
SARS-CoV-2 Vaccination Rate and SARS-CoV-2 Infection of Health Care Workers in Aerosol-Generating Medical Disciplines

 , , , ,
, , , ,  , ,
, ,  , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Statistical Analysis
3. Results
3.1. Sample Characteristics
3.2. HCW Infection Rate
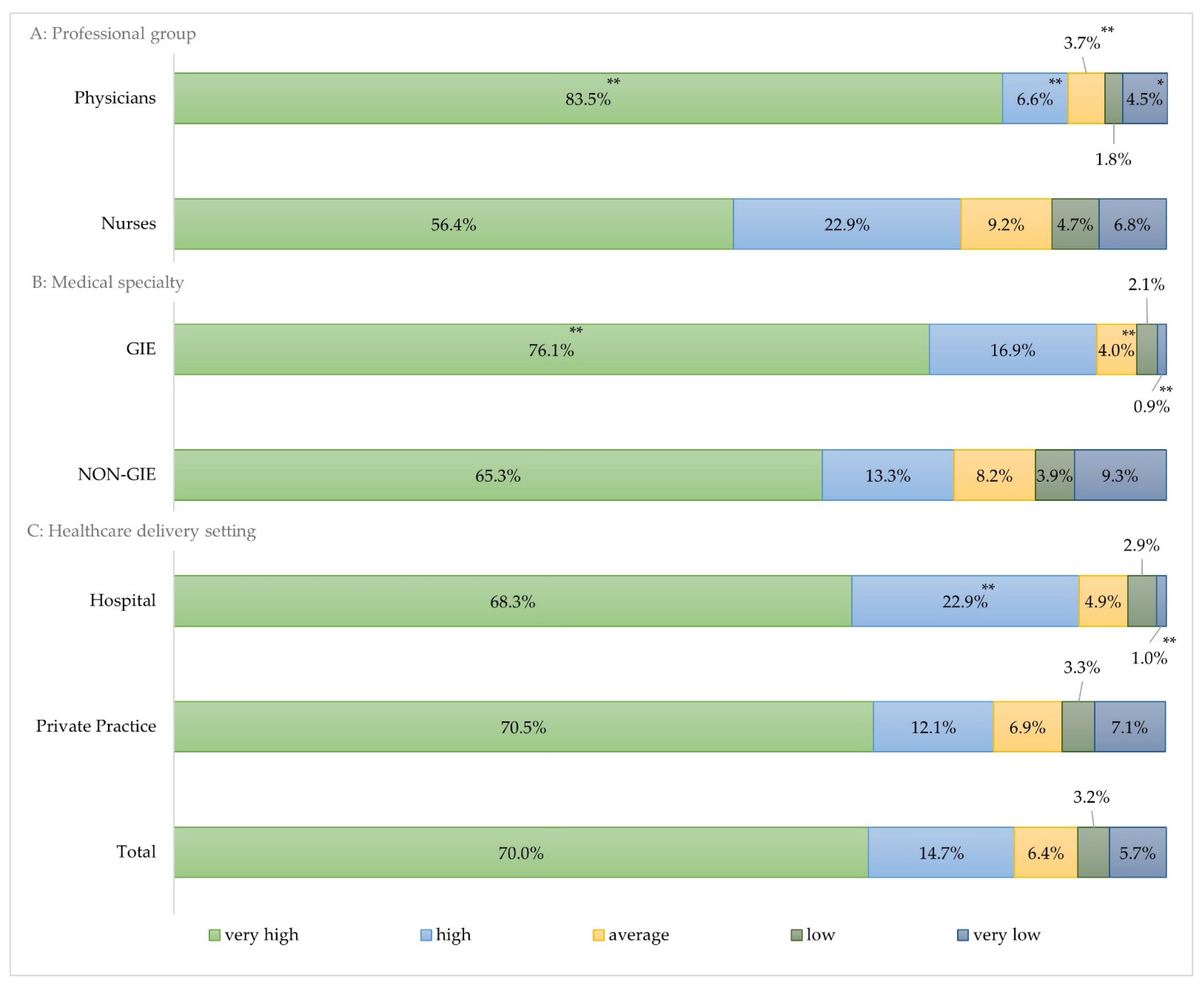
3.3. Perceived Risk of Infection among HCW
3.4. Vaccination Rates among HCW
3.5. Vaccination Rates Depending on Perceived Risk of SARS-CoV-2 Infection
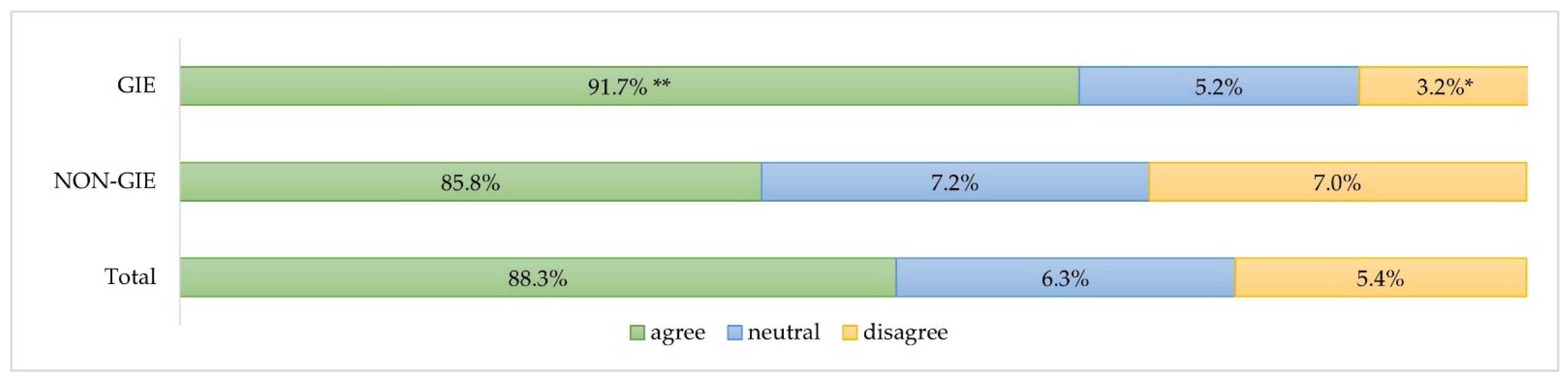
3.6. Perceived Vaccination Protection among Fully Vaccinated Study Participants
4. Discussion
4.1. Vaccination Rates in Professional Groups
4.2. Infection Rate
4.3. Limitations
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Cucinotta, D.; Vanelli, M. WHO Declares COVID-19 a Pandemic. Acta Biomed. 2020, 91, 157–160. [Google Scholar] [CrossRef] [PubMed]
- John Hopkins Coronavirus Resource Center. 2021. Available online: https://coronavirus.jhu.edu/map.html (accessed on 6 April 2022).
