
COVID-19 in Older Patients: Assessment of Post-COVID-19 Sarcopenia
 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
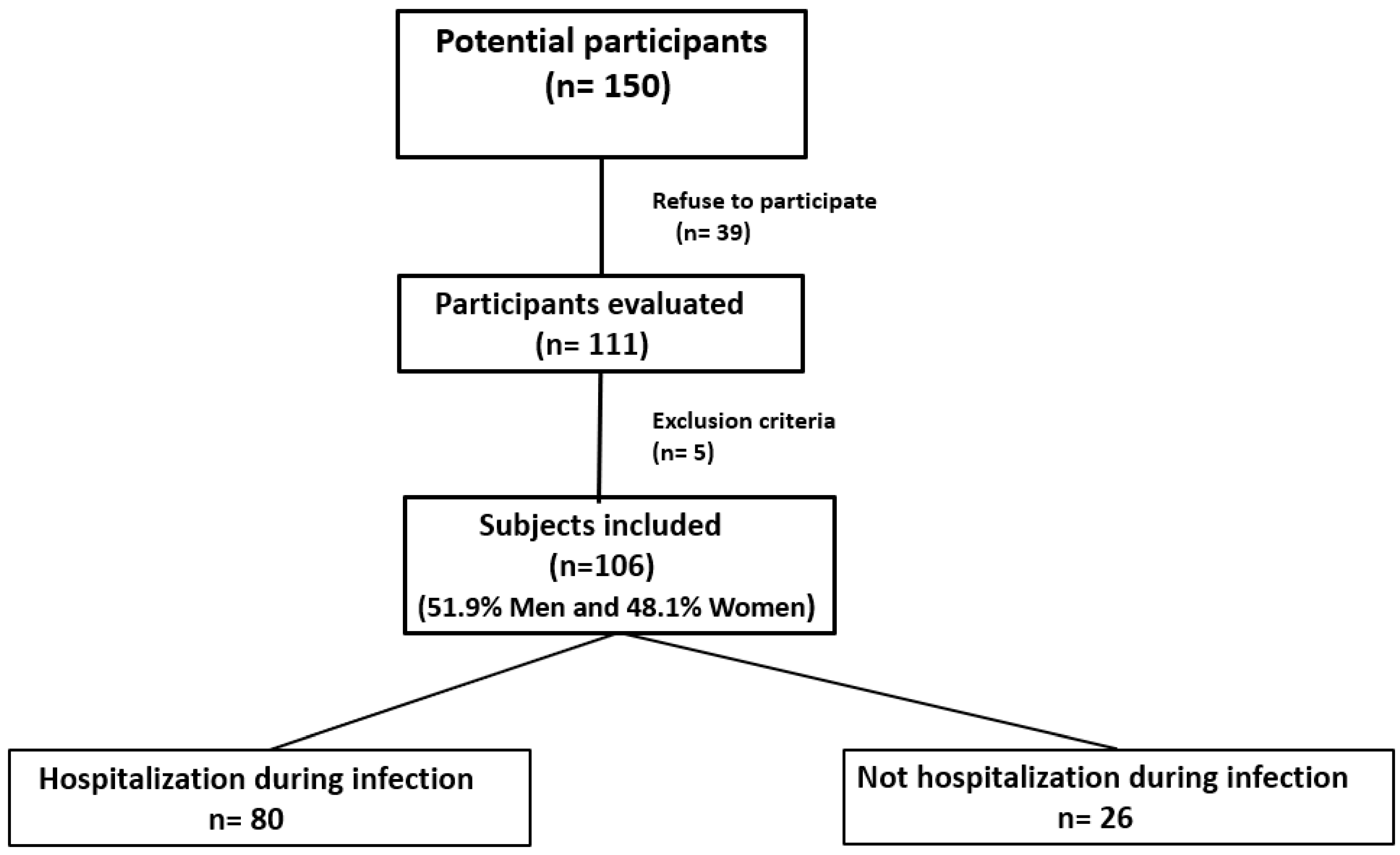
2.1. Study Design and Recruited Population
2.2. Written Informed Consent
2.3. Clinical Data Collection
2.4. Visits
2.5. Sarcopenia Assessment
2.6. Dietary Assessment
2.7. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Ministerio de Sanidad. Situación Actual Enfermedad por Nuevo Coronavirus, COVID-19: Información para Profesionales; Ministerio de Sanidad, Consumoy Bienestar Social: Madrid, Spain, 2020; Available online: https://www.sanidad.gob.es/profesionales/saludPublica/ccayes/alertasActual/nCov/situacionActual.htm (accessed on 13 March 2022).
