
Self-Perceived Physical Activity and Adherence to the Mediterranean Diet in Healthy Adolescents during COVID-19: Findings from the DIMENU Pilot Study

 , and
, and
Abstract
:
1. Introduction
2. Materials and Methods
2.1. Survey Development
2.2. Questionnaire
2.3. Statistical Analysis
3. Results
3.1. Description of Study Sample
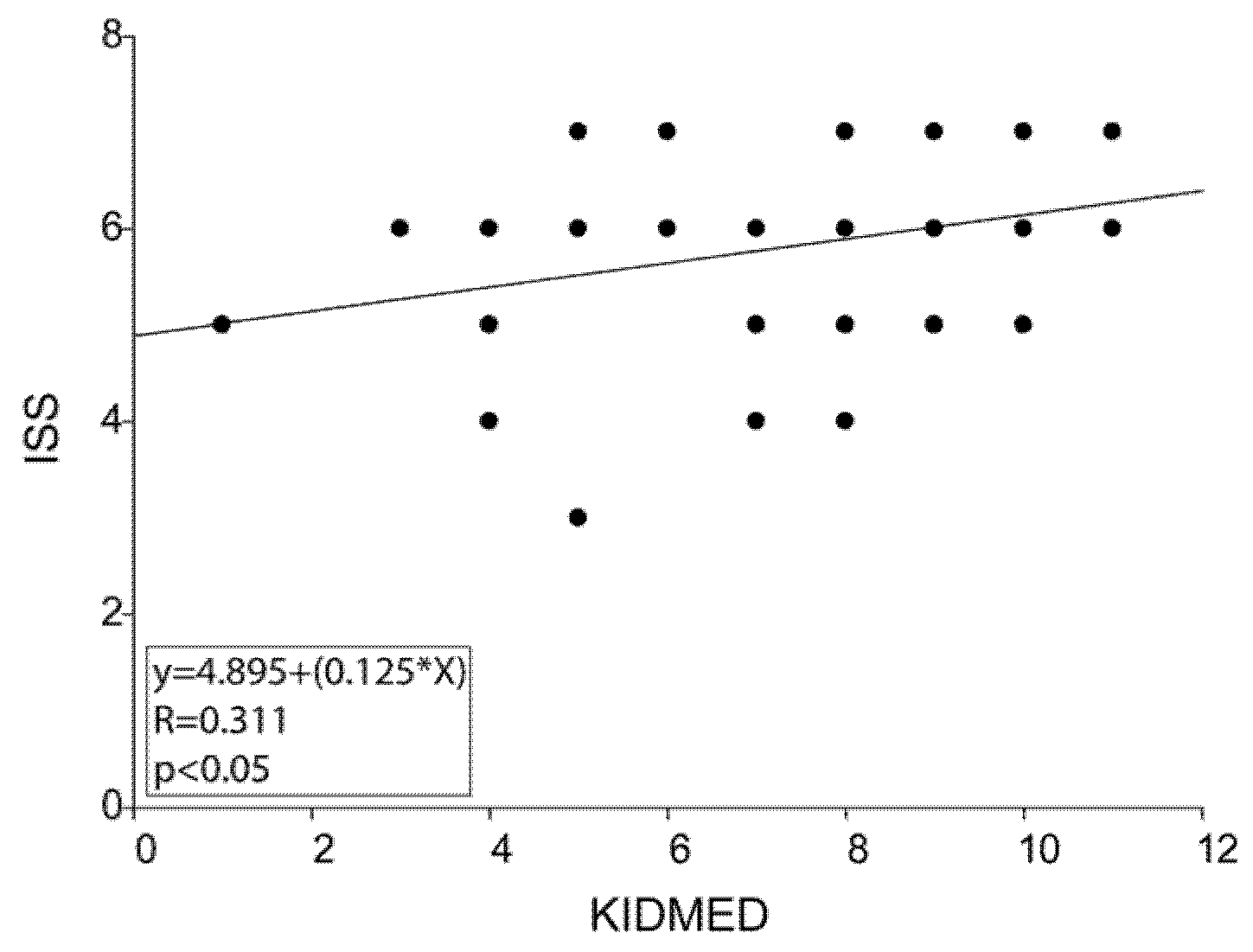
3.2. Multiple Regression Analysis with KIDMED or Lifestyle and ISS, Age, and Sex
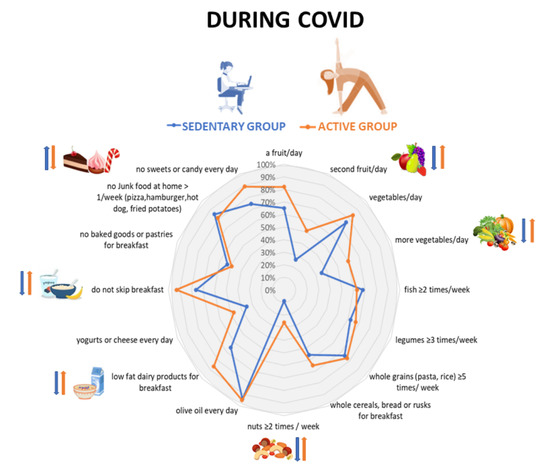
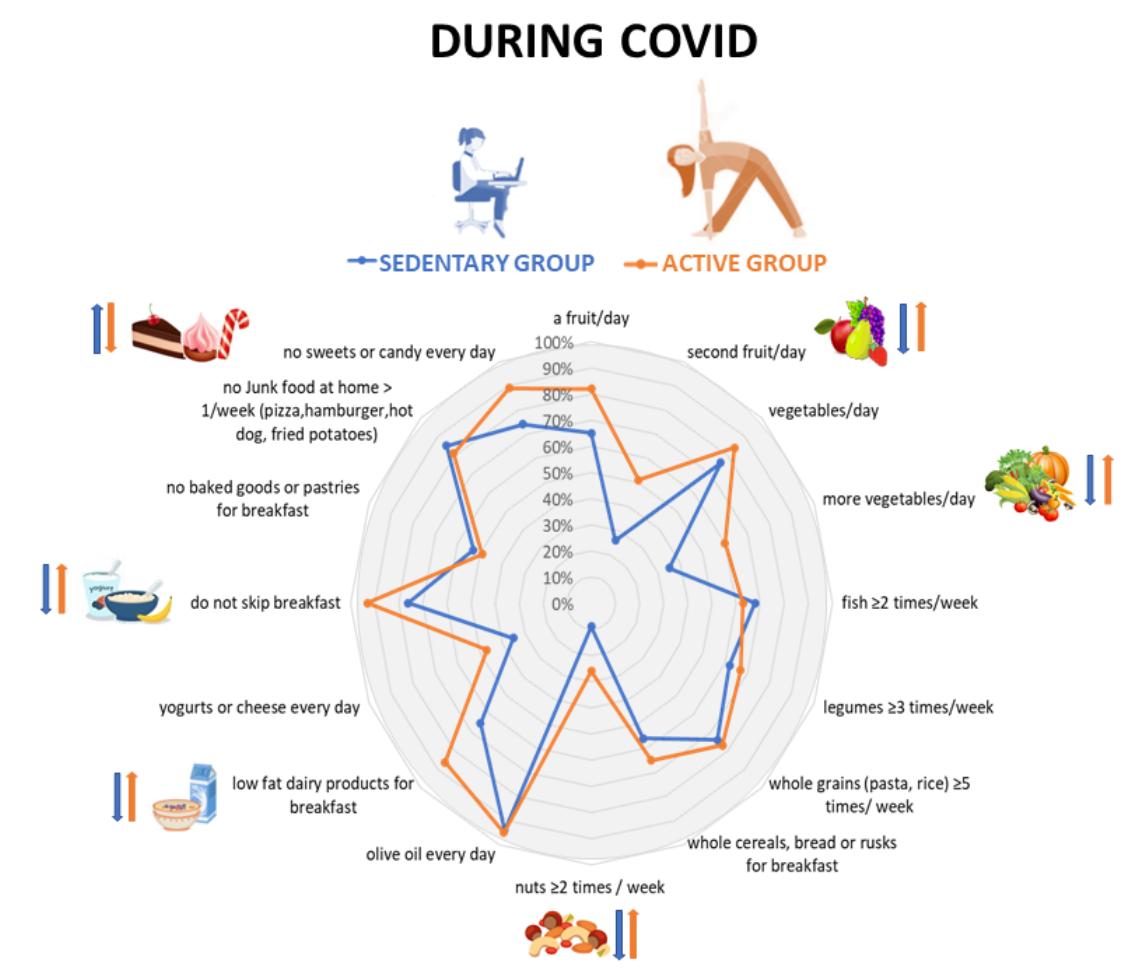
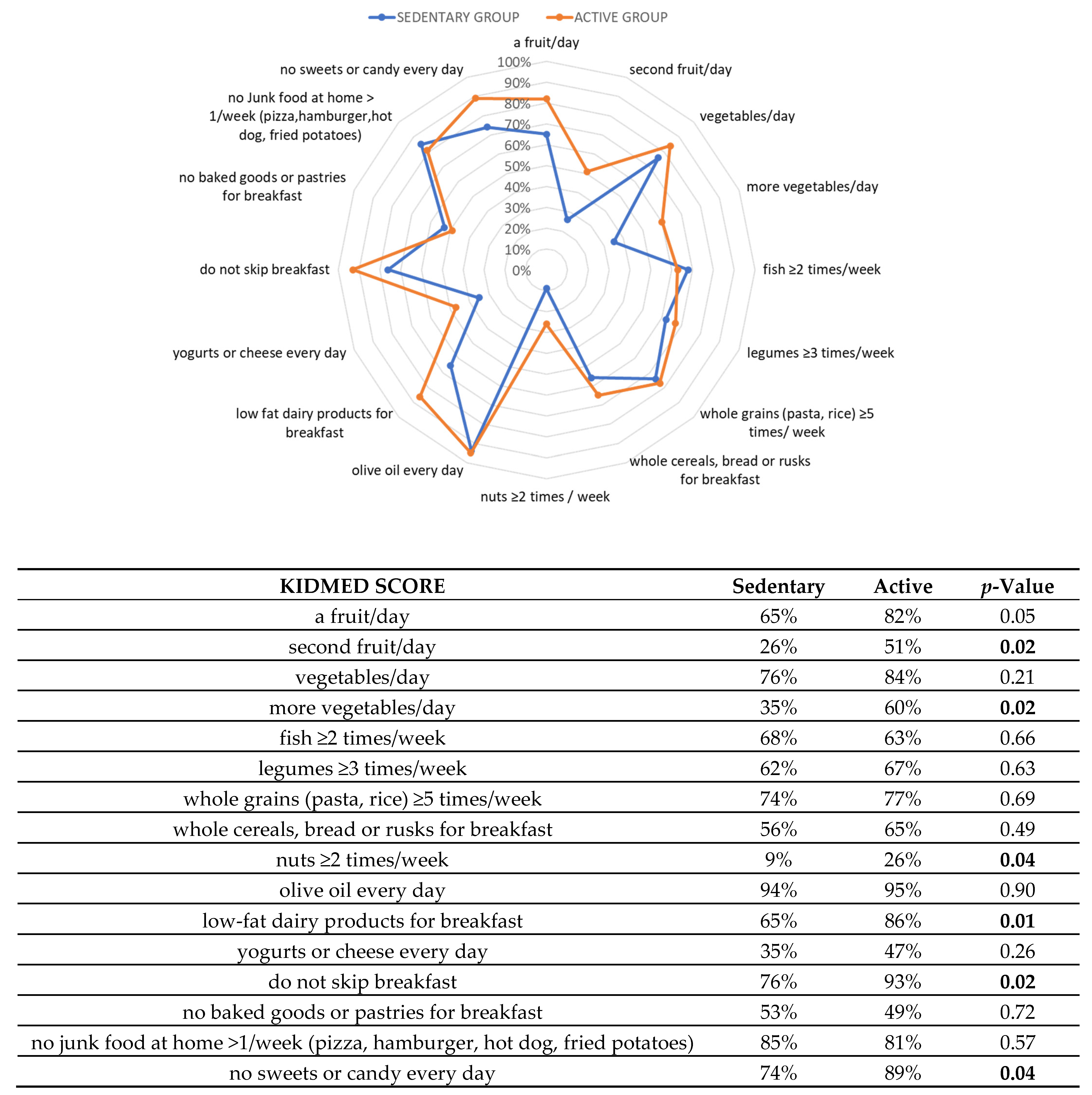
3.3. Dietary and Physical Activity Behaviors in Sedentary and Active Adolescents during the Lockdown Period
3.4. Self-Perceived Physical Activity and the Relation to Life Satisfaction in Sedentary and Active Adolescents during the COVID-19 Lockdown
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
| KIDMED SCORE | |||
|---|---|---|---|
| 1. | Takes a fruit or fruit juice every day | Yes/No | |
| 2. | Has a second fruit every day | Yes/No | |
| 3. | Has fresh or cooked vegetables regularly once a day | Yes/No | |
