
COVID-19: A Cross-Sectional Study of Healthcare Students’ Perceptions of Life during the Pandemic in the United States and Brazil

 ,
,  and
and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Sample Characteristics
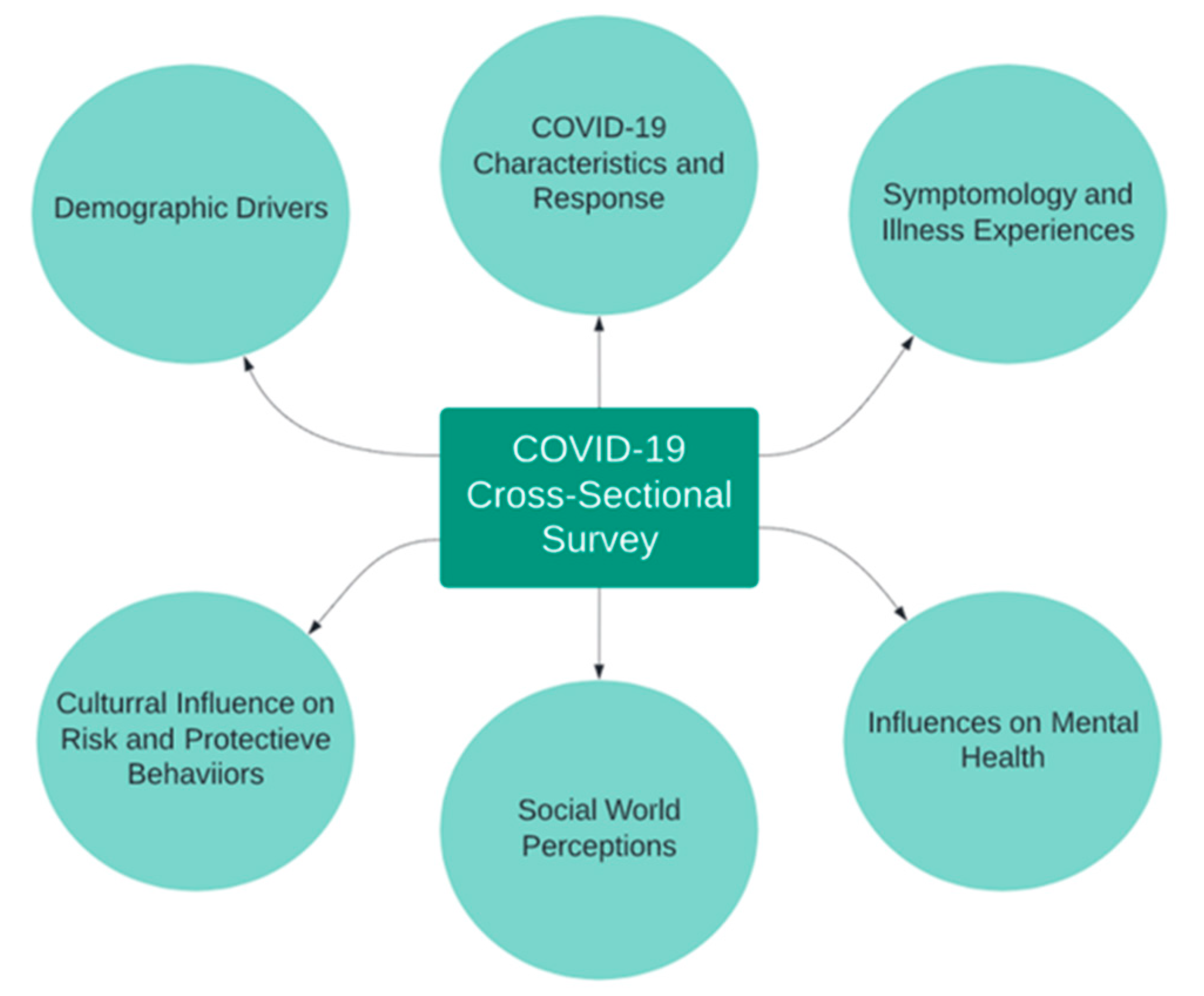
2.2. Survey Development and Implementation
2.3. Statistical Methods
3. Results
3.1. Demographics
3.2. COVID-19 Physical Characteristics and Symptomatology
3.3. Risk and Protective Behaviors
3.4. Social World and Mental Health
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Browning, M.H.E.M.; Larson, L.R.; Sharaievska, I.; Rigolon, A.; McAnirlin, O.; Mullenbach, L.; Cloutier, S.; Vu, T.M.; Thomsen, J.; Reigner, N.; et al. Psychological impacts from COVID-19 among university students: Risk factors across seven states in the United States. PLoS ONE 2021, 16, e0245327. [Google Scholar] [CrossRef] [PubMed]
- Blake, H.; Knight, H.; Jia, R.; Corner, J.; Morling, J.R.; Denning, C.; Ball, J.K.; Bolton, K.; Figueredo, G.; Morris, D.E.; et al. Students’ Views towards Sars-Cov-2 Mass Asymptomatic Testing, Social Distancing and Self-Isolation in a University Setting during the COVID-19 Pandemic: A Qualitative Study. Int. J. Environ. Res. Public Health 2021, 18, 4182. [Google Scholar] [CrossRef] [PubMed]
- Schlesselman, L.S.; Cain, J.; DiVall, M. Improving and Restoring the Well-being and Resilience of Pharmacy Students during a Pandemic. Am. J. Pharm. Educ. 2020, 84, ajpe8144. [Google Scholar] [CrossRef] [PubMed]
- Belian, R.; Leite, L.; Lima-Filho, J.; Geer, L.A. Facing Global Health Crises Using Mobile Communications: An international virtual exchange experience. eLearn 2020. [Google Scholar] [CrossRef]
