
Age-Dependent Biomarkers for Prediction of In-Hospital Mortality in COVID-19 Patients


Abstract
:1. Introduction
2. Methods
2.1. Study Design and Population
2.2. Data Source, Measurements, and Variables
2.3. Laboratory Methods
2.4. Statistical Analysis
3. Results
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
References
- WHO. Director-General’s Opening Remarks at The Media Briefing on COVID-19—11-March-2020. Available online: https://www.who.int/director-general/speeches/detail/who-director-general-s-opening-remarks-at-the-media-briefing-on-COVID-19—11-March-2020 (accessed on 4 December 2021).
- Petrilli, C.M.; Jones, S.A.; Yang, J.; Rajagopalan, H.; O’Donnell, L.; Chernyak, Y.; Tobin, K.A.; Cerfolio, R.J.; Francois, F.; Horwitz, L.I. Factors associated with hospital admission and critical illness among 5279 people with coronavirus disease 2019 in New York City: Prospective cohort study. BMJ 2020, 369, m1966. [Google Scholar] [CrossRef] [PubMed]
- Ciotti, M.; Angeletti, S.; Minieri, M.; Giovannetti, M.; Benvenuto, D.; Pascarella, S.; Sagnelli, C.; Bianchi, M.; Bernardini, S.; Ciccozzi, M. COVID-19 Outbreak: An Overview. Chemotherapy 2020, 64, 215–223. [Google Scholar] [CrossRef] [PubMed]
- Richardson, S.; Hirsch, J.S.; Narasimhan, M.; Crawford, J.M.; McGinn, T.; Davidson, K.W.; the Northwell COVID-19 Research Consortium. Presenting Characteristics, Comorbidities, and Outcomes among 5700 Patients Hospitalized with COVID-19 in the New York City Area. JAMA—J. Am. Med. Assoc. 2020, 323, 2052–2059. [Google Scholar] [CrossRef] [PubMed]
- Asch, D.A.; Sheils, N.E.; Islam, N.; Chen, Y.; Werner, R.M.; Buresh, J.; Doshi, J.A. Variation in US Hospital Mortality Rates for Patients Admitted with COVID-19 during the First 6 Months of the Pandemic. JAMA Intern. Med. 2021, 181, 471–478. [Google Scholar] [CrossRef] [PubMed]
- Strålin, K.; Wahlström, E.; Walther, S.; Bennet-Bark, A.M.; Heurgren, M.; Lindén, T.; Holm, J.; Hanberger, H. Mortality trends among hospitalised COVID-19 patients in Sweden: A nationwide observational cohort study. Lancet Reg. Health—Eur. 2021, 4, 100054. [Google Scholar] [CrossRef] [PubMed]
- Ministry of Health. COVID-19 Dashboard 2022. Available online: https://datadashboard.health.gov.il/COVID-19/general (accessed on 25 April 2022).