| 4. | Has fresh or cooked vegetables more than once a day | Yes/No | |
| 5. | Consumes fish regularly (≥2 times/week) | Yes/No | |
| 6. | Likes legumes and eats them ≥3 times/week | Yes/No | |
| 7. | Consumes whole grains (pasta or rice) almost every day or ≥5 times/week | Yes/No | |
| 8. | Has whole cereals or grains (bread or rusks) for breakfast | Yes/No | |
| 9. | Consumes nuts regularly (every day) | Yes/No | |
| 10. | Uses olive oil at home | Yes/No | |
| 11. | Has a low-fat dairy product for breakfast (yogurt, milk, etc.) | Yes/No | |
| 12. | Takes two yogurts and/or some cheese (40 g) daily | Yes/No | |
| 13. | Skips breakfast | Yes/No | |
| 14. | Has commercially baked goods or pastries for breakfast | Yes/No | |
| 15. | Goes > 1/week to a fast-food restaurant (hamburger) | Yes/No | |
| 16. | Takes sweets and candy several times every day | Yes/No | |
| ISS SCORE | |||
| 17. | Are you exercising at least 1 h a day at home? | Yes/No | |
| 18. | Currently in your free time, do you spend a maximum of 2 h a day on your PC/tablet/TV/smartphone? (excluding the time you dedicate to studying) | Yes/No | |
