. Rheumatol. 2020, 39, 3205–3213. [Google Scholar] [CrossRef] [PubMed]
- Cao, Y.-G.; Li, Y.; Shen, J.; Shao, M.-M.; Lin, X.-D.; Zhu, J.-J.; Huang, X.-Y.; Cheng, Z.-C.; Yan, J.-Y.; Chen, K.-Y. Clinical activity changes in the neurology department of Wenzhou during the COVID-19 pandemic: An observational analysis. Neurol. Sci. 2021, 42, 1653–1659. [Google Scholar] [CrossRef]
- Hsia, R.Y.; Niedzwiecki, M. Avoidable emergency department visits: A starting point. Int. J. Qual. Health Care 2017, 29, 642–645. [Google Scholar] [CrossRef]
- Honigman, L.S.; Wiler, J.L.; Rooks, S.; Ginde, A.A. National Study of Non-urgent Emergency Department Visits and Associated Resource Utilization. West. J. Emerg. Med. 2013, 14, 609–616. [Google Scholar] [CrossRef]
- Sacco, S.; Ricci, S.; Ornello, R.; Eusebi, P.; Petraglia, L.; Toni, D.; Rota, E.; Bruzzone, G.; Testa, L.; Bongioanni, R.; et al. Reduced Admissions for Cerebrovascular Events During COVID-19 Outbreak in Italy. Stroke 2020, 51, 3746–3750. [Google Scholar] [CrossRef] [PubMed]
- Zhao, J.; Li, H.; Kung, D.; Fisher, M.; Shen, Y.; Liu, R. Impact of the COVID-19 Epidemic on Stroke Care and Potential Solutions. Stroke 2020, 51, 1996–2001. [Google Scholar] [CrossRef] [PubMed]
- Rudilosso, S.; Laredo, C.; Vera, V.; Vargas, M.; Renú, A.; Llull, L.; Obach, V.; Amaro, S.; Urra, X.; Torres, F.; et al. Acute stroke care is at risk in the era of COVID-19: Experience at a comprehensive stroke center in Barcelona. Stroke 2020, 51, 1991–1995. [Google Scholar] [CrossRef]
- Thornton, J. Stroke: “striking reductions” are seen in number of people with symptoms seeking help. BMJ 2020, 369, m1406. [Google Scholar] [CrossRef] [Green Version]
- Aguiar de Sousa, D.; Sandset, E.C.; Elkind, M.S.V. The curious case of the missing strokes during the COVID-19 pandemic. Am. Heart Assoc. 2020, 51, 1921–1923. [Google Scholar]
- Helmich, R.C.; Bloem, B.R. The Impact of the COVID-19 Pandemic on Parkinson’s Disease: Hidden Sorrows and Emerging Opportunities. J. Park. Dis. 2020, 10, 351–354. [Google Scholar] [CrossRef] [Green Version]
- Shalash, A.; Roushdy, T.; Essam, M.; Fathy, M.; Dawood, N.L.; Abushady, E.M.; Elrassas, H.; Helmi, A.; Hamid, E. Mental Health, Physical Activity, and Quality of Life in Parkinson’s Disease During COVID-19 Pandemic. Mov. Disord. 2020, 35, 1097–1099. [Google Scholar] [CrossRef]
- Hamdy, S.M.; Abdel-Naseer, M.; Shehata, H.S.; Hassan, A.; Elmazny, A.; Shalaby, N.M.; Abokrysha, N.T.; Kishk, N.A.; Nada, M.A.F.; Ahmed, S.M.; et al. Managing Disease-Modifying Therapies and Breakthrough Activity in Multiple Sclerosis Patients During the COVID-19 Pandemic: Toward an Optimized Approach. Ther. Clin. Risk Manag. 2020, 16, 651–662. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Shi, L.; Que, J.; Lu, Q.; Liu, L.; Lu, Z.; Xu, Y.; Liu, J.; Sun, Y.; Meng, S.; et al. The impact of quarantine on mental health status among general population in China during the COVID-19 pandemic. Mol. Psychiatry 2021, 1–10. [Google Scholar] [CrossRef]