- Strålin, K.; Wahlström, E.; Walther, S.; Bennet-Bark, A.M.; Heurgren, M.; Lindén, T.; Holm, J.; Hanberger, H. Mortality in hospitalized COVID-19 patients was associated with the COVID-19 admission rate during the first year of the pandemic in Sweden. Infect. Dis. 2022, 54, 145–151. [Google Scholar] [CrossRef]
- Brosh-nissimov, T.; Orenbuch-harroch, E.; Chowers, M.; Elbaz, M.; Nesher, L.; Stein, M.; Maor, Y.; Cohen, R.; Hussein, K.; Weinberger, M.; et al. BNT162b2 vaccine breakthrough: Clinical characteristics of 152 fully vaccinated hospitalized COVID-19 patients in Israel. Clin. Microbiol. Infect. 2021, 27, 1652–1657. [Google Scholar] [CrossRef]
- Luo, X.; Zhou, W.; Yan, X.; Guo, T.; Wang, B.; Xia, H.; Ye, L.; Xiong, J.; Jiang, Z.; Liu, Y.; et al. Prognostic Value of C-Reactive Protein in Patients With Coronavirus 2019. Clin. Infect. Dis. 2020, 71, 2174–2179. [Google Scholar] [CrossRef]
- Benjamin, G.M.; Ghazal, A.; Katya, L.; Yang, L.; Siff, E.J.; Chiang, S.S.; Salazar-Mather, T.P.; Dumenco, L.; Savaria, M.C.; Aung, S.N.; et al. Predictors of COVID-19 severity: A literature review. Rev. Med. Virol. 2021, 31, 1–10. [Google Scholar] [CrossRef]
- Cecconi, M.; Piovani, D.; Brunetta, E.; Aghemo, A.; Greco, M.; Ciccarelli, M.; Angelini, C.; Voza, A.; Omodei, P.; Vespa, E.; et al. Early predictors of clinical deterioration in a cohort of 239 patients hospitalized for COVID-19 infection in Lombardy. Italy J. Clin. Med. Res. 2020, 9, 1548. [Google Scholar] [CrossRef]
- Malik, P.; Patel, U.; Mehta, D.; Patel, N.; Kelkar, R.; Akrmah, M.; Gabrilove, J.L.; Sacks, H. Biomarkers and outcomes of COVID-19 hospitalisations: Systematic review and meta-analysis. BMJ Evid.-Based Med. 2021, 26, 107–108. [Google Scholar] [CrossRef] [PubMed]
- Tan, L.; Wang, Q.; Zhang, D.; Ding, J.; Huang, Q.; Tang, Y.-Q.; Wang, Q.; Miao, H. Lymphopenia predicts disease severity of COVID-19: A descriptive and predictive study. Signal Transduct. Target. Ther. 2020, 5, 1–3. [Google Scholar] [CrossRef] [Green Version]