- Martinchek, M.; Beiting, K.J.; Walker, J.; Graupner, J.; Huisingh-Scheetz, M.; Thompson, K.; Gleason, L.J.; Levine, S. Weight loss in COVID-19-positive nursing home residents. J. Am. Med. Dir. Assoc. 2021, 22, 257–258. [Google Scholar] [CrossRef] [PubMed]
- Di Filippo, L.; De Lorenzo, R.; D’Amico, M.; Sofia, V.; Roveri, L.; Mele, R.; Saibene, A.; Rovere-Querini, P.; Conte, C. COVID-19 is associated with clinically significant weight loss and risk of malnutrition, independent of hospitalisation: A post-hoc analysis of a prospective cohort study. Clin. Nutr. 2020, 40, 2420–2426. [Google Scholar] [CrossRef]
- Cruz-Jentoft, A.J.; Bahat, G.; Bauer, J.; Boirie, Y.; Bruyère, O.; Cederholm, T.; Cooper, C.; Landi, F.; Rolland, Y.; Sayer, A.A.; et al. Writing Group for the European Working Group on Sarcopenia in Older People 2 (EWGSOP2), and the Extended Group for EWGSOP2. Sarcopenia: Revised European consensus on definition and diagnosis. Age Ageing 2019, 48, 16–31. [Google Scholar] [CrossRef] [Green Version]
- Beaudart, C.; Reginster, J.Y.; Petermans, J.; Gillain, S.; Quabron, A.; Locquet, M.; Slomian, J.; Buckinx, F.; Bruyère, O. Quality of life and physical components linked to sarcopenia: The SarcoPhAge study. Exp. Gerontol. 2015, 69, 103–110. [Google Scholar] [CrossRef]
- Bischoff-Ferrari, H.A.; Orav, J.E.; Kanis, J.A.; Rizzoli, R.; Schlögl, M.; Staehelin, H.B.; Willett, W.C.; Dawson-Hughes, B. Comparative performance of current definitions of sarcopenia against the prospective incidence of falls among community-dwelling seniors age 65 and older. Osteoporos. Int. 2015, 26, 2793–2802. [Google Scholar] [CrossRef]
- Wilson, D.; Jackson, T.; Sapey, E.; Lord, J.M. Frailty and sarcopenia: The potential role of an aged immune system. Ageing Res. Rev. 2017, 36, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Landi, F.; Cruz-Jentoft, A.J.; Liperoti, R.; Russo, A.; Giovannini, S.; Tosato, M.; Capoluongo, E.; Bernabei, R.; Onder, G. Sarcopenia and mortality risk in frail older persons aged 80 years and older: Results from ilSIRENTE study. Age Ageing 2013, 42, 203–209. [Google Scholar] [CrossRef] [Green Version]
- Welch, C.; Hassan-Smith, Z.K.; Greig, C.A.; Lord, J.M.; Jackson, T.A. Acute Sarcopenia Secondary to Hospitalisation—An Emerging Condition Affecting Older Adults. Aging Dis. 2018, 9, 151–164. [Google Scholar] [CrossRef] [Green Version]
- Kim, T.N.; Choi, K.M. Sarcopenia: Definition, epidemiology, and pathophysiology. J. Bone Metab. 2013, 20, 1–10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Reginster, J.Y.; Cooper, C.; Rizzoli, R.; Kanis, J.A.; Appelboom, G.; Bautmans, I.; Bischoff-Ferrari, H.A.; Boers, M.; Brandi, M.L.; Bruyère., O.; et al. Recommendations for the conduct of clinical trials for drugs to treat or prevent sarcopenia. Aging Clin. Exp. Res. 2016, 28, 47–58. [Google Scholar] [CrossRef] [Green Version]
