1. Introduction
Diabetic macular edema (DME) is the main ocular disease that impairs central vision in patients with diabetic retinopathy [
1]. DME is caused by increased permeability of retinal capillaries, microaneurysms, and disruption of the blood–retinal barrier [
2]. Prolonged hyperglycemia leads to chronic retinal microvascular damage and hypoxia, and increases intraocular levels of vascular endothelial growth factor (VEGF) [
2,
3]. At present, intravitreal injection of anti-VEGF agents is the first-line treatment for DME [
4]. Many large-scale clinical studies have demonstrated that this therapy has a promising effect in normalizing retinal thickness and improving visual acuity [
5,
6]. Anti-VEGF treatment regimens include monthly and bi-monthly dosing, as well as the pro re nata (PRN) regimen, in which injections of anti-VEGF agents are administered in response to the recurrence of the edema, and the treat and extend (TAE) regimen, in which the injection interval is coordinated in accordance with the retinal thickness and visual acuity [
7].
A study using an animal model showed that, after a single injection of anti-VEGF agent, the concentration of the agent in the vitreous decreased over time [
8,
9]. Indeed, frequent injections of anti-VEGF agents are required to maintain the therapeutic effect. Matsunaga et al. showed that anti-VEGF-treated patients who were lost to follow-up for a prolonged period experienced a modest decline in visual acuity, which recovered after restarting injections [
10]. In addition, we recently reported that better visual improvement cannot be achieved without prompt injection once edema recurrence has been identified [
11]. Therefore, it is clinically important to monitor the status of DME through regular visits to ophthalmologists, and to administer anti-VEGF agents at the appropriate time.
Coronavirus disease 2019 (COVID-19) was first reported in China in December 2019 and was detected in Japan in January 2020. The number of COVID-19 patients increased dramatically, peaked, and then decreased, repeatedly. To date (July 2022), six such waves have been observed in Japan [
12]. The outbreak of the COVID-19 pandemic has had a major impact on human activities, including medical care. Outpatient and surgical volumes decreased during the height of the pandemic, and treatment was restricted to urgent or emergency conditions [
13,
14]. The progression of COVID-19 can lead to acute respiratory distress syndrome and even death, and its common symptoms are fever, cough, and fatigue [
15]. In ophthalmology practice, the distance between the ophthalmologist and patient is small. Although Ophthalmology Departments often receive patients without symptoms of infection, it is fundamental to follow the rules of infection control to prevent nosocomial infections [
16]. Ophthalmologists are thus instructed to wear gloves and masks and attach a shield to the slit-lamp microscope [
16]. While it may not have affected the number of injections of anti-VEGF agents, the pandemic also affected the way of practice in ophthalmology clinic.
In this multicenter study in Japan, we conducted a questionnaire-based survey to determine how ophthalmologists responded to the COVID-19 pandemic. In addition, we investigated the relationship between the number of COVID-19 positive patients and the number of anti-VEGF injections in patients with DME.
2. Methods
This multicenter, retrospective, observational study was conducted at 23 institutions in Japan. This study was approved by the University of Fukui Institutional Review Board (IRB No. 20210144) and the ethics committees of the other participating facilities: Mie University, Shinshu University, Tokushima University, Sapporo Municipal Hospital, Kobe University, Tsukuba University, National Defense Medical College, Nara Medical University, Tohoku University, St. Marianna Medical University, Kagoshima University, Tsukazaki Hospital, Hokkaido University, Kagawa University, Gunma University, Kurume University, Nagoya City University, Tokyo Medical University, Hachioji Medical Center, Osaka Medical and Pharmaceutical University, Kyorin University, Shiga Medical University, and Yamaguchi University. The study complied with the principles of the Declaration of Helsinki for all research procedures. It was registered in the UMIN Registry (Number 000048935). No personal identifiable information was collected or stored, and thus informed consent was waived. For COVID-19 positive patients, inclusion of visual acuity or central retinal thickness in the data was not permitted.
We tabulated the number of intravitreal injections of aflibercept and ranibizumab for DME administered by month from the records of the 23 institutions, from January 1, 2019 to February 28, 2022. We also tallied the number of new COVID-19 infections by month for the period from February 1, 2020, to February 28, 2022, based on the number of cases released by each prefecture where the participating institutions are located. The period from the first to the sixth waves was defined based on the number of new COVID-19-positive patients released by the Japanese Ministry of Health, Labor, and Welfare. The number of intravitreal injections of anti-VEGF drugs administered in patients diagnosed with DME per month was measured over the same period.
