
The Association of Cardiometabolic Disease with Psychological Factors in Colombian People during the COVID-19 Pandemic: A Cross-Sectional Study

 , , ,
, , ,  ,
,  , and
, and 
Abstract
:1. Introduction
2. Materials and Methods
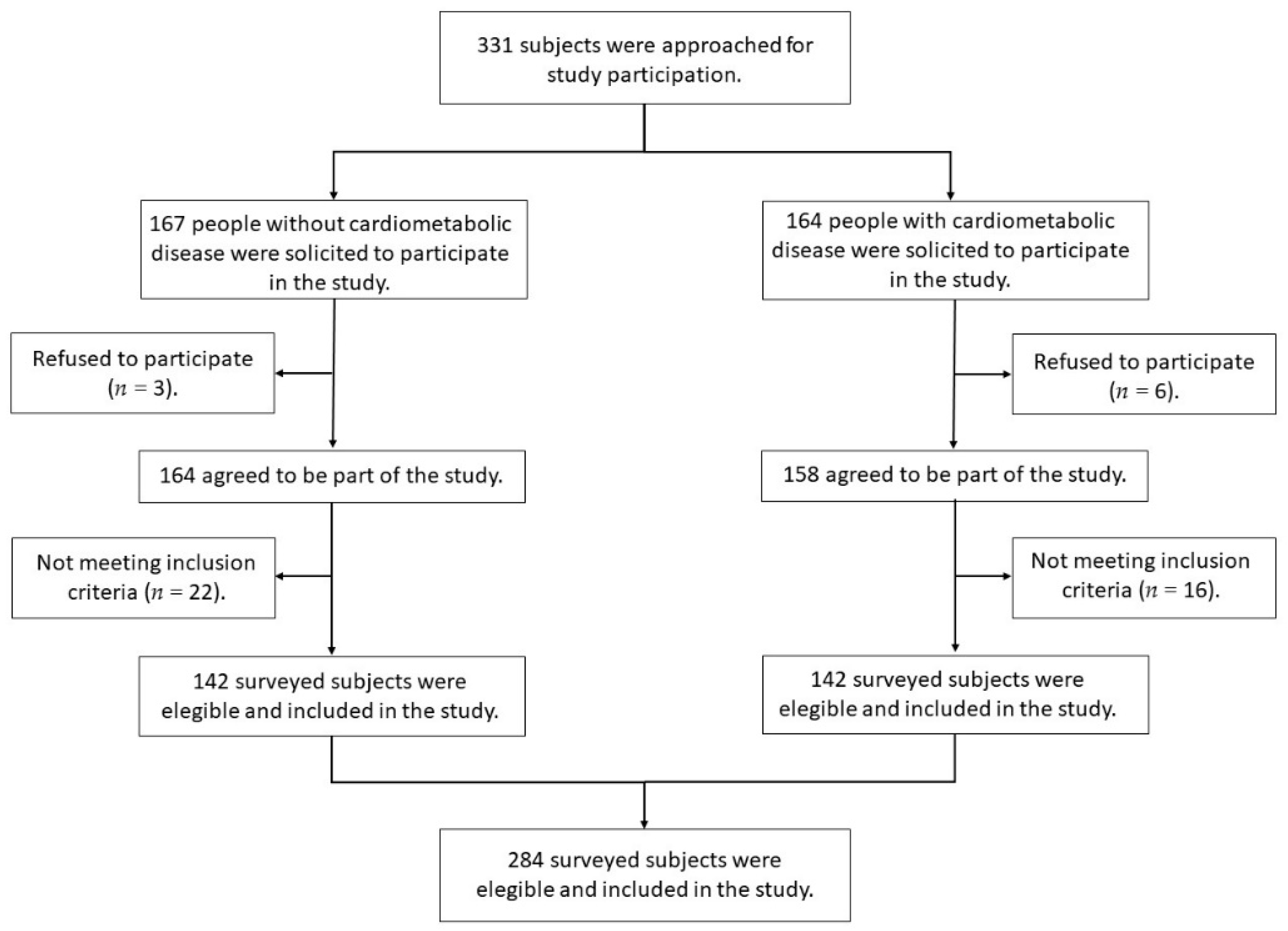
2.1. Study Design and Participants
2.2. Outcome Variables
2.2.1. Quality of Life Related to Health
2.2.2. Sleep Quality
2.2.3. Depression
2.3. Covariates
2.3.1. Sociodemographic and Anthropometric Data
2.3.2. Level of Physical Activity
2.4. Sample Size Calculation
2.5. Data Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- OPS/OMS. Actualización Epidemiológica: Enfermedad por Coronavirus (COVID-19)—19 de Junio, 2021. Available online: https://www.paho.org/es/documentos/actualizacion-epidemiologica-enfermedad-por-coronavirus-covid-19-19-junio-2021 (accessed on 20 June 2021).
