
Determinants of Pain-Induced Disability in German Women with Endometriosis during the COVID-19 Pandemic

 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Recruitment of the Sample Population/Study Participants
2.2. Pain Intensity
2.3. Pain Disability Index (PDI)
2.4. Patient Health Questionnaire for Depression and Anxiety (PHQ-4)
2.5. Brief Resilience Scale (BRS)
2.6. Statistical Analyses
3. Results
3.1. Demographic Characteristics of the Study Group
3.2. Level of Self-Reported Pain-Induced Disability in Women with Endometriosis during the COVID-19 Pandemic in Comparison with Previously Described Populations
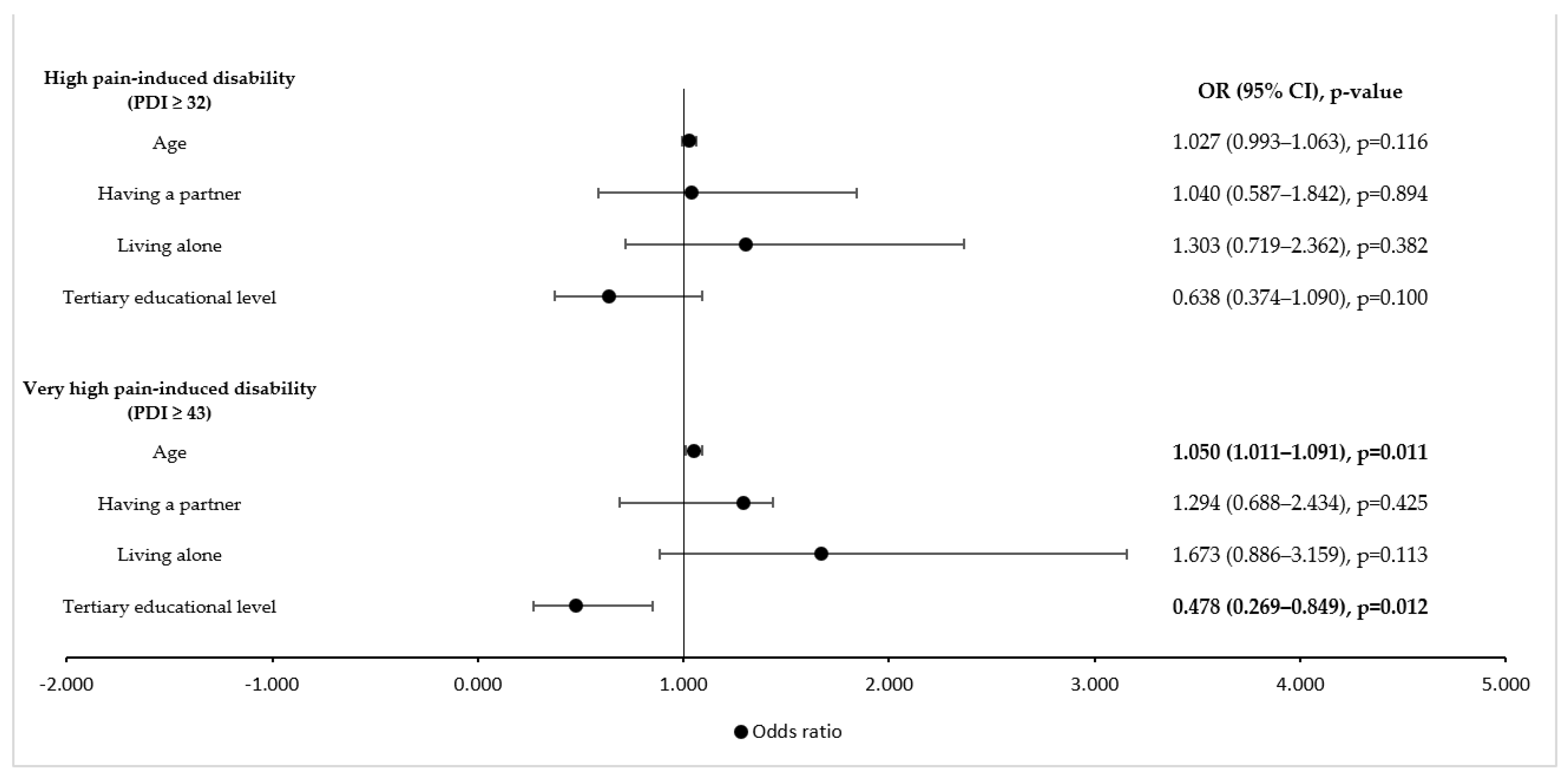
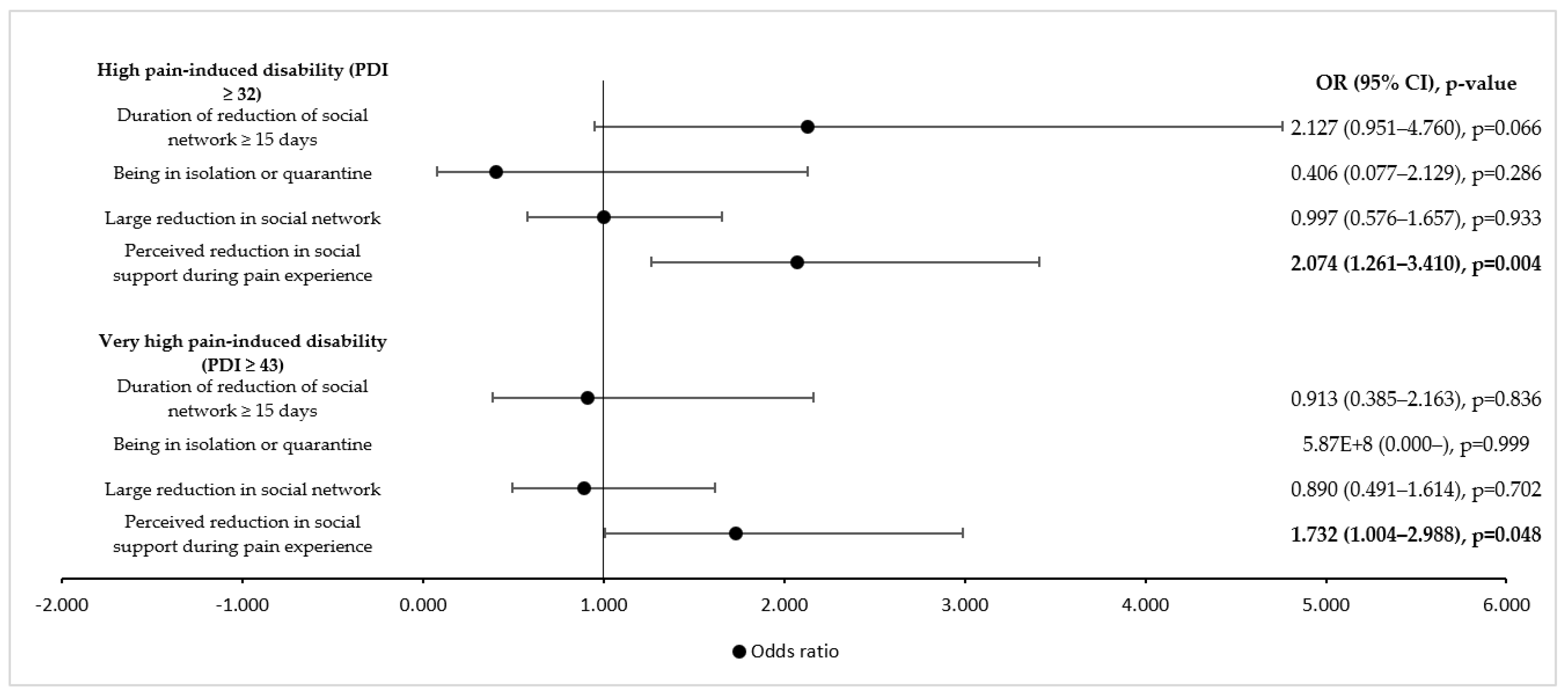
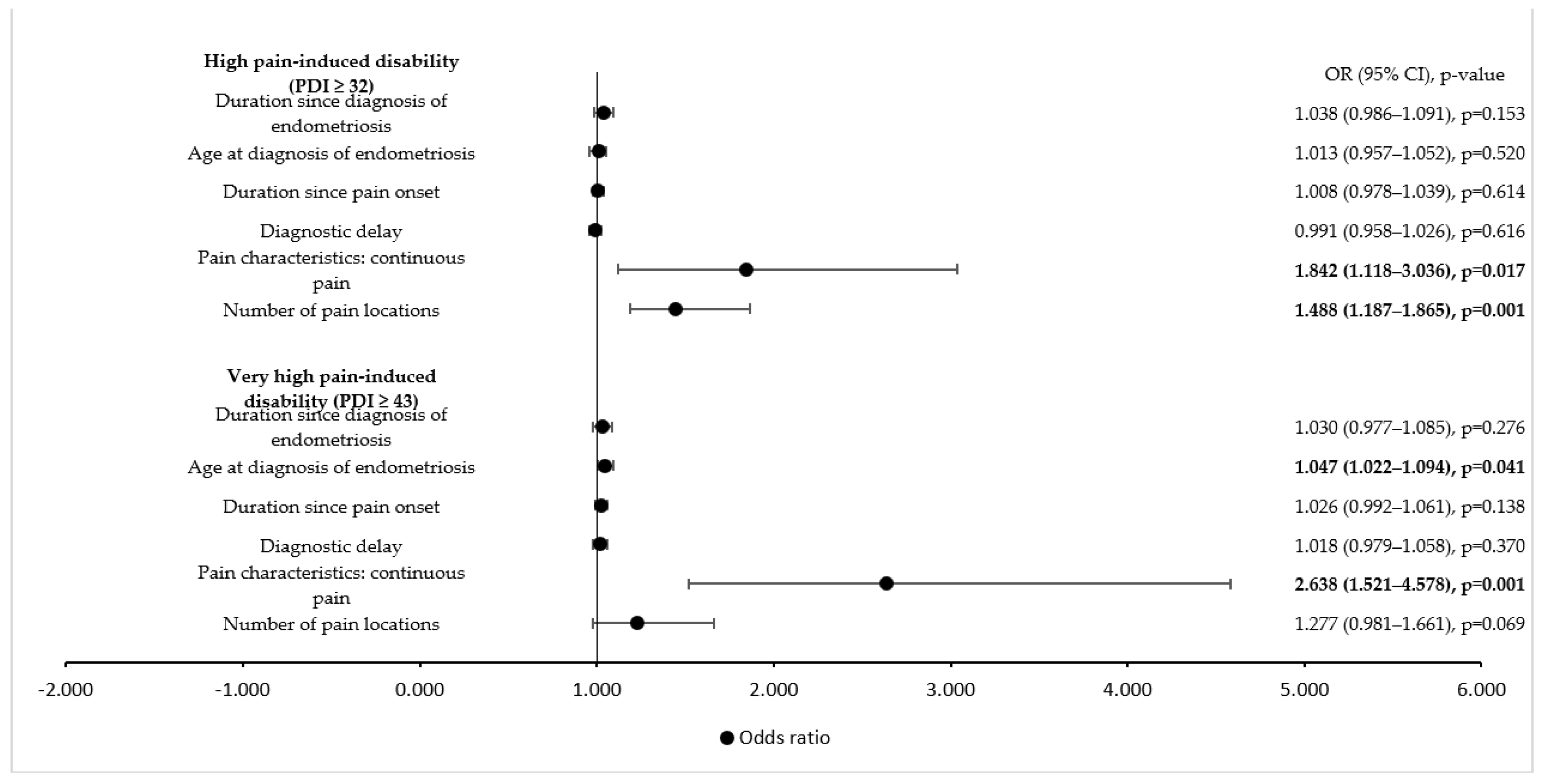
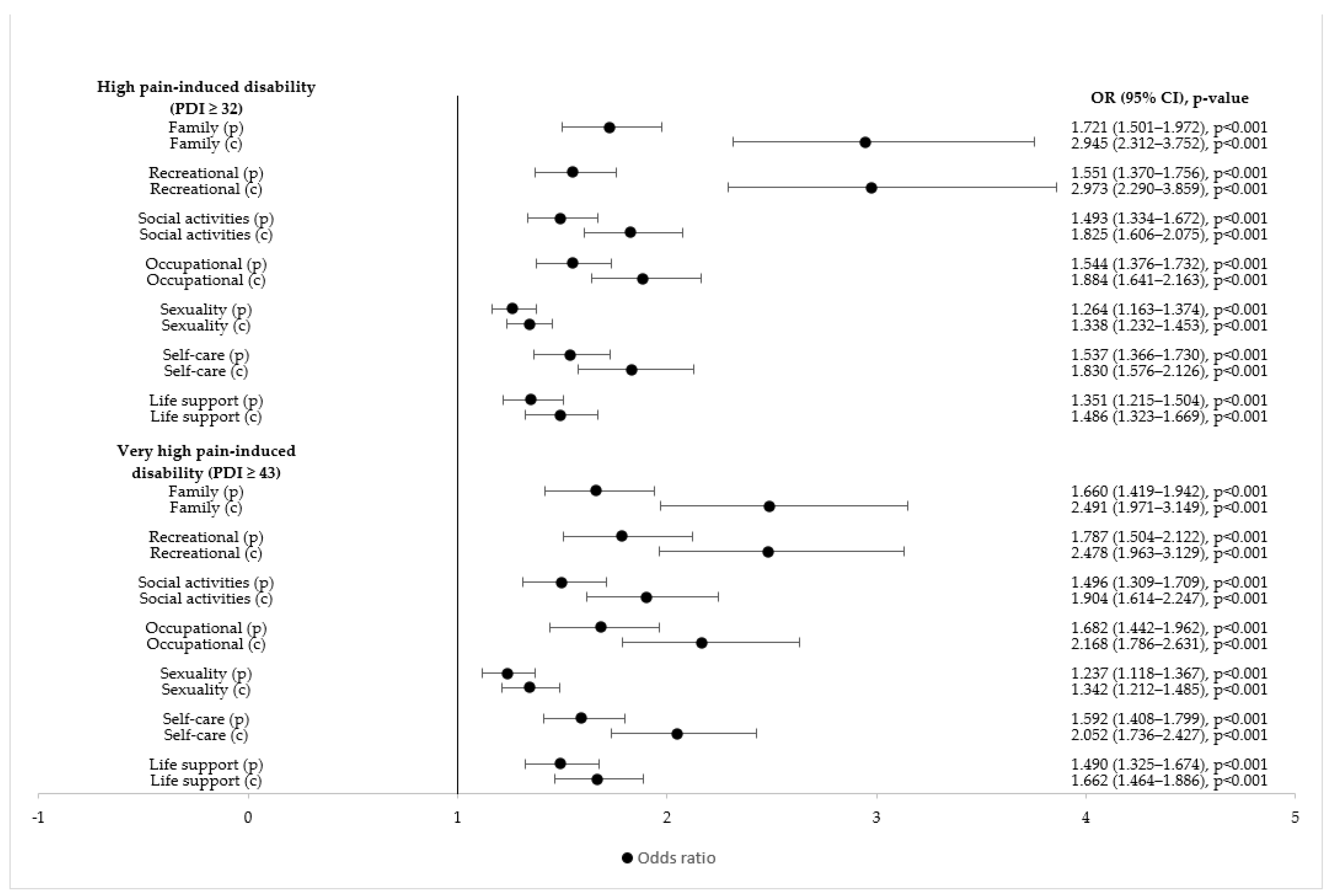
3.3. Identification of Predictors of Pain-Induced Disability
4. Discussion
Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Zondervan, K.T.; Becker, C.M.; Missmer, S.A. Endometriosis. N. Engl. J. Med. 2020, 382, 1244–1256. [Google Scholar] [CrossRef] [PubMed]
- Ruszała, M.; Dłuski, D.F.; Winkler, I.; Kotarski, J.; Rechberger, T.; Gogacz, M. The State of Health and the Quality of Life in Women Suffering from Endometriosis. J. Clin. Med. 2022, 11, 2059. [Google Scholar] [CrossRef] [PubMed]
