
Post-COVID Syndrome: The Research Progress in the Treatment of Pulmonary sequelae after COVID-19 Infection

 ,
,  and
and
Abstract
:1. Introduction
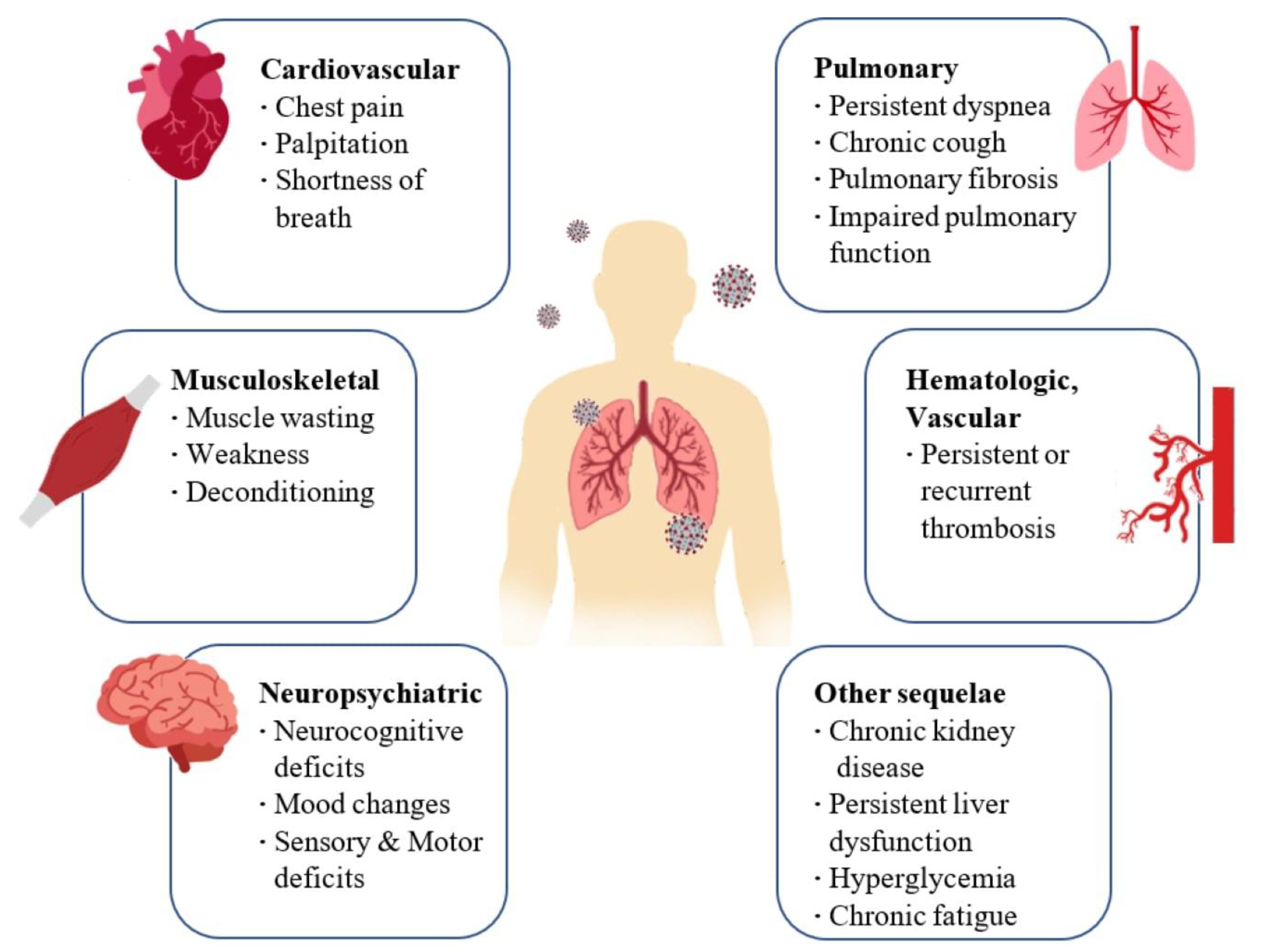
2. Long-Term Consequences and Aftereffects of COVID Infection
3. Management of Patients with Post-COVID Syndrome and after Effects of SARS-CoV-2 Infection

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Drug | Category | Mode of Action | References |
|---|---|---|---|
| Flavonoids (luteolin, apigenin, kaempferol, fisetin, quercetin, genistein, and epigallocatechin gallate) | Mast cell level Stabilizers | Anti-inflammatory and mast cell-stabilizing effects | [40,42,43] |
| Antihistamine drugs (olopatadine, rupatadine, and ketotifen) | Mast cell level Stabilizers | Anti-inflammatory and mast cell-stabilizing effects | [40,42,44] |
| Clarithromycin | Mast cell level Stabilizers | Anti-inflammatory and mast cell-stabilizing effects | [41,45] |
| Dexamethasone | Corticosteroids | Decreases the inflammation linked with cytokine release syndrome | [48] |
| Ciclesonide | Corticosteroids | Anti-inflammatory action | [53] |
| Azithromycin | Antibiotics | Inhibit the proliferation of fibroblasts, reduce the production of collagen and the levels of TGF-β | [57] |
| Pirfenidone | Antifibrotic | Inhibit the synthesis of collagen induced by TGF-β; suppresses the production of TNF-α, IFN-γ, IL-1β- and IL-6; suppresses the differentiation of fibroblasts associated with TGF-β | [61] |
| Curcumin | Antifibrotic | Decreasing the expression of the TGF-β II receptor (TGF-ß RII), as well as in directly reducing the expression of the TGF-β protein and its mRNA | [22] |
| N-Acetylcysteine (NAC) | Antioxidants | Inhibits virus replication and expression of pro-inflammatory molecules. Boosting a type of cell in the immune system that attacks infections | [63] |
| GSH | Antioxidants | Blocks viral replication through redox state modulation | [64] |
| Molnupiravir | Antivirals | Inhibits the replication of SARS-CoV-2, acting on the enzyme that the virus uses to generate copies of itself by introducing errors into its genetic code | [66] |
| Zofin | Derived from human amniotic fluid | Suppressor of cytokine activation | [67] |
| Ampion | Biological Drug | Modulate inflammatory cytokine levels | [69] |
4. Post-COVID Inhalation Therapy
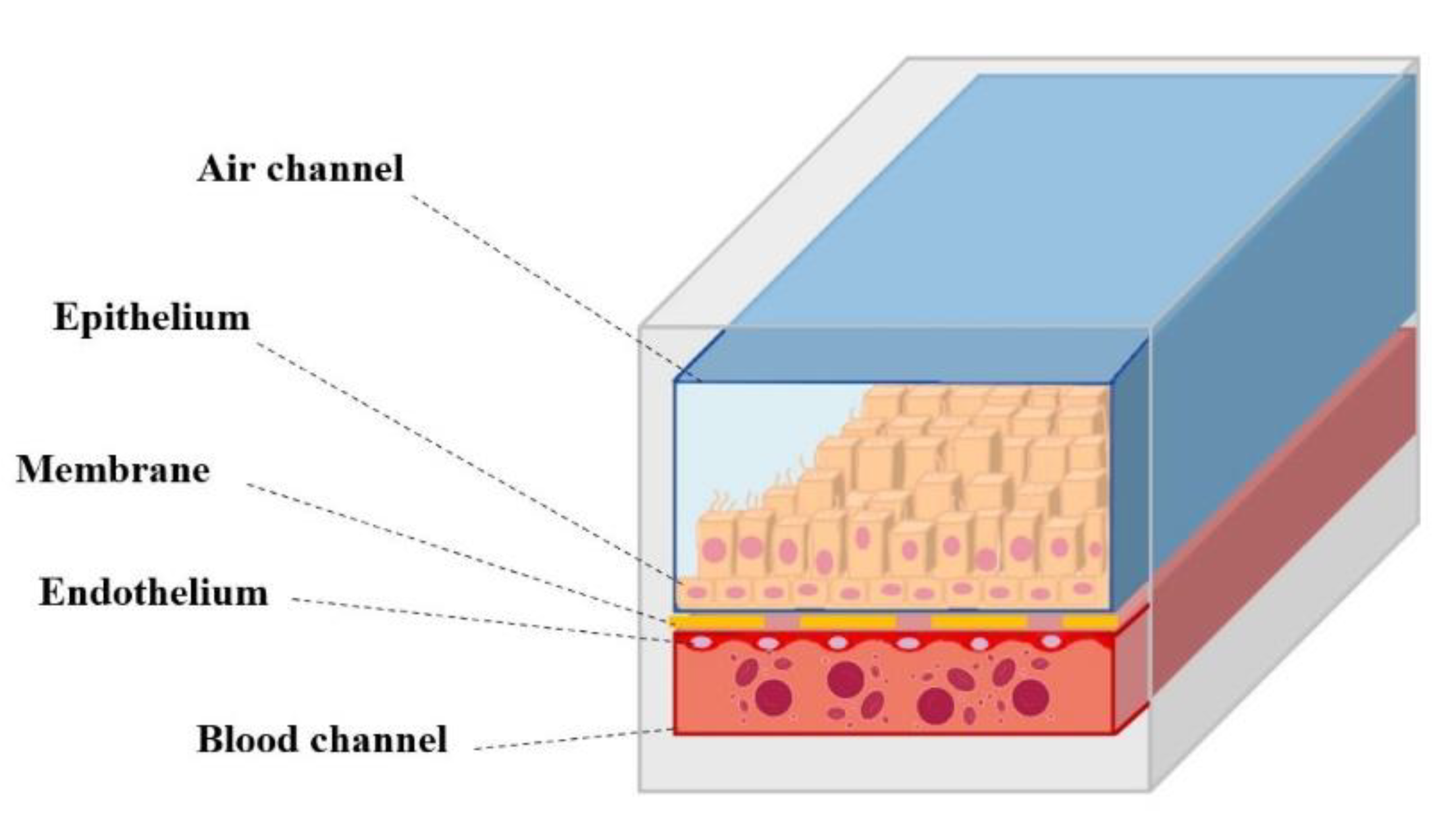
5. In Vitro Models for the Study of Post-COVID Syndrome Drugs
6. Conclusions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Yan, Z.; Yang, M.; Lai, C.-L. Long COVID-19 syndrome: A comprehensive review of its effect on various organ systems and recommendation on rehabilitation plans. Biomedicines 2021, 9, 966. [Google Scholar] [CrossRef] [PubMed]
- Jiang, D.H.; McCoy, R.G. Planning for the post-COVID syndrome: How payers can mitigate long-term complications of the pandemic. J. Gen. Intern. Med. 2020, 35, 3036–3039. [Google Scholar] [CrossRef] [PubMed]
- Nalbandian, A.; Sehgal, K.; Gupta, A.; Madhavan, M.V.; McGroder, C.; Stevens, J.S.; Cook, J.R.; Nordvig, A.S.; Shalev, D.; Sehrawat, T.S.; et al. Post-acute COVID-19 syndrome. Nat. Med. 2021, 27, 601–615. [Google Scholar] [CrossRef] [PubMed]
- Hackett, M.L.; Glozier, N.S.; Martiniuk, A.L.; Jan, S.; Anderson, C.S. Sydney Epilepsy Incidence Study to Measure Illness Consequences: The SESIMIC Observational Epilepsy Study Protocol. BMC Neurol. 2011, 11, 3. [Google Scholar] [CrossRef] [Green Version]
