
Relationships between Depression, Fear of Childbirth, and Obsessive-Compulsive Symptoms among Pregnant Women under the COVID-19 Pandemic in Japan

Abstract
:1. Introduction
2. Methods
2.1. Study Procedure and Participants
2.2. Measurements
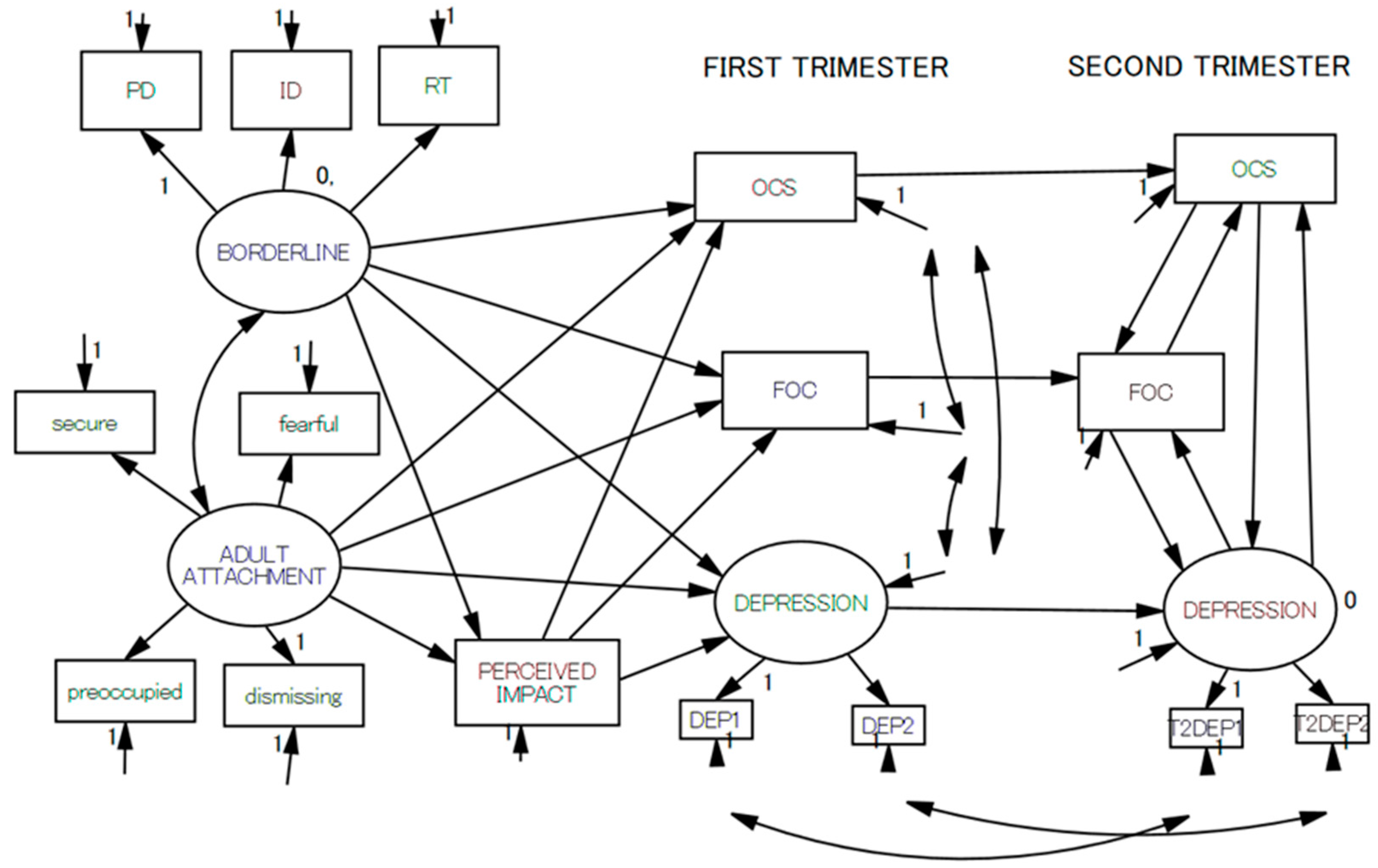
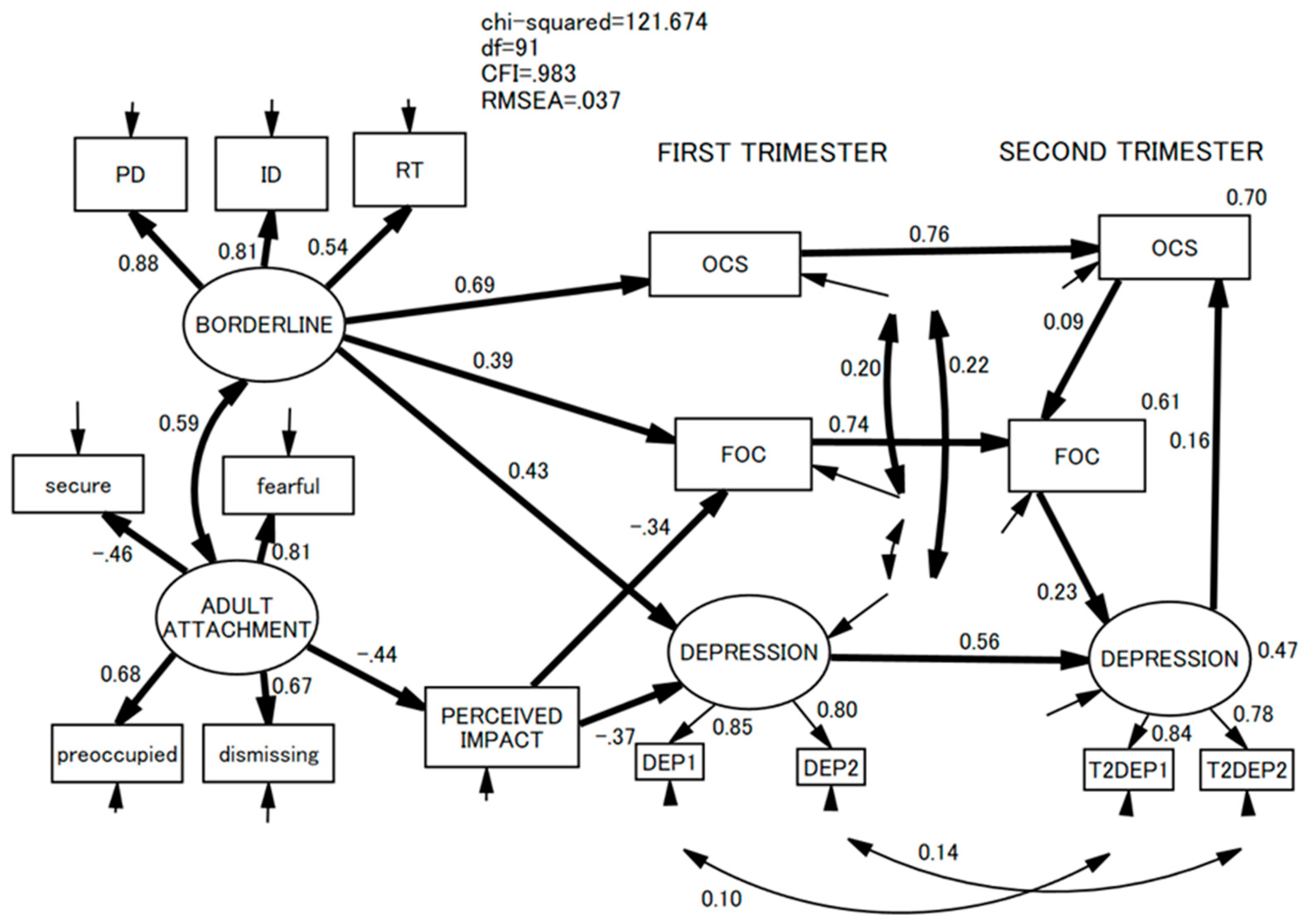
2.3. Data Analysis
2.4. Ethical Considerations
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Yin, X.; Sun, N.; Jiang, N.; Xu, X.; Gan, Y.; Zhang, J.; Qiu, L.; Yang, C.; Shi, X.; Chang, J.; et al. Prevalence and associated factors of antenatal depression: Systematic reviews and meta-analyses. Clin. Psychol. Rev. 2021, 83, 101932. [Google Scholar] [CrossRef]
- Biaggi, A.; Conroy, S.; Pawlby, S.; Pariante, C.M. Identifying the women at risk of antenatal anxiety and depression: A systematic review. J. Affect. Disord. 2016, 191, 62–77. [Google Scholar] [CrossRef] [Green Version]
- Orsolini, L.; Valchera, A.; Vecchiotti, R.; Tomasetti, C.; Iasevoli, F.; Fornaro, M.; Berardis, D.; de Perna, G.; Pompili, M.; Bellantuono, C. Suicide during perinatal period: Epidemiology, risk factors, and clinical correlates. Front. Psychiatry 2016, 7, 1–6. [Google Scholar] [CrossRef] [Green Version]
- Kitamura, T.; Shima, S.; Sugawara, M.; Toda, M.A. Clinical and psychosocial correlates of antenatal depression: A review. Psychother. Psychosom. 1996, 65, 117–123. [Google Scholar] [CrossRef]
- Minatani, M.; Kita, S.; Ohashi, Y.; Kitamura, T.; Haruna, M.; Sakanashi, K.; Tanaka, T. Temperament, character, and depressive symptoms during pregnancy: A study of a Japanese population. Depress. Res. Treat. 2013, 140169. [Google Scholar] [CrossRef] [Green Version]
- Takegata, M.; Ohashi, Y.; Haruna, M.; Kitamura, T. Theoretical framework for interper-sonal psychotherapy in the prevention of post-partum depression: A commentary. Int. J. Nurs. Sci. 2014, 1, 37–40. [Google Scholar]
- Kitamura, T.; Toda, M.A.; Shima, S.; Sugawara, K.; Sugawara, M. Social support and pregnancy: I. Factorial structure and psychosocial correlates of perceived social support. Psychiatry Clin. Neurosci. 1998, 52, 29–36. [Google Scholar] [CrossRef]
- Kitamura, T.; Toda, M.A.; Shima, S.; Sugawara, K.; Sugawara, M. Social support and pregnancy: II. Its relationship with depressive symptoms among Japanese women. Psychiatry Clin. Neurosci. 1998, 52, 37–45. [Google Scholar] [CrossRef]
- Chen, Z.; Tanaka, N.; Uji, M.; Hiramura, H.; Shikai, N.; Fujihara, S.; Kitamura, T. The role of personality for marital adjustment of Japanese couples. Soc. Behav. Pers. 2007, 35, 561–572. [Google Scholar] [CrossRef]