| 19. | Is physical activity currently performed at home (at least 1 h) 3 times a week? | Yes/No | |
| 20. | Having to stay at home all day, do you respect a night’s rest of at least 6–8 h? | Yes/No | |
| 21. | Are you dedicating time to some hobbies? (music, reading, drawing, creative activities) | Yes/No | |
| 22. | Are you helping the family with some housework? (dusting, making the bed, setting the table) | Yes/No | |
| 23. | Are you using the web to integrate your study activity with other cultural activities? | Yes/No | |
| PERCEPTION OF CHANGES IN LIFESTYLE AND EATING HABITS AT HOME. | |||
| 24. | How do you define your lifestyle currently? | Active Sedentary | |
| 25. | In this period, how do you consider physical activity practiced at home? | Tiring Boring It makes me feel good It temps me to continue in the sport | |
| 26. | During this period does your eating habits changed? | Yes/No | |
| 27. | During this period how many meals/day do you have? | 1–2 meal/day 3 meals/day 4 meals/day 5 meals/day | |
| 28. | Do you drink at least 2 L/day of water? | Yes/No | |
| 29. | Before COVID-19 emergency did you practice regularly physical activity or did you gradually start exercising at home? | Yes, I practiced physical activity regularly and I am continuing it at home Yes I practiced physical activity regularly but I’m NOT continuing it at home Yes I gradually started exercising at homeNone of the above | |
| 30. | What kind of physical activity are you doing? | Bodyweight exercises/jumping rope/running or tapis roullant or cyclette/abdominal exercises/step/exercise with objects at home/squat/or lunges or buttocks or legs exercises/push-ups/exergame/stretching/weight training | |
References
- Velavan, T.P.; Meyer, C.G. The COVID-19 epidemic. Trop. Med. Int. Health 2020, 25, 278–280. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lesser, I.A.; Nienhuis, C.P. The Impact of COVID-19 on Physical Activity Behavior and Well-Being of Canadians. Int. J. Environ. Res. Public Health 2020, 17, 3899. [Google Scholar] [CrossRef]
- Government, I. Nuovo Coronavirus. Available online: http://www.salute.gov.it/portale/nuovocoronavirus/dettaglioFaqNuovoCoronavirus.jsp?lingua=italiano&id=228#11 (accessed on 7 May 2020).