- Giudice, L. Endometriosis. NEJM 2010, 362, 2389–2398. [Google Scholar] [CrossRef] [PubMed]
- David Adamson, G.; Kennedy, S.; Hummelshoj, L. Creating solutions in endometriosis: Global collaboration through the World Endometriosis Research Foundation. J. Endometr. 2010, 2, 3–6. [Google Scholar] [CrossRef] [Green Version]
- Gambadauro, P.; Carli, V.; Hadlaczky, G. Depressive symptoms among women with endometriosis: A systematic review and meta-analysis. Am. J. Obstet. Gynecol. 2019, 220, 230–241. [Google Scholar] [CrossRef]
- Márki, G.; Bokor, A.; Rigó, J.; Rigó, A. Physical pain and emotion regulation as the main predictive factors of health-related quality of life in women living with endometriosis. Hum. Reprod. 2017, 32, 1432–1438. [Google Scholar] [CrossRef]
- Hudelist, G.; Fritzer, N.; Thomas, A.; Niehues, C.; Oppelt, P.; Haas, D.; Tammaa, A.; Salzer, H. Diagnostic delay for endometriosis in Austria and Germany: Causes and possible consequences. Hum. Reprod. 2012, 27, 3412–3416. [Google Scholar] [CrossRef]
- Gruppo Italiano per lo Studio dell’Endometriosi. Relationship between stage, site and morphological characteristics of pelvic endometriosis and pain. Hum. Reprod. 2001, 16, 2668–2671. [Google Scholar] [CrossRef]
- De Graaff, A.A.; Van Lankveld, J.; Smits, L.J.; Van Beek, J.J.; Dunselman, G.A.J. Dyspareunia and depressive symptoms are associated with impaired sexual functioning in women with endometriosis, whereas sexual functioning in their male partners is not affected. Hum. Reprod. 2016, 31, 2577–2586. [Google Scholar] [CrossRef] [Green Version]
- Dückelmann, A.M.; Taube, E.; Abesadze, E.; Chiantera, V.; Sehouli, J.; Mechsner, S. When and how should peritoneal endometriosis be operated on in order to improve fertility rates and symptoms? The experience and outcomes of nearly 100 cases. Arch. Gynecol. Obstet. 2021, 304, 143–155. [Google Scholar] [CrossRef]
- The Practice Committee of the American Society for Reproductive Medicine. Treatment of pelvic pain associated with endometriosis. Fertil. Steril. 2008, 90, 260–269. [Google Scholar] [CrossRef] [PubMed]