- Quirk, S.E.; Berk, M.; Pasco, J.A.; Brennan-Olsen, S.L.; Chanen, A.M.; Koivumaa-Honkanen, H.; Burke, L.M.; Jackson, H.J.; Hulbert, C.; Olsson, C.A.; et al. The prevalence, age distribution and comorbidity of personality disorders in Australian women. Aust. N. Z. J. Psychiatry 2017, 51, 141–150. [Google Scholar] [CrossRef] [Green Version]
- Lenzenweger, M.F.; Lane, M.C.; Loranger, A.W.; Kessler, R.C. DSM-IV Personality Disorders in the National Comorbidity Survey Replication. Biol. Psychiatry 2007, 62, 553–564. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nilsson, C.; Hessman, E.; Sjöblom, H.; Dencker, A.; Jangsten, E.; Mollberg, M.; Patel, H.; Sparud-Lundin, C.; Wigert, H.; Begley, C. Definitions, measurements and prevalence of fear of childbirth: A systematic review. BMC Pregnancy Childbirth 2018, 18, 28. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nilsson, C.; Lundgren, I. Women’s lived experience of fear of childbirth. Midwifery 2009, 25, e1–e9. [Google Scholar] [CrossRef] [PubMed]
- Takegata, M.; Haruna, M.; Morikawa, M.; Yonezawa, K.; Komada, M.; Severinsson, E. Qualitative exploration of fear of childbirth and preferences for mode of birth among Japanese primiparas. Nurs. Health Sci. 2018, 20, 338–345. [Google Scholar] [CrossRef]
- Pettersson, F.D.; Hellgren, C.; Nyberg, F.; Åkerud, H.; Sundström-Poromaa, I. Depressed mood, anxiety, and the use of labor analgesia. Arch. Womens Ment. Health 2016, 19, 11–16. [Google Scholar] [CrossRef]
- Rondung, E.; Thomtén, J.; Sundin, Ö. Psychological perspectives on fear of childbirth. J. Anxiety Disord. 2016, 44, 80–91. [Google Scholar] [CrossRef] [Green Version]
- Storksen, H.T.; Eberhard-Gran, M.; Garthus-Niegel, S.; Eskild, A. Fear of childbirth; The relation to anxiety and depression. Acta Obstet. Gynecol. Scand. 2012, 91, 237–242. [Google Scholar] [CrossRef]
- Viswasam, K.; Eslick, G.D.; Starcevic, V. Prevalence, onset and course of anxiety disorders during pregnancy: A systematic review and meta analysis. J. Anxiety Disord. 2019, 255, 27–40. [Google Scholar] [CrossRef]
- Miller, E.S.; Hoxha, D.; Wisner, K.L.; Gossett, D.R. The impact of perinatal depression on the evolution of anxiety and obsessive-compulsive symptoms. Arch. Womens Ment. Health 2015, 18, 457–461. [Google Scholar] [CrossRef]
- Wisner, K.L.; Sit, D.K.Y.; McShea, M.C.; Rizzo, D.M.; Zoretich, R.A.; Hughes, C.L.; Eng, H.F.; Luther, J.F.; Wisniewski, S.R.; Costantino, M.L.; et al. Onset timing, thoughts of self-harm, and diagnoses in postpartum women with screen-positive depression findings. JAMA Psychiatry 2013, 70, 490–498. [Google Scholar] [CrossRef]