- Mijnarends, D.M.; Meijers, J.M.; Halfens, R.J.; ter Borg, S.; Luiking, Y.C.; Verlaan, S.; Schoberer, D.; Cruz Jentoft, A.J.; van Loon, L.J.; Schols, J.M. Validity and reliability of tools to measure muscle mass, strength, and physical performance in community-dwelling older people: A systematic review. J. Am. Med. Dir. Assoc. 2013, 14, 170–178. [Google Scholar] [CrossRef]
- Carfì, A.; Bernabei, R.; Landi, F. Gemelli Against COVID-19 Post-Acute Care Study Group. Persistent Symptoms in Patients After Acute COVID-19. JAMA 2020, 324, 603–605. [Google Scholar] [CrossRef]
- Greenhalgh, T.; Knight, M.; A’Court, C.; Buxton, M.; Husain, L. Management of post-acute covid-19 in primary care. BMJ 2020, 370, m3026. [Google Scholar] [CrossRef] [PubMed]
- Morley, J.E.; Kalantar-Zadeh, K.; Anker, S.D. COVID-19: A major cause of cachexia and sarcopenia? J. Cachexia Sarcopenia Muscle 2020, 11, 863–865. [Google Scholar] [CrossRef]
- Paneroni, M.; Simonelli, C.; Saleri, M.; Bertacchini, L.; Venturelli, M.; Troosters, T.; Ambrosino, N.; Vitacca, M. Muscle Strength and Physical Performance in Patients Without Previous Disabilities Recovering From COVID-19 Pneumonia. Am. J. Phys. Med. Rehabil. 2021, 100, 105–109. [Google Scholar] [CrossRef] [PubMed]
- Mahoney, F.I.; Barthel, D.W. Functional evaluation: The Barthel Index. Md. State Med. J. 1965, 14, 61–65. [Google Scholar]
- Rius, C.; Pérez, G.; Martínez, J.M.; Bares, M.; Schiaffino, A.; Gispert, R.; Fernández, E. An adaptation of Charlson comorbidity index predicted subsequent mortality in a health survey. J. Clin. Epidemiol. 2004, 57, 403–408, Erratum in: J. Clin. Epidemiol. 2007, 60, 643. [Google Scholar] [CrossRef] [PubMed]
- Norris, D.; Clark, M.S.; Shipley, S. The Mental Status Examination. Am. Fam. Physician 2016, 94, 635–641. [Google Scholar]
- Kojima, G.; Iliffe, S.; Walters, K. Frailty index as a predictor of mortality: A systematic review and meta-analysis. Age Ageing 2018, 47, 193–200. [Google Scholar] [CrossRef] [Green Version]
- Sousa-Santos, A.R.; Amaral, T.F. Differences in handgrip strength protocols to identify sarcopenia and frailty—A systematic review. BMC Geriatr. 2017, 17, 238. [Google Scholar] [CrossRef] [Green Version]
- Malmstrom, T.K.; Miller, D.K.; Simonsick, E.M.; Ferrucci, L.; Morley, J.E. SARC-F: A symptom score to predict persons with sarcopenia at risk for poor functional outcomes. J. Cachexia Sarcopenia Muscle 2016, 7, 28–36. [Google Scholar] [CrossRef]
- Trichopoulu, A.; Costacou, T.; Bamia, C. Adherence to a Mediterranean Diet and Survival in a Greek Population. N. Engl. J. Med. 2003, 348, 687–696. [Google Scholar] [CrossRef] [Green Version]
- da Rocha, A.Q.; Lobo, P.C.B.; Pimentel, G.D. Muscle Function Loss and Gain of Body Weight during the COVID-19 Pandemic in Elderly Women: Effects of One Year of Lockdown. J. Nutr. Health Aging 2021, 25, 1028–1029. [Google Scholar] [CrossRef] [PubMed]