- Ahmed, H.; Patel, K.; Greenwood, D.; Halpin, S.; Lewthwaite, P.; Salawu, A.; Eyre, L.; Breen, A.; O’Connor, R.; Jones, A.; et al. Long-Term Clinical Outcomes in Survivors of Severe Acute Respiratory Syndrome and Middle East Respiratory Syndrome Coronavirus Outbreaks after Hospitalisation or ICU Admission: A Systematic Review and Meta-Analysis. J. Rehabil. Med. 2020, 52, jrm00063. [Google Scholar] [CrossRef]
- Hui, D.S. Impact of Severe Acute Respiratory Syndrome (SARS) on Pulmonary Function, Functional Capacity and Quality of Life in a Cohort of Survivors. Thorax 2005, 60, 401–409. [Google Scholar] [CrossRef] [Green Version]
- Daugherty, S.E.; Guo, Y.; Heath, K.; Dasmariñas, M.C.; Jubilo, K.G.; Samranvedhya, J.; Lipsitch, M.; Cohen, K. Risk of clinical sequelae after the acute phase of SARS-CoV-2 infection: Retrospective cohort study. BMJ 2021, 373, n1098. [Google Scholar] [CrossRef]
- Garg, M.; Maralakunte, M.; Garg, S.; Dhooria, S.; Sehgal, I.; Bhalla, A.S.; Vijayvergiya, R.; Grover, S.; Bhatia, V.; Jagia, P.; et al. The conundrum of ‘Long-COVID-19’: A narrative review. IJGM 2021, 14, 2491–2506. [Google Scholar] [CrossRef]
- Michalski, J.E.; Kurche, J.S.; Schwartz, D.A. From ARDS to pulmonary fibrosis: The next phase of the COVID-19 pandemic? Transl. Res. 2022, 241, 13–24. [Google Scholar] [CrossRef]
- Udwadia, Z.; Koul, P.; Richeldi, L. Post-COVID lung fibrosis: The tsunami that will follow the earthquake. Lung India 2021, 38, 41. [Google Scholar] [CrossRef]
- Boechat, J.L.; Chora, I.; Morais, A.; Delgado, L. The immune response to SARS-CoV-2 and COVID-19 immunopathology—Current perspectives. Pulmonology 2021, 27, 423–437. [Google Scholar] [CrossRef] [PubMed]
- Eedara, B.B.; Alabsi, W.; Encinas-Basurto, D.; Polt, R.; Ledford, J.G.; Mansour, H.M. Inhalation delivery for the treatment and prevention of COVID-19 infection. Pharmaceutics 2021, 13, 1077. [Google Scholar] [CrossRef] [PubMed]
- Fratta Pasini, A.M.; Stranieri, C.; Cominacini, L.; Mozzini, C. Potential role of antioxidant and anti-inflammatory therapies to prevent severe SARS-CoV-2 complications. Antioxidants 2021, 10, 272. [Google Scholar] [CrossRef] [PubMed]
- Salamanna, F.; Veronesi, F.; Martini, L.; Landini, M.P.; Fini, M. Post-COVID-19 Syndrome: The Persistent Symptoms at the Post-Viral Stage of the Disease. A Systematic Review of the Current Data. Front. Med. 2021, 8, 653516. [Google Scholar] [CrossRef] [PubMed]
- Sivashanmugam, K.; Kandasamy, M.; Subbiah, R.; Ravikumar, V. Repurposing of histone deacetylase inhibitors: A promising strategy to combat pulmonary fibrosis promoted by TGF-β signalling in COVID-19 survivors. Life Sci. 2021, 266, 118883. [Google Scholar]
- Ali, R.M.M.; Ghonimy, M.B.I. Post-COVID-19 pneumonia lung fibrosis: A worrisome sequelae in surviving patients. Egypt. J. Radiol. Nucl. Med. 2021, 52, 101. [Google Scholar] [CrossRef]
- Lutchmansingh, D.D.; Knauert, M.P.; Antin-Ozerkis, D.E.; Chupp, G.; Cohn, L.; Dela Cruz, C.S.; Ferrante, L.E.; Herzog, E.L.; Koff, J.; Rochester, C.L.; et al. A clinic blueprint for post-coronavirus disease 2019 RECOVERY. Chest 2021, 159, 949–958. [Google Scholar] [CrossRef]
- Mehandru, S.; Merad, M. Pathological Sequelae of Long-Haul COVID. Nat. Immunol. 2022, 23, 194–202. [Google Scholar] [CrossRef]
- Rezkalla, S.H.; Kloner, R.A. Post-acute sequelae of SARS-COVID-2 syndrome: Just the beginning. Cardiol Res 2021, 12, 279–285. [Google Scholar] [CrossRef]