- Ayaz, R.; Hocaoǧlu, M.; Günay, T.; Yardlmcl, O.D.; Turgut, A.; Karateke, A. Anxiety and depression symptoms in the same pregnant women before and during the COVID-19 pandemic. J. Perinat. Med. 2020, 48, 965–970. [Google Scholar] [CrossRef] [PubMed]
- Berthelot, N.; Lemieux, R.; Garon-Bissonnette, J.; Drouin-Maziade, C.; Martel, É.; Maziade, M. Uptrend in distress and psychiatric symptomatology in pregnant women during the coronavirus disease 2019 pandemic. Acta Obstet. Gynecol. Scand. 2020, 99, 848–855. [Google Scholar] [CrossRef] [PubMed]
- Ceulemans, M.; Hompes, T.; Foulon, V. Mental health status of pregnant and breastfeeding women during the COVID-19 pandemic: A call for action. Int. J. Gynecol. Obstet. 2020, 151, 146–147. [Google Scholar] [CrossRef]
- Dagklis, T.; Tsakiridis, I.; Mamopoulos, A.; Athanasiadis, A.; Pearson, R.; Papazisis, G. Impact of the COVID-19 lockdown on antenatal mental health in Greece. Psychiatry Clin. Neurosci. 2020, 74, 616–617. [Google Scholar] [CrossRef] [PubMed]
- Dib, S.; Rougeaux, E.; Vázquez-Vázquez, A.; Wells, J.C.K.; Fewtrell, M. Maternal mental health and coping during the COVID-19 lockdown in the UK: Data from the COVID-19 New Mum Study. Int. J. Gynecol. Obstet. 2020, 151, 407–414. [Google Scholar] [CrossRef]
- Farewell, C.V.; Jewell, J.; Walls, J.; Leiferman, J.A. A Mixed-Methods Pilot Study of Perinatal Risk and Resilience During COVID-19. J. Prim. Care Community Health 2020, 11. [Google Scholar] [CrossRef]
- Farrell, T.; Reagu, S.; Mohan, S.; Elmidany, R.; Qaddoura, F.; Ahmed, E.E.; Corbett, G.; Lindow, S.; Abuyaqoub, S.M.; Alabdulla, M.A. The impact of the COVID-19 pandemic on the perinatal mental health of women. J. Perinat. Med. 2020, 48, 971–976. [Google Scholar] [CrossRef]
- Fukase, Y.; Ichikura, K.; Murase, H.; Tagaya, H. Depression, risk factors, and coping strategies in the context of social dislocations resulting from the second wave of COVID-19 in Japan. BMC Psychiatry 2021, 21, 33. [Google Scholar] [CrossRef]
- Gur, R.E.; White, L.K.; Waller, R.; Barzilay, R.; Moore, T.M.; Kornfield, S.; Njoroge, W.F.M.; Duncan, A.F.; Chaiyachati, B.H.; Parish-Morris, J.; et al. The Disproportionate Burden of the COVID-19 Pandemic Among Pregnant Black Women. Psychiatry Res. 2020, 293, 113475. [Google Scholar] [CrossRef]
- Liang, P.; Wang, Y.; Shi, S.; Liu, Y.; Xiong, R. Prevalence and factors associated with postpartum depression during the COVID-19 pandemic among women in Guangzhou, China: A cross-sectional study. BMC Psychiatry 2020, 20, 557. [Google Scholar] [CrossRef]
- Liu, C.H.; Erdei, C.; Mittal, L. Risk factors for depression, anxiety, and PTSD symptoms in perinatal women during the COVID-19 Pandemic. Psychiatry Res. 2021, 295, 113552. [Google Scholar] [CrossRef] [PubMed]