Intravitreal injections were performed in a standard manner by a trained ophthalmologist using 0.4% oxybuprocaine hydrochloride (0.4% Benoxil ophthalmic solution, Santen Co. Ltd., Osaka, Japan) and 2% xylocaine as anesthetic and povidone iodine for sterilization. The injection volumes of ranibizumab (Lucentis; Novartis Pharma K.K., Tokyo, Japan) and aflibercept (Eylea; Bayer Yakuhin Ltd., Tokyo, Japan) was 0.5 mg/0.05 mL and 2 mg/0.05 mL, respectively.
Additionally, a questionnaire survey with four items was administered to the chief of the ophthalmologists’ group treating DME at each facility. These items were as follows: (1) Do you feel that the number of anti-VEGF injections and number of outpatient visits have changed as compared to pre-pandemic levels? (2) For what period of time before and after COVID-19 vaccination were intravitreal injections not administered? (3) Did you extend the interval between patients’ visits to the ophthalmologist due to the COVID-19 pandemic? (4) Did you change the anti-VEGF treatment regimen for DME? We also asked if the ophthalmologists used masks, gloves, and slit-lamp microscope shields during outpatient consultation since the start of the pandemic. The questionnaire survey was conducted in March 2022.
JMP 10.0.2 (SAS Institute Japan Ltd., Tokyo, Japan) was used for statistical analysis. A paired t-test was used to compare between the different time points. All data are expressed as mean ± SE. The level of statistical significance was set at p < 0.05.
3. Results
3.1. Temporal Profiles of the Number of the COVID-19 Positive Patients and Injections
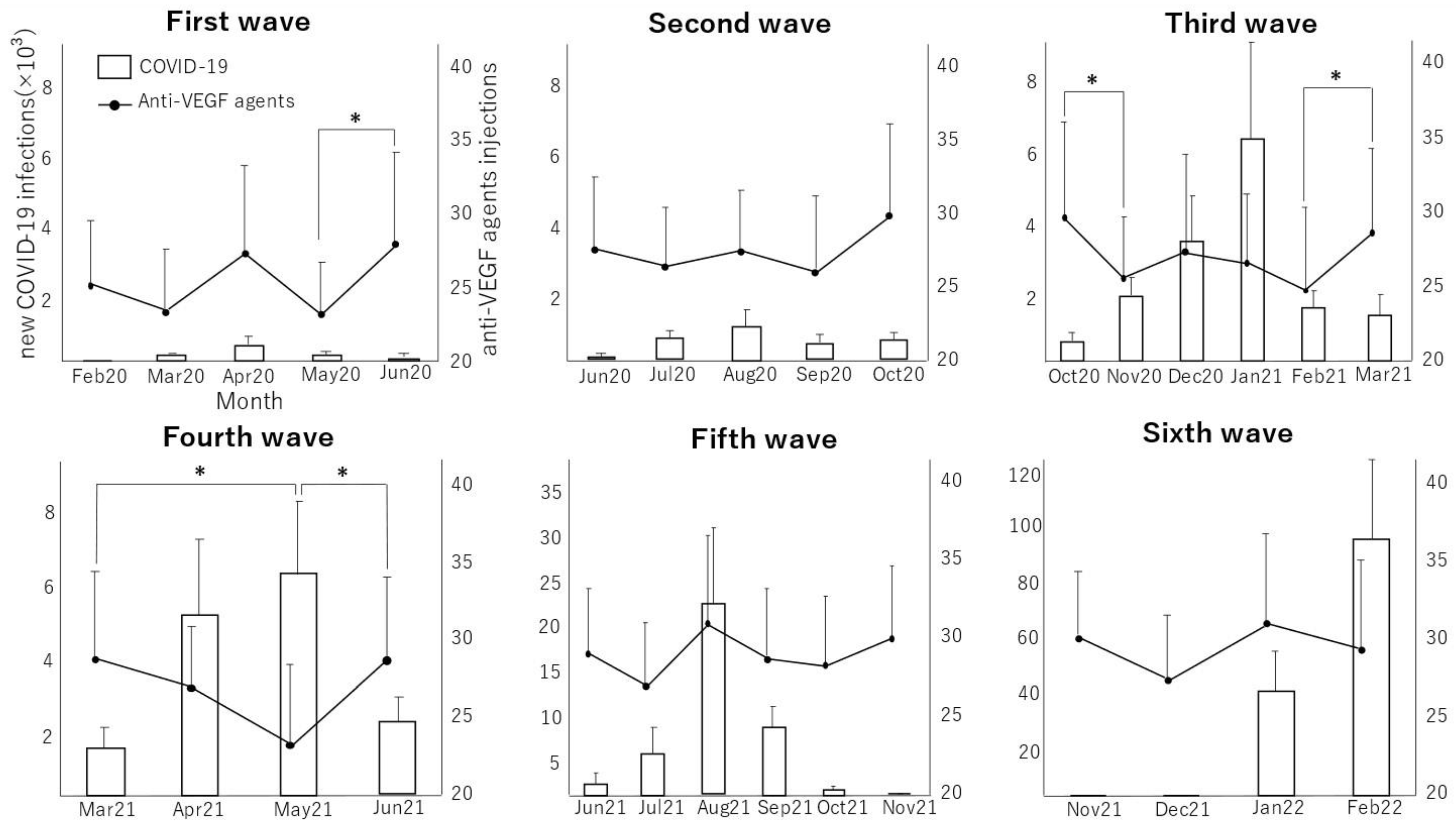
The average monthly numbers of new COVID-19-positive patients and of intravitreal injections of anti-VEGF drugs in DME patients are shown in