- Fazal, M. C-Reactive Protein a Promising Biomarker of COVID-19 Severity. Korean J. Clin. Lab. Sci. 2021, 53, 201–207. [Google Scholar] [CrossRef]
- Yassin, A.; Ghzawi, A.; Al-Mistarehi, A.-H.; El-Salem, K.; Benmelouka, A.Y.; Sherif, A.M.; BenhadjDahman, N.; AlAdamat, N.; Jemel, A.; Negida, A.; et al. Mortality rate and biomarker expression within COVID-19 patients who develop acute ischemic stroke: A systematic review and meta-analysis. Future Sci. OA 2021, 7, FSO713. [Google Scholar] [CrossRef]
- Loomba, R.S.; Villarreal, E.G.; Farias, J.S.; Aggarwal, G.; Aggarwal, S.; Flores, S. Serum biomarkers for prediction of mortality in patients with COVID-19. Ann. Clin. Biochem. 2022, 59, 15–22. [Google Scholar] [CrossRef] [PubMed]
- Wang, G.; Wu, C.; Zhang, Q.; Wu, F.; Yu, B.; Lv, J.; Li, Y.; Li, T.; Zhang, S.; Wu, C.; et al. C-reactive protein level may predict the risk of COVID-19 aggravation. Open Forum Infect. Dis. 2020, 7, 1–5. [Google Scholar] [CrossRef]
- Villoteau, A.; Asfar, M.; Otekpo, M.; Loison, J.; Gautier, J.; Annweiler, C.; on behalf of the GERIA-COVID study group. Elevated C-reactive protein in early COVID-19 predicts worse survival among hospitalized geriatric patients. PLoS ONE 2021, 16, e0256931. [Google Scholar] [CrossRef]
- Milenkovic, M.; Hadzibegovic, A.; Kovac, M.; Jovanovic, B.; Stanisavljevic, J.; Djikic, M.; Sijan, D.; Ladjevic, N.; Palibrk, I.; Djukanovic, M.; et al. D-dimer, CRP, PCT, and IL-6 Levels at Admission to ICU Can Predict In-Hospital Mortality in Patients with COVID-19 Pneumonia. Oxid. Med. Cell. Longev. 2022, 2022, 8997709. [Google Scholar] [CrossRef]
- Yitbarek, G.Y.; Walle Ayehu, G.; Asnakew, S.; Ayele, F.Y.; Gare, M.B.; Mulu, A.T.; Dagnaw, F.T.; Melesie, B.D. The role of C-reactive protein in predicting the severity of COVID-19 disease: A systematic review. SAGE Open Med. 2021, 9, 20503121211050755. [Google Scholar] [CrossRef]