- Bastiaanse, L.P.; Hilgenkamp, T.I.; Echteld, M.A.; Evenhuis, H.M. Prevalence and associated factors of sarcopenia in older adults with intellectual disabilities. Res. Dev. Disabil. 2012, 33, 2004–2012. [Google Scholar] [CrossRef] [PubMed]
- Tay, L.; Ding, Y.Y.; Leung, B.P.; Ismail, N.H.; Yeo, A.; Yew, S.; Tay, K.S.; Tan, C.H.; Chong., M.S. Sex-specific differences in risk factors for sarcopenia amongst community-dwelling older adults. Age 2015, 37, 121. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, Y.S.; Lee, Y.; Chung, Y.S.; Lee, D.J.; Joo, N.S.; Hong, D.; Song, G.E.; Kim, H.J.; Choi, Y.J.; Kim, K.M. Prevalence of sarcopenia and sarcopenic obesity in the Korean population based on the Fourth Korean National Health and Nutritional Examination Surveys. J. Gerontol. A. Biol. Sci. Med. Sci. 2012, 67, 1107–1113. [Google Scholar] [CrossRef]
- Lieber, C.S. Relationships between nutrition, alcohol use, and liver disease. Alcohol Res. Health 2003, 27, 220–231. [Google Scholar]
- Wang, T.; Feng, X.; Zhou, J.; Gong, H.; Xia, S.; Wei, Q.; Hu, X.; Tao, R.; Li, L.; Qian, F.; et al. Type 2 diabetes mellitus is associated with increased risks of sarcopenia and pre-sarcopenia in Chinese elderly. Sci. Rep. 2016, 6, 38937. [Google Scholar] [CrossRef] [Green Version]
- Moga, T.D.; Nistor-Cseppento, C.D.; Bungau, S.G.; Tit, D.M.; Sabau, A.M.; Behl, T.; Nechifor, A.C.; Bungau, A.F.; Negrut, N. The Effects of the ’Catabolic Crisis’ on Patients’ Prolonged Immobility after COVID-19 Infection. Medicina 2022, 58, 828. [Google Scholar] [CrossRef]
- González-Islas, D.; Sánchez-Moreno, C.; Orea-Tejeda, A.; Hernández-López, S.; Salgado-Fernández, F.; Keirns-Davis, C.; Galicia-Amor, S.; Trejo-Mellado, E.; Gochicoa-Rangel, L.; Castorena-Maldonado, A. Body composition and risk factors associated with sarcopenia in post-COVID patients after moderate or severe COVID-19 infections. BMC Pulm. Med. 2022, 22, 223. [Google Scholar] [CrossRef]
- Beaufrère, B.; Morio, B. Fat and protein redistribution with aging: Metabolic considerations. Eur. J. Clin. Nutr. 2000, 54, S48–S53. [Google Scholar] [CrossRef] [Green Version]
- Choo, Y.J.; Chang, M.C. Prevalence of Sarcopenia Among the Elderly in Korea: A Meta-Analysis. J. Prev. Med. Public Health 2021, 54, 96–102. [Google Scholar] [CrossRef] [PubMed]
- De Spiegeleer, A.; Kahya, H.; Sanchez-Rodriguez, D.; Piotrowicz, K.; Surquin, M.; Marco, E.; Detremerie, C.; Hussein, D.; Hope, S.; Dallmeier, D.; et al. Acute sarcopenia changes following hospitalization: Influence of pre-admission care dependency level. Age Ageing 2021, 50, 2140–2146. [Google Scholar] [CrossRef]
- Gariballa, S.; Alessa, A. Sarcopenia: Prevalence and prognostic significance in hospitalized patients. Clin. Nutr. 2013, 32, 772–776. [Google Scholar] [CrossRef]
- Abate, M.; Di Iorio, A.; Di Renzo, D.; Paganelli, R.; Saggini, R.; Abate, G. Frailty in the elderly: The physical dimension. Eura. Medicophys. 2007, 43, 407–415. [Google Scholar] [PubMed]