Figure 1. During the observational period, six waves of COVID-19 occurred, as shown by the temporal profiles of the number of newly diagnosed COVID-19-positive patients. In the first month of the third wave of the pandemic, when the number of COVID-19 positive patients began to increase (October 2020 to November 2020), the number of anti-VEGF drug injections decreased significantly (
p = 0.0218). During the increasing phase of the fourth wave (March 2021 to May 2021), the number of anti-VEGF injections again decreased significantly (
p = 0.0014). In contrast, the number of injections increased significantly during the last month of the convergence of waves 1 (
p = 0.0195), 3 (
p = 0.0345), and 4 (
p = 0.0023). No significant monthly change in the number of injections administered was observed during waves 2, 5, and 6. No significant differences in the monthly average number of injections of anti-VEGF drugs was found among first to sixth waves (
p > 0.05, comparison of all pairs using Turkey–Kramer’s HSD test, wave 1: 25.39 ± 5.08, wave 2: 27.66 ± 5.01, wave 3: 27.26 ± 5.29, wave 4: 27.08 ± 4.96, wave 5: 28.79 ± 5.07, wave 6: 29.24 ± 5.12). The annual number of injections in 2019, before the pandemic, was 315.63 ± 58.85, while those in 2020 and 2021 were 316.84 ± 59.97 and 330.95 ± 58.37, respectively. The monthly number of injections in 2019, before the pandemic, was 26.30 ± 4.90, while those in 2020 and 2021 were 26.40 ± 5.00 and 27.58 ± 4.86, respectively. No significant differences were observed between the annual numbers of injections (
p > 0.05, comparison of all pairs using Turkey–Kramer’s HSD test). In this study, none of the patients who received anti-VEGF therapy died from COVID-19.