- Proal, A.D.; VanElzakker, M.B. Long COVID or post-acute sequelae of COVID-19 (PASC): An overview of biological factors that may contribute to persistent symptoms. Front. Microbiol. 2021, 12, 698169. [Google Scholar] [CrossRef]
- Jackson, C.B.; Farzan, M.; Chen, B.; Choe, H. Mechanisms of SARS-CoV-2 entry into cells. Nat. Rev. Mol. Cell Biol. 2022, 23, 3–20. [Google Scholar] [CrossRef] [PubMed]
- Yo, E.C.; Kadharusman, M.M.; Karman, A.P.; Louisa, M.; Arozal, W. Potential pharmacological options and new avenues using inhaled curcumin nanoformulations for treatment of post-COVID-19 fibrosis. Syst. Rev. Pharm. 2021, 12, 1119–1128. [Google Scholar]
- Banu, N.; Panikar, S.S.; Leal, L.R.; Leal, A.R. Protective role of ACE2 and its downregulation in SARS-CoV-2 infection leading to macrophage activation syndrome: Therapeutic implications. Life Sci. 2020, 256, 117905. [Google Scholar] [CrossRef] [PubMed]
- Ramasamy, S.; Subbian, S. Critical determinants of cytokine storm and type I interferon response in COVID-19 pathogenesis. Clin. Microbiol. Rev. 2021, 34, e00299-20. [Google Scholar] [CrossRef]
- Channappanavar, R.; Perlman, S. Pathogenic human coronavirus infections: Causes and consequences of cytokine storm and immunopathology. Semin. Immunopathol. 2017, 39, 529–539. [Google Scholar] [CrossRef]
- Thompson, B.T.; Chambers, R.C.; Liu, K.D. Acute Respiratory Distress Syndrome. N. Engl. J. Med. 2017, 377, 562–572. [Google Scholar] [CrossRef]
- Suess, C.; Hausmann, R. Gross and histopathological pulmonary findings in a COVID-19 associated death during self-isolation. Int. J. Leg. Med. 2020, 134, 1285–1290. [Google Scholar] [CrossRef]
- Oronsky, B.; Larson, C.; Hammond, T.C.; Oronsky, A.; Kesari, S.; Lybeck, M.; Reid, T.R. A review of persistent post-COVID syndrome (PPCS). Clin. Rev. Allergy Immunol. 2021, 1–9. [Google Scholar] [CrossRef]
- Plataki, M.; Hubmayr, R.D. The physical basis of ventilator-induced lung injury. Expert Rev. Respir. Med. 2010, 4, 373–385. [Google Scholar] [CrossRef] [Green Version]
- Cabrera-Benitez, N.E.; Laffey, J.G.; Parotto, M.; Spieth, P.M.; Villar, J.; Zhang, H.; Slutsky, A.S. Mechanical ventilation–associated lung fibrosis in acute respiratory distress syndrome. Anesthesiology 2014, 121, 189–198. [Google Scholar] [CrossRef] [Green Version]
- Abodonya, A.M.; Abdelbasset, W.K.; Awad, E.A.; Elalfy, I.E.; Salem, H.A.; Elsayed, S.H. Inspiratory muscle training for recovered COVID-19 patients after weaning from mechanical ventilation: A pilot control clinical study. Medicine 2021, 100, e25339. [Google Scholar] [CrossRef] [PubMed]
- Umemura, Y.; Mitsuyama, Y.; Minami, K.; Nishida, T.; Watanabe, A.; Okada, N.; Yamakawa, K.; Nochioka, K.; Fujimi, S. Efficacy and safety of Nintedanib for pulmonary fibrosis in severe pneumonia induced by COVID-19: An interventional study. Int. J. Infect. Dis. 2021, 108, 454–460. [Google Scholar] [CrossRef] [PubMed]
- Wang, F.; Kream, R.M.; Stefano, G.B. Long-term respiratory and neurological sequelae of COVID-19. Med. Sci. Monit. 2020, 26, e928996-1–e928996-10. [Google Scholar] [CrossRef] [PubMed]
- Esendağli, D.; Yilmaz, A.; Akçay, Ş.; Özlü, T. Post-COVID syndrome: Pulmonary complications. Turk. J. Med. Sci. 2021, 51, 3359–3371. [Google Scholar] [CrossRef]
- Ong, K.-C.; Ng, A.W.-K.; Lee, L.S.-U.; Kaw, G.; Kwek, S.-K.; Leow, M.K.-S.; Earnest, A. 1-Year Pulmonary Function and Health Status in Survivors of Severe Acute Respiratory Syndrome. Chest 2005, 128, 1393–1400. [Google Scholar] [CrossRef] [Green Version]