- Liu, F.; Li, L.; Xu, M.; Wu, J.; Luo, D.; Zhu, Y.; Li, B.; Song, X.; Zhou, X. Prognostic value of IL-6, CRP, and PCT in patients with COVID-19. J. Clin. Virol. 2020, 127, 104370. [Google Scholar] [CrossRef]
- Smilowitz, N.R.; Nguy, V.; Aphinyanaphongs, Y.; Newman, J.D.; Xia, Y.; Reynolds, H.R.; Hochman, J.S.; Fishman, G.I.; Berger, J.S. Multiple Biomarker Approach to Risk Stratification in COVID-19. Circulation 2021, 143, 1338–1340. [Google Scholar] [CrossRef] [PubMed]
- Pepys, M.B. C-reactive protein predicts outcome in COVID-19: Is it also a therapeutic target? Eur. Heart J. 2021, 42, 2280–2283. [Google Scholar] [CrossRef] [PubMed]
- Feigin, E.; Levinson, T.; Berliner, S.; Zeltser, D.; Itzhak, S.; Shenhar-Tsarfaty, S.; Egoz, E.; Meilik, A.; Goldiner, I.; Rogowski, O.; et al. Patients who are admitted to the Department of Internal Medicine with a very low C-reactive protein concentration. Eur. J. Inflamm. 2021, 19, 1–7. [Google Scholar] [CrossRef]
- Brusselaers, N.; Lagergren, J. The Charlson Comorbidity Index in Registry-based Research. Methods Inf. Med. 2017, 56, 401–406. [Google Scholar] [CrossRef]
- Ziv-Baran, T.; Wasserman, A.; Goldiner, I.; Stark, M.; Shenhar-Tsarfaty, S.; Shapira, I.; Zeltser, D.; Mailis, I.; Berliner, S.; Rogowski, O. The association between C-reactive protein and common blood tests in apparently healthy individuals undergoing a routine health examination. Clin. Chim. Acta 2020, 501, 33–41. [Google Scholar] [CrossRef]
- Kass, G.V. An Exploratory Technique for Investigating Large Quantities of Categorical Data. Appl. Stat. 1980, 29, 119–127. [Google Scholar] [CrossRef]
- Bartolomeo, N.; Giotta, M.; Trerotoli, P. In-Hospital Mortality in Non-COVID-19-Related Diseases before and during the Pandemic: A Regional Retrospective Study. Int. J. Environ. Res. Public Health 2021, 18, 10886. [Google Scholar] [CrossRef]