- PAHO/WHO. Epidemiological Update: Variants of SARS-CoV-2 in the Americas. 26 January 2021. Available online: https://iris.paho.org/bitstream/handle/10665.2/53239/EpiUpdate26January2021_eng.pdf?sequence=1&isAllowed=y (accessed on 20 June 2021).
- Pinilla-Roncancio, M. The reality of disability: Multidimensional poverty of people with disability and their families in Latin America. Disabil. Health J. 2018, 11, 398–404. [Google Scholar] [CrossRef] [PubMed]
- Holmes, E.A.; O’Connor, R.C.; Perry, V.H.; Tracey, I.; Wessely, S.; Arseneault, L.; Ballard, C.; Christensen, H.; Silver, R.C.; Everall, I.; et al. Multidisciplinary research priorities for the COVID-19 pandemic: A call for action for mental health science. Lancet Psychiatry 2020, 7, 547–560. [Google Scholar] [CrossRef]
- Hossain, M.M.; Tasnim, S.; Sultana, A.; Faizah, F.; Mazumder, H.; Zou, L.; McKyer, E.L.J.; Ahmed, H.U.; Ma, P. Epidemiology of mental health problems in COVID-19: A review. F1000Research 2020, 9, 636. [Google Scholar] [CrossRef]
- Torales, J.; O’Higgins, M.; Castaldelli-Maia, J.M.; Ventriglio, A. The outbreak of COVID-19 coronavirus and its impact on global mental health. Int. J. Soc. Psychiatry 2020, 66, 317–320. [Google Scholar] [CrossRef] [Green Version]
- Grolli, R.E.; Mingoti, M.E.D.; Bertollo, A.G.; Luzardo, A.R.; Quevedo, J.; Réus, G.Z.; Ignácio, Z.M. Impact of COVID-19 in the Mental Health in Elderly: Psychological and Biological Updates. Mol. Neurobiol. 2021, 58, 1905–1916. [Google Scholar] [CrossRef]
- Klimkiewicz, A.; Schmalenberg, A.; Klimkiewicz, J.; Jasińska, A.; Jasionowska, J.; Machura, W.; Wojnar, M. COVID-19 Pandemic Influence on Healthcare Professionals. J. Clin. Med. 2021, 10, 1280. [Google Scholar] [CrossRef]
- Singh, S.; Roy, D.; Sinha, K.; Parveen, S.; Sharma, G.; Joshi, G. Impact of COVID-19 and lockdown on mental health of children and adolescents: A narrative review with recommendations. Psychiatry Res. 2020, 293, 113429. [Google Scholar] [CrossRef]
- Zhou, S.J.; Zhang, L.G.; Wang, L.L.; Guo, Z.C.; Wang, J.Q.; Chen, J.C.; Liu, M.; Chen, X.; Chen, J.X. Prevalence and socio-demographic correlates of psychological health problems in Chinese adolescents during the outbreak of COVID-19. Eur. Child Adolesc. Psychiatry 2020, 29, 749–758. [Google Scholar] [CrossRef]
- Wu, T.; Jia, X.; Shi, H.; Niu, J.; Yin, X.; Xie, J.; Wang, X. Prevalence of mental health problems during the COVID-19 pandemic: A systematic review and meta-analysis. J. Affect. Disord. 2021, 281, 91–98. [Google Scholar] [CrossRef]
- Rangaraj, V.R.; Knutson, K.L. Association between sleep deficiency and cardiometabolic disease: Implications for health disparities. Sleep Med. 2016, 18, 19–35. [Google Scholar] [CrossRef] [Green Version]
- WHO. Noncommunicable Diseases: Progress Monitor 2020; World Health Organization: Geneva, Switzerland, 2020. [Google Scholar]
- Zurique Sánchez, M.S.; Zurique Sánchez, C.P.; Camacho López, P.A.; Sanchez Sanabria, M.; Hernández Hernández, S.C. Prevalencia de hipertensión arterial en Colombia: Revisión sistemática y meta-análisis. Acta Méd. Colomb. 2019, 44. [Google Scholar] [CrossRef]
- Minsalud. Obesidad, un Factor de Riesgo en el COVID-19. Available online: https://www.minsalud.gov.co/Paginas/Obesidad-un-factor-de-riesgo-en-el-covid-19.aspx (accessed on 20 April 2021).