- Torres-Castro, R.; Vasconcello-Castillo, L.; Alsina-Restoy, X.; Solis-Navarro, L.; Burgos, F.; Puppo, H.; Vilaró, J. Respiratory Function in Patients Post-Infection by COVID-19: A Systematic Review and Meta-Analysis. Pulmonology 2021, 27, 328–337. [Google Scholar] [CrossRef]
- Gerardo, A.M.; Almeida, T.; Maduro, S.; Carvalho, M.; Boléo-Tomé, J.P.; Liberato, H. Pulmonary function, functional capacity and health status in COVID-19 survivors. Rev. Med. Clínica 2021, 5, e11052105023. [Google Scholar]
- Afrin, L.B.; Weinstock, L.B.; Molderings, G.J. COVID-19 hyperinflammation and post-COVID-19 illness may be rooted in mast cell activation syndrome. Int. J. Infect. Dis. 2020, 100, 327–332. [Google Scholar] [CrossRef]
- Kritas, S.K. Mast Cells Contribute to Coronavirus-Induced Inflammation: New Anti-Inflammatory Strategy. J. Biol. Regul. Homeost. Agents 2020, 34, 9–14. [Google Scholar]
- Hafezi, B.; Chan, L.; Knapp, J.P.; Karimi, N.; Alizadeh, K.; Mehrani, Y.; Bridle, B.W.; Karimi, K. Cytokine storm syndrome in SARS-CoV-2 infections: A functional role of mast cells. Cells 2021, 10, 1761. [Google Scholar] [CrossRef]
- Kazama, I. Stabilizing mast cells by commonly used drugs: A novel therapeutic target to relieve post-COVID syndrome? Drug Discov. Ther. 2020, 14, 259–261. [Google Scholar] [CrossRef] [PubMed]
- Kilinç, E.; Baranoğlu, Y. Mast Cell Stabilizers as a Supportive Therapy Can Contribute to Alleviate Fatal Inflammatory Responses and Severity of Pulmonary Complications in COVID-19 Infection. Anadolu Klin. Tıp Bilimleri Derg. 2020, 25, 111–118. [Google Scholar] [CrossRef]
- Kakavas, S.; Karayiannis, D.; Mastora, Z. The Complex Interplay between Immunonutrition, Mast Cells, and Histamine Signaling in COVID-19. Nutrients 2021, 13, 3458. [Google Scholar] [CrossRef]
- Baba, A.; Tachi, M.; Maruyama, Y.; Kazama, I. Olopatadine Inhibits Exocytosis in Rat Peritoneal Mast Cells by Counteracting Membrane Surface Deformation. Cell. Physiol. Biochem. 2015, 35, 386–396. [Google Scholar] [CrossRef] [PubMed]
- Kazama, I.; Saito, K.; Baba, A.; Mori, T.; Abe, N.; Endo, Y.; Toyama, H.; Ejima, Y.; Matsubara, M.; Yamauchi, M. Clarithromycin Dose-Dependently Stabilizes Rat Peritoneal Mast Cells. Chemotherapy 2016, 61, 295–303. [Google Scholar] [CrossRef]
- Manniello, M.D.; Del Gaudio, P.; Aquino, R.P.; Russo, P. Clarithromycin and N-acetylcysteine co-spray-dried powders for pulmonary drug delivery: A focus on drug solubility. Int. J. Pharm. 2017, 533, 463–469. [Google Scholar] [CrossRef]
- Manniello, M.D.; Del Gaudio, P.; Porta, A.; Aquino, R.P.; Russo, P. Aerodynamic properties, solubility and in vitro antibacterial efficacy of dry powders prepared by spray drying: Clarithromycin versus its hydrochloride salt. Eur. J. Pharm. Biopharm. 2016, 104, 1–6. [Google Scholar] [CrossRef]
- The RECOVERY Collaborative Group Dexamethasone in Hospitalized Patients with COVID-19. N. Engl. J. Med. 2021, 384, 693–704. [CrossRef]
- Cano, E.J.; Fonseca Fuentes, X.; Corsini Campioli, C.; O’Horo, J.C.; Abu Saleh, O.; Odeyemi, Y.; Yadav, H.; Temesgen, Z. Impact of Corticosteroids in Coronavirus Disease 2019 Outcomes. Chest 2021, 159, 1019–1040. [Google Scholar] [CrossRef]
- Griesel, M.; Wagner, C.; Mikolajewska, A.; Stegemann, M.; Fichtner, F.; Metzendorf, M.-I.; Nair, A.A.; Daniel, J.; Fischer, A.-L.; Skoetz, N. Inhaled Corticosteroids for the Treatment of COVID-19. Cochrane Database Syst. Rev. 2022, 3, 1–59. [Google Scholar]