- Chen, P.; Mao, L.; Nassis, G.P.; Harmer, P.; Ainsworth, B.E.; Li, F. Coronavirus disease (COVID-19): The need to maintain regular physical activity while taking precautions. J. Sport Health Sci. 2020, 9, 103–104. [Google Scholar] [CrossRef]
- Ammar, A.; Brach, M.; Trabelsi, K.; Chtourou, H.; Boukhris, O.; Masmoudi, L.; Bouaziz, B.; Bentlage, E.; How, D.; Ahmed, M.; et al. Effects of COVID-19 Home Confinement on Eating Behaviour and Physical Activity: Results of the ECLB-COVID19 International Online Survey. Nutrients 2020, 12, 1583. [Google Scholar] [CrossRef] [PubMed]
- Stockwell, S.T.M.; Tully, M.; Shin, J.; Barnett, Y.; Butler, L.; McDermott, D.; Schuch, F.; Smith, L. Changes in physical activity and sedentary behaviours from before to during the COVID-19 pandemic lockdown: A systematic review. BMJ Open Sport Exerc. Med. 2021, 1, e000960. [Google Scholar] [CrossRef]
- Hoffmann, B.; Kobel, S.; Wartha, O.; Kettner, S.; Dreyhaupt, J.; Steinacker, J.M. High sedentary time in children is not only due to screen media use: A cross-sectional study. BMC Pediatr. 2019, 19, 154. [Google Scholar] [CrossRef]
- Celis-Morales, C.; Salas-Bravo, C.; Yanez, A.; Castillo, M. Physical inactivity and sedentary lifestyle-The other side of the side effects of the COVID-19 Pandemic. Rev. Med. Chile 2020, 148, 885–886. [Google Scholar] [CrossRef] [PubMed]
- Ruiz-Roso, M.B.; de Carvalho Padilha, P.; Matilla-Escalante, D.C.; Brun, P.; Ulloa, N.; Acevedo-Correa, D.; Arantes Ferreira Peres, W.; Martorell, M.; Rangel Bousquet Carrilho, T.; de Oliveira Cardoso, L.; et al. Changes of Physical Activity and Ultra-Processed Food Consumption in Adolescents from Different Countries during Covid-19 Pandemic: An Observational Study. Nutrients 2020, 12, 2289. [Google Scholar] [CrossRef]
- Pietrobelli, A.; Pecoraro, L.; Ferruzzi, A.; Heo, M.; Faith, M.; Zoller, T.; Antoniazzi, F.; Piacentini, G.; Fearnbach, S.N.; Heymsfield, S.B. Effects of COVID-19 Lockdown on Lifestyle Behaviors in Children with Obesity Living in Verona, Italy: A Longitudinal Study. Obesity (Silver Spring) 2020, 28, 1382–1385. [Google Scholar] [CrossRef] [PubMed]
- Ruiz-Roso, M.B.; de Carvalho Padilha, P.; Mantilla-Escalante, D.C.; Ulloa, N.; Brun, P.; Acevedo-Correa, D.; Arantes Ferreira Peres, W.; Martorell, M.; Aires, M.T.; de Oliveira Cardoso, L.; et al. Covid-19 Confinement and Changes of Adolescent's Dietary Trends in Italy, Spain, Chile, Colombia and Brazil. Nutrients 2020, 12, 1807. [Google Scholar] [CrossRef]
- Morelli, C.; Avolio, E.; Galluccio, A.; Caparello, G.; Manes, E.; Ferraro, S.; De Rose, D.; Santoro, M.; Barone, I.; Catalano, S.; et al. Impact of Vigorous-Intensity Physical Activity on Body Composition Parameters, Lipid Profile Markers, and Irisin Levels in Adolescents: A Cross-Sectional Study. Nutrients 2020, 12, 742. [Google Scholar] [CrossRef] [Green Version]
- Willett, W.; Rockstrom, J.; Loken, B.; Springmann, M.; Lang, T.; Vermeulen, S.; Garnett, T.; Tilman, D.; DeClerck, F.; Wood, A.; et al. Food in the Anthropocene: The EAT-Lancet Commission on healthy diets from sustainable food systems. Lancet 2019, 393, 447–492. [Google Scholar] [CrossRef]
- Garcia Cabrera, S.; Herrera Fernandez, N.; Rodriguez Hernandez, C.; Nissensohn, M.; Roman-Vinas, B.; Serra-Majem, L. Kidmed Test; Prevalence of Low Adherence to the Mediterranean Diet in Children and Young; a Systematic Review. Nutr. Hosp. 2015, 32, 2390–2399. [Google Scholar] [CrossRef]
- Revitalizing the Mediterranean Diet from a Healthy Dietary Pattern to a Healthy Mediterranean Sustainable Lifestyle. Available online: http://www.ifmed.org/1st-world-conference-on-the-mediterranean-diet/ (accessed on 30 October 2020).