- Kirwan, R.; McCullough, D.; Butler, T.; Perez de Heredia, F.; Davies, I.G.; Stewart, C. Sarcopenia during COVID-19 lockdown restrictions: Long-term health effects of short-term muscle loss. Geroscience 2020, 42, 1547–1578. [Google Scholar] [CrossRef] [PubMed]
- Cobos-Palacios, L.; Muñoz-Úbeda, M.; Ruiz-Moreno, M.I.; Vilches-Perez, A.; Vargas-Candela, A.; Benítez-Porres, J.; Navarro-Sanz, A.; Lopez-Carmona, M.D.; Pérez-Belmonte, L.M.; Sanz-Canovas, J.; et al. Lifestyle Modification Program on a Metabolically Healthy Elderly Population with Overweight/Obesity, Young-Old vs. Old-Old. CONSEQUENCES of COVID-19 Lockdown in This Program. Int. J. Environ. Res. Public Health 2021, 18, 11926. [Google Scholar] [CrossRef]
- Martinez-Ferran, M.; de la Guía-Galipienso, F.; Sanchis-Gomar, F.; Pareja-Galeano, H. Metabolic Impacts of Confinement during the COVID-19 Pandemic Due to Modified Diet and Physical Activity Habits. Nutrients 2020, 12, 1549. [Google Scholar] [CrossRef]
- Visser, M.; Pahor, M.; Taaffe, D.R.; Goodpaster, B.H.; Simonsick, E.M.; Newman, A.B.; Nevitt, M.; Harris, T.B. Relationship of interleukin-6 and tumor necrosis factor-alpha with muscle mass and muscle strength in elderly men and women: The Health ABC Study. J. Gerontol. A. Biol. Sci. Med. Sci. 2002, 57, M326–M332. [Google Scholar] [CrossRef] [Green Version]
- Schaap, L.A.; Pluijm, S.M.; Deeg, D.J.; Harris, T.B.; Kritchevsky, S.B.; Newman, A.B.; Colbert, L.H.; Pahor, M.; Rubin, S.M.; Tylavsky, F.A.; et al. Health ABC Study. Higher inflammatory marker levels in older persons: Associations with 5-year change in muscle mass and muscle strength. J. Gerontol. A. Biol. Sci. Med. Sci. 2009, 64, 1183–1189. [Google Scholar] [CrossRef] [Green Version]
- Manini, T.M.; Clark, B.C. Dynapenia and aging: An update. J. Gerontol. A. Biol. Sci. Med. Sci. 2012, 67, 28–40. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Delmonico, M.J.; Harris, T.B.; Visser, M.; Park, S.W.; Conroy, M.B.; Velasquez-Mieyer, P.; Boudreau, R.; Manini, T.M.; Nevitt, M.; Newman, A.B.; et al. Health, Aging, and Body. Longitudinal study of muscle strength, quality, and adipose tissue infiltration. Am. J. Clin. Nutr. 2009, 90, 1579–1585. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Clark, B.C.; Manini, T.M. Sarcopenia =/= dynapenia. J. Gerontol. A. Biol. Sci. Med. Sci. 2008, 63, 829–834. [Google Scholar] [CrossRef] [PubMed]
- Sieber, C.C. Malnutrition and sarcopenia. Aging Clin. Exp. Res. 2019, 31, 793–798. [Google Scholar] [CrossRef]
- Cawood, A.L.; Walters, E.R.; Smith, T.R.; Sipaul, R.H.; Stratton, R.J. A Review of Nutrition Support Guidelines for Individuals with or Recovering from COVID-19 in the Community. Nutrients 2020, 12, 3230. [Google Scholar] [CrossRef]
- Barazzoni, R.; Bischoff, S.C.; Breda, J.; Wickramasinghe, K.; Krznaric, Z.; Nitzan, D.; Pirlich, M.; Singer, P. endorsed by the ESPEN Council. ESPEN expert statements and practical guidance for nutritional management of individuals with SARS-CoV-2 infection. Clin. Nutr. 2020, 39, 1631–1638. [Google Scholar] [CrossRef]