- Milne, S.; Li, X.; Yang, C.X.; Leitao Filho, F.S.; Hernández Cordero, A.I.; Yang, C.W.T.; Shaipanich, T.; van Eeden, S.F.; Leung, J.M.; Lam, S.; et al. Inhaled Corticosteroids Downregulate SARS-CoV-2-Related Genes in COPD: Results from a Randomised Controlled Trial. Eur. Respir. J. 2021, 58, 2100130. [Google Scholar] [CrossRef] [PubMed]
- Maruta, H.; He, H. PAK1-Blockers: Potential Therapeutics against COVID-19. Med. Drug Discov. 2020, 6, 100039. [Google Scholar] [CrossRef] [PubMed]
- Clemency, B.M.; Varughese, R.; Gonzalez-Rojas, Y.; Morse, C.G.; Phipatanakul, W.; Koster, D.J.; Blaiss, M.S. Efficacy of Inhaled Ciclesonide for Outpatient Treatment of Adolescents and Adults with Symptomatic COVID-19: A Randomized Clinical Trial. JAMA Intern. Med. 2022, 182, 42. [Google Scholar] [CrossRef] [PubMed]
- Ripa, M.; Galli, L.; Poli, A.; Oltolini, C.; Spagnuolo, V.; Mastrangelo, A.; Muccini, C.; Monti, G.; De Luca, G.; Landoni, G.; et al. Secondary infections in patients hospitalized with COVID-19: Incidence and predictive factors. Clin. Microbiol. Infect. 2021, 27, 451–457. [Google Scholar] [CrossRef]
- Langford, B.J.; So, M.; Raybardhan, S.; Leung, V.; Westwood, D.; MacFadden, D.R.; Soucy, J.-P.R.; Daneman, N. Bacterial co-infection and secondary infection in patients with COVID-19: A living rapid review and meta-analysis. Clin. Microbiol. Infect. 2020, 26, 1622–1629. [Google Scholar] [CrossRef] [PubMed]
- Hama Amin, B.J.; Kakamad, F.H.; Ahmed, G.S.; Ahmed, S.F.; Abdulla, B.A.; mohammed, S.H.; Mikael, T.M.; Salih, R.Q.; Ali, R.K.; Salh, A.M.; et al. Post COVID-19 Pulmonary Fibrosis; a Meta-Analysis Study. Ann. Med. Surg. 2022, 77, 103590. [Google Scholar] [CrossRef] [PubMed]
- Echeverría-Esnal, D.; Martin-Ontiyuelo, C.; Navarrete-Rouco, M.E.; De-Antonio Cuscó, M.; Ferrández, O.; Horcajada, J.P.; Grau, S. Azithromycin in the Treatment of COVID-19: A Review. Expert Rev. Anti Infect. Ther. 2021, 19, 147–163. [Google Scholar] [CrossRef]
- Raghu, G.; Richeldi, L. Current Approaches to the Management of Idiopathic Pulmonary Fibrosis. Respir. Med. 2017, 129, 24–30. [Google Scholar] [CrossRef]
- Margaritopoulos, G.A.; Vasarmidi, E.; Antoniou, K.M. Pirfenidone in the treatment of idiopathic pulmonary fibrosis: An evidence-based review of its place in therapy. Core Evid. 2016, 11, 11–22. [Google Scholar] [CrossRef] [Green Version]
- Jin, J.; Togo, S.; Kadoya, K.; Tulafu, M.; Namba, Y.; Iwai, M.; Watanabe, J.; Nagahama, K.; Okabe, T.; Hidayat, M.; et al. Pirfenidone Attenuates Lung Fibrotic Fibroblast Responses to Transforming Growth Factor-Β1. Respir. Res. 2019, 20, 119. [Google Scholar] [CrossRef] [Green Version]
- Zhang, F.; Wei, Y.; He, L.; Zhang, H.; Hu, Q.; Yue, H.; He, J.; Dai, H. A Trial of Pirfenidone in Hospitalized Adult Patients with Severe Coronavirus Disease 2019. Chin. Med. J. 2022, 135, 368–370. [Google Scholar] [CrossRef] [PubMed]
- Liu, Z.; Ying, Y. The inhibitory effect of curcumin on virus-induced cytokine storm and its potential use in the associated severe pneumonia. Front. Cell Dev. Biol. 2020, 8, 479. [Google Scholar] [CrossRef] [PubMed]
- Memorial Sloan Kettering Cancer Center Phase II Study of N-Acetylcysteine in Severe or Critically Ill Patients with Refractory COVID-19 Infection. 2021. Available online: clinicaltrials.gov (accessed on 18 May 2022).