- Anche Gli Adolescenti si Muovono a Casa. Available online: https://www.epicentro.iss.it/coronavirus/sars-cov-2-stili-vita-attivita-fisica-12-17-anni (accessed on 9 February 2021).
- Caparello, G.; Galluccio, A.; Giordano, C.; Lofaro, D.; Barone, I.; Morelli, C.; Sisci, D.; Catalano, S.; Ando, S.; Bonofiglio, D. Adherence to the Mediterranean diet pattern among university staff: A cross-sectional web-based epidemiological study in Southern Italy. Int. J. Food Sci. Nutr. 2020, 71, 581–592. [Google Scholar] [CrossRef]
- Dragun, R.; Vecek, N.N.; Marendic, M.; Pribisalic, A.; Divic, G.; Cena, H.; Polasek, O.; Kolcic, I. Have Lifestyle Habits and Psychological Well-Being Changed among Adolescents and Medical Students Due to COVID-19 Lockdown in Croatia? Nutrients 2020, 13, 97. [Google Scholar] [CrossRef] [PubMed]
- Glabska, D.; Skolmowska, D.; Guzek, D. Population-Based Study of the Changes in the Food Choice Determinants of Secondary School Students: Polish Adolescents' COVID-19 Experience (PLACE-19) Study. Nutrients 2020, 12, 2640. [Google Scholar] [CrossRef] [PubMed]
- Bates, L.C.; Zieff, G.; Stanford, K.; Moore, J.B.; Kerr, Z.Y.; Hanson, E.D.; Barone Gibbs, B.; Kline, C.E.; Stoner, L. COVID-19 Impact on Behaviors across the 24-Hour Day in Children and Adolescents: Physical Activity, Sedentary Behavior, and Sleep. Children 2020, 7, 138. [Google Scholar] [CrossRef] [PubMed]
- Janssen, I.; Leblanc, A.G. Systematic review of the health benefits of physical activity and fitness in school-aged children and youth. Int. J. Behav. Nutr. Phys. Act. 2010, 7, 40. [Google Scholar] [CrossRef] [Green Version]
- Saunders, T.J.; Gray, C.E.; Poitras, V.J.; Chaput, J.P.; Janssen, I.; Katzmarzyk, P.T.; Olds, T.; Connor Gorber, S.; Kho, M.E.; Sampson, M.; et al. Combinations of physical activity, sedentary behaviour and sleep: Relationships with health indicators in school-aged children and youth. Appl. Physiol. Nutr. Metab. 2016, 41, S283–S293. [Google Scholar] [CrossRef] [Green Version]
- WHO. Physical Activity. Available online: https://www.who.int/news-room/fact-sheets/detail/physical-activity#:~:text=Children%20and%20adolescents%20aged%205,least%203%20days%20a%20week (accessed on 9 February 2021).
- Iannotti, R.J.; Kogan, M.D.; Janssen, I.; Boyce, W.F. Patterns of adolescent physical activity, screen-based media use, and positive and negative health indicators in the U.S. and Canada. J. Adolesc. Health 2009, 44, 493–499. [Google Scholar] [CrossRef] [Green Version]
- Leung, M.M.; Agaronov, A.; Grytsenko, K.; Yeh, M.C. Intervening to Reduce Sedentary Behaviors and Childhood Obesity among School-Age Youth: A Systematic Review of Randomized Trials. J. Obes. 2012, 2012, 685430. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wu, X.Y.; Han, L.H.; Zhang, J.H.; Luo, S.; Hu, J.W.; Sun, K. The influence of physical activity, sedentary behavior on health-related quality of life among the general population of children and adolescents: A systematic review. PLoS ONE 2017, 12, e0187668. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- ISS. Teenagers Can also Take Exercise at Home. Available online: https://www.epicentro.iss.it/en/coronavirus/pdf/physical-activity-at-home-for-adolescents-12-17-yy.pdf (accessed on 9 February 2021).
- UNICAL. Coronavirus, I Consigli Degli Esperti per uno Stile di Vita Salutare. Available online: https://www.unical.it/portale/portaltemplates/view/view.cfm?98612 (accessed on 9 February 2021).
- Dieta Mediterranea e Nuoto. Available online: https://www.dimenu.it/ (accessed on 9 February 2021).
- Dieta Mediterranea e Nuoto Facebook Page. Available online: https://www.facebook.com/dimenu2019 (accessed on 9 February 2021).