- Treede, R.-D.; Rief, W.; Barke, A.; Aziz, Q.; Bennett, M.I.; Benoliel, R.; Cohen, M.; Evers, S.; Finnerup, N.B.; First, M.B.; et al. Chronic pain as a symptom or a disease: The IASP Classification of Chronic Pain for the International Classification of Diseases (ICD-11) Rolf-Detlef. Pain 2018, 160, 19–27. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schwab, R.; Anić, K.; Stewen, K.; Schmidt, M.W.; Kalb, S.R.; Kottmann, T.; Brenner, W.; Domidian, J.S.; Krajnak, S.; Battista, M.J.; et al. Pain experience and social support of endometriosis patients during the COVID-19 pandemic in Germany—Results of a web-based cross-sectional survey. PLoS ONE 2021, 16, e0256433. [Google Scholar] [CrossRef] [PubMed]
- Bettini, L.; Moore, K. Central Sensitization in Functional Chronic Pain Syndromes: Overview and Clinical Application. Pain Manag. Nurs. 2016, 17, 333–338. [Google Scholar] [CrossRef] [PubMed]
- Fourquet, J.; Baez, L.; Figueroa, M.; Iriarte, I.; Flores, I. Quantification of the impact of endometriosis symptoms on health-related quality of life and work productivity. Fertil. Steril. 2011, 96, 107–112. [Google Scholar] [CrossRef] [Green Version]