- Horowitz, R.I.; Freeman, P.R.; Bruzzese, J. Efficacy of Glutathione Therapy in Relieving Dyspnea Associated with COVID-19 Pneumonia: A Report of 2 Cases. Respir. Med. Case Rep. 2020, 30, 101063. [Google Scholar] [CrossRef] [PubMed]
- Vitiello, A.; Troiano, V.; La Porta, R. What will be the role of molnupiravir in the treatment of COVID-19 infection? Drugs Perspect. 2021, 37, 579–580. [Google Scholar] [CrossRef]
- Molnupiravir and Remdesivir Available for the Treatment of Non-Hospitalized COVID-19 Patients at High Risk of Progressing to Severe Disease. Available online: https://www.aifa.gov.it/en/-/disponibilit%C3%A0-molnupiravir-e-remdesivir-trattamento-pazienti-non-ospedalizzati-covid-19-1 (accessed on 19 May 2022).
- Mitrani, M.I.; Bellio, M.A.; Meglin, A.; Khan, A.; Xu, X.; Haskell, G.; Arango, A.; Shapiro, G.C. Treatment of a COVID-19 long hauler with an amniotic fluid-derived extracellular vesicle biologic. Respir. Med. Case Rep. 2021, 34, 101502. [Google Scholar] [CrossRef]
- Mitrani, M.I.; Bellio, M.A.; Sagel, A.; Saylor, M.; Kapp, W.; VanOsdol, K.; Haskell, G.; Stewart, D.; Abdullah, Z.; Santos, I.; et al. Case report: Administration of amniotic fluid-derived nanoparticles in three severely Ill COVID-19 patients. Front. Med. 2021, 8, 242. [Google Scholar] [CrossRef]
- Ampio Pharmaceuticals Receives Investigational Review Board Approval for Its Phase I Long COVID-19 Trial (AP-018). Available online: https://www.biospace.com/article/ampio-pharmaceuticals-receives-investigational-review-board-approval-for-its-phase-i-long-covid-19-trial-ap-018-/ (accessed on 19 May 2022).
- Ragab, D.; Salah Eldin, H.; Taeimah, M.; Khattab, R.; Salem, R. The COVID-19 cytokine storm; What we know so far. Front. Immunol. 2020, 11, 1446. [Google Scholar] [CrossRef]
- Abdellatif, A.A.H.; Tawfeek, H.M.; Abdelfattah, A.; El-Saber Batiha, G.; Hetta, H.F. Recent updates in COVID-19 with emphasis on inhalation therapeutics: Nanostructured and targeting systems. J. Drug Deliv. Sci. Technol. 2021, 63, 102435. [Google Scholar] [CrossRef]
- Lechowicz, K.; Drożdżal, S.; Machaj, F.; Rosik, J.; Szostak, B.; Zegan-Barańska, M.; Biernawska, J.; Dabrowski, W.; Rotter, I.; Kotfis, K. COVID-19: The potential treatment of pulmonary fibrosis associated with SARS-CoV-2 infection. JCM 2020, 9, 1917. [Google Scholar] [CrossRef]
- Newman, S.P. Drug delivery to the lungs: Challenges and opportunities. Ther. Deliv. 2017, 8, 647–661. [Google Scholar] [CrossRef]
- Wright, J. Inhaler Devices for the Treatment of Asthma and Chronic Obstructive Airways Disease (COPD). Qual. Saf. Health Care 2002, 11, 376–382. [Google Scholar] [CrossRef] [PubMed]
- Thorley, A.J.; Tetley, T.D. New Perspectives in Nanomedicine. Pharmacol. Ther. 2013, 140, 176–185. [Google Scholar] [CrossRef] [PubMed]
- Mahmud, A.; Discher, D.E. Lung Vascular Targeting through Inhalation Delivery: Insight from Filamentous Viruses and Other Shapes. IUBMB Life 2011, 63, 607–612. [Google Scholar] [CrossRef] [PubMed]
- Sung, J.C.; Pulliam, B.L.; Edwards, D.A. Nanoparticles for Drug Delivery to the Lungs. Trends Biotechnol. 2007, 25, 563–570. [Google Scholar] [CrossRef]
- Brain, J.D.; Knudson, D.E.; Sorokin, S.P.; Davis, M.A. Pulmonary Distribution of Particles given by Intratracheal Instillation or by Aerosol Inhalation. Environ. Res. 1976, 11, 13–33. [Google Scholar] [CrossRef]
- Groneberg, D.A.; Witt, C.; Wagner, U.; Chung, K.F.; Fischer, A. Fundamentals of Pulmonary Drug Delivery. Respir. Med. 2003, 97, 382–387. [Google Scholar] [CrossRef] [Green Version]
- Borghardt, J.M.; Kloft, C.; Sharma, A. Inhaled Therapy in Respiratory Disease: The Complex Interplay of Pulmonary Kinetic Processes. Can. Respir. J. 2018, 2018, 2732017. [Google Scholar] [CrossRef] [Green Version]
- Colombo, P.; Alhaique, F.; Caramella, C.; Conti, B.; Gazzaniga, A.; Vidale, E. Principi di Tecnologia Farmaceutica, 2nd ed.; Ambrosiana: Milano, Italy, 2015. [Google Scholar]
- Labiris, N.R.; Dolovich, M.B. Pulmonary Drug Delivery. Part I: Physiological Factors Affecting Therapeutic Effectiveness of Aerosolized Medications: Physiological Factors Affecting the Effectiveness of Inhaled Drugs. Br. J. Clin. Pharmacol. 2003, 56, 588–599. [Google Scholar] [CrossRef]
- Newman, S. Improving Inhaler Technique, Adherence to Therapy and the Precision of Dosing: Major Challenges for Pulmonary Drug Delivery. Expert Opin. Drug Deliv. 2014, 11, 365–378. [Google Scholar] [CrossRef]