- Wang, C.; Horby, P.W.; Hayden, F.G.; Gao, G.F. A novel coronavirus outbreak of global health concern. Lancet 2020, 395, 470–473. [Google Scholar] [CrossRef] [Green Version]
- Cucinotta, D.; Vanelli, M. WHO Declares COVID-19 a Pandemic. Acta Biomed. 2020, 91, 157–160. [Google Scholar] [CrossRef] [PubMed]
- Stawicki, S.P.; Jeanmonod, R.; Miller, A.C.; Paladino, L.; Gaieski, D.F.; Yaffee, A.Q.; De Wulf, A.; Grover, J.; Papadimos, T.J.; Bloem, C.; et al. The 2019–2020 Novel Coronavirus (Severe Acute Respiratory Syndrome Coronavirus 2) Pandemic: A Joint American College of Academic International Medicine-World Academic Council of Emergency Medicine Multidisciplinary COVID-19 Working Group Consensus Paper. J. Glob. Infect. Dis. 2020, 12, 47–93. [Google Scholar] [CrossRef] [PubMed]
- Maslow, A.H. Motivation and Personality; Prabhat Prakashan: New Delhi, India, 1987. [Google Scholar]
- Sorci, G.; Faivre, B.; Morand, S. Explaining among-country variation in COVID-19 case fatality rate. Sci. Rep. 2020, 10, 18909. [Google Scholar] [CrossRef] [PubMed]
- Bruns, D.P.; Kraguljac, N.V.; Bruns, T.R. COVID-19: Facts, Cultural Considerations, and Risk of Stigmatization. J. Transcult. Nurs. 2020, 31, 326–332. [Google Scholar] [CrossRef] [PubMed]
- Airhihenbuwa, C.O.; Iwelunmor, J.; Munodawafa, D.; Ford, C.L.; Oni, T.; Agyemang, C.; Mota, C.; Ikuomola, O.B.; Simbayi, L.; Fallah, M.P.; et al. Culture Matters in Communicating the Global Response to COVID-19. Prev. Chronic Dis. 2020, 17, E60. [Google Scholar] [CrossRef] [PubMed]
- Johns Hopkins Coronavirus Resource Center. Mortality Analyses. Available online: https://coronavirus.jhu.edu/data/mortality (accessed on 9 July 2021).