3.2. Questionnaire
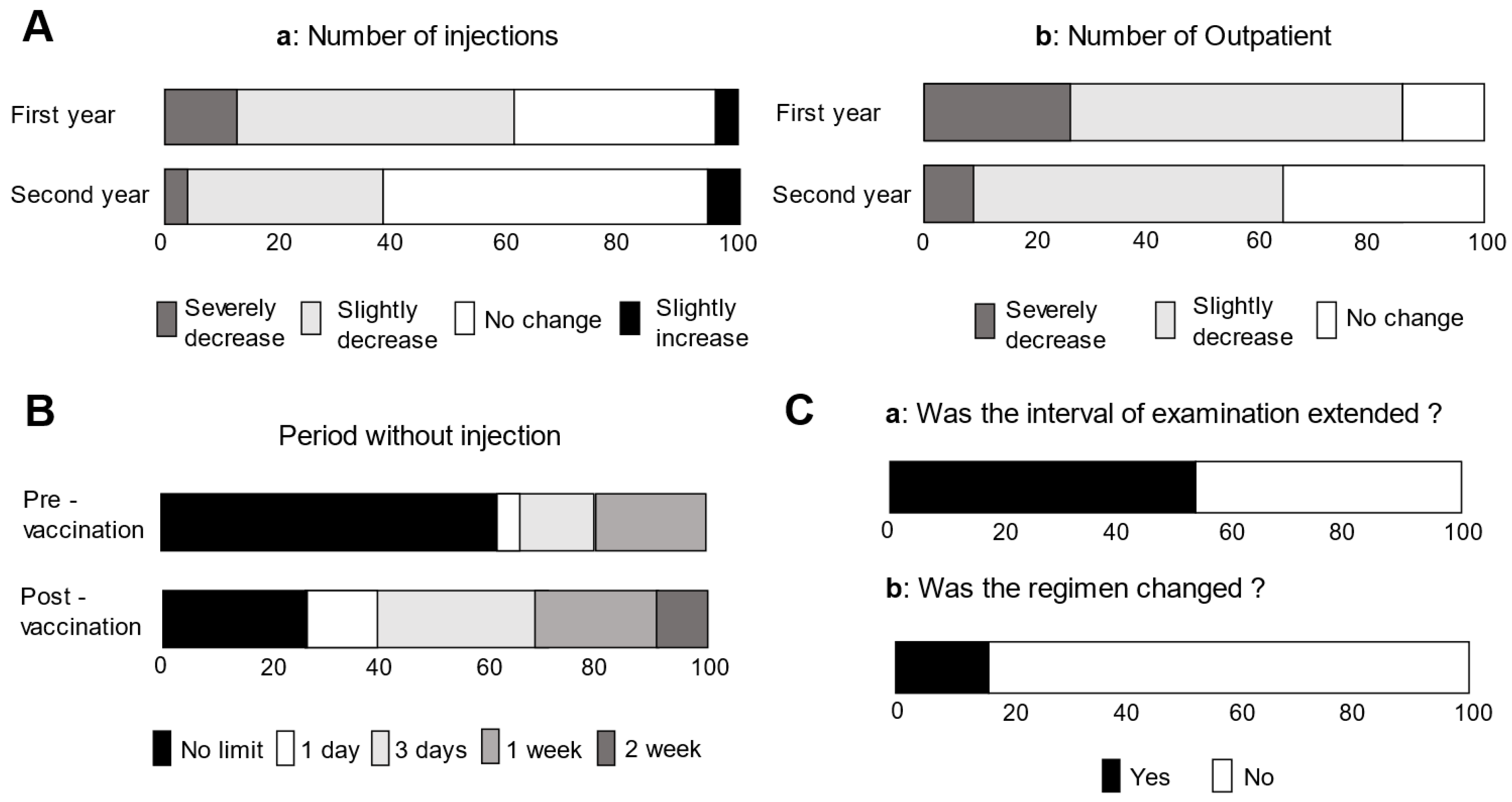
The survey responses obtained from the 23 facilities are shown in
Figure 2. Compared to the period before the COVID-19 pandemic occurred, 60.9% and 87.0% of facilities considered the number of injections
Figure 2A(a) and outpatients
Figure 2A(b) decreased in the first year of the pandemic (1 February 2020 through 31 January 2021: corresponding to waves 1–3). Fewer facilities felt that the number of injections (39.1%) and patients (65.2%) had decreased in the second year (1 February 2021 through 27 February 2022: corresponding to waves 4–6) than did in the first year.
When asked how long to avoid injecting anti-VEGF drugs before vaccination, 4.3%, 13.0%, and 21.7% responded 1 day, 3 days, and 1 week, respectively (
Figure 2B). The percentages of facilities that responded that the period of time during which injections were not administered after vaccination was 1 day, 3 days, 1 week, and 2 weeks were 13.0%, 30.4%, 21.7%, and 8.7%, respectively. Prior to the pandemic, the anti-VEGF treatment regimen at all facilities was PRN. Twelve facilities (52.2%) reported that they extended the interval between visits of the DME patients to the clinic
Figure 2C(a). Four facilities (17.4%) changed the mode of treatment from PRN to TAE during the pandemic
Figure 2C(b).