- O’Callaghan, C.; Barry, P.W. The Science of Nebulised Drug Delivery. Thorax 1997, 52, S31–S44. [Google Scholar] [CrossRef]
- Sou, T.; Bergström, C.A.S. Contemporary Formulation Development for Inhaled Pharmaceuticals. J. Pharm. Sci. 2021, 110, 66–86. [Google Scholar] [CrossRef] [PubMed]
- Pilcer, G.; Amighi, K. Formulation Strategy and Use of Excipients in Pulmonary Drug Delivery. Int. J. Pharm. 2010, 392, 1–19. [Google Scholar] [CrossRef] [PubMed]
- Rubin, B.K.; Fink, J.B. Optimizing Aerosol Delivery by Pressurized Metered-Dose Inhalers. Respir. Care 2005, 50, 1191–1200. [Google Scholar] [PubMed]
- Fink, J.B. Metered-dose inhalers, dry powder inhalers, and transitions. Respir. Care 2000, 45, 623–635. [Google Scholar]
- Ahookhosh, K.; Saidi, M.; Mohammadpourfard, M.; Aminfar, H.; Hamishehkar, H.; Farnoud, A.; Schmid, O. Flow Structure and Particle Deposition Analyses for Optimization of a Pressurized Metered Dose Inhaler (PMDI) in a Model of Tracheobronchial Airway. Eur. J. Pharm. Sci. 2021, 164, 105911. [Google Scholar] [CrossRef]
- Chandel, A.; Goyal, A.K.; Ghosh, G.; Rath, G. Recent Advances in Aerosolised Drug Delivery. Biomed. Pharmacother. 2019, 112, 108601. [Google Scholar] [CrossRef] [PubMed]
- Yawn, B.; Colice, G. Practical Aspects of Inhaler Use in the Management of Chronic Obstructive Pulmonary Disease in the Primary Care Setting. COPD 2012, 7, 495. [Google Scholar] [CrossRef] [Green Version]
- Pothirat, C.; Chaiwong, W.; Phetsuk, N.; Pisalthanapuna, S.; Chetsadaphan, N.; Choomuang, W. Evaluating Inhaler Use Technique in COPD Patients. COPD 2015, 10, 1291. [Google Scholar] [CrossRef] [Green Version]
- van Beerendonk, I.; Mesters, I.; Mudde, A.N.; Tan, T.D. Assessment of the Inhalation Technique in Outpatients with Asthma or Chronic Obstructive Pulmonary Disease Using a Metered-Dose Inhaler or Dry Powder Device. J. Asthma 1998, 35, 273–279. [Google Scholar] [CrossRef]
- Plaza, V.; Giner, J.; Rodrigo, G.J.; Dolovich, M.B.; Sanchis, J. Errors in the Use of Inhalers by Health Care Professionals: A Systematic Review. J. Allergy Clin. Immunol. Pract. 2018, 6, 987–995. [Google Scholar] [CrossRef]
- Lavorini, F.; Magnan, A.; Christophe Dubus, J.; Voshaar, T.; Corbetta, L.; Broeders, M.; Dekhuijzen, R.; Sanchis, J.; Viejo, J.L.; Barnes, P.; et al. Effect of Incorrect Use of Dry Powder Inhalers on Management of Patients with Asthma and COPD. Respir. Med. 2008, 102, 593–604. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Telko, M.J.; Hickey, A.J. Dry Powder Inhaler Formulation. Respir. Care 2005, 50, 1209–1227. [Google Scholar] [PubMed]
- Mehta, P. Dry Powder Inhalers: A Focus on Advancements in Novel Drug Delivery Systems. J. Drug Deliv. 2016, 2016, 8290963. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Islam, N.; Gladki, E. Dry Powder Inhalers (DPIs)—A Review of Device Reliability and Innovation. Int. J. Pharm. 2008, 360, 1–11. [Google Scholar] [CrossRef]
- Roy, A.; Battle, K.; Lurslurchachai, L.; Halm, E.A.; Wisnivesky, J.P. Inhaler Device, Administration Technique, and Adherence to Inhaled Corticosteroids in Patients with Asthma. Prim. Care Respir. J. 2011, 20, 148–154. [Google Scholar] [CrossRef]
- Sumby, B.; Slater, A.; Atkins, P.J.; Prime, D. Review of dry powder inhalers. Adv. Drug Deliv. Rev. 1997, 26, 51–58. [Google Scholar]
- Haughney, J.; Price, D.; Barnes, N.C.; Virchow, J.C.; Roche, N.; Chrystyn, H. Choosing Inhaler Devices for People with Asthma: Current Knowledge and Outstanding Research Needs. Respir. Med. 2010, 104, 1237–1245. [Google Scholar] [CrossRef] [Green Version]
- Heinen, N.; Klöhn, M.; Steinmann, E.; Pfaender, S. In vitro lung models and their application to study SARS-CoV-2 pathogenesis and disease. Viruses 2021, 13, 792. [Google Scholar] [CrossRef]
- Seyfoori, A.; Amereh, M.; Dabiri, S.M.H.; Askari, E.; Walsh, T.; Akbari, M. The role of biomaterials and three dimensional (3D) in Vitro tissue models in fighting against COVID-19. Biomater. Sci. 2021, 9, 1217–1226. [Google Scholar] [CrossRef]
- Jenkins, R.G.; Moore, B.B.; Chambers, R.C.; Eickelberg, O.; Königshoff, M.; Kolb, M.; Laurent, G.J.; Nanthakumar, C.B.; Olman, M.A.; Pardo, A.; et al. An official american thoracic society workshop report: Use of animal models for the preclinical assessment of potential therapies for pulmonary fibrosis. Am. J. Respir. Cell Mol. Biol. 2017, 56, 667–679. [Google Scholar] [CrossRef] [Green Version]