- López-Morales, H.; del Valle, M.V.; Canet-Juric, L.; Andrés, M.L.; Galli, J.I.; Poó, F.; Urquijo, S. Mental health of pregnant women during the COVID-19 pandemic: A longitudinal study. Psychiatry Res. 2021, 295, 113567. [Google Scholar] [CrossRef] [PubMed]
- Matsushima, M.; Horiguchi, H. The COVID-19 pandemic and mental well-being of pregnant women in Japan: Need for Economic and Social Policy interventions. Disaster Med. Public Health Prep. 2022, 16, 449–454. [Google Scholar] [CrossRef] [PubMed]
- Molgora, S.; Accordini, M. Motherhood in the Time of Coronavirus: The Impact of the Pandemic Emergency on Expectant and Postpartum Women’s Psychological Well-Being. Front. Psychol. 2020, 11, 1–16. [Google Scholar] [CrossRef]
- Parra-Saavedra, M.; Villa-Villa, I.; Pérez-Olivo, J.; Guzman-Polania, L.; Galvis-Centurion, P.; Cumplido-Romero, Á.; Santacruz-Vargas, D.; Rivera-Moreno, E.; Molina-Giraldo, S.; Guillen-Burgos, H.; et al. Attitudes and collateral psychological effects of COVID-19 in pregnant women in Colombia. Int. J. Gynecol. Obstet. 2020, 151, 203–208. [Google Scholar] [CrossRef] [PubMed]
- Qi, M.; Li, X.; Liu, S.; Li, Y.; Huang, W. Impact of the COVID-19 epidemic on patterns of pregnant women’s perception of threat and its relationship to mental state: A latent class analysis. PLoS ONE 2020, 15, e0239697. [Google Scholar] [CrossRef] [PubMed]
- Ravaldi, C.; Ricca, V.; Wilson, A.; Homer, C.; Vannacci, A. Previous psychopathology predicted severe COVID-19 concern, anxiety, and PTSD symptoms in pregnant women during “lockdown” in Italy. Arch. Womens Ment. Health 2020, 23, 783–786. [Google Scholar] [CrossRef]
- Spinola, O.; Liotti, M.; Speranza, A.M.; Tambelli, R. Effects of COVID-19 Epidemic Lockdown on Postpartum Depressive Symptoms in a Sample of Italian Mothers. Front. Psychiatry 2020, 11, 1–10. [Google Scholar] [CrossRef]
- Wang, Y.; Chen, L.; Wu, T.; Shi, H.; Li, Q.; Jiang, H.; Zheng, D.; Wang, X.; Wei, Y.; Zhao, Y.; et al. Impact of Covid-19 in pregnancy on mother’s psychological status and infant’s neurobehavioral development: A longitudinal cohort study in China. BMC Med. 2020, 18, 347. [Google Scholar] [CrossRef]
- Wu, Y.; Zhang, C.; Liu, H.; Duan, C.; Li, C.; Fan, J.; Li, H.; Chen, L.; Xu, H.; Li, X.; et al. Perinatal depressive and anxiety symptoms of pregnant women during the coronavirus disease 2019 outbreak in China. Am. J. Obstet. Gynecol. 2020, 223, 240.e1–240.e9. [Google Scholar] [CrossRef]
- Hessami, K.; Romanelli, C.; Chiurazzi, M.; Cozzolino, M. COVID-19 pandemic and maternal mental health: A systematic review and meta-analysis. J. Matern. Neonatal Med. 2020, 35, 4014–4021. [Google Scholar] [CrossRef]
