Previous studies have shown that the role of HCPs in emergencies exceeds far beyond providing medical care and that they have a significant impact on the social and economic functioning of communities during disasters [
1]. While HCPs worldwide have been praised for their frontline efforts in the care and treatment of patients with COVID-19, very little is known about how HCPs have responded to the current emergency and the specific global and local events that trigger their responses [
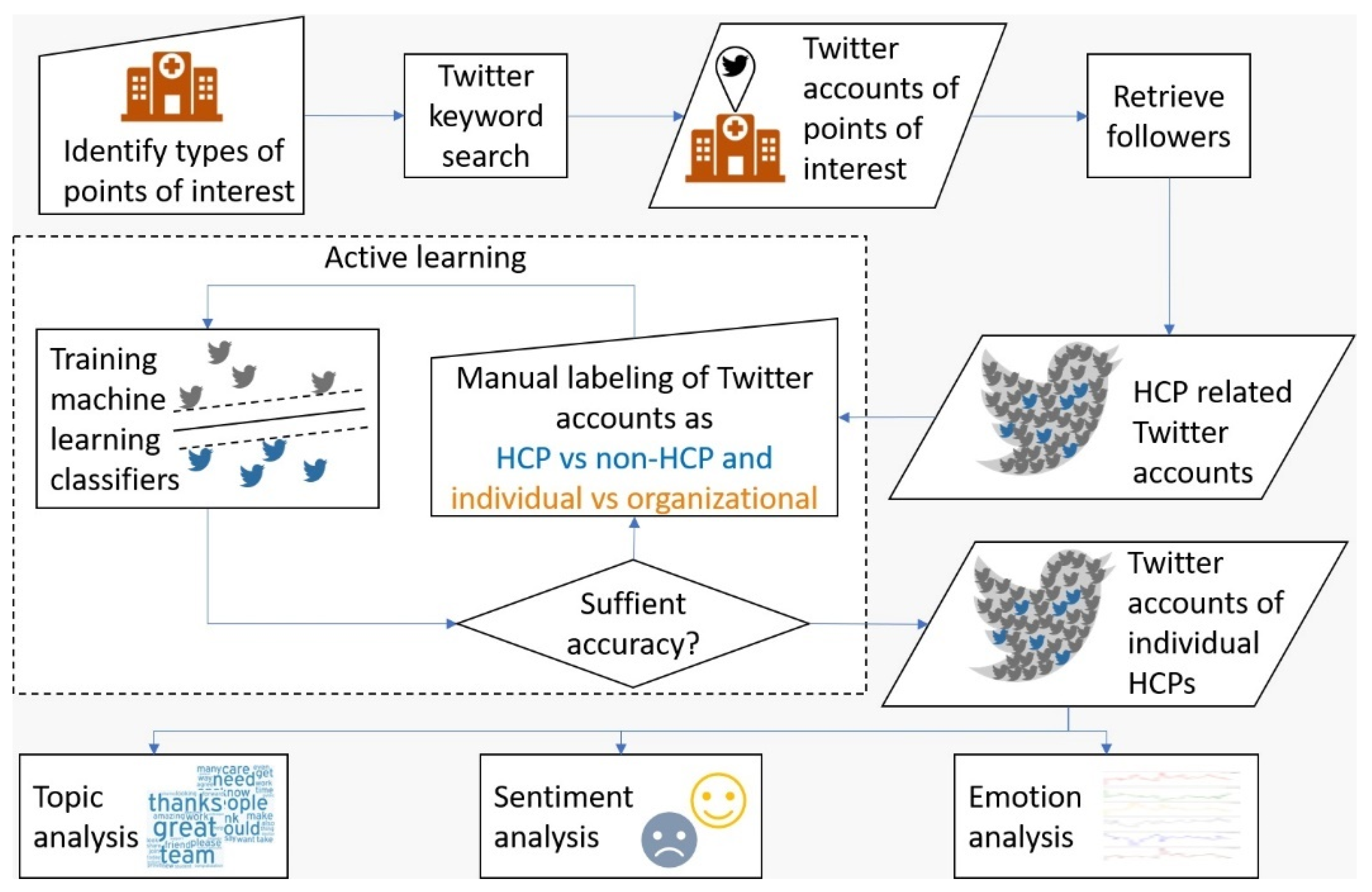
34]. Using an analysis of HCPs’ Twitter posts before and during the COVID-19 outbreak in the US and UK, the current study examined to what extent HCPs’ discourse and emotional display are associated with local and global social, cultural, and political contexts.