- Pigaiani, Y.; Zoccante, L.; Zocca, A.; Arzenton, A.; Menegolli, M.; Fadel, S.; Ruggeri, M.; Colizzi, M. Adolescent Lifestyle Behaviors, Coping Strategies and Subjective Wellbeing during the COVID-19 Pandemic: An Online Student Survey. Healthcare 2020, 8, 472. [Google Scholar] [CrossRef] [PubMed]
- Ardeshirlarijani, E.; Namazi, N.; Jabbari, M.; Zeinali, M.; Gerami, H.; Jalili, R.B.; Larijani, B.; Azadbakht, L. The link between breakfast skipping and overweigh/obesity in children and adolescents: A meta-analysis of observational studies. J. Diabetes Metab. Disord. 2019, 18, 657–664. [Google Scholar] [CrossRef] [PubMed]
- Morelli, C.; Avolio, E.G.; Caparello, G.; Manes, E.; Ferraro, S.; Caruso, A.; De Rose, D.; Barone, I.; Adornetto, C. Nutrition Education Program and Physical Activity affect the Adherence to the Mediterranean Diet and associate with lower Inflammatory Biomarker levels in Healthy Adolescents: The DIMENU longitudinal study. Front. Nutr. 2021. under review. [Google Scholar]
- Naja, F.; Hamadeh, R. Nutrition amid the COVID-19 pandemic: A multi-level framework for action. Eur. J. Clin. Nutr. 2020, 74, 1117–1121. [Google Scholar] [CrossRef] [PubMed] [Green Version]


| Characteristics | Total Sample | Girls | Boys |
|---|---|---|---|
| Subjects (number) | 91 | 42 (46%) | 49 (54%) |
| Age (years ± SD, range) | 16.60 ± 1.28 (13–19) | 16.83 ± 1.27 (14–18) | 16.40 ± 1.26 (13–19) |
| Current lifestyle | |||
| Sedentary | 34 (37%) | 18 (20%) | 16 (17%) |
| Active | 57 (63%) | 25 (26%) | 32 (37%) |
| ISS score (M ± SD, range) | 5.37 ± 1.19 (1–7) | 5.23 ± 1.1 (1–7) | 5.49 ± 1.27 (3–7) |
| Low (0–3) | 20 (22%) | 11 (26%) | 9 (18%) |
| High (4–7) | 71 (78%) | 31 (74%) | 40 (82%) |
| Eating habits change | 34 (37%) | 17 (41%) | 17 (35%) |
| Meals/day | |||
| 1–2 meals/day | 4 (4%) | 0 | 4 (8%) |
| 3 meals/day | 28 (31%) | 15 (36%) | 13 (27%) |
| 4 meals/day | 35 (39%) | 15 (36%) | 20 (41%) |
| 5 meals/day | 24 (26%) | 12 (28%) | 12 (24%) |
| KIDMED score (M ± SD, range) | 6.52 ± 2.45 (0–11) | 6.28 ± 2.68 (1–11) | 6.73 ± 2.24 (0–11) |
| Optimal adherence (≥8) | 37 (41%) | 16 (38%) | 21 (43%) |
| Medium adherence (4–7) | 45 (49%) | 20 (48%) | 25 (51%) |
| Poor adherence (≤3) | 9 (10%) | 6 (14%) | 3 (6%) |
| Variables | KIDMED | Lifestyle Habits | ||||
|---|---|---|---|---|---|---|
| β | se | p-Value | β | se | p-Value | |
| ISS | 0.375 | 0.206 | <0.001 | 0.432 | 0.039 | <0.001 |
| Age | 0.140 | 0.194 | 0.170 | −0.087 | 0.037 | 0.373 |
| Sex | 0.076 | 0.491 | 0.454 | 0.045 | 0.093 | 0.642 |
| R = 0.388 | R2 = 0.151 | Adj R2 = 0.122 | R = 0.463 | R2 = 0.215 | Adj R2 = 0.188 | |
| Characteristics | Total Sample (n = 91) | p-Value | |
|---|---|---|---|
| Sedentary (n = 34) | Active (n = 57) | ||
| Age (years ± SD, range) | 16.88 ± 1.26 (15–19) | 16.43 ± 1.28 (13–19) | 0.1063 |
| ISS score (M ± SD, range) | 4.67 ± 1.22 (1–7) | 5.78 ± 1.2 (3–7) | 0.0001 |
| Low (0–3) | 6 (18%) | 1 (2%) | 0.005 |
| High (4–7) | 28 (82%) | 56 (98%) | 0.005 |
| Eating habits change | 16 (47%) | 18 (31%) | 0.1398 |
| Meals/day | |||
| 1–2 meals/day | 2 (6%) | 2 (4%) | 0.5931 |