- Sade, S.; Sheiner, E.; Wainstock, T.; Hermon, N.; Salem, S.Y.; Kosef, T.; Battat, T.L.; Oron, S.; Pariente, G. Risk for depressive symptoms among hospitalized women in high-risk pregnancy units during the COVID-19 pandemic. J. Clin. Med. 2020, 9, 2449. [Google Scholar] [CrossRef]
- Silverman, M.E.; Medeiros, C.; Burgos, L. Early pregnancy mood before and during COVID-19 community restrictions among women of low socioeconomic status in New York City: A preliminary study. Arch. Womens Ment. Health 2020, 23, 779–782. [Google Scholar] [CrossRef]
- Yan, H.; Ding, Y.; Guo, W. Mental Health of Pregnant and Postpartum Women During the Coronavirus Disease 2019 Pandemic: A Systematic Review and Meta-Analysis. Front. Psychol. 2020, 11, 1–12. [Google Scholar] [CrossRef]
- Zhou, Y.; Shi, H.; Liu, Z.; Peng, S.; Wang, R.; Qi, L.; Li, Z.; Yang, J.; Ren, Y.; Song, X.; et al. The prevalence of psychiatric symptoms of pregnant and non-pregnant women during the COVID-19 epidemic. Transl. Psychiatry 2020, 10, 319. [Google Scholar] [CrossRef] [PubMed]
- Bromet, E.J.; Havenaar, J.M. Psychological and perceived health effects of the chernobyl disaster: A 20-year review. Health Phys. 2007, 93, 516–521. [Google Scholar] [CrossRef]
- Bromet, E.; Schulberg, H.C.; Dunn, L. Reactions of Psychiatric Patients to the Three Mile Island Nuclear Accident. Arch. Gen. Psychiatry 1982, 39, 725–730. [Google Scholar] [CrossRef]
- Bowling, A. Just one question: If one question works, why ask several? J. Epidemiol. Community Health 2005, 59, 342–345. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chochinov, H.M.; Wilson, K.G.; Enns, M.; Lander, S. “Are you depressed?” Screening for depression in the terminally ill. Am. J. Psychiatry 1997, 154, 674–676. [Google Scholar] [CrossRef]
- Cutler, C.B.; Legano, L.A.; Dreyer, B.P.; Fierman, A.H.; Berkule, S.B.; Lusskin, S.I.; Tomopoulos, S.; Roth, M.; Mendelsohn, A.L. Screening for maternal depression in a low education population using a two item questionnaire. Arch. Womens Ment. Health 2007, 10, 277–283. [Google Scholar] [CrossRef]
- De Boer, A.G.E.M.; van Lanschot, J.J.B.; Stalmeier, P.F.M.; van Sandick, J.W.; Hulscher, J.B.F.; de Haes, J.C.J.M.; Sprangers, M.A.G. Is a single-item visual analogue scale as valid, reliable and responsive as multi-item scales in measuring quality of life? Qual. Life Res. 2004, 13, 311–320. [Google Scholar] [CrossRef]