- Castelo-Branco, C.; Soveral, I. The immune system and aging: A review. Gynecol. Endocrinol. 2014, 30, 16–22. [Google Scholar] [CrossRef]
- Pepys, M.B.; Hirschfield, G.M. C-reactive protein: A critical update. J. Clin. Investig. 2003, 112, 299. [Google Scholar] [CrossRef]
- Zimmerman, O.; Rogowski, O.; Aviram, G.; Mizrahi, M.; Zeltser, D.; Justo, D.; Dahan, E.; Arad, R.; Touvia, O.; Tau, L.; et al. C-reactive protein serum levels as an early predictor of outcome in patients with pandemic H1N1 influenza A virus infection. BMC Infect. Dis. 2010, 10, 288. [Google Scholar] [CrossRef] [Green Version]
- Ward, C. Point-of-care C-reactive protein testing to optimise antibiotic use in a primary care urgent care centre setting. BMJ Open Qual. 2018, 7, e000391. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Boere, T.M.; van Buul, L.W.; Hopstaken, R.M.; van Tulder, M.W.; Twisk, J.W.M.R.; Verheij, T.J.M.; Hertogh, C.M.P.M. Effect of C reactive protein point-of-care testing on antibiotic prescribing for lower respiratory tract infections in nursing home residents: Cluster randomised controlled trial. BMJ 2021, 374, n2198, Erratum in BMJ 2021, 375, n2894. [Google Scholar] [CrossRef] [PubMed]
- Spaeth, B.; Shephard, M.; Kokcinar, R.; Duckworth, L.; Omond, R. Impact of point-of-care testing for white blood cell count on triage of patients with infection in the remote Northern Territory of Australia. Pathology 2019, 51, 512–517. [Google Scholar] [CrossRef] [PubMed]
- Horby, P.; Lim, W.S.; Emberson, J.; Mafham, M.; Bell, J.; Linsell, L. Effect of Dexamethasone in Hospitalized Patients With COVID-19: Preliminary Report. N. Engl. J. Med. 2020, 383, 1. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Parameter | All (N = 762) |
|---|---|
| Age (years), median (IQR) | 70.9 (57.8–82.0) |