- Trichopoulou, A.; Kouris-Blazos, A.; Wahlqvist, M.L.; Gnardellis, C.; Lagiou, P.; Polychronopoulos, E.; Vassilakou, T.; Lipworth, L.; Trichopoulos, D. Diet and overall survival in elderly people. BMJ 1995, 311, 1457–1460. [Google Scholar] [CrossRef] [Green Version]
- Kelaiditi, E.; Jennings, A.; Steves, C.J.; Skinner, J.; Cassidy, A.; MacGregor, A.J.; Welch, A.A. Measurements of skeletal muscle mass and power are positively related to a Mediterranean dietary pattern in women. Osteoporos Int. 2016, 27, 3251–3260. [Google Scholar] [CrossRef] [Green Version]
- Marzetti, E.; Calvani, R.; Landi, F.; Hoogendijk, E.O.; Fougère, B.; Vellas, B.; Pahor, M.; Bernabei, R.; Cesari, M. SPRINTT Consortium. Innovative Medicines Initiative: The SPRINTT Project. J. Frailty Aging 2015, 4, 207–208. [Google Scholar]
- Izquierdo, M.; Morley, J.E.; Lucia, A. Exercise in people over 85. BMJ 2020, 368, m402. [Google Scholar] [CrossRef]
- Nambi, G.; Abdelbasset, W.K.; Alrawaili, S.M.; Elsayed, S.H.; Verma, A.; Vellaiyan, A.; Eid, M.M.; Aldhafian, O.R.; Nwihadh, N.B.; Saleh, A.K. Comparative effectiveness study of low versus high-intensity aerobic training with resistance training in community-dwelling older men with post-COVID 19 sarcopenia: A randomized controlled trial. Clin. Rehabil. 2022, 36, 59–68. [Google Scholar] [CrossRef] [PubMed]
- Chaabene, H.; Prieske, O.; Herz, M.; Moran, J.; Höhne, J.; Kliegl, R.; Ramirez-Campillo, R.; Behm, D.G.; Hortobágyi, T.; Granacher, U. Home-based exercise programmes improve physical fitness of healthy older adults: A PRISMA-compliant systematic review and meta-analysis with relevance for COVID-19. Ageing Res. Rev. 2021, 67, 101265. [Google Scholar] [CrossRef] [PubMed]
- Fried, L.P.; Tangen, C.M.; Walston, J.; Newman, A.B.; Hirsch, C.; Gottdiener, J.; Seeman, T.; Tracy, R.; Kop, W.J.; Burke, G.; et al. Cardiovascular Health Study Collaborative Research Group. Frailty in older adults: Evidence for a phenotype. J. Gerontol. A. Biol. Sci. Med. Sci. 2001, 56, M146–M156. [Google Scholar] [CrossRef] [PubMed]
- Carrazco-Peña, K.B.; Tene, C.E.; Del Río-Valdivia, J. Sarcopenia y dependencia funcional (DF) en el anciano [Sarcopenia and functional disability in aged]. Gac. Med. Mex. 2016, 152, 444–451. (In Spanish) [Google Scholar]
- Pacifico, J.; Geerlings, M.A.J.; Reijnierse, E.M.; Phassouliotis, C.; Lim, W.K.; Maier, A.B. Prevalence of sarcopenia as a comorbid disease: A systematic review and meta-analysis. Exp. Gerontol. 2020, 131, 110801. [Google Scholar] [CrossRef]
- Zhou, X.; Wang, J.L.; Lu, J.; Song, Y.; Kwak, K.S.; Jiao, Q.; Rosenfeld, R.; Chen, Q.; Boone, T.; Simonet, W.S.; et al. Reversal of cancer cachexia and muscle wasting by ActRIIB antagonism leads to prolonged survival. Cell 2010, 142, 531–543. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