- Mitchell, A.J. Are one or two simple questions sufficient to detect depression in cancer and palliative care? A Bayesian meta-analysis. Br. J. Cancer 2008, 98, 1934–1943. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mishina, H.; Hayashino, Y.; Fukuhara, S. Test performance of two-question screening for postpartum depressive symptoms. Pediatr. Int. 2009, 51, 48–53. [Google Scholar] [CrossRef]
- Mitchell, A.J.; Coyne, J.C. Do ultra-short screening instruments accurately detect depression in primary care? A pooled analysis and meta- analysis of 22 studies. Br. J. Gen. Pract. 2007, 57, 144–151. [Google Scholar]
- Richardson, L.P.; Rockhill, C.; Russo, J.E.; Grossman, D.C.; Richards, J.; McCarty, C.; McCauley, E.; Katon, W. Evaluation of the PHQ-2 as a brief screen for detecting major depression among adolescents. Pediatrics 2010, 125, e1097–e1103. [Google Scholar] [CrossRef] [Green Version]
- Yamada, F.; Kataoka, Y.; Kitamura, T. Development and Validation of a Short Version of the Primary Scales of the Inventory of Personality Organization: A Study among Japanese University Students. Psychology 2022, 13, 872–890. [Google Scholar] [CrossRef]
- Kernberg, O.F.; Clarkin, J.F. The Inventory of Personality Organization; The New York Hospital Cornell Medical Center: New York, NY, USA, 1995. [Google Scholar]
- Matsuoka, N.; Uji, M.; Hiramura, H.; Chen, Z.; Shikai, N.; Kishida, Y.; Kitamura, T. Adolescents’ attachment style and early experiences: A gender difference. Arch. Womens Ment. Health 2006, 9, 23–29. [Google Scholar] [CrossRef]
- Bartholomew, K.; Horowitz, L.M. Attachment Styles Among Young Adults: A Test of a Four-Category Model. J. Pers. Soc. Psychol. 1991, 61, 226–244. [Google Scholar] [CrossRef]
- Takegata, M.; Haruna, M.; Matsuzaki, M.; Shiraishi, M.; Murayama, R.; Okano, T.; Severinsson, E. Translation and validation of the Japanese version of the Wijma Delivery Expectancy/Experience Questionnaire version A. Nurs. Health Sci. 2013, 15, 326–332. [Google Scholar] [CrossRef]
- Wijma, K.; Wijma, B.; Zar, M. Psychometric aspects of the W-DEQ; A new questionnaire for the measurement of fear of childbirth. J. Psychosom. Obstet. Gynaecol. 1998, 19, 84–97. [Google Scholar] [CrossRef]
- Koike, H.; Tsuchiyagaito, A.; Hirano, Y.; Oshima, F.; Asano, K.; Sugiura, Y.; Kobori, O.; Ishikawa, R.; Nishinaka, H.; Shimizu, E.; et al. Reliability and validity of the Japanese version of the Obsessive-Compulsive Inventory-Revised (OCI-R). Curr. Psychol. 2020, 39, 89–95. [Google Scholar] [CrossRef]
- Foa, E.B.; Huppert, J.D.; Leiberg, S.; Langner, R.; Kichic, R.; Hajcak, G.; Salkovskis, P.M. The obsessive-compulsive inventory: Development and validation of a short version. Psychol. Assess. 2020, 14, 485–496. [Google Scholar] [CrossRef]