Overall, our results indicate that HCPs in the US and UK faced similar health and social challenges related to the pandemic, which is reflected in their discussion topics, sentiments, and emotional display. However, the experiences of HCPs in the two countries are also subject to local socio-political trends, as well as cultural norms in their emotional display. Some key findings and lessons that emerge from our results are summarized below.
4.1. Discourse Topics and Sentiments
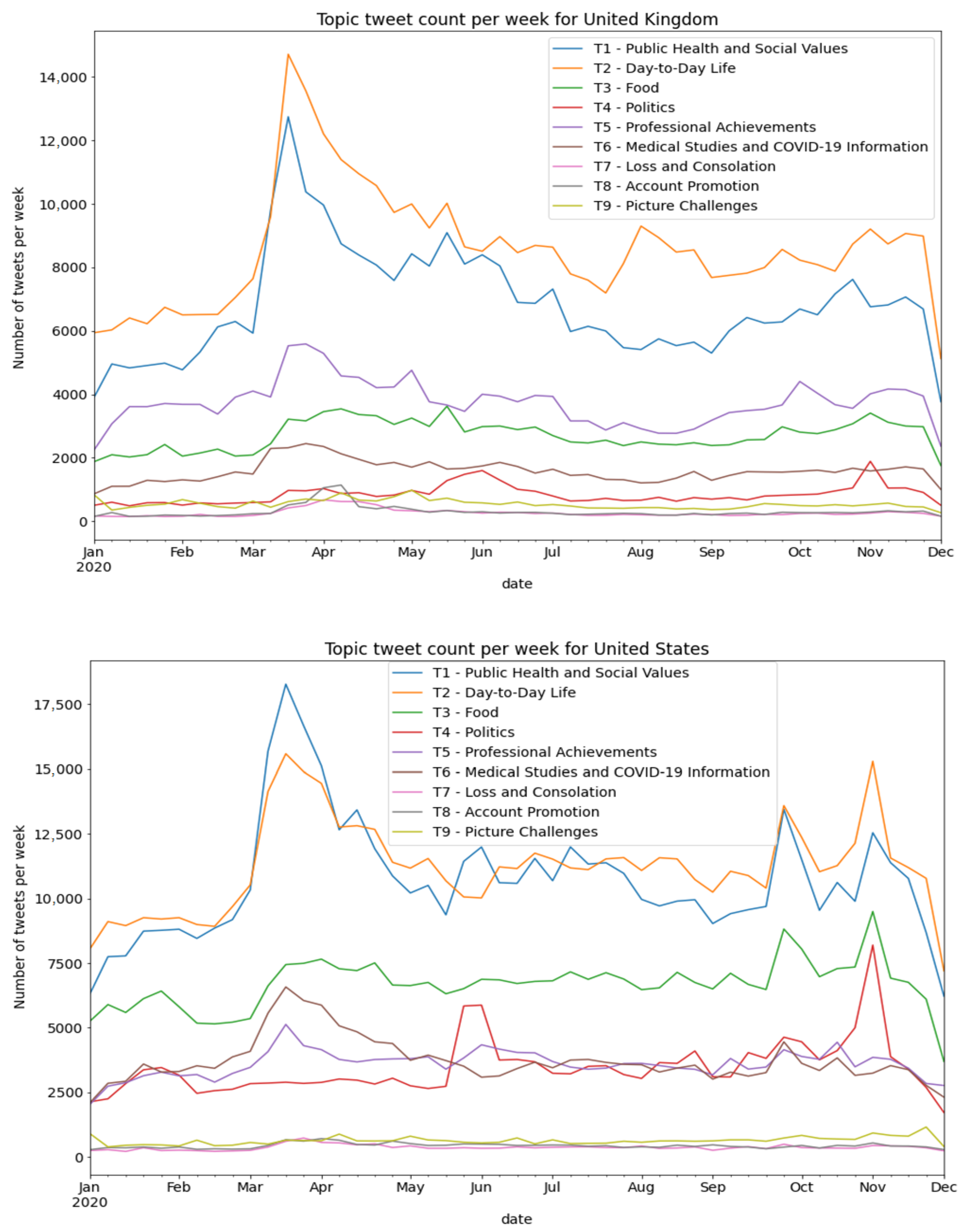
Our analysis of the discussion topics highlighted similarities and differences between the experience of HCPs in the US and the UK. For HCPs in both countries, the greatest proportion of discussion was directly associated with professional content (public health, social values, personal achievement, and COVID-19). In both countries, a full quarter of the discussions were related to public health and social values, which was the leading topic of interest. In both countries, just 1% of HCPs’ discussions focused on loss and condolences. However, British HCPs dedicated a larger proportion of their discussions to daily life issues and professional achievements, while American HCPs were significantly busier with discussions on politics and food.