| Total (n = 106) | Men (n = 55) | Women (n = 51) | p | |
|---|---|---|---|---|
| Barthel Index (points) | 93.7 ± 15.7 | 95.5 ± 12.6 | 91.7 ± 18.4 | 0.3 |
| Charlson Index (points) | 4.6 ± 1.8 | 4.9 ± 1.9 | 4.2 ± 1.6 | 0.3 |
| MMSE Index (points) | 28.05 ± 3.5 | 28.26 ± 2.96 | 27.8 ± 3.98 | 0.4 |
| FRAIL Index (points) | 1.34 ± 1.25 | 1.32 ± 1.32 | 1.37 ± 1.19 | 0.6 |
| Hypertension (%) | 81.1 | 78.2 | 84.3 | 0.2 |
| Dyslipidemia (%) | 47.2 | 40 | 54.9 | 0.1 |
| Cardiopathy (%) | 34.9 | 45.4 | 23.6 | 0.02 |
| Diabetes (%) | 29.3 | 32.7 | 25.5 | 0.5 |
| Smoking (%) | 28.3 | 47.3 | 7.8 | <0.001 |
| COPD (%) | 16 | 25.5 | 5.9 | <0.001 |
| Depression (%) | 15.1 | 1.8 | 31.4 | <0.001 |
| Dementia (%) | 13.2 | 12.7 | 13.7 | 0.9 |
| Neoplasm (%) | 13.2 | 20 | 5.9 | 0.04 |
| Anxiety (%) | 13.2 | 3.6 | 23.5 | <0.001 |
| AF (%) | 12.3 | 16.4 | 7.8 | 0.4 |
| CKD (%) | 11.3 | 12.7 | 9.8 | 0.7 |
| SAHS (%) | 7.5 | 12.7 | 2 | 0.06 |
| Stroke (%) | 6.6 | 9.1 | 3.9 | 0.4 |
| Asthma (%) | 6.6 | 5.5 | 7.8 | 0.7 |
| Alcoholism (%) | 4.7 | 9.1 | 0 | 0.05 |
| Liver disease (%) | 3.8 | 1.8 | 5.9 | 0.2 |
| Hemodialysis (%) | 1.9 | 0 | 3.9 | 0.2 |
| Symptoms | Population | 3 Months | 12 Months | p |
|---|---|---|---|---|
| Asthenia (%) | Total | 51.9 | 26 | <0.001 |
| Men | 41.8 | 10.3 | 0.003 | |
| Women | 62.7 | 42.1 | 0.01 | |
| Dyspnea (%) | Total | 50.9 | 20.8 | <0.001 |
| Men | 49.1 | 7.7 | <0.001 | |
| Women | 52.9 | 34.2 | 0.018 | |
| Weight loss (%) | Total | 27.4 | 1.3 | <0.001 |
| Men | 38.2 | 2.6 | 0.001 | |
| Women | 15.7 | 0 | ||
| Cough (%) | Total | 20.8 | 7.8 | <0.001 |
| Men | 20 | 5.1 | 0.02 | |
| Women | 21.6 | 10.5 | 0.01 | |
| Anxiety (%) | Total | 17 | 3.9 | 0.02 |
| Men | 21.8 | 1.3 | 0.08 | |
| Women | 11.8 | 7.9 | 0.01 | |
| MMII Weakness (%) | Total | 17 | 6.5 | 0.02 |
| Men | 14.5 | 5.1 | 0.10 | |
| Women | 19.6 | 7.9 | 0.08 | |
| Chest pain (%) | Total | 13.2 | 3.9 | 0.06 |
| Men | 14.5 | 5.1 | 0.18 | |
| Women | 11.8 | 2.6 | 0.18 | |
| Anosmia–Ageusia (%) | Total | 12.3 | 0 | |
| Men | 9.1 | 0 | ||
| Women | 15.7 | 0 | ||
| Mucus (%) | Total | 9.4 | 0 | |
| Men | 14.5 | 0 | ||
| Women | 3.9 | 0 | ||
| Diarrhea (%) | Total | 7.5 | 0 | |
| Men | 12.7 | 0 | ||
| Women | 2 | 0 | ||
| Headache (%) | Total | 5.7 | 5.2 | 0.66 |
| Men | 1.8 | 5.1 | 0.57 | |
| Women | 9.8 | 5.3 | 0.16 | |
| Skin lesions (%) | Total | 4.7 | 0 | |
| Men | 3.6 | 0 | ||
| Women | 5.9 | 0 |
| 3 Months | 12 Months | p | ||
|---|---|---|---|---|
| Weight (kg) | Total | 71.9 ± 12.1 | 74.7 ± 12.7 | <0.001 |
| Men | 78.6 ± 9.9 | 81.5 ± 10.5 | <0.001 | |
| Women | 66.6 ± 10.9 | 68 ± 11.3 | 0.03 | |
| BMI (kg/m2) | Total | 28.1 ± 3.5 | 29.1 ± 4.5 | <0.001 |
| Men | 28.4 ± 3.4 | 29.5 ± 3.7 | <0.001 | |
| Women | 28.3 ± 5.2 | 28.9 ± 5.3 | 0.01 | |
| Body fat (%) | Total | 32.2 ± 7.3 | 33 ± 8.4 | <0.05 |
| Men | 28.5 ± 5.4 | 30.7 ± 6.8 | 0.001 | |
| Women | 35.7 ± 9 | 35.9 ± 9 | 0.25 | |
| Fat mass (kg) | Total | 23.9 ± 7.4 | 25.1 ± 9.2 | 0.002 |