- Bentler, P.M. Comparative fit indexes in structural models. Psychol. Bull. 1990, 107, 238–246. [Google Scholar] [CrossRef] [PubMed]
- Schermelleh-Engel, K.; Moosbrugger, H.; Müller, H. Evaluating the fit of structural equation models: Tests of significance and descriptive goodness-of-fit measures. Methods Psychol. Res. Online 2003, 8, 23–74. [Google Scholar]
- Lebel, C.; Mackinnon, A.; Bagshawe, M.; Anna, M. Elevated depression and anxiety symptoms among pregnant individuals during the COVID-19 pandemic. J. Affect. Disord. 2020, 277, 5–13. [Google Scholar] [CrossRef]
- Prasad, D.; Kuhathasan, N.; de Azevedo Cardoso, T.; Suh, J.S.; Frey, B.N. The prevalence of borderline personality features and borderline personality disorder during the perinatal period: A systematic review and meta-analysis. Arch. Womens Ment. Health 2020, 25, 227–289. [Google Scholar] [CrossRef]
- Blankley, G.; Galbally, M.; Snellen, M.; Power, J.; Lewis, A.J. Borderline Personality Disorder in the perinatal period: Early infant and maternal outcomes. Australas. Psychiatry 2015, 23, 688–692. [Google Scholar] [CrossRef]
- Monk, C.; Leight, K.L.; Fang, Y. The relationship between women’s attachment style and perinatal mood disturbance: Implications for screening and treatment. Arch. Womens Ment. Health 2008, 11, 117–129. [Google Scholar] [CrossRef] [Green Version]
- Zhang, L.; Wang, L.; Yuan, Q.; Huang, C.; Cui, S.; Zhang, K.; Zhou, X. The mediating role of prenatal depression in adult attachment and maternal-fetal attachment in primigravida in the third trimester. BMC Pregnancy Childbirth 2021, 21, 307. [Google Scholar] [CrossRef]
- Kitamura, T.; Yoshida, K.; Okano, T.; Kinoshita, K.; Hayashi, M.; Toyoda, N.; Ito, M.; Kudo, N.; Tada, K.; Kanazawa, K.; et al. Multicentre prospective study of perinatal depression in Japan: Incidence and correlates of antenatal and postnatal depression. Arch. Womens Ment. Health 2006, 9, 121–130. [Google Scholar] [CrossRef]
- Hada, A.; Kubota, C.; Imura, M.; Takauma, F.; Tada, K.; Kitamura, T. The Edinburgh Postnatal Depression Scale: Model Comparison of Factor Structure and its Psychosocial Correlates Among Mothers at One Month After Childbirth in Japan. Open Fam. Stud. J. 2019, 11, 1–17. [Google Scholar] [CrossRef]
- Kubota, C.; Okada, T.; Aleksic, B.; Nakamura, Y.; Kunimoto, S.; Morikawa, M.; Shiino, T.; Tamaji, A.; Ohoka, H.; Banno, N.; et al. Factor structure of the Japanese version of the Edinburgh postnatal depression scale in the postpartum period. PLoS ONE 2014, 9, e103941. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
| Mean (SD) or N (%) | T1 Depression | T2 Depression | |
|---|---|---|---|