- Vygen-Bonnet, S.; Koch, J.; Bogdan, C.; Harder, T.; Heininger, U.; Kling, K.; Littmann, M.; Meerpohl, J.; Meyer, H.; Mertens, T.; et al. Beschluss und Wissenschaftliche Begründung der Ständigen Impfkommission (STIKO) für die COVID-19-Impfempfehlung. Epid. Bull. 2020, 2, 3–63. [Google Scholar] [CrossRef]
- Waize, M.; Scholz, S.; Wichmann, O.; Harder, T.; Treskova-Schwarzbach, M.; Falman, A.; Weidemann, F.; Karch, A.; Lange, B.; Kuhlmann, A.; et al. Die Impfung gegen COVID-19 in Deutschland zeigt eine hohe Wirksamkeit gegen SARS-CoV-2-Infektionen, Krankheitslast und Sterbefälle. Epid. Bull. 2021, 35, 3–10. [Google Scholar] [CrossRef]
- Jespersen, S.; Mikkelsen, S.; Greve, T.; Kaspersen, K.A.; Tolstrup, M.; Boldsen, J.K.; Redder, J.D.; Nielsen, K.; Abildgaard, A.M.; Kolstad, H.A.; et al. SARS-CoV-2 seroprevalence survey among 17,971 healthcare and administrative personnel at hospitals, pre-hospital services, and specialist practitioners in the Central Denmark Region. Clin. Infect. Dis. 2020, 73, e2853–e2860. [Google Scholar] [CrossRef]
- Chou, R.; Dana, T.; Buckley, D.I.; Selph, S.; Fu, R.; Totten, A.M. Update Alert 3: Epidemiology of and Risk Factors for Coronavirus Infection in Health Care Workers. Ann. Intern. Med. 2020, 173, W123–W124. [Google Scholar] [CrossRef]
- Sallam, M. COVID-19 Vaccine Hesitancy Worldwide: A Concise Systematic Review of Vaccine Acceptance Rates. Vaccines 2021, 9, 160. [Google Scholar] [CrossRef]
- Campbell, F.; Archer, B.; Laurenson-Schafer, H.; Jinnai, Y.; Konings, F.; Batra, N.; Pavlin, B.; Vandemaele, K.; Van Kerkhove, M.D.; Jombart, T.; et al. Increased transmissibility and global spread of SARS-CoV-2 variants of concern as at June 2021. Eurosurveillance 2021, 26, 2100509. [Google Scholar] [CrossRef]
- Neuzil, K.M. Interplay between Emerging SARS-CoV-2 Variants and Pandemic Control. N. Engl. J. Med. 2021, 384, 1952–1954. [Google Scholar] [CrossRef]
- Römmele, C.; Ebigbo, A.; Kahn, M.; Zellmer, S.; Muzalyova, A.; Hammel, G.; Breitling, L.P.; Bartenschlager, C.; Beyer, A.; Rosendahl, J.; et al. SARS-CoV-2-Infektionsrisiko und Seroprävalenz bei Mitarbeitern des Gesundheitswesens in aerosolerzeugenden Tätigkeiten in Deutschland. Z. Gastroenterol. 2021, 59, e310. [Google Scholar] [CrossRef]
- Römmele, C.; Ebigbo, A.; Kahn, M.; Zellmer, S.; Muzalyova, A.; Hammel, G.; Bartenschlager, C.; Beyer, A.; Rosendahl, J.; Schlittenbauer, T.; et al. Health-care workers in gastrointestinal endoscopy are at higher risk for SARS-CoV-2 infection compared to other aerosol-generating disciplines. medRxiv 2021. [Google Scholar] [CrossRef]
- Mayer, M.; Zellmer, S.; Zenk, J.; Arens, C.; Ebigbo, A.; Muzalyova, A.; Thoelken, R.; Jering, M.; Kahn, M.; Breitling, L.P.; et al. Status quo after one year of COVID-19 pandemic in otolaryngological hospital-based departments and private practices in Germany. Eur. Arch. Otorhinolaryngol. 2021, 279, 1063–1070. [Google Scholar] [CrossRef] [PubMed]
- Zellmer, S.; Kahn, M.; Ebigbo, A.; Muzalyova, A.; Classen, J.; Grünherz, V.; Böser, J.; Breitling, L.P.; Beyer, A.; Rosendahl, J.; et al. Ein Jahr Covid-19: Testung, Verwendung von Schutzausrüstung und Auswirkungen auf die Gastrointestinale Endoskopie in Deutschland. Z. Gastroenterol. 2021, 59, 1278–1287. [Google Scholar] [CrossRef]
- Robert-Koch-Institut: SurvStat@RKI 2.0. 2021. Available online: https://survstat.rki.de/ (accessed on 22 January 2022).
- Bundesamt, D.S. Bevölkerungsstand: Amtliche Einwohnerzahl Deutschlands 2021. 2021. Available online: https://www.destatis.de/DE/Themen/Gesellschaft-Umwelt/Bevoelkerung/Bevoelkerungsstand/_inhalt.html (accessed on 9 December 2021).