- Gómez, L.F.; Mora, M.; Riascos, S.; Parra, D. Prevalencias de diabetes e hipertensión en Colombia: Un revisión sistemática. Rev. Fac. Nac. De Salud Pública 2019, 37. [Google Scholar] [CrossRef]
- Pascual-Sánchez, A.; Caballo-Escribano, C. Funcionamiento y calidad de vida en personas con enfermedades crónicas: Poder predictivo de distintas variables psicológicas. J. Enfermería Glob. 2017, 16, 281–294. [Google Scholar] [CrossRef] [Green Version]
- Damares-Garcia, G.; Alcalá-Pompeo, D.; Palota-Eid, L.; Bernardi-Cesarino, C.; Pinto, M.H.; Gonçalves, L.W.P. Relationship between anxiety, depressive symptoms and compulsive overeating disorder in patients with cardiovascular diseases. Rev. Lat. Am. De Enferm. 2018, 26, 1–9. [Google Scholar]
- Choi, Y.; Choi, J.W. Association of sleep disturbance with risk of cardiovascular disease and all-cause mortality in patients with new-onset type 2 diabetes: Data from the Korean NHIS-HEALS. Cardiovasc. Diabetol. 2020, 19, 61. [Google Scholar] [CrossRef]
- Cappuccio, F.P.; Miller, M.A. Sleep and Cardio-Metabolic Disease. Curr. Cardiol. Rep. 2017, 19, 110. [Google Scholar] [CrossRef] [Green Version]
- Khaledi, M.; Haghighatdoost, F.; Feizi, A.; Aminorroaya, A. The prevalence of comorbid depression in patients with type 2 diabetes: An updated systematic review and meta-analysis on huge number of observational studies. Acta Diabetol. 2019, 56, 631–650. [Google Scholar] [CrossRef]
- Ho, A.K.; Thorpe, C.T.; Pandhi, N.; Palta, M.; Smith, M.A.; Johnson, H.M. Association of anxiety and depression with hypertension control: A US multidisciplinary group practice observational study. J. Hypertens. 2015, 33, 2215–2222. [Google Scholar] [CrossRef] [Green Version]
- Li, Z.; Li, Y.; Chen, L.; Chen, P.; Hu, Y. Prevalence of Depression in Patients With Hypertension: A Systematic Review and Meta-Analysis. Medicine 2015, 94, e1317. [Google Scholar] [CrossRef]
- Mejia-Lancheros, C.; Estruch, R.; Martínez-González, M.A.; Salas-Salvadó, J.; Corella, D.; Gómez-Gracia, E.; Fiol, M.; Santos, J.M.; Fitó, M.; Arós, F.; et al. Blood pressure values and depression in hypertensive individuals at high cardiovascular risk. BMC Cardiovasc. Disord. 2014, 14, 109. [Google Scholar] [CrossRef] [Green Version]
- Endomba, F.T.; Mazou, T.N.; Bigna, J.J. Epidemiology of depressive disorders in people living with hypertension in Africa: A systematic review and meta-analysis. BMJ Open 2020, 10, e037975. [Google Scholar] [CrossRef]
- Lloyd, C.E.; Roy, T.; Nouwen, A.; Chauhan, A.M. Epidemiology of depression in diabetes: International and cross-cultural issues. J. Affect. Disord. 2012, 142, S22–S29. [Google Scholar] [CrossRef]
- Mukeshimana, M.; McHunu, G. Management of Co-Morbidity of Depression and Chronic Non-Communicable Diseases in Rwanda. Ethiop. J. Health Sci. 2017, 27, 17–26. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wright, J.; Mazumdar, P.; Barua, D.; Lina, S.; Bibi, H.; Kanwal, A.; Mujeeb, F.; Naz, Q.; Safi, R.; Ul Haq, B.; et al. Integrating depression care within NCD provision in Bangladesh and Pakistan: A qualitative study. Int. J. Ment. Health Syst. 2020, 14, 63. [Google Scholar] [CrossRef]
- Eze-Nliam, C.M.; Thombs, B.D.; Lima, B.B.; Smith, C.G.; Ziegelstein, R.C. The association of depression with adherence to antihypertensive medications: A systematic review. J. Hypertens. 2010, 28, 1785–1795. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, P.S.; Bohn, R.L.; Knight, E.; Glynn, R.J.; Mogun, H.; Avorn, J. Noncompliance with antihypertensive medications: The impact of depressive symptoms and psychosocial factors. J. Gen. Intern. Med. 2002, 17, 504–511. [Google Scholar] [CrossRef] [Green Version]
- Bauer, A.M.; Parker, M.M.; Moffet, H.H.; Schillinger, D.; Adler, N.E.; Adams, A.S.; Schmittdiel, J.A.; Katon, W.J.; Karter, A.J. Depressive symptoms and adherence to cardiometabolic therapies across phases of treatment among adults with diabetes: The Diabetes Study of Northern California (DISTANCE). Patient Prefer. Adherence 2017, 11, 643–652. [Google Scholar] [CrossRef] [Green Version]
- WHO. Integrating the Prevention, Treatment and Care of Mental Health Conditions and Other Noncommunicable Diseases within Health Systems. 2019. Available online: https://www.euro.who.int/__data/assets/pdf_file/0004/397786/Mental-Health-Conditions-ENG.pdf (accessed on 22 June 2021).