| Demographic and obstetric variables | |||
| Age | 32.2 (4.2) | 0.013 | −0.009 |
| Gestational age | 13.2 (1.1) | −0.042 | 0.112 |
| Gravidity | 1.8 (1.1) | −0.175 * | −0.087 |
| Primipara | 131 (53.5) | --- | --- |
| Infertility treatment | 85 (34.7) | --- | --- |
| Have a partner | 243 (99.2) | --- | --- |
| Borderline personality traits | |||
| T1 Primitive defense | 4.44 (3.66) | 0.403 * | 0.352 * |
| T1 Identity diffusion | 7.34 (4.73) | 0.428 * | 0.355 * |
| T1 Reality testing | 1.58 (2.64) | 0.231 * | 0.332 * |
| T1 Total | 13.4 (9.3) | 0.440 * | 0.412 * |
| Adult attachment | |||
| T1 Total | −2.3 (3.9) | 0.306 * | 0.271 * |
| Perception of the impact of the current pregnancy | |||
| Perceived impact of pregnancy | 84.0 (27.7) | −0.452 * | −0.364 * |
| Fear of child birth | |||
| T1 Total | 62.0 (20.3) | 0.428 * | 0.395 * |
| T2 Total | 66.0 (21.4) | 0.358 * | 0.425 * |
| Obsessive-compulsive symptoms | |||
| T1 Total | 27.4 (16.8) | 0.448 * | 0.366 * |
| T2 Total | 28.1 (17.6) | 0.399 * | 0.427 * |
| Perceived threat of COVID-19 | |||
| T1 Perceived threat | 13.1 (3.6) | −0.048 | −0.091 |
| 1. Depression | 2. Borderline Personality Traits | 3. Adult Attachment | 4. Perceived Impact of Pregnancy | 5. W-DEQ | 6. OCI-R | 7. Perceived Threat | |
|---|---|---|---|---|---|---|---|
| 1. | --- | 0.412 * | 0.271 * | −0.364 * | 0.425 * | 0.427 * | −0.174 * |
| 2. | 0.440 * | --- | --- | --- | --- | --- | --- |
| 3. | 0.306 * | 0.431 * | --- | --- | --- | --- | --- |
| 4. | −0.452 * | −0.314 * | −0.278 * | --- | --- | --- | --- |
| 5. | 0.428 * | 0.453 * | 0.302 * | −0.465 * | --- | 0.427 * | 0.023 |
| 6. | 0.448 * | 0.621 * | 0.318 * | −0.240 * | 0.465 * | --- | 0.009 |
| 7. | −0.094 | −0.007 | 0.101 | 0.042 | −0.003 | 0.061 | --- |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Usui, Y.; Takegata, M.; Takeda, S.; Kitamura, T. Relationships between Depression, Fear of Childbirth, and Obsessive-Compulsive Symptoms among Pregnant Women under the COVID-19 Pandemic in Japan. Healthcare 2023, 11, 361. https://doi.org/10.3390/healthcare11030361
Usui Y, Takegata M, Takeda S, Kitamura T. Relationships between Depression, Fear of Childbirth, and Obsessive-Compulsive Symptoms among Pregnant Women under the COVID-19 Pandemic in Japan. Healthcare. 2023; 11(3):361. https://doi.org/10.3390/healthcare11030361
Chicago/Turabian StyleUsui, Yuriko, Mizuki Takegata, Satoru Takeda, and Toshinori Kitamura. 2023. "Relationships between Depression, Fear of Childbirth, and Obsessive-Compulsive Symptoms among Pregnant Women under the COVID-19 Pandemic in Japan" Healthcare 11, no. 3: 361. https://doi.org/10.3390/healthcare11030361