We expected that HCPs would share their impressions of (or reflections on) their daily encounters with illness and death on social media. However, in contrast to our expectations, loss and trauma were underrepresented in HCPs’ discussions. This finding aligns with the recent work of Ojo et al. [
35], who found that tweets with healthcare-led hashtags expressed more positivity and more action-oriented language than non-healthcare-initiated hashtags. It is possible that the reluctance of HCPs to share negative events on social media reflects societal expectations of professionalism from medical experts [
13,
36].
Similarities and differences between the two groups (US and UK) were also pronounced in the sentiments that accompanied their discussions. Both US and UK authors expressed fear after the virus reproduction rate increased and anger in the face of death. Additionally, in both the American and British groups, discussing politics was associated with the lowest level of positive sentiments. However, we found that British HCPs were more likely to express positive sentiment than American HCPs across all discussion topics.
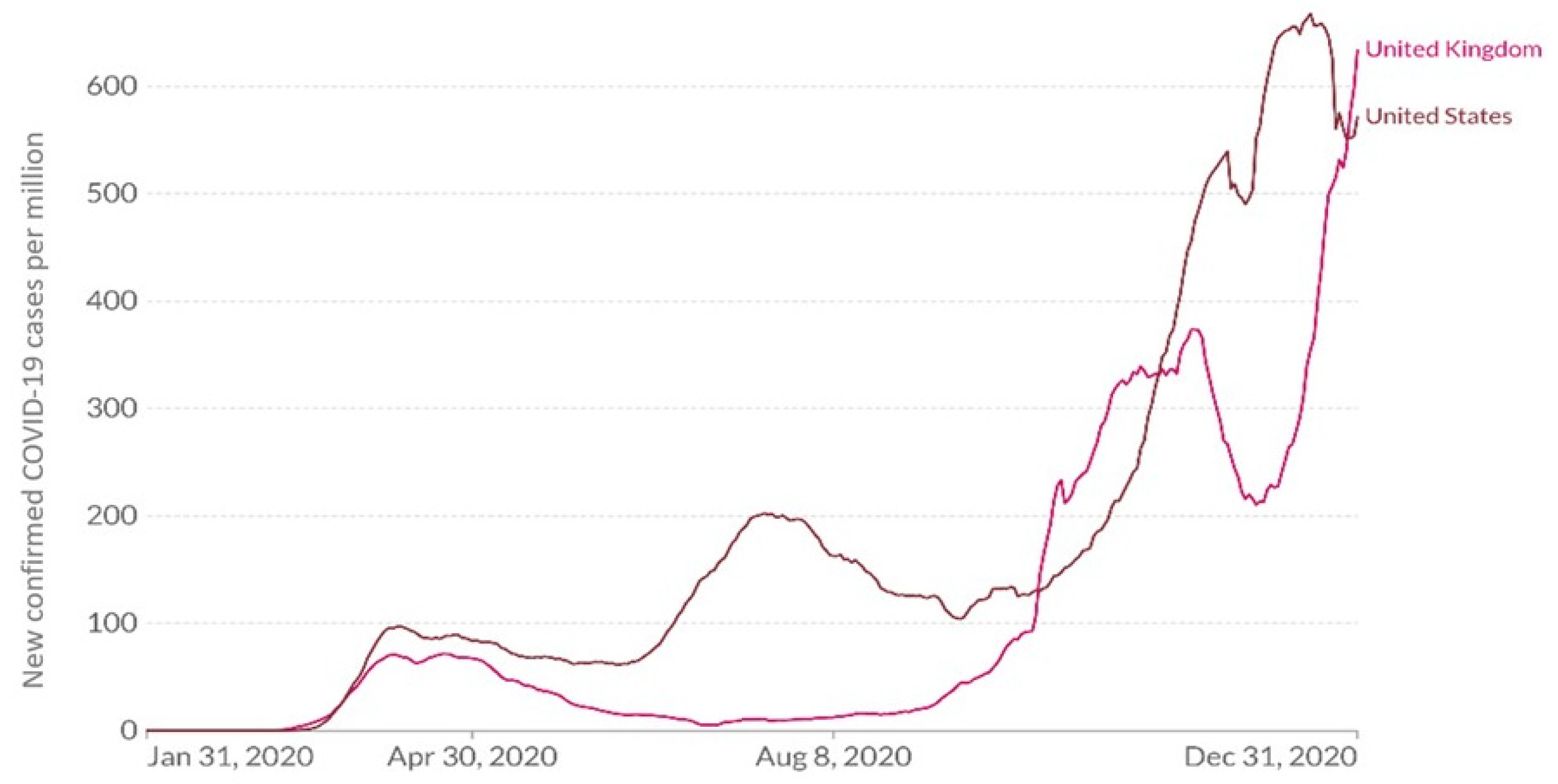
Examining time-related changes in the topics discussed showed an increase in the number of posts published by the two groups at the beginning of the pandemic. Moreover, political discourse increased in both groups following George Floyd’s death (25 May 2020) and the American elections (3 November 2020), with a sharp increase seen in the discourse of HCPs from the US and a slight increase among HCPs from the UK. Overall, however, the groups differed in terms of the trends in the topics discussed. For example, American HCPs published an increasing number of posts on public health and social values as the pandemic waves approached their peaks, whereas in British HCPs such a trend was obtained only in the first wave.
4.2. Emotional Display
Consistent with previous studies on the general population [
37] and HCPs [
38], among both British and American HCPs, we observed an increase in negative emotions and a decrease in positive emotions throughout 2020 (compared to 2019). For instance, a recent study examining the expression of the six basic emotions on Twitter during the COVID-19 pandemic in Portugal revealed an association between the emotional patterns observed in tweets and the pandemic’s evolution, with more negative tweets posted at the beginning of the pandemic [
39].
As is evidenced by prior studies [
20,