- Brocato, J.; Wu, F.; Chen, Y.; Shamy, M.; Alghamdi, M.A.; Khoder, M.I.; Alkhatim, A.A.; Abdou, M.H.; Costa, M. Association between sleeping hours and cardiometabolic risk factors for metabolic syndrome in a Saudi Arabian population. BMJ Open 2015, 5, e008590. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, S.W.H.; Ng, K.Y.; Chin, W.K. The impact of sleep amount and sleep quality on glycemic control in type 2 diabetes: A systematic review and meta-analysis. Sleep Med. Rev. 2017, 31, 91–101. [Google Scholar] [CrossRef]
- Rusu, A.; Ciobanu, D.; Bala, C.; Cerghizan, A.; Roman, G. Social jetlag, sleep-related parameters, and glycemic control in adults with type 1 diabetes: Results of a cross-sectional study. J. Diabetes 2019, 11, 394–401. [Google Scholar] [CrossRef] [PubMed]
- Mosavat, M.; Mirsanjari, M.; Arabiat, D.; Smyth, A.; Whitehead, L. The Role of Sleep Curtailment on Leptin Levels in Obesity and Diabetes Mellitus. Obes. Facts 2021, 14, 214–221. [Google Scholar] [CrossRef]
- Sayeed, A.; Kundu, S.; Al Banna, M.H.; Christopher, E.; Hasan, M.T.; Begum, M.R.; Chowdhury, S.; Khan, M.S.I. Mental Health Outcomes of Adults with Comorbidity and Chronic Diseases during the COVID-19 Pandemic: A Matched Case-Control Study. Psychiatr. Danub. 2020, 32, 491–498. [Google Scholar] [CrossRef] [PubMed]
- Medina-Ortiz, O.; Araque-Castellanos, F.; Ruiz-Domínguez, L.C.; Riaño-Garzón, M.; Bermudez, V. Trastornos del sueño a consecuencia de la pandemia por COVID-19. J Rev. Peru. De Med. Exp. Y Salud Publica 2020, 37, 755–761. [Google Scholar] [CrossRef]
- Mandelkorn, U.; Genzer, S.; Choshen-Hillel, S.; Reiter, J.; Meira, E.C.M.; Hochner, H.; Kheirandish-Gozal, L.; Gozal, D.; Gileles-Hillel, A. Escalation of sleep disturbances amid the COVID-19 pandemic: A cross-sectional international study. J. Clin. Sleep Med. JCSM Off. Publ. Am. Acad. Sleep Med. 2021, 17, 45–53. [Google Scholar] [CrossRef]
- Ara, T.; Rahman, M.M.; Hossain, M.A.; Ahmed, A. Identifying the Associated Risk Factors of Sleep Disturbance During the COVID-19 Lockdown in Bangladesh: A Web-Based Survey. Front. Psychiatry 2020, 11, 966. [Google Scholar] [CrossRef] [PubMed]
- Wańkowicz, P.; Szylińska, A.; Rotter, I. The Impact of the COVID-19 Pandemic on Psychological Health and Insomnia among People with Chronic Diseases. J. Clin. Med. 2021, 10, 1206. [Google Scholar] [CrossRef] [PubMed]
- Ramírez-Vélez, R.; Agredo-Zuñiga, R.A.; Jerez-Valderrama, A.M. The reliability of preliminary normative values from the short form health survey (SF-12) questionnaire regarding Colombian adults. Rev. De Salud Publica 2010, 12, 807–819. [Google Scholar]
- Buysse, D.J.; Reynolds, C.F., 3rd; Monk, T.H.; Berman, S.R.; Kupfer, D.J. The Pittsburgh Sleep Quality Index: A new instrument for psychiatric practice and research. Psychiatry Res. 1989, 28, 193–213. [Google Scholar] [CrossRef]
- Escobar-Córdoba, F.; Eslava-Schmalbach, J. Colombian validation of the Pittsburgh Sleep Quality Index. Rev. De Neurol. 2005, 40, 150–155. [Google Scholar]