To prevent infection during outpatient consultations, ophthalmologists at all facilities wore masks and attached shields to the slit-lamp microscopes. Of the facilities, 30.4% additionally fitted staff with face guards. In 22 facilities (95.7%), the ophthalmologists used alcohol disinfection of hands, and at 14 facilities (60.9%) they used plastic gloves.
4. Discussion
Intravitreal injection of anti-VEGF agents is currently the first-line treatment for DME [
4,
17]. According to a survey of Japanese retinal specialists, the most common anti-VEGF treatment regimen is PRN, which involves injection at each recurrence [
7,
18]. However, delayed injection timing for DME recurrence has been reported to worsen visual prognosis [
11]. Moreover, an increase in drop-offs and interruptions in ophthalmology visits are associated with worse visual prognosis [
19]. Therefore, monitoring DME by regular visits is essential for maintaining a favorable visual improvement effect with anti-VEGF therapy. In this study, we investigated the influence of the COVID-19 pandemic on the number of anti-VEGF injections administered for DME. The COVID-19 pandemic has had a major impact on ophthalmic care in Japan. The COVID-19 pandemic has been reported to have reduced the rate of hospital visits greatly [
16], possibly because both patients and healthcare workers were concerned about infection. Additionally, ophthalmology guidance was issued to prioritize urgent surgeries [
16]. The results of the survey conducted in the present study showed that, during the year since the pandemic began, 87.0% of the participating facilities responded that the number of outpatients had decreased, and that 52.2% of facilities had extended the interval between clinic visits after the start of the pandemic. It is possible that social restrictions and inadequate number of visits on clinic may be contributing to poor glycemic control in the patients with diabetes.
In Japan, there have been at least six waves of COVID-19, based on the numbers of positive-testing patients during the observation period since its first identification in January 2020 until February 2022. Our analysis showed that, during the third and fourth waves of the pandemic, an increase in the number of patients and a decrease in the number of anti-VEGF drug injections occurred simultaneously. There are two possible reasons for the confinement of this inverse correlation between the number of patients and the number of injections to the third and fourth waves. In the first and second waves of the pandemic, the spread of infection was limited to urban areas. In the third and fourth waves, the number of COVID-19-positive patients increased nationwide, which may have caused patients to refrain from visiting their ophthalmologists, as reflected in the decrease in the number of injections. The second reason is the reassurance provided by the widespread use of vaccination. The widespread use of vaccination, considered an effective medical treatment against COVID-19, began with older individuals and healthcare workers during the third and fourth waves of the pandemic [
20]. Hence, in the fifth wave, the number of anti-VEGF agent injections was probably less affected by the number of infected patients, because of a sense of relief that the number of infected patients had decreased due to the widespread use of vaccines. Behavioral restrictions implemented to prevent infection, such as the use of masks and face guards and maintaining a safe distance from others, were also established during this period. In addition to the lack of established knowledge about COVID-19 and mechanisms to prevent infection, lockdown of the city and reduced income due to reduced economic activity also increased people’s anxiety. The inverse correlation between the increase in the number of COVID-19-positive patients and anti-VEGF treatment may therefore reflect a variety of physical, emotional, and economic anxieties regarding COVID-19.
During the third and fourth waves, the number of injections decreased as the number of COVID-19 positive patients increased; however, the average number of injections during these periods was not significantly different from that in the first, second, fifth, and sixth waves. One possible reason for this is that the number of injections increased significantly with the decrease in the number of positive patients in each of the 1-month periods at the end of waves 1, 3, and 4. It can be assumed that the number of patients who received injections had increased due to the sense of relief resulting from a lightening of the pandemic. In other words, during the convergence period, many injections were administered to compensate for patients who refrained from visiting the ophthalmologists during the pandemic. Since the 6th wave did not subside at the endpoint of this study, it is unclear in the relationship between the number of the injections and the COVID-19 positive patients in the convergence period of the 6th wave and thereafter. Although the monthly number of injections did not differ significantly among the pandemic waves, many ophthalmologists (60.9%) indicated in the questionnaire that they felt that the number of injections had decreased since the start of the pandemic. This discrepancy may be because of the strong impression left by the decreased number of injections during the third and fourth waves. The first and second years after the start of the pandemic corresponded to waves 1–3 and waves 4–6, respectively. The survey results indicated that fewer facilities felt that there was a pandemic-induced decrease in injections and outpatient visits in the second year than in the first year. In the second year, the number of infected patients increased markedly as compared to that in the first year, but the risk of serious illness decreased due to the mutation of the virus and the widespread use of vaccines. The anxiety of both patients and ophthalmologists seems to have reduced and medical activity appears to have returned to pre-pandemic levels.