- Lazarus, J.V.; Ratzan, S.C.; Palayew, A.; Gostin, L.O.; Larson, H.J.; Rabin, K.; Kimball, S.; El-Mohandes, A. A global survey of potential acceptance of a COVID-19 vaccine. Nat. Med. 2021, 27, 225–228. [Google Scholar] [CrossRef] [PubMed]
- Neumann-Bohme, S.; Varghese, N.E.; Sabat, I.; Barros, P.P.; Brouwer, W.; van Exel, J.; Schreyögg, J.; Stargardt, T. Once we have it, will we use it? A European survey on willingness to be vaccinated against COVID-19. Eur. J. Health Econ. 2020, 21, 977–982. [Google Scholar] [CrossRef] [PubMed]
- Dror, A.A.; Eisenbach, N.; Taiber, S.; Morozov, N.G.; Mizrachi, M.; Zigron, A.; Srouji, S.; Sela, E. Vaccine hesitancy: The next challenge in the fight against COVID-19. Eur. J. Epidemiol. 2020, 35, 775–779. [Google Scholar] [CrossRef]
- Gagneux-Brunon, A.; Detoc, M.; Bruel, S.; Tardy, B.; Rozaire, O.; Frappe, P.; Botelho-Nevers, E. Intention to get vaccinations against COVID-19 in French healthcare workers during the first pandemic wave: A cross-sectional survey. J. Hosp. Infect. 2021, 108, 168–173. [Google Scholar] [CrossRef]
- Biswas, N.; Mustapha, T.; Khubchandani, J.; Price, J.H. The Nature and Extent of COVID-19 Vaccination Hesitancy in Healthcare Workers. J. Community Health 2021, 46, 1244–1251. [Google Scholar] [CrossRef]
- Martin, C.; Montesinos, I.; Dauby, N.; Gilles, C.; Dahma, H.; Van Den Wijngaert, S.; De Wit, S.; Delforge, M.; Clumeck, N.; Vandenberg, O. Dynamics of SARS-CoV-2 RT-PCR positivity and seroprevalence among high-risk healthcare workers and hospital staff. J. Hosp. Infect. 2020, 106, 102–106. [Google Scholar] [CrossRef]
- Kambhampati, A.K.; O’Halloran, A.C.; Whitaker, M.; Magill, S.S.; Chea, N.; Chai, S.J.; Kirley, P.D.; Herlihy, R.K.; Kawasaki, B.; Meek, J.; et al. COVID-19-Associated Hospitalizations Among Health Care Personnel—COVID-NET, 13 States, March 1–May 31, 2020. MMWR Morb. Mortal. Wkly. Rep. 2020, 69, 1576–1583. [Google Scholar] [CrossRef]
- Delbaere, K.; Close, J.C.; Brodaty, H.; Sachdev, P.; Lord, S.R. Determinants of disparities between perceived and physiological risk of falling among elderly people: Cohort study. BMJ 2010, 341, c4165. [Google Scholar] [CrossRef]
- Gao, Z.; Xu, Y.; Sun, C.; Wang, X.; Guo, Y.; Qiu, S.; Ma, K. A systematic review of asymptomatic infections with COVID-19. J. Microbiol. Immunol. Infect. 2021, 54, 12–16. [Google Scholar] [CrossRef] [PubMed]
- WHO. WHO Concept for Fair Access and Equitable Allocation of COVID-19 Health Products. 2020. Available online: https://www.who.int/docs/default-source/coronaviruse/who-covid19-vaccine-allocation-final-working-version-9sept.pdf (accessed on 25 January 2022).