- Doi, Y.; Minowa, M.; Uchiyama, M.; Okawa, M.; Kim, K.; Shibui, K.; Kamei, Y. Psychometric assessment of subjective sleep quality using the Japanese version of the Pittsburgh Sleep Quality Index (PSQI-J) in psychiatric disordered and control subjects. Psychiatry Res. 2000, 97, 165–172. [Google Scholar] [CrossRef]
- Çalışkan, F.; Toker, İ.; Tur, B.; Hacar, S.; Türe, B. Assessment of the Pittsburgh Sleep Quality Index among Physician’s Speciality Who Work Night Shifts. Emerg. Med. Open J. 2015, 1, 5–11. [Google Scholar] [CrossRef]
- Zung, W.W. A self-rating depression scale. Arch. Gen. Psychiatry 1965, 12, 63–70. [Google Scholar] [CrossRef] [PubMed]
- Campo-Arias, A.; Diaz Martinez, L.; Rueda-Jaimes, G.; Barros, J. Validación de la escala de Zung para depresión en universitarias de Bucaramanga, Colombia. Rev. Colomb. Psiquiatr. 2005, 34, 54–62. [Google Scholar]
- Colombia, G.d. Ley 142 de 1994. Available online: https://www.funcionpublica.gov.co/eva/gestornormativo/norma.php?i=2752 (accessed on 25 February 2021).
- WHO. 10 Datos Sobre La Obesidad. Available online: https://www.who.int/features/factfiles/obesity/facts/es/ (accessed on 20 July 2021).
- Craig, C.L.; Marshall, A.L.; Sjöström, M.; Bauman, A.E.; Booth, M.L.; Ainsworth, B.E.; Pratt, M.; Ekelund, U.; Yngve, A.; Sallis, J.F.; et al. International physical activity questionnaire: 12-country reliability and validity. Med. Sci. Sports Exerc. 2003, 35, 1381–1395. [Google Scholar] [CrossRef] [Green Version]
- Fan, M.; Lyu, J.; He, P. Guidelines for data processing and analysis of the International Physical Activity Questionnaire (IPAQ). 2005. Zhonghua Liu Xing Bing Xue Za Zhi Zhonghua Liuxingbingxue Zazhi 2014, 35, 961–964. [Google Scholar]
- Calvo, M.O.; Domínguez, A.C. Regresión logística no condicionada y tamaño de muestra: Una revisión bibliográfica. Rev. Esp. Salud Publica 2002, 76, 85–93. [Google Scholar] [CrossRef] [Green Version]
- Zhang, Y.; Chen, Y.; Ma, L. Depression and cardiovascular disease in elderly: Current understanding. J. Clin. Neurosci. Off. J. Neurosurg. Soc. Australas. 2018, 47, 1–5. [Google Scholar] [CrossRef] [PubMed]
- Shinn, E.H.; Poston, W.S.; Kimball, K.T.; St Jeor, S.T.; Foreyt, J.P. Blood pressure and symptoms of depression and anxiety: A prospective study. Am. J. Hypertens. 2001, 14, 660–664. [Google Scholar] [CrossRef] [Green Version]
- Tian, W.; Jiang, W.; Yao, J.; Nicholson, C.J.; Li, R.H.; Sigurslid, H.H.; Wooster, L.; Rotter, J.I.; Guo, X.; Malhotra, R. Predictors of mortality in hospitalized COVID-19 patients: A systematic review and meta-analysis. J. Med. Virol. 2020, 92, 1875–1883. [Google Scholar] [CrossRef]
- Rajkumar, R.P. COVID-19 and mental health: A review of the existing literature. Asian J. Psychiatry 2020, 52, 102066. [Google Scholar] [CrossRef]
- Bish, A.; Michie, S. Demographic and attitudinal determinants of protective behaviours during a pandemic: A review. Br. J. Health Psychol. 2010, 15, 797–824. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, S.; Feng, B.; Liao, W.; Pan, W. Internet Use, Risk Awareness, and Demographic Characteristics Associated With Engagement in Preventive Behaviors and Testing: Cross-Sectional Survey on COVID-19 in the United States. J. Med. Internet Res. 2020, 22, e19782. [Google Scholar] [CrossRef] [PubMed]