In the early days of the COVID-19 pandemic, information on the effectiveness and side effects of vaccines against COVID-19 is scarce. The effect of the vaccines on intravitreal anti-VEGF injections is not well-understood. Thus, this survey found that the timing of injections in relation to vaccine administration varied across facilities. Of the facilities, 73.8% reported that they did not administer anti-VEGF injections immediately after vaccination. Injections for DME were considered less urgent than were treatment for other ocular diseases, such as retinal detachment and endophthalmitis, and therefore were easier to postpone. In fact, 52.2% of the facilities surveyed indicated that they had extended the interval between visits for injections. Nevertheless, the actual number of injections per year did not show a significant decrease as compared with the pre-pandemic levels. One possible reason is that the number of injections did not decrease because of the larger number of injections administered at the end of COVID-19 waves, even though the interval between visits had increased. Alternatively, the change from the PRN to the TAE regimen might reduce the number of clinic visits because of the planned injections. However, Japanese ophthalmologists generally made efforts to avoid changing their pre-pandemic anti-VEGF treatment policies and injection numbers.
To minimize exposure to COVID-19, the guidelines recommend that ophthalmologists should wear gloves and masks, limit unnecessary conversations and examinations, and keep patients at a distance from each other in waiting rooms [
16]. Our questionnaire showed that ophthalmologists at all facilities wore masks and attached shields to the slit-lamp microscopes. Additionally, face guards and gloves were used to protect the ophthalmologists against infection. These findings suggest that Japanese ophthalmologists should follow these guidelines and make efforts to prevent infection.
This study had several limitations. First, the participating facilities were limited to university hospitals and do not reflect data from other clinics. It is ideal to be expanded all clinics around Japan. Changes in the number of COVID-19-positive patients at each participating facility could not be examined, to protect personal information. Therefore, the number of patients released for the entire prefecture in which the facility was located was used in the data analysis. However, patients themselves only knew the number of COVID-19-positive patients released by the prefecture, which is the number thought to have influenced patients’ psychological status and their visits to medical facilities. As a second limitation, in this study we could not compare the changes in central retinal thickness or visual acuity before and after the pandemic. The reason for this is that COVID-19 positive individuals may have been included in our data. To prevent disclosure of personal information, we were not able to examine the visual acuity or central retinal thickness of the COVID-19 positive patients. On the other hand, the injection number of anti-VEGF agents could be examined regardless of the infection of COVID-19. Thus, it is unclear what effect the pandemic had on the improvement in visual acuity and edema in this study.
In conclusion, this study showed that, although there was a temporary decrease in the number of anti-VEGF injections during the third and fourth waves of the COVID-19 pandemic, the annual number of injections for the treatment of DME was in fact maintained at a level similar to that before the pandemic. Moreover, Japanese ophthalmologists followed recommended precautions to prevent infection.
Author Contributions
R.K., Y.T., Y.Y. and M.M. contributed to data collection, data analysis, drafting of the article, and critical revision of the article. H.M., T.H., Y.M., M.S., S.K., T.M., R.N., T.U., H.K., T.J., H.T., D.N., K.N. (Kousuke Noda), R.O., K.N. (Kazuki Nagai), S.Y., M.N., H.N., G.I., A.T., O.S. and K.K. participated in data collection. M.I. and Y.T. contributed to conceptualization. All authors have read and agreed to the published version of the manuscript.
Funding
This study was supported in part by a grant-in-aid for scientific research (J160000936) from the Japan Society for the Promotion of Science, Tokyo, Japan.
Institutional Review Board Statement
The study was conducted according to the guidelines of the Declaration of Helsinki, and approved by Ethics Committee of University of Fukui, Mie University Graduate School of Medicine, Shinshu University School of Medicine, Tokushima University Graduate School, Sapporo City General Hospital, Kobe University Graduate School of Medicine, University of Tsukuba, National Defense Medical College, Nara Medical University, Tohoku University Graduate School of Medicine, St. Marianna University School of Medicine, Kagoshima University Graduate School of Medical and Dental Sciences, Saneikai Tsukazaki Hospital, Hokkaido University, Kagawa University Hospital, Gunma University Hospital, Kurume University, Nagoya City University Graduate School of Medical Sciences, Tokyo Medical University Hachioji Medical Center, Osaka Medical and Pharmaceutical University, Kyorin University, Shiga University of Medical Science, and Yamaguchi university school of medicine (protocol code 20210144 and date of approval: 23 March 2022).