- Mazumder, A.; Bandhu Kalanidhi, K.; Sarkar, S.; Ranjan, P.; Sahu, A.; Kaur, T.; Kaur, D.; Bhattacharya, A.; Priyadarshini Suna, S.; Prakash, B.; et al. Psycho-social and behavioural impact of COVID 19 on young adults: Qualitative research comprising focused group discussion and in-depth interviews. Diabetes Metab. Syndr. 2021, 15, 309–312. [Google Scholar] [CrossRef] [PubMed]
- Papadimos, T.J.; Soghoian, S.E.; Nanayakkara, P.; Singh, S.; Miller, A.C.; Saddikuti, V.; Jayatilleke, A.U.; Dubhashi, S.P.; Firstenberg, M.S.; Dutta, V.; et al. COVID-19 Blind Spots: A Consensus Statement on the Importance of Competent Political Leadership and the Need for Public Health Cognizance. J. Glob. Infect. Dis. 2020, 12, 167–190. [Google Scholar] [CrossRef] [PubMed]
- Kurian, S.J.; Bhatti, A.U.R.; Alvi, M.A.; Ting, H.H.; Storlie, C.; Wilson, P.M.; Shah, N.D.; Liu, H.; Bydon, M. Correlations Between COVID-19 Cases and Google Trends Data in the United States: A State-by-State Analysis. Mayo Clin. Proc. 2020, 95, 2370–2381. [Google Scholar] [CrossRef] [PubMed]
- Roberts, J.D.; Tehrani, S.O. Environments, Behaviors, and Inequalities: Reflecting on the Impacts of the Influenza and Coronavirus Pandemics in the United States. Int. J. Environ. Res. Public Health 2020, 17, 4484. [Google Scholar] [CrossRef] [PubMed]
- Guimarães, V.H.A.; de Oliveira-Leandro, M.; Cassiano, C.; Marques, A.L.P.; Motta, C.; Freitas-Silva, A.L.; de Sousa, M.A.D.; Silveira, L.A.M.; Pardi, T.C.; Gazotto, F.C.; et al. Knowledge About COVID-19 in Brazil: Cross-Sectional Web-Based Study. JMIR Public Health Surveill 2021, 7, e24756. [Google Scholar] [CrossRef] [PubMed]
- Johns Hopkins Coronavirus Resource Center. Understanding Vaccination Progress. Available online: https://coronavirus.jhu.edu/vaccines/international (accessed on 9 July 2021).
- Lieberman-Cribbin, W.; Tuminello, S.; Flores, R.M.; Taioli, E. Disparities in COVID-19 Testing and Positivity in New York City. Am. J. Prev. Med. 2020, 59, 326–332. [Google Scholar] [CrossRef] [PubMed]
- Bailenson, J.N. Nonverbal Overload: A Theoretical Argument for the Causes of Zoom Fatigue. Technol. Mind Behav. 2021, 2. [Google Scholar] [CrossRef]
- Grimes, D.A.; Schulz, K.F. Descriptive studies: What they can and cannot do. Lancet 2002, 359, 145–149. [Google Scholar] [CrossRef]
- Althubaiti, A. Information bias in health research: Definition, pitfalls, and adjustment methods. J. Multidiscip. Healthc. 2016, 9, 211–217. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
| United States (n = 53) | Brazil (n = 55) | p-Value | |
|---|---|---|---|
| Age | <0.001 | ||
| Mean (Range) | 29 (22–56) | 22 (17–31) | |
| Gender | 0.006 | ||
| Male | 11 (21%) | 27 (49%) | |
| Female | 41 (77%) | 28 (51%) | |
| Transgender Male | 1 (2%) | 0 | |
| Race | |||
| White | 8 (15%) | - | |
| Black or African American | 26 (49%) | - | |
| Asian | 10 (19%) | - | |
| Other | 9 (17%) | - | |
| Ethnicity | |||
| Hispanic or Latino/a | 45 (84%) | - | |
| Non-Hispanic or Latino/a | 6 (11%) | - | |
| Do Not know | 1 (2%) | - | |
| Prefer not to answer | 1 (2%) | - | |
| Born Outside the U.S. | <0.001 | ||
| No | 34 (64%) | 0 | |
| Yes | 19 (36%) | 55 (100%) | |
| Undergraduate/Graduate Course | <0.001 | ||
| Public Health | 45 (85%) | 0 | |
| Medicine | 5 (9%) | 51 (93%) | |
| MD/MPH | 1 (2%) | 0 | |
| Psychology | 2 (4%) | 4 (7%) | |
| Health Professional | <0.001 | ||
| No | 27 (51%) | 47 (86%) | |