- González-Castro, J.L.; Ubillos-Landa, S.; Puente-Martínez, A.; Gracia-Leiva, M. Perceived Vulnerability and Severity Predict Adherence to COVID-19 Protection Measures: The Mediating Role of Instrumental Coping. Front. Psychol. 2021, 12, 674032. [Google Scholar] [CrossRef]
- Dwyer, M.J.; Pasini, M.; De Dominicis, S.; Righi, E. Physical activity: Benefits and challenges during the COVID-19 pandemic. Scand. J. Med. Sci. Sports 2020, 30, 1291–1294. [Google Scholar] [CrossRef]
- Swift, D.L.; McGee, J.E.; Earnest, C.P.; Carlisle, E.; Nygard, M.; Johannsen, N.M. The Effects of Exercise and Physical Activity on Weight Loss and Maintenance. Prog. Cardiovasc. Dis. 2018, 61, 206–213. [Google Scholar] [CrossRef]
- Sallis, R.; Young, D.R.; Tartof, S.Y.; Sallis, J.F.; Sall, J.; Li, Q.; Smith, G.N.; Cohen, D.A. Physical inactivity is associated with a higher risk for severe COVID-19 outcomes: A study in 48 440 adult patients. Br. J. Sports Med. 2021, 55, 1099–1105. [Google Scholar] [CrossRef]
- Kriaucioniene, V.; Petkeviciene, J.; Raskiliene, A. Nutrition and physical activity counselling by general practitioners in Lithuania, 2000–2014. BMC Fam. Pract. 2019, 20, 125. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sarris, J.; O’Neil, A.; Coulson, C.E.; Schweitzer, I.; Berk, M. Lifestyle medicine for depression. BMC Psychiatry 2014, 14, 107. [Google Scholar] [CrossRef] [Green Version]
- Carney, R.M.; Freedland, K.E.; Veith, R.C. Depression, the autonomic nervous system, and coronary heart disease. Psychosom. Med. 2005, 67 (Suppl. 1), S29–S33. [Google Scholar] [CrossRef] [PubMed]
- Dolynna, O.V. Autonomic nervous system unbalance in patients with ischemic heart disease and depression. Likars’ka Sprav. 2013, 5, 27–31. [Google Scholar]
- Semenkovich, K.; Brown, M.E.; Svrakic, D.M.; Lustman, P.J. Depression in type 2 diabetes mellitus: Prevalence, impact, and treatment. Drugs 2015, 75, 577–587. [Google Scholar] [CrossRef]
- Faulconbridge, L.F.; Driscoll, C.F.B.; Hopkins, C.M.; Bailer Benforado, B.; Bishop-Gilyard, C.; Carvajal, R.; Berkowitz, R.I.; DeRubeis, R.; Wadden, T.A. Combined Treatment for Obesity and Depression: A Pilot Study. Obesty 2018, 26, 1144–1152. [Google Scholar] [CrossRef] [PubMed]
- Lazarevich, I.; Irigoyen Camacho, M.E.; Velázquez-Alva, M.C.; Flores, N.L.; Nájera Medina, O.; Zepeda Zepeda, M.A. Depression and food consumption in Mexican college students. Nutr. Hosp. 2018, 35, 620–626. [Google Scholar] [CrossRef]
- Oliffe, J.L.; Rossnagel, E.; Seidler, Z.E.; Kealy, D.; Ogrodniczuk, J.S.; Rice, S.M. Men’s Depression and Suicide. Curr. Psychiatry Rep. 2019, 21, 103. [Google Scholar] [CrossRef] [PubMed]
- Knowlden, A.P.; Higginbotham, J.C.; Grandner, M.A.; Allegrante, J.P. Modeling Risk Factors for Sleep- and Adiposity-Related Cardiometabolic Disease: Protocol for the Short Sleep Undermines Cardiometabolic Health (SLUMBRx) Observational Study. JMIR Res. Protoc. 2021, 10, e27139. [Google Scholar] [CrossRef] [PubMed]