- Kiener, M.; Roldan, N.; Machahua, C.; Sengupta, A.; Geiser, T.; Guenat, O.T.; Funke-Chambour, M.; Hobi, N.; Kruithof-de Julio, M. Human-based advanced in vitro approaches to investigate lung fibrosis and pulmonary effects of COVID-19. Front. Med. 2021, 8, 555. [Google Scholar] [CrossRef] [PubMed]
- Gerckens, M.; Alsafadi, H.N.; Wagner, D.E.; Lindner, M.; Burgstaller, G.; Königshoff, M. Generation of human 3D lung tissue cultures (3D-LTCs) for disease modeling. JoVE 2019, 144, 58437. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sundarakrishnan, A.; Chen, Y.; Black, L.D.; Aldridge, B.B.; Kaplan, D.L. Engineered cell and tissue models of pulmonary fibrosis. Adv. Drug Deliv. Rev. 2018, 129, 78–94. [Google Scholar] [CrossRef] [PubMed]
- Liu, G.; Betts, C.; Cunoosamy, D.M.; Åberg, P.M.; Hornberg, J.J.; Sivars, K.B.; Cohen, T.S. Use of precision cut lung slices as a translational model for the study of lung biology. Respir. Res. 2019, 20, 162. [Google Scholar] [CrossRef]
- Hui, K.P.Y.; Cheung, M.-C.; Perera, R.A.P.M.; Ng, K.-C.; Bui, C.H.T.; Ho, J.C.W.; Ng, M.M.T.; Kuok, D.I.T.; Shih, K.C.; Tsao, S.-W.; et al. Tropism, Replication Competence, and Innate Immune Responses of the Coronavirus SARS-CoV-2 in Human Respiratory Tract and Conjunctiva: An Analysis in Ex-Vivo and In-Vitro Cultures. Lancet Respir. Med. 2020, 8, 687–695. [Google Scholar] [CrossRef]
- Martin, C. Human lung slices: New uses for an old model. Am. J. Respir. Cell Mol. Biol. 2021, 65, 471–472. [Google Scholar] [CrossRef]
- Bai, Y.; Krishnamoorthy, N.; Patel, K.R.; Rosas, I.; Sanderson, M.J.; Ai, X. Cryopreserved human precision-cut lung slices as a bioassay for live tissue banking. A viability study of bronchodilation with bitter-taste receptor agonists. Am. J. Respir. Cell Mol. Biol. 2016, 54, 656–663. [Google Scholar] [CrossRef]
- Sun, A.M.; Hoffman, T.; Luu, B.Q.; Ashammakhi, N.; Li, S. Application of lung microphysiological systems to COVID-19 modeling and drug discovery: A review. Bio-Des. Manuf. 2021, 4, 757–775. [Google Scholar] [CrossRef]
- Strikoudis, A.; Cieślak, A.; Loffredo, L.; Chen, Y.-W.; Patel, N.; Saqi, A.; Lederer, D.J.; Snoeck, H.-W. Modeling of fibrotic lung disease using 3D organoids derived from human pluripotent stem cells. Cell Rep. 2019, 27, 3709–3723.e5. [Google Scholar] [CrossRef] [Green Version]
- Low, L.A.; Mummery, C.; Berridge, B.R.; Austin, C.P.; Tagle, D.A. Organs-on-chips: Into the next decade. Nat. Rev. Drug Discov. 2021, 20, 345–361. [Google Scholar] [CrossRef]
- Esch, E.W.; Bahinski, A.; Huh, D. Organs-on-chips at the frontiers of drug discovery. Nat. Rev. Drug Discov. 2015, 14, 248–260. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Si, L.; Bai, H.; Oh, C.Y.; Jin, L.; Prantil-Baun, R.; Ingber, D.E. Clinically Relevant Influenza Virus Evolution Reconstituted in a Human Lung Airway-on-a-Chip. Microbiol. Spectr. 2021, 9, e00257-21. [Google Scholar] [CrossRef] [PubMed]
- Zhang, M.; Wang, P.; Luo, R.; Wang, Y.; Li, Z.; Guo, Y.; Yao, Y.; Li, M.; Tao, T.; Chen, W.; et al. Biomimetic Human Disease Model of SARS-CoV-2-Induced Lung Injury and Immune Responses on Organ Chip System. Adv. Sci. 2021, 8, 2002928. [Google Scholar] [CrossRef] [PubMed]
- Thacker, V.V.; Sharma, K.; Dhar, N.; Mancini, G.; Sordet-Dessimoz, J.; McKinney, J.D. Rapid Endotheliitis and Vascular Damage Characterize SARS-CoV-2 Infection in a Human Lung-on-chip Model. EMBO Rep. 2021, 22, e52744. [Google Scholar] [CrossRef]
- Wu, Q.; Liu, J.; Wang, X.; Feng, L.; Wu, J.; Zhu, X.; Wen, W.; Gong, X. Organ-on-a-chip: Recent breakthroughs and future prospects. BioMed. Eng. OnLine 2020, 19, 9. [Google Scholar] [CrossRef] [Green Version]




Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ruggiero, V.; Aquino, R.P.; Del Gaudio, P.; Campiglia, P.; Russo, P. Post-COVID Syndrome: The Research Progress in the Treatment of Pulmonary sequelae after COVID-19 Infection. Pharmaceutics 2022, 14, 1135. https://doi.org/10.3390/pharmaceutics14061135
Ruggiero V, Aquino RP, Del Gaudio P, Campiglia P, Russo P. Post-COVID Syndrome: The Research Progress in the Treatment of Pulmonary sequelae after COVID-19 Infection. Pharmaceutics. 2022; 14(6):1135. https://doi.org/10.3390/pharmaceutics14061135
Chicago/Turabian StyleRuggiero, Valentina, Rita P. Aquino, Pasquale Del Gaudio, Pietro Campiglia, and Paola Russo. 2022. "Post-COVID Syndrome: The Research Progress in the Treatment of Pulmonary sequelae after COVID-19 Infection" Pharmaceutics 14, no. 6: 1135. https://doi.org/10.3390/pharmaceutics14061135