21], HCPs in both counties shared a sharp increase in their levels of fear during the first wave of the pandemic, which gradually reduced with time, and an increase in sadness that was maintained over time. Fear was also experienced by both groups in response to an increase in the virus reproduction rates, whereas anger was experienced by both groups in response to a rise in the number of COVID deaths. Despite the similar patterns of emotional response, the magnitude of HCPs’ emotions was higher among American HCPs than among their British counterparts.
Interestingly, our results showed that HCPs from both the US and the UK responded in a similar way, emotionally, to global health changes as well as to socio-political events. Our analysis showed that the death of Gorge Floyd was reflected by a sharp increase in fear, anger, and disgust among American, as well as British HCPs. As in the US, this event also resulted in a wave of protests in the UK, which had the largest Black Lives Matter protests in the world outside the US. Even before George Floyd’s death, protesters were already galvanized by the death of a Black transport worker in London. The worker was killed in a racist attack at work that occurred after she reported that a White man spat on her and was denied proper protection [
40].
Together, these results paint a detailed and dynamic portrait of HCPs’ state of mind in times of emergency [
22,
34]. Specifically, these findings suggest that HCPs around the globe are influenced by similar health, social, and political events but that these events elicit a similar profile of cognitive and emotional responses. For example, our results demonstrated that both British and American HCPs experienced elevated levels of negative emotions with increasing number of COVID-19 case, as well as with political instability. These results are in line with previous studies showing that changes in mood word frequencies on Twitter corresponded with real-world events, such as the unexpected deaths of popular individuals, public unrest, or natural disasters [
41,
42]. Such studies showed that negative mood indicators coincided both with periodic events, such as holidays or the new school year, but also with major socio-political events, such as the announcement of public spending cuts by the government and riots [
43,
44]. Thus, this study provides further support for the vast potential of utilizing Twitter to monitor and predict public health responses in times of emergency [
45,
46].
In addition to the similarities observed in the quality and timing of American and British HCPs’ responses to the pandemic, our findings revealed important differences between the two groups. These differences were found in the discussion topics, as well as in the prevalence and magnitude of emotional expression. Generally, HCPs in the UK reported fewer and weaker negative sentiments and emotions than their counterparts in the US, both before and during the COVID-19 outbreak.