| Male, n (%) | 455 (59.7%) |
| COPD, n (%) | 76 (12.4%) |
| CHF, n (%) | 52 (8.5%) |
| DM, n (%) | 203 (33.1%) |
| Charlson comorbidity index, median (IQR) | 4 (2–5) |
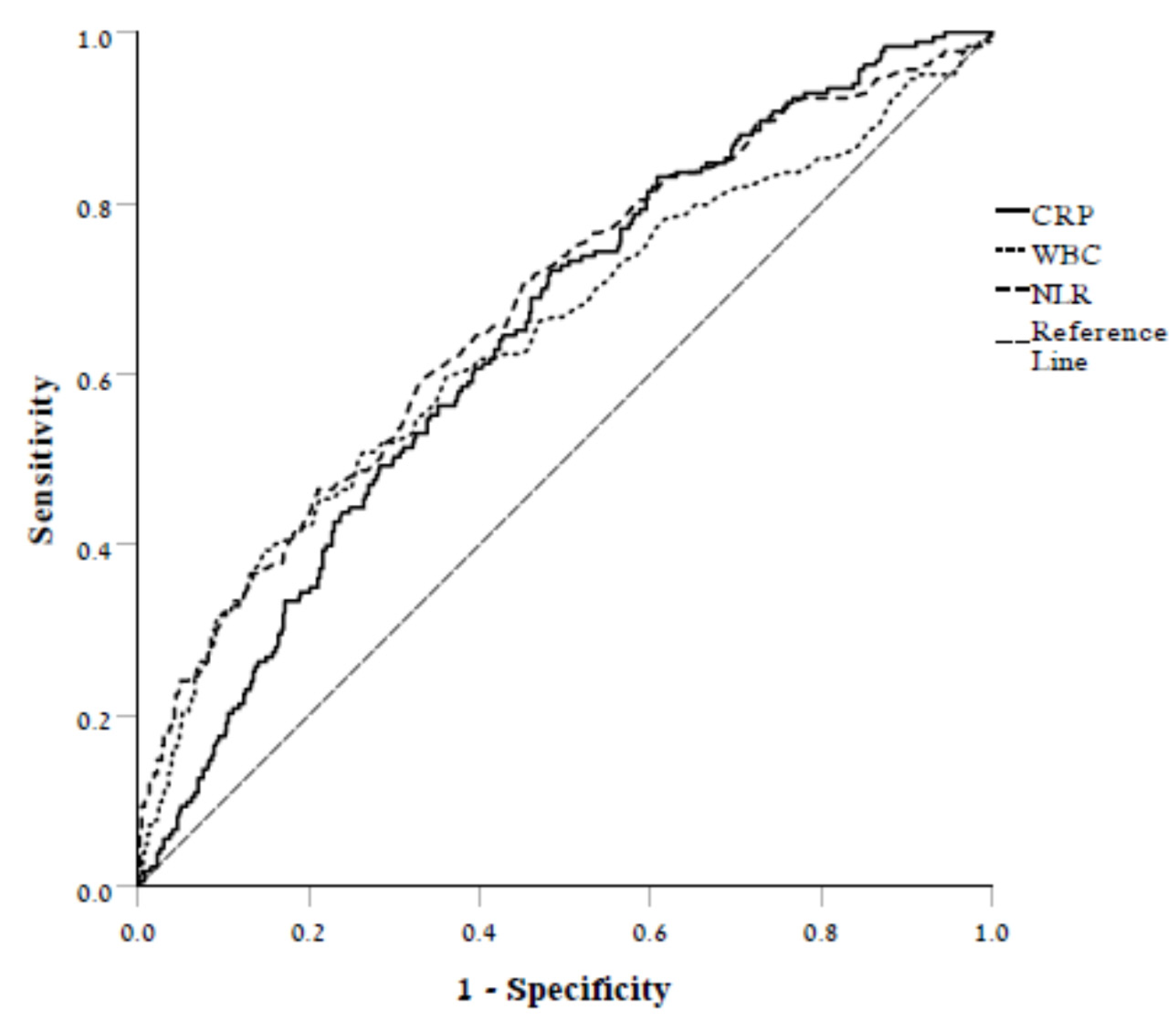
| CRP (mg/L), median (IQR) | 95.4 (36.9–155.6) |
| WBC count (K/µL), median (IQR) | 6.9 (5.1–9.8) |
| NLR, median (IQR) | 6.35 (3.40–11.30) |
| Parameter | In-Hospital Mortality | p | |
|---|---|---|---|
| Survived (N = 571) | Died (N = 191) | ||
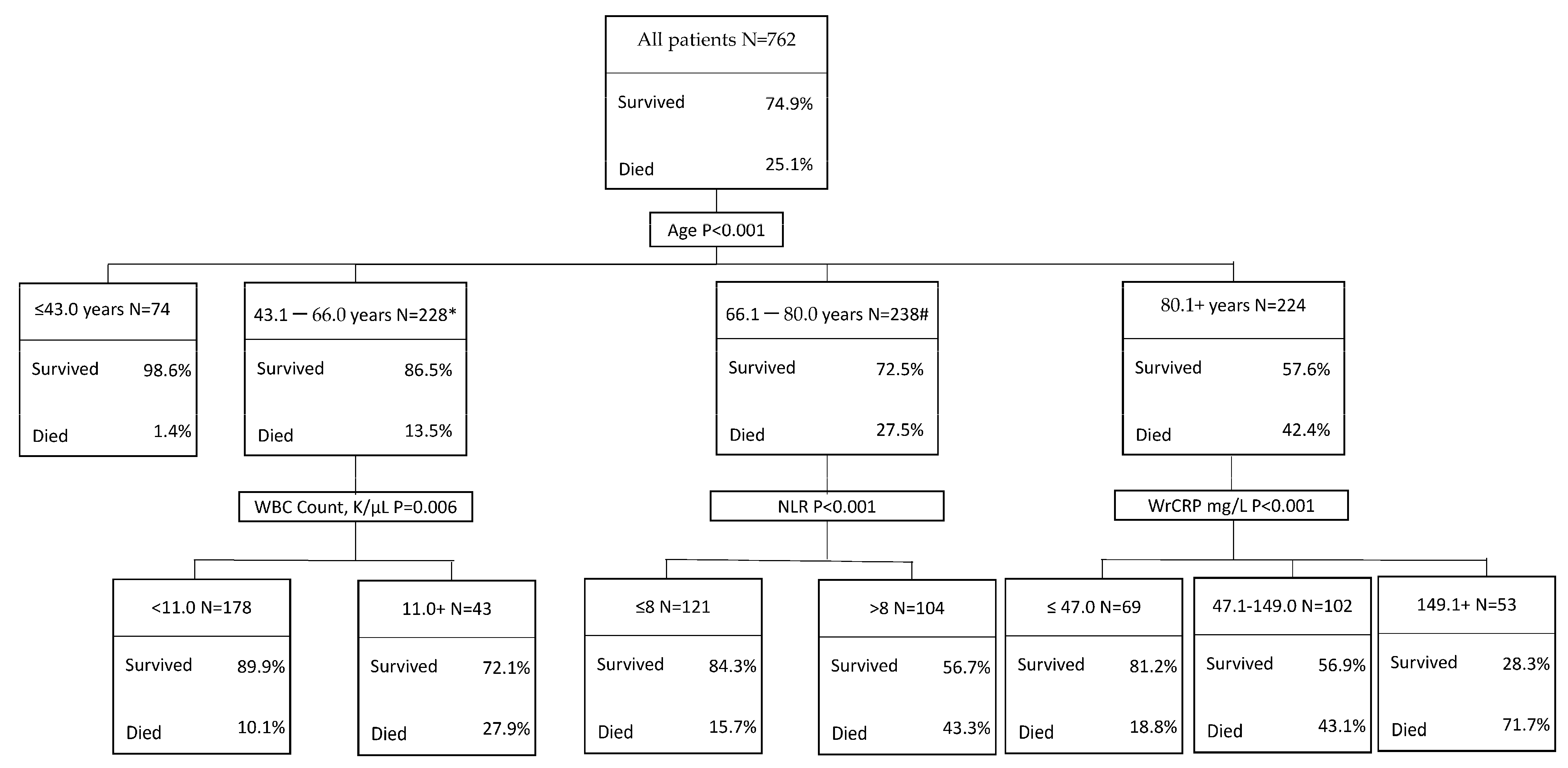
| Age (years), median (IQR) | 67.6 (53.7–78.9) | 79.8 (70.5–87.2) | <0.001 |
| Male, n (%) | 329 (57.6%) | 126 (66.0%) | 0.042 |
| COPD, n (%) | 59 (12.7%) | 17 (11.4%) | 0.680 |
| CHF, n (%) | 35 (7.5%) | 17 (11.4%) | 0.139 |
| DM, n (%) | 147 (31.6%) | 56 (37.6%) | 0.178 |
| Charlson comorbidity index, median (IQR) | 3 (2–5) | 5 (4–7) | <0.001 |
| CRP (mg/L), median (IQR) | 84.9 (28.9–149.5) | 138.2 (69.0–187.6) | <0.001 |
| WBC count (K/µL), median (IQR) | 6.6 (5.0–8.8) | 8.5 (5.9–12.8) | <0.001 |
| NLR, median (IQR) | 5.4 (3.0–9.8) | 9.2 (5.2–19.3) | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Feigin, E.; Levinson, T.; Wasserman, A.; Shenhar-Tsarfaty, S.; Berliner, S.; Ziv-Baran, T. Age-Dependent Biomarkers for Prediction of In-Hospital Mortality in COVID-19 Patients. J. Clin. Med. 2022, 11, 2682. https://doi.org/10.3390/jcm11102682
Feigin E, Levinson T, Wasserman A, Shenhar-Tsarfaty S, Berliner S, Ziv-Baran T. Age-Dependent Biomarkers for Prediction of In-Hospital Mortality in COVID-19 Patients. Journal of Clinical Medicine. 2022; 11(10):2682. https://doi.org/10.3390/jcm11102682
Chicago/Turabian StyleFeigin, Eugene, Tal Levinson, Asaf Wasserman, Shani Shenhar-Tsarfaty, Shlomo Berliner, and Tomer Ziv-Baran. 2022. "Age-Dependent Biomarkers for Prediction of In-Hospital Mortality in COVID-19 Patients" Journal of Clinical Medicine 11, no. 10: 2682. https://doi.org/10.3390/jcm11102682