| Yes | 26 (49%) | 8 (15%) | |
| Employed Before the Pandemic | <0.001 | ||
| No | 9 (17%) | 49 (91%) | |
| Yes | 44 (83%) | 5 (9%) | |
| Current Employment Status | <0.001 | ||
| Employed | 35 (67%) | 6 (11%) | |
| Unemployed | 17 (33%) | 48 (89%) | |
| Employment Satisfaction | 0.101 | ||
| Satisfied with Job | 16 (47%) | 5 (83%) | |
| Not Satisfied with Job | 18 (53%) | 1 (17%) | |
| Employment Seeking | <0.001 | ||
| Not Seeking Employment | 6 (35%) | 45 (94%) | |
| Seeking Employment | 11 (65%) | 3 (6%) |
| United States (n = 53) | Brazil (n = 55) | p-Value | |
|---|---|---|---|
| COVID-19 # of Symptoms1 | 0.840 | ||
| 0 | 23 (46%) | 19 (39%) | |
| 1–2 | 12 (24%) | 15 (31%) | |
| 3–4 | 9 (18%) | 8 (16%) | |
| 5–8 | 6 (12%) | 7 (14%) | |
| COVID-19 Symptoms Experienced2 | |||
| Fatigue | 17 | 15 | 0.325 |
| Headache | 13 | 16 | 0.696 |
| Loss of Taste or Smell | 11 | 6 | 0.087 |
| Sore Throat | 10 | 13 | 0.629 |
| Dry Cough | 10 | 12 | 0.819 |
| Fever | 8 | 10 | 0.764 |
| Difficulty Breathing or Shortness of Breath | 7 | 7 | 0.820 |
| Chest Pain or Pressure | 3 | 3 | 0.891 |
| Medication Taken for COVID-19 | 0.324 | ||
| No | 50 (94%) | 49 (89%) | |
| Yes | 3 (6%) | 6 (11%) | |
| COVID-19 Tests | <0.001 | ||
| No Tests Taken | 17 (32%) | 41 (75%) | |
| Negative Result | 29 (55%) | 10 (18%) | |
| Positive Result | 7 (13%) | 4 (7%) | |
| COVID-19 Test Availability | 0.012 | ||
| Not Widely Available | 4 (8%) | 15 (27%) | |
| Widely Available and Free of Cost | 40 (76%) | 26 (47%) | |
| Widely Available, but Not Free of Cost | 5 (9%) | 10 (18%) | |
| Do Not Know | 4 (8%) | 4 (7%) | |
| Agree with City/Region COVID-19 Policies | <0.001 | ||
| No | 3 (6%) | 12 (22%) | |
| Yes | 27 (51%) | 8 (15%) | |
| Partially | 19 (36%) | 27 (49%) | |
| Does Not Apply | 4 (8%) | 8 (15%) |
| United States (n = 53) | Brazil (n = 55) | p-Value | |
|---|---|---|---|
| Personal Risk Factors | 0.130 | ||
| None | 40 (76%) | 47 (86%) | |
| Asthma | 7 (13%) | 1 (2%) | |
| High Blood Pressure/Heart Disease | 1 (2%) | 0 | |
| Overweight/Obesity | 5 (9%) | 6 (11%) | |
| Smoking | 0 | 1 (2%) | |
| Most Important Risk Factor Opinion 1 | |||
| Crowded Places | 47 | 55 | 0.270 |
| People Without Masks | 42 | 40 | 0.428 |
| Closed Places Without Ventilation | 38 | 35 | 0.371 |
| Contaminated Shopped Items | 12 | 14 | 0.732 |
| Enough Sanitization at Places Frequented | 0.004 | ||
| No | 6 (11%) | 17 (31%) | |
| Yes | 32 (60%) | 17 (31%) | |
| Partially | 15 (28%) | 21 (38%) | |
| Enough Self-Sanitization | 0.069 | ||
| No | 6 (11%) | 9 (16%) | |
| Yes | 32 (60%) | 21 (38%) | |
| Partially | 15 (28%) | 25 (46%) | |
| Number of Sanitization Procedures Implemented | 0.249 | ||
| 1 | 14 (26%) | 13 (24%) | |
| 2–3 | 20 (38%) | 29 (53%) | |
| 4–5 | 19 (36%) | 13 (24%) | |
| Sanitization Procedures Implemented 1 | |||
| Alcohol 70% Gel | 31 | 41 | 0.077 |
| Alcohol 70% Spray | 30 | 40 | 0.079 |
| Soap | 40 | 40 | 0.745 |
| Household Bleach | 21 | 14 | 0.116 |
| Lysol-Type Sprays | 29 | 6 | <0.001 |
| Properly Using PPE | 0.121 | ||
| No | 0 | 1 | |
| Yes | 50 | 45 | |
| Partially | 3 | 9 | |
| Number of PPE Used | 0.002 | ||
| 1 | 15 (28%) | 35 (64%) | |
| 2 | 31 (59%) | 18 (33%) | |
| 3 | 6 (11%) | 1 (2%) | |
| 4 | 1 (2%) | 1 (2%) | |
| PPE Used 1 | |||
| Washable Mask | 40 | 52 | 0.005 |
| Disposable Mask | 48 | 22 | <0.001 |
| Face Shield | 8 | 3 | 0.098 |
| Disposable Cover | 3 | 1 | 0.291 |