Several explanations may shed light on the consistent differences observed between American and British HCPs in the prevalence and magnitude of the expression of negative emotions. One possible explanation relates to cultural differences regarding the rules of emotional display. Although the US and UK share a common language and a historical past, they often differ in the socio-cultural norms of emotional expression [
47,
48]. Previous studies have suggested that Americans are more likely to express negative emotions (particularly at work) than people from Britain. These studies suggest that the British are more driven by social desirability and have a greater reluctance in disclosing their feelings or expressing their emotions [
45]. Moreover, a study examining the emotional expression of workers from the US and UK found that American workers were more likely than British workers to expect warmth from their colleagues and more likely to expect this to be genuine than the British. Additionally, British workers were significantly more likely to suppress their anger in their workplace than Americans [
48].
Another possible explanation for the differences observed between the groups relates to differences in language expression of emotions. Based on an analysis of words carrying emotional content in 20th-century English language books, Acerbi et al. [
49] found that American English has become decidedly more “emotional” than British English. This difference has apparently developed only since the 1960s as part of a more general stylistic differentiation between American and British English. The authors suggested that the relative increase in American mood words was associated with both the increase in antisocial and narcissistic sentiments in American popular culture and a corresponding decrease in words indicating social interactions. While these findings do not indicate that Americans are more emotion-driven in their real-world interactions, their use of words is an informative sample of possible cultural differences.
From another point of view, the differences observed between the US and UK HCPs may be associated with the healthcare systems’ response to the COVID-19 crisis [
24,
25,
26,
27]. While all countries faced common challenges, including a shortage of medical technology and scaling up testing capacity [
50], differences exist in health system capacity and political leadership. A recent comparative analysis of health policy responses to COVID-19 in Canada, Ireland, the UK, and the US from January to November 2020 suggested that in the US, the lack of universal health coverage has created barriers to accessing care and political pushback against scientific leadership, thus negatively affecting crisis response [
51].
4.3. Relationships between Politics and Health
Relationships between politics and public health have been discussed in the literature; for example, one study examined the impact of government styles and health outcomes over the years [
52]. However, the COVID-19 pandemic accelerated and intensified political aspects of the health process [
53]. The close connection between politics and pandemics is a known issue. According to Tognotti [
54], pandemics’ control has always been controversial, since the associated policies raise ethical, political, and socioeconomic issues, trying to balance public interest and individual rights.
Next, we discuss how this study highlights the political aspects of HCPs’ discourse. First, we found that the public health and social values topics had the second-highest relationship with the political topics (after day-to-day life, which had the greatest relationship), as seen in
Table 3. Second, the political topic maintains its volume throughout 2020 among US and UK HCPs, with increases seen around the Gorge Floyd incident and the American election. While of all the topics examined, sentiment for the political topics was found to be the lowest in both countries, UK authors were more positive and spoke about political issues less frequently than the US authors. Sentiment in political discourse is sometimes used as a proxy for trust [
55]. Thus, the low sentiment score of the political topic in both countries could be an indication of the low level of trust that HCPs have in politicians and the policies they promote. The issue of trust is crucial during emergencies for increasing citizens’ adherence to guidelines, especially in the health context [
56]. The WHO [
57] defined risk communication as “the real-time exchange of information, advice, and opinions between experts or officials and people who face a threat (hazard) to their survival, health, or economic or social wellbeing”. Its ultimate purpose is to enable everyone at risk to make informed decisions to mitigate the effects of the threat (hazard), such as a disease outbreak, and take protective and preventive action”. According to a recent report, the WHO [
58] emphasized that risk communication has shifted from a focus on the dissemination of information to an improved understanding of the communication process leading to changes in behaviors and beliefs. To achieve this goal, and based on the results presented in this study, more attention should be given to the relationships between policymaking, politicians, and HCPs.
4.4. Limitations and Recommendations for Further Studies
There are a few limitations of this research that need to be considered. First, this study is limited to HCPs who are active on Twitter, and therefore, we cannot generalize our findings to the entire HCP population. In addition, since the topics, sentiment, and emotion analysis were performed using machine learning algorithms, our results are an estimation of HCPs’ experiences as opposed to experiences confirmed by HCPs. Finally, our data collection consists of tweets from January 2019 through January 2021, and additional waves of the COVID-19 pandemic have occurred since then. Further research on the long-term effects of the pandemic on the well-being of HCPs is needed.


 ,
, 

{kind=link}
{kind=link}
{kind=link}
{kind=link}