| 3 meals/day | 12 (35%) | 16 (28%) | 0.4701 |
| 4 meals/day | 13 (38%) | 22 (39%) | 0.9727 |
| 5 meals/day | 7 (21%) | 17 (30%) | 0.3334 |
| KIDMED score (M ± SD, range) | 5.5 ± 2.47 (0–10) | 7.14 ± 2.45 (1–11) | 0.0028 |
| Optimal adherence (≥8) | 8 (23%) | 29 (51%) | 0.01 |
| Medium adherence (4–7) | 20 (59%) | 25 (44%) | 0.1672 |
| Poor adherence (≤3) | 6 (18%) | 3 (5%) | 0.05 |
| ISS Questionnaire | Sedentary | Active | p-Value |
|---|---|---|---|
| Are you exercising at least 1 h a day at home? | 14 (41%) | 51 (89%) | 0.00001 |
| Currently in your free time, do you spend a maximum of 2 h a day on your PC/tablet/TV/smartphone? (excluding the time, you dedicate to studying) | 21 (62%) | 44 (77%) | 0.1150 |
| Is physical activity currently performed at home (at least 1 h) 3 times a week? | 20 (59%) | 53 (93%) | 0.00007 |
| Having to stay at home all day, do you respect a night’s rest of at least 6–8 h? | 27 (79%) | 54 (95%) | 0.02 |
| Are you dedicating time to some hobbies? (music, reading, drawing, creative activities) | 28 (82%) | 50 (88%) | 0.4791 |
| Are you helping the family with some housework? (dusting, making the bed, setting/clearing the table) | 29 (85%) | 55 (96%) | 0.05 |
| Are you using the web to integrate your study activity with other cultural activities? | 18 (53%) | 22 (39%) | 0.1822 |
| ITEMS | Sedentary | Active | p-Value |
|---|---|---|---|
| Yes, I practiced physical activity regularly and I am continuing it at home | 12 (35%) | 43 (75%) | 0.0001 |
| Yes, I practiced physical activity regularly but I’m NOT continuing it at home | 14 (41%) | 1 (2%) | 0.00001 |
| Yes, I gradually started exercising at home | 7 (21%) | 12 (21%) | 0.9579 |
| None of the above | 1 (3%) | 1 (2%) | 0.8833 |
| In this Period, How Do You Consider Physical Activity Practiced at Home? | Sedentary | Active | p-Value |
|---|---|---|---|
| Tiring | 3 (9%) | 2 (3%) | 0.2817 |
| Boring | 15 (44%) | 9 (16%) | 0.003 |
| It makes me feel good | 11 (32%) | 31 (58%) | 0.01 |
| It temps me to continue in the sport | 5 (15%) | 13 (23%) | 0.3479 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Galluccio, A.; Caparello, G.; Avolio, E.; Manes, E.; Ferraro, S.; Giordano, C.; Sisci, D.; Bonofiglio, D. Self-Perceived Physical Activity and Adherence to the Mediterranean Diet in Healthy Adolescents during COVID-19: Findings from the DIMENU Pilot Study. Healthcare 2021, 9, 622. https://doi.org/10.3390/healthcare9060622
Galluccio A, Caparello G, Avolio E, Manes E, Ferraro S, Giordano C, Sisci D, Bonofiglio D. Self-Perceived Physical Activity and Adherence to the Mediterranean Diet in Healthy Adolescents during COVID-19: Findings from the DIMENU Pilot Study. Healthcare. 2021; 9(6):622. https://doi.org/10.3390/healthcare9060622
Chicago/Turabian StyleGalluccio, Angelo, Giovanna Caparello, Ennio Avolio, Emanuele Manes, Simona Ferraro, Cinzia Giordano, Diego Sisci, and Daniela Bonofiglio. 2021. "Self-Perceived Physical Activity and Adherence to the Mediterranean Diet in Healthy Adolescents during COVID-19: Findings from the DIMENU Pilot Study" Healthcare 9, no. 6: 622. https://doi.org/10.3390/healthcare9060622