- Meurling, I.J.; Shea, D.O.; Garvey, J.F. Obesity and sleep: A growing concern. Curr. Opin. Pulm. Med. 2019, 25, 602–608. [Google Scholar] [CrossRef]
- Raphael, K. Recall Bias: A Proposal for Assessment and Control. Int. J. Epidemiol. 1987, 16, 167–170. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
| Without CD (n = 142) | With CD (n = 142) | p | ||||
|---|---|---|---|---|---|---|
| Age. mean (SD) | 41.53 (10.06) | 48.15 (10.15) | 1.000 | |||
| Sex. n (%) | Male | 74 (52.11) | 84 (59.15) | 0.232 | ||
| Female | 68 (47.89) | 58 (40.85) | ||||
| * BMI. n (%) | Underweight | 1 (0.07) | 1 (0.07) | 0.000 | ||
| Normal range | 84 (59.15) | 15 (10.56) | ||||
| Overweight | 1 (0.07) | 8 (5.63) | ||||
| Preobese | 56 (39.43) | 59 (41.54) | ||||
| Obese class 1 | 0 (0) | 43 (30.28) | ||||
| Obese class 2 | 0 (0) | 14 (9.85) | ||||
| Obese class 3 | 0 (0) | 2 (1.40) | ||||
| Marital status. n (%) | Single/Free union | 84 (59.16) | 64 (45.97) | 0.113 | ||
| Married | 46 (32.39) | 66 (46.48) | ||||
| Separated/widower | 12 (8.45) | 12 (8.45) | ||||
| Residence. n (%) | Rural area | 18 (12.68) | 19 (13.38) | |||
| Urban area | 124 (87.32) | 123 (86.62) | ||||
| ** Socioeco-nomic strata n (%) | Low | 6 (4.23) | 15 (9.15) | 0.069 | ||
| Medium | 76 (53.52) | 77 (54.22) | ||||
| High | 60 (42.25) | 50 (35.21) | ||||
| Smoker. n (%) | No | 138 (97.18) | 141 (99.30) | 0.175 | ||
| Yes | 4 (2.82) | 1 (0.70) | ||||
| Alcohol. n (%) | Not consumption | 60 (42.25) | 67 (47.18) | 0.501 | ||
| Yes consumption | 82 (57.74) | 75 (52.82) | ||||
| Frequency | Occasional | 77 (54.23) | 69 (48.59) | |||
| Frequently | 5 (3.51) | 6 (4.23) | ||||
| Living with people at risk of COVID-19. n (%) | No | 97 (68.31) | 96 (67.61) | 0.898 | ||
| Yes | 45 (31.69) | 46 (32.39) | ||||
| Presence of COVID-19 symptoms. n (%) | No | 142 (100.00) | 141 (99.30) | 0.316 | ||
| Yes | 0 (0.00) | 1 (0.70) | ||||
| IPAQ. n (%) | Active | 68 (47.89) | 92 (64.79) | 0.004 | ||
| Insufficiently active | 74 (52.11) | 50 (35.21) | ||||
| Without CD (n = 142) | With CD (n = 142) | p | |||
|---|---|---|---|---|---|
| SF-12v2. mean (SD) | Physical Health dimension | Physical functioning | 94.36 (13.44) | 82.21 (26.39) | 0.000 |
| Physical role | 87.32 (31.19) | 84.50 (33.25) | 0.462 | ||
| Bodily pain | 91.90 (15.62) | 87.85 (17.79) | 0.042 | ||
| General health | 81.52 (14.65) | 63.55 (21.61) | 0.000 | ||
| PCS | 88.77 (13.40) | 79.53 (16.82) | 0.000 | ||
| Mental Health dimension | Vitality | 77.04 (19.19) | 76.05 (21.20) | 0.681 | |
| Social functioning | 89.08 (17.47) | 86.26 (22.98) | 0.246 | ||
| Emotional role | 90.14 (28.08) | 84.85 (31.50) | 0.137 | ||
| Mental health | 77.60 (17.86) | 75.84 (20.42) | 0.440 | ||
| MCS | 83.46 (15.21) | 80.75 (18.23) | 0.174 | ||
| Total score for SF-12v2 | 86.53 (12.88) | 81.03 (16.56) | 0.002 | ||
| SF-12v2. n (%) | Quality of life BA | 3 (2.11) | 9 (6.34) | 0.076 | |