- Rossell, S.L.; Neill, E.; Phillipou, A.; Tan, E.J.; Toh, W.L.; Van Rheenen, T.E.; Meyer, D. An overview of current mental health in the general population of Australia during the COVID-19 pandemic: Results from the COLLATE project. Psychiatry Res. 2021, 296, 113660. [Google Scholar] [CrossRef]
- Burke, T.; Berry, A.; Taylor, L.K.; Stafford, O.; Murphy, E.; Shevlin, M.; McHugh, L.; Carr, A. Increased Psychological Distress during COVID-19 and Quarantine in Ireland: A National Survey. J. Clin. Med. 2020, 9, 3481. [Google Scholar] [CrossRef]
- Shah, S.M.A.; Mohammad, D.; Qureshi, M.F.H.; Abbas, M.Z.; Aleem, S. Prevalence, Psychological Responses and Associated Correlates of Depression, Anxiety and Stress in a Global Population, During the Coronavirus Disease (COVID-19) Pandemic. Community Ment. Health J. 2021, 57, 101–110. [Google Scholar] [CrossRef]
- Naldi, A.; Vallelonga, F.; Di Liberto, A.; Cavallo, R.; Agnesone, M.; Gonella, M.; Sauta, M.D.; Lochner, P.; Tondo, G.; Bragazzi, N.L.; et al. COVID-19 pandemic-related anxiety, distress and burnout: Prevalence and associated factors in healthcare workers of North-West Italy. BJPsych Open 2021, 7, e27. [Google Scholar] [CrossRef]
- Maciaszek, J.; Ciulkowicz, M.; Misiak, B.; Szczesniak, D.; Luc, D.; Wieczorek, T.; Fila-Witecka, K.; Gawlowski, P.; Rymaszewska, J. Mental Health of Medical and Non-Medical Professionals during the Peak of the COVID-19 Pandemic: A Cross-Sectional Nationwide Study. J. Clin. Med. 2020, 9, 2527. [Google Scholar] [CrossRef] [PubMed]
- Wańkowicz, P.; Szylińska, A.; Rotter, I. Insomnia, Anxiety, and Depression Symptoms during the COVID-19 Pandemic May Depend on the Pre-Existent Health Status Rather than the Profession. Brain Sci. 2021, 11, 1001. [Google Scholar] [CrossRef]
- Wańkowicz, P.; Szylińska, A.; Rotter, I. The Impact of the COVID-19 Pandemic on Psychological Health and Insomnia among People with Chronic Diseases. J. Clin. Med. 2021, 10, 1206. [Google Scholar] [CrossRef] [PubMed]
- Van der Heide, A.; Meinders, M.J.; Bloem, B.R.; Helmich, R.C. The impact of the COVID-19 pandemic on psychological distress, physical activity, and symptom severity in Parkinson’s disease. J. Parkinsons Dis. 2020, 10, 1355–1364. [Google Scholar] [CrossRef]
- Cagnin, A.; Di Lorenzo, R.; Marra, C.; Bonanni, L.; Cupidi, C.; Laganà, V.; Rubino, E.; Vacca, A.; Provero, P.; Isella, V.; et al. Behavioral and Psychological Effects of Coronavirus Disease-19 Quarantine in Patients with Dementia. Front. Psychiatry 2020, 11, 916. [Google Scholar] [CrossRef]
- De Girolamo, G.; Cerveri, G.; Clerici, M.; Monzani, E.; Spinogatti, F.; Starace, F.; Tura, G.; Vita, A. Mental health in the coronavirus disease 2019 emergency—The Italian response. JAMA Psychiatry 2020, 77, 974–976. [Google Scholar] [CrossRef]