- Shehab, M.; Alrashed, F.; Shuaibi, S.; Alajmi, D.; Barkun, A. Gastroenterological and hepatic manifestations of patients with COVID-19, prevalence, mortality by country, and intensive care admission rate: Systematic review and meta-analysis. BMJ Open Gastroenterol. 2021, 8, e000571. [Google Scholar] [CrossRef] [PubMed]
- da Rosa Mesquita, R.; Francelino Silva Junior, L.C.; Santos Santana, F.M.; de Oliveira, T.F.; Campos Alcantara, R.; Monteiro Arnozo, G.; da Silva Filho, E.R.; dos Santos, A.G.G.; da Cunha, E.J.O.; de Aquino, S.H.S.; et al. Clinical manifestations of COVID-19 in the general population: Systematic review. Wien. Klin. Wochenschr. 2021, 133, 377–382. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Hospital | Private Practice | Total | |||||||
|---|---|---|---|---|---|---|---|---|---|
| n | % | HCW Number | n | % | HCW Number | n | % | HCW Number | |
| GIE | 146 | 17.5 | 2303 | 201 | 24.2 | 2184 | 347 | 41.7 | 4487 |
| NON-GIE | 49 | 5.9 | 2907 | 436 | 52.4 | 3818 | 485 | 58.3 | 6725 |
| Total | 195 | 23.4 | 5210 | 637 | 76.6 | 6002 | 832 | 100.0 | 11,212 |
| GIE | NON-GIE | Total | ||||
|---|---|---|---|---|---|---|
| n | % | n | % | n | % | |
| AGP treatment | 321 | 92.0 | 450 | 92.6 | 771 | 90.8 |
| Job-related contact frequency | 259 | 74.2 | 364 | 74.9 | 623 | 73.4 |
| Close contact with patients | 244 | 69.9 | 351 | 72.2 | 595 | 70.1 |
| Long stay with patients in the treatment room | 192 | 55.0 | 275 | 56.6 | 467 | 55.0 |
| Frequently asymptomatic courses of COVID-19 infection | 179 | 51.3 | 277 | 57.0 | 456 | 53.7 |
| Variants of concern (VOC) | 105 | 30.1 | 173 | 35.6 | 278 | 32.7 |
| Unreasonable patients | 118 | 33.8 | 155 | 31.9 | 273 | 32.2 |
| Low sensitivity of the rapid antigen test | 59 | 16.9 | 72 | 14.8 | 131 | 15.4 |
| GIE | NON-GIE | Total | ||||
|---|---|---|---|---|---|---|
| n | % | n | % | n | % | |
| Less concerns | 310 | 92.0 ** | 359 | 80.3 | 669 | 85.3 |
| Same concerns | 27 | 8.0 | 88 | 19.7 | 115 | 14.7 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Muzalyova, A.; Ebigbo, A.; Kahn, M.; Zellmer, S.; Beyer, A.; Rosendahl, J.; Zenk, J.; Al-Nawas, B.; Frankenberger, R.; Hoffmann, J.; et al. SARS-CoV-2 Vaccination Rate and SARS-CoV-2 Infection of Health Care Workers in Aerosol-Generating Medical Disciplines. J. Clin. Med. 2022, 11, 2751. https://doi.org/10.3390/jcm11102751
Muzalyova A, Ebigbo A, Kahn M, Zellmer S, Beyer A, Rosendahl J, Zenk J, Al-Nawas B, Frankenberger R, Hoffmann J, et al. SARS-CoV-2 Vaccination Rate and SARS-CoV-2 Infection of Health Care Workers in Aerosol-Generating Medical Disciplines. Journal of Clinical Medicine. 2022; 11(10):2751. https://doi.org/10.3390/jcm11102751
Chicago/Turabian StyleMuzalyova, Anna, Alanna Ebigbo, Maria Kahn, Stephan Zellmer, Albert Beyer, Jonas Rosendahl, Johannes Zenk, Bilal Al-Nawas, Roland Frankenberger, Juergen Hoffmann, and et al. 2022. "SARS-CoV-2 Vaccination Rate and SARS-CoV-2 Infection of Health Care Workers in Aerosol-Generating Medical Disciplines" Journal of Clinical Medicine 11, no. 10: 2751. https://doi.org/10.3390/jcm11102751