| Pandemic Behavior | 0.001 | ||
| Staying at Home. All Needs Come from Delivery Services | 1 (2%) | 2 (4%) | |
| Staying at Home. Leave Only When Necessary | 16 (30%) | 34 (62%) | |
| Usually at Home. Leave to Meet Friends Sometimes | 12 (23%) | 13 (24%) | |
| Frequently Leave House by Choice Despite Pandemic | 6 (11%) | 1 (2%) | |
| Frequently Leave House for Work | 18 (34%) | 5 (9%) |
| United States (n = 53) | Brazil (n = 55) | p-Value | |
|---|---|---|---|
| Living Location | |||
| House/Apartment | 53 (100%) | 55 (100%) | |
| Household | 0.308 | ||
| Self | 3 (6%) | 1 (2%) | |
| Parents/Family | 42 (79%) | 50 (91%) | |
| Spouse/Partner | 4 (8%) | 1 (2%) | |
| Friends | 4 (8%) | 3 (6%) | |
| Attending In-Person Class | |||
| No | 53 (100%) | 54 (100%) | |
| Yes | 0 | 0 | |
| Reliable Internet | 0.556 | ||
| Always | 43 (81%) | 44 (80%) | |
| Sometimes | 9 (17%) | 11 (20%) | |
| Rarely | 1 (2%) | 0 | |
| Feeling Well about Home Environment | 0.998 | ||
| No | 2 (4%) | 2 (4%) | F |
| Yes | 33 (62%) | 34 (62%) | |
| Partially | 18 (34%) | 19 (35%) | |
| Social Relationships | 0.698 | ||
| Not Contacted Friends and Family | 5 (9%) | 3 (6%) | |
| Contacted Friends and Family Just A Few Times | 22 (42%) | 28 (51%) | |
| Contacted Friends and Family A Lot | 9 (17%) | 7 (13%) | |
| Contacted Friends and Family Regularly | 17 (32%) | 17 (31%) | |
| Social Relationship Difficulty1 | |||
| No Difficulty | 34 | 38 | 0.164 |
| Lack of Time | 13 | 11 | 0.571 |
| Lack of Availability | 11 | 6 | 0.160 |
| Lack of Volition | 8 | 17 | 0.051 |
| Lack of Reliable Internet/Technology | 2 | 3 | 0.678 |
| Feeling Around the Pandemic | 0.793 | ||
| Doing Well | 15 (28%) | 18 (33%) | |
| Living One Day at a Time | 24 (45%) | 23 (42%) | |
| Overwhelmed with Problems | 3 (6%) | 5 (9%) | |
| Going Through Difficulties | 4 (8%) | 5 (9%) | |
| Really Tough | 7 (13%) | 4 (7%) | |
| Mental Health | 0.624 | ||
| Never Had Counselling | 30 (57%) | 27 (49%) | |
| Regular Counselling and Have Continued | 4 (8%) | 5 (9%) | |
| Had Counselling My Lifetime | 13 (25%) | 19 (35%) | |
| Sought Counseling Since the Pandemic Started | 6 (11%) | 4 (7%) | |
| Employment Changes Impact on Mental Health | 0.275 | ||
| No Impact on Mental Health | 20 (41%) | 14 (58%) | |
| Impacted Mental Health | 13 (27%) | 6 (25%) | |
| Partially Impacted Mental Health | 16 (33%) | 4 (17%) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Geer, L.A.; Radigan, R.; Bruneli, G.d.L.; Leite, L.S.; Belian, R.B. COVID-19: A Cross-Sectional Study of Healthcare Students’ Perceptions of Life during the Pandemic in the United States and Brazil. Int. J. Environ. Res. Public Health 2021, 18, 9217. https://doi.org/10.3390/ijerph18179217
Geer LA, Radigan R, Bruneli GdL, Leite LS, Belian RB. COVID-19: A Cross-Sectional Study of Healthcare Students’ Perceptions of Life during the Pandemic in the United States and Brazil. International Journal of Environmental Research and Public Health. 2021; 18(17):9217. https://doi.org/10.3390/ijerph18179217
Chicago/Turabian StyleGeer, Laura A., Rachel Radigan, Guilherme de Lima Bruneli, Lucas Sampaio Leite, and Rosalie Barreto Belian. 2021. "COVID-19: A Cross-Sectional Study of Healthcare Students’ Perceptions of Life during the Pandemic in the United States and Brazil" International Journal of Environmental Research and Public Health 18, no. 17: 9217. https://doi.org/10.3390/ijerph18179217