| Men | 23.4 ± 6.4 | 25.1 ± 7.1 | 0.005 | |
| Women | 24.8 ± 10.8 | 25.3 ± 11.4 | 0.15 | |
| Lean mass (kg) | Total | 49.6 ± 10 | 49.9 ± 10 | 0.29 |
| Men | 56.5 ± 6.1 | 57.3 ± 7.2 | 0.18 | |
| Women | 41.7 ± 4.9 | 41.8 ± 4.6 | 0.92 | |
| Waist circumference (cm) | Total | 96.9 ± 10.8 | 99.1 ± 15.9 | 0.02 |
| Men | 101.3 ± 7.3 | 105.9 ± 15.3 | 0.04 | |
| Women | 90.3 ± 11.8 | 91.9 ± 13.9 | 0.17 | |
| Hb (g/dL) | Total | 14.4 ± 14.1 | 14.4 ± 14.2 | 0.9 |
| Platelets (U/µL) | Total | 272.8 ± 113.9 | 257.1 ± 145.3 | 0.3 |
| Leukocytes (U/µL) | Total | 7700 ± 4356 | 9520 ± 5678 | 0.5 |
| Neutrophils (U/µL) | Total | 5800 ± 3021 | 4210 ± 2134 | <0.0001 |
| Lymphocytes (U/µL) | Total | 1130 ± 596 | 1540 ± 578 | <0.0001 |
| TP (sg) | Total | 92.6 ± 18.4 | 87.1 ± 15 | 0.7 |
| INR | Total | 1.13 ± 0.8 | 1.09 ± 0.6 | 0.6 |
| D-dimer (ng/mL) | Total | 700.5 ± 1199 | 458 ± 545 | <0.05 |
| LDH (U/L) | Total | 168.8 ± 42.5 | 181.8 ± 41.8 | 0.3 |
| GOT (U/L) | Total | 29.3 ± 12.7 | 26.1 ± 24.1 | 0.3 |
| GGT (U/L) | Total | 32.8 ± 23.3 | 24.4 ± 13.3 | 0.07 |
| Ferritin (ng/mL) | Total | 93 ± 144 | 90 ± 110.9 | 0.7 |
| CRP (mg/mL) | Total | 4.5 ± 7 | 4.2 ± 6.8 | 0.6 |
| IL-6 (pg/mL) | Total | 4.7 ± 11.6 | 1.5 ± 2.4 | <0.05 |
| 3 Months | 12 Months | p | ||
|---|---|---|---|---|
| Dynamometry value (kg) | Total | 16.8 ± 8.3 | 18. ± 8.7 | 0.06 |
| Men | 21 ± 8 | 23.5 ± 8.3 | 0.03 | |
| Women | 12 ± 4.2 | 12.6 ± 4.7 | 0.45 | |
| Possible sarcopenia diagnosis by dynamometry (%) | Total | 81.4 | 57.35 | 0.07 |
| Men | 78 | 48 | 0.01 | |
| Women | 84.8 | 66.7 | 0.56 | |
| SARC-F value (points) | Total | 2.6 ± 1.9 | 2 ± 1.8 | 0.06 |
| Men | 2.23 ± 1.67 | 1.16 ± 1.2 | 0.01 | |
| Women | 3.11 ± 1.8 | 2.85 ± 1.92 | 0.31 | |
| Sarcopenia diagnosis by SARC-F (%) | Total | 32.65 | 19 | 0.07 |
| Men | 32.7 | 10.5 | 0.03 | |
| Women | 32.6 | 27.5 | 0.10 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
López-Sampalo, A.; Cobos-Palacios, L.; Vilches-Pérez, A.; Sanz-Cánovas, J.; Vargas-Candela, A.; Mancebo-Sevilla, J.J.; Hernández-Negrín, H.; Gómez-Huelgas, R.; Bernal-López, M.R. COVID-19 in Older Patients: Assessment of Post-COVID-19 Sarcopenia. Biomedicines 2023, 11, 733. https://doi.org/10.3390/biomedicines11030733
López-Sampalo A, Cobos-Palacios L, Vilches-Pérez A, Sanz-Cánovas J, Vargas-Candela A, Mancebo-Sevilla JJ, Hernández-Negrín H, Gómez-Huelgas R, Bernal-López MR. COVID-19 in Older Patients: Assessment of Post-COVID-19 Sarcopenia. Biomedicines. 2023; 11(3):733. https://doi.org/10.3390/biomedicines11030733
Chicago/Turabian StyleLópez-Sampalo, Almudena, Lidia Cobos-Palacios, Alberto Vilches-Pérez, Jaime Sanz-Cánovas, Antonio Vargas-Candela, Juan José Mancebo-Sevilla, Halbert Hernández-Negrín, Ricardo Gómez-Huelgas, and María Rosa Bernal-López. 2023. "COVID-19 in Older Patients: Assessment of Post-COVID-19 Sarcopenia" Biomedicines 11, no. 3: 733. https://doi.org/10.3390/biomedicines11030733