- Upadhyay, A.K.; Shukla, S. Correlation study to identify the factors affecting COVID-19 case fatality rates in India. Diabetes Metab. Syndr. Clin. Res. Rev. 2021, 15, 993–999. [Google Scholar] [CrossRef]
- Penlioglou, T.; Stoian, A.P.; Papanas, N. Diabetes, Vascular Aging and Stroke: Old Dogs, New Tricks? J. Clin. Med. 2021, 10, 4620. [Google Scholar] [CrossRef]
- Stasiolek, M. Neurological symptoms and signs in thyroid disease. Thyroid Res. 2015, 8, A25. [Google Scholar] [CrossRef] [Green Version]
- Tondo, G.; De Marchi, F.; Terazzi, E.; Prandi, P.; Sacchetti, M.; Comi, C.; Cantello, R. Chronic obstructive pulmonary disease may complicate Alzheimer’s disease: A comorbidity problem. Neurol. Sci. 2018, 39, 1585–1589. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Group | Pre-COVID-19 (n = 223) | LOCKDOWN (n = 318) | p Value |
|---|---|---|---|
| Age mean ± SD (years) | 62.8 ± 17.4 | 60.6 ± 17.3 | 0.154 |
| Sex female, N (%) | 111 (50%) | 170 (53%) | 0.399 |
| First evaluation N (%) | 106 (48%) | 130 (41%) | 0.125 |
| Reason for requesting a non-deferrable neurological evaluation N (%) | |||
| Cognitive decline | 14 (6%) | 26 (8%) | 0.406 |
| CVDs | 58 (26%) | 38 (12%) | 0.000 ** |
| Epilepsy | 26 (12%) | 32 (10%) | 0.555 |
| Headache | 37 (17%) | 34 (11%) | 0.045 * |
| MS | 5 (2%) | 22 (7%) | 0.014 * |
| NM disorders | 18 (8%) | 34 (11%) | 0.309 |
| NPSs | 7 (3%) | 13 (4%) | 0.565 |
| Other | 6 (3%) | 7 (2%) | 0.714 |
| Pain | 13 (6%) | 20 (6%) | 0.826 |
| PD and other MDs | 13 (6%) | 53 (17%) | 0.000 ** |
| TAC | 7 (3%) | 26 (8%) | 0.016 * |
| Vertigo | 19 (8%) | 13 (4%) | 0.031 * |
| Prevalence of diagnosis at discharge N (%) | |||
| Cognitive decline | 13 (6%) | 20 (6%) | 0.826 |
| CVDs | 49 (22%) | 31 (10%) | 0.000 ** |
| Epilepsy | 29 (13%) | 36 (11%) | 0.553 |
| Primary headache | 35 (16%) | 28 (9%) | 0.014 * |
| MS | 3 (1%) | 20 (6%) | 0.005 ** |
| NM disorders | 29 (13%) | 44 (14%) | 0.780 |
| No diagnosis | 14 (6%) | 12 (4%) | 0.180 |
| Non-neurological | 12 (5%) | 17 (5%) | 0.986 |
| NPSs | 16 (7%) | 57 (18%) | 0.000 ** |
| Other | 10 (4%) | 15 (5%) | 0.899 |
| PD, ET and other MDs | 13 (6%) | 38 (12%) | 0.016 * |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tondo, G.; Aprile, D.; Tesser, F.; Comi, C. Increased Prevalence of Neuropsychiatric Disorders during COVID-19 Pandemic in People Needing a Non-Deferrable Neurological Evaluation. J. Clin. Med. 2021, 10, 5169. https://doi.org/10.3390/jcm10215169
Tondo G, Aprile D, Tesser F, Comi C. Increased Prevalence of Neuropsychiatric Disorders during COVID-19 Pandemic in People Needing a Non-Deferrable Neurological Evaluation. Journal of Clinical Medicine. 2021; 10(21):5169. https://doi.org/10.3390/jcm10215169
Chicago/Turabian StyleTondo, Giacomo, Davide Aprile, Fabiana Tesser, and Cristoforo Comi. 2021. "Increased Prevalence of Neuropsychiatric Disorders during COVID-19 Pandemic in People Needing a Non-Deferrable Neurological Evaluation" Journal of Clinical Medicine 10, no. 21: 5169. https://doi.org/10.3390/jcm10215169