Informed Consent Statement
Informed consent was waived since no personal identifiable information was collected or stored in this study.
Data Availability Statement
The datasets generated and/or analyzed during the current study are available from the corresponding author upon reasonable request.
Acknowledgments
We would like to thank Teruyo Kida from Osaka Medical and Pharmaceutical University, Makoto Inoue from Kyorin University, and Takamasa Kinoshita from Sapporo City General Hospital for useful discussions.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Moss, S.E.; Klein, R.; Klein, B.E.K. The 14-year incidence of visual loss in a diabetic population. Ophthalmology 1998, 105, 998–1003. [Google Scholar] [CrossRef]
- Aiello, L.P.; Avery, R.L.; Arrigg, P.G.; Keyt, B.A.; Jampel, H.D.; Shah, S.T.; Pasquale, L.R.; Thieme, H.; Iwamoto, M.A.; Park, J.E.; et al. Vascular Endothelial Growth Factor in Ocular Fluid of Patients with Diabetic Retinopathy and Other Retinal Disorders. N. Engl. J. Med. 1994, 331, 1480–1487. [Google Scholar] [CrossRef] [PubMed]
- Funatsu, H.; Noma, H.; Mimura, T.; Eguchi, S.; Hori, S. Association of Vitreous Inflammatory Factors with Diabetic Macular Edema. Ophthalmology 2009, 116, 73–79. [Google Scholar] [CrossRef] [PubMed]
- Yoshida, S.; Murakami, T.; Nozaki, M.; Suzuma, K.; Baba, T.; Hirano, T.; Sawada, O.; Sugimoto, M.; Takamura, Y.; Tsuiki, E. Review of clinical studies and recommendation for a therapeutic flow chart for diabetic macular edema. Graefes Arch. Clin. Exp. Ophthalmol. 2020, 259, 815–836. [Google Scholar] [CrossRef] [PubMed]
- Wells, J.A.; Glassman, A.R.; Ayala, A.R.; Jampol, L.M.; Bressler, N.M.; Bressler, S.B.; Brucker, A.J.; Ferris, F.L.; Hampton, G.R.; Jhaveri, C.; et al. Aflibercept, Bevacizumab, or Ranibizumab for Diabetic Macular Edema two-year results from a comparative effectiveness randomized clinical trial. Ophthalmology 2016, 123, 1351–1359. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nguyen, Q.D.; Brown, D.M.; Marcus, D.M.; Boyer, D.S.; Patel, S.; Feiner, L.; Gibson, A.; Sy, J.; Rundle, A.C.; Hopkins, J.J.; et al. Ranibizumab for Diabetic Macular Edema: Results from 2 phase III randomized trials: RISE and RIDE. Ophthalmology 2012, 119, 789–801. [Google Scholar] [CrossRef] [PubMed]
- Ogura, Y.; Shiraga, F.; Terasaki, H.; Ohji, M.; Ishida, S.; Sakamoto, T.; Hirakata, A.; Ishibashi, T. Clinical practice pattern in management of diabetic macular edema in Japan: Survey results of Japanese retinal specialists. Jpn. J. Ophthalmol. 2016, 61, 43–50. [Google Scholar] [CrossRef] [PubMed]
- Niwa, Y.; Kakinoki, M.; Sawada, T.; Wang, X.; Ohji, M. Ranibizumab and Aflibercept: Intraocular Pharmacokinetics and Their Effects on Aqueous VEGF Level in Vitrectomized and Nonvitrectomized Macaque Eyes. Investig. Opthalmology Vis. Sci. 2015, 56, 6501–6505. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kakinoki, M.; Sawada, O.; Sawada, T.; Saishin, Y.; Kawamura, H.; Ohji, M. Effect of Vitrectomy on Aqueous VEGF Concentration and Pharmacokinetics of Bevacizumab in Macaque Monkeys. Investig. Opthalmology Vis. Sci. 2012, 53, 5877–5880. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Matsunaga, D.R.; Salabati, M.; Obeid, A.; Wibbelsman, T.D.; Wu, C.; Mahmoudzadeh, R.; Ojalvo, I.; Bilello, J.; Sivalingam, A.; Ho, A.C.; et al. Outcomes of Eyes With Diabetic Macular Edema That Are Lost to Follow-up After Anti–Vascular Endothelial Growth Factor Therapy. Am. J. Ophthalmol. 2021, 233, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Takamura, Y.; Kida, T.; Noma, H.; Inoue, M.; Yoshida, S.; Nagaoka, T.; Noda, K.; Yamada, Y.; Morioka, M.; Gozawa, M.; et al. The Impact of Interval between Recurrence and Reinjection in Anti-VEGF Therapy for Diabetic Macular Edema in Pro Re Nata Regimen. J. Clin. Med. 2021, 10, 5738. [Google Scholar] [CrossRef] [PubMed]
- Korobelnik, J.-F.; Loewenstein, A.; Eldem, B.; Joussen, A.M.; Koh, A.; Lambrou, G.N.; Lanzetta, P.; Li, X.; Lövestam-Adrian, M.; Navarro, R.; et al. Anti-VEGF intravitreal injections in the era of COVID-19: Responding to different levels of epidemic pressure. Graefes Arch. Clin. Exp. Ophthalmol. 2021, 259, 567–574. [Google Scholar] [CrossRef] [PubMed]
- Yang, K.-B.; Feng, H.; Zhang, H. Effects of the COVID-19 Pandemic on Anti-vascular Endothelial Growth Factor Treatment in China. Front. Med. 2020, 7, 576275. [Google Scholar] [CrossRef] [PubMed]
- Galiero, R.; Pafundi, P.C.; Nevola, R.; Rinaldi, L.; Acierno, C.; Caturano, A.; Salvatore, T.; Adinolfi, L.E.; Costagliola, C.; Sasso, F.C. The Importance of Telemedicine during COVID-19 Pandemic: A Focus on Diabetic Retinopathy. J. Diabetes Res. 2020, 2020, 9036847. [Google Scholar] [CrossRef] [PubMed]
- Wong, T.Y.; Bandello, F. Academic Ophthalmology during and after the COVID-19 Pandemic. Ophthalmology 2020, 127, e51–e52. [Google Scholar] [CrossRef] [PubMed]
- Korobelnik, J.-F.; Loewenstein, A.; Eldem, B.; Joussen, A.M.; Koh, A.; Lambrou, G.N.; Lanzetta, P.; Li, X.; Lövestam-Adrian, M.; Navarro, R.; et al. Guidance for anti-VEGF intravitreal injections during the COVID-19 pandemic. Graefes Arch. Clin. Exp. Ophthalmol. 2020, 258, 1149–1156. [Google Scholar] [CrossRef] [PubMed]
- Terasaki, H.; Ogura, Y.; Kitano, S.; Sakamoto, T.; Murata, T.; Hirakata, A.; Ishibashi, T. Management of diabetic macular edema in Japan: A review and expert opinion. Jpn. J. Ophthalmol. 2017, 62, 1–23. [Google Scholar] [CrossRef] [PubMed]
- Sugimoto, M.; Tsukitome, H.; Okamoto, F.; Oshika, T.; Ueda, T.; Niki, M.; Mitamura, Y.; Ishikawa, H.; Gomi, F.; Kitano, S.; et al. Clinical preferences and trends of anti-vascular endothelial growth factor treatments for diabetic macular edema in Japan. J. Diabetes Investig. 2018, 10, 475–483. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Weiss, M.; Sim, D.A.; Herold, T.; Schumann, R.G.; Liegl, R.; Kern, C.; Kreutzer, T.; Schiefelbein, J.; Rottmann, M.; Priglinger, S.; et al. Compliance and Adherence of Patients With Diabetic Macular Edema to Intravitreal Anti–Vascular Endothelial Growth Factor Therapy in Daily Practice. Retina 2018, 38, 2293–2300. [Google Scholar] [CrossRef] [PubMed]
- Kosaka, M.; Hashimoto, T.; Ozaki, A.; Tanimoto, T.; Kami, M. Delayed COVID-19 vaccine roll-out in Japan. Lancet 2021, 397, 2334–2335. [Google Scholar] [CrossRef]
| Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).

 ,
, {kind=link}
{kind=link}