| Quality of life AA | 139 (97.89) | 133 (93.66) | 0.076 | ||
| PSQI. mean (SD) | Sleep quality domain | 0.58 (0.66) | 1.09 (0.68) | 0.000 | |
| Sleep latency domain | 0.52 (0.69) | 1.38 (0.85) | 0.000 | ||
| Sleep duration domain | 0.76 (0.69) | 1.50 (0.81) | 0.000 | ||
| Sleep efficiency domain | 0.48 (0.81) | 0.58 (0.70) | 0.276 | ||
| Sleep disturbances domain | 0.66 (0.63) | 1.17 (0.67) | 0.000 | ||
| Use of sleeping medication domain | 0.35 (0.66) | 0.56 (0.64) | 0.009 | ||
| Daytime dysfunction domain | 0.30 (0.47) | 0.73 (0.73) | 0.000 | ||
| Total score for PSQI | 3.69 (3.41) | 7.00 (3.34) | 0.000 | ||
| PSQI. n (%) | Without LSQ | 97 (68.31) | 54 (38.03) | 0.000 | |
| With LSQ | 45 (31.69) | 88 (61.97) | 0.000 | ||
| ZSDS. n (%) | Without DS | 89 (62.68) | 65 (45.77) | 0.000 | |
| With DS | 53 (37.32) | 77 (54.23) | 0.000 | ||
| OR | p > |z| | [95% CI] Min–Max | |
|---|---|---|---|
| BA-SF-12v2 | 0.32 | 0.09 | 0.08–1.20 |
| LSQ-PSQI | 3.51 | 0.00 | 2.15–5.73 |
| DS-ZSDS | 1.98 | 0.00 | 1.24–3.19 |
| Without CD | With CD | ||||||
|---|---|---|---|---|---|---|---|
| OR | [95% CI] | p > |z| | OR | [95% CI] | p > |z| | ||
| min–max | min–max | ||||||
| DS-ZSDS | Sex (male) | 3.21 | 1.45–7.12 | 0.004 | — | — | — |
| Living with people at risk of COVID-19 (Yes) | 4.86 | 2.14–11.03 | 0.000 | — | — | — | |
| * BMI | — | — | — | 2.45 | 1.66–3.60 | 0.000 | |
| Cons | 0.18 | 0.09–0.37 | 0.000 | 0.02 | 0.01–0.12 | 0.000 | |
| LSQ-PSQI | Living with people at risk of COVID-19 (yes) | 4.22 | 2.58–6.91 | 0.000 | 3.64 | 1.17–11.28 | 0.025 |
| * BMI | — | — | — | 5.88 | 1.15–2.74 | 0.000 | |
| Cons | 0.01 | 0.00–0.07 | 0.000 | 0.00 | 0.00–0.01 | 0.000 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
García-Garro, P.A.; Aibar-Almazán, A.; Rivas-Campo, Y.; Vega-Ávila, G.C.; Afanador-Restrepo, D.F.; Martínez-Amat, A.; Afanador-Rodríguez, M.I.; Castellote-Caballero, Y.; Hita-Contreras, F. The Association of Cardiometabolic Disease with Psychological Factors in Colombian People during the COVID-19 Pandemic: A Cross-Sectional Study. J. Clin. Med. 2021, 10, 4959. https://doi.org/10.3390/jcm10214959
García-Garro PA, Aibar-Almazán A, Rivas-Campo Y, Vega-Ávila GC, Afanador-Restrepo DF, Martínez-Amat A, Afanador-Rodríguez MI, Castellote-Caballero Y, Hita-Contreras F. The Association of Cardiometabolic Disease with Psychological Factors in Colombian People during the COVID-19 Pandemic: A Cross-Sectional Study. Journal of Clinical Medicine. 2021; 10(21):4959. https://doi.org/10.3390/jcm10214959
Chicago/Turabian StyleGarcía-Garro, Patricia Alexandra, Agustín Aibar-Almazán, Yulieth Rivas-Campo, Gloria Cecilia Vega-Ávila, Diego Fernando Afanador-Restrepo, Antonio Martínez-Amat, María Isabel Afanador-Rodríguez, Yolanda Castellote-Caballero, and Fidel Hita-Contreras. 2021. "The Association of Cardiometabolic Disease with Psychological Factors in Colombian People during the COVID-19 Pandemic: A Cross-Sectional Study" Journal of Clinical Medicine 10, no. 21: 4959. https://doi.org/10.3390/jcm10214959