- Nnoaham, K.E.; Hummelshoj, L.; Webster, P.; D’Hooghe, T.; De Cicco Nardone, F.; De Cicco Nardone, C.; Jenkinson, C.; Kennedy, S.H.; Zondervan, K.T. Impact of endometriosis on quality of life and work productivity: A multicenter study across ten countries. Fertil. Steril. 2011, 96, 366–373.e8. [Google Scholar] [CrossRef] [Green Version]
- Muharam, R.; Amalia, T.; Pratama, G.; Harzif, A.K.; Agiananda, F.; Maidarti, M.; Azyati, M.; Sumapraja, K.; Winarto, H.; Wiweko, B.; et al. Chronic Pelvic Pain in Women with Endometriosis is Associated with Psychiatric Disorder and Quality of Life Deterioration. Int. J. Women’s Health 2022, 14, 131. [Google Scholar] [CrossRef]
- Facchin, F.; Barbara, G.; Saita, E.; Mosconi, P.; Roberto, A.; Fedele, L.; Vercellini, P. Impact of endometriosis on quality of life and mental health: Pelvic pain makes the difference. J. Psychosom. Obstet. Gynecol. 2015, 36, 135–141. [Google Scholar] [CrossRef]
- Schwab, R.; Stewen, K.; Ost, L.; Kottmann, T.; Theis, S.; Elger, T.; Schmidt, M.W.; Anic, K.; Kalb, S.R.; Brenner, W.; et al. Predictors of Psychological Distress in Women with Endometriosis during the COVID-19 Pandemic. Int. J. Environ. Res. Public Health 2022, 19, 4927. [Google Scholar] [CrossRef]
- Culley, L.; Law, C.; Hudson, N.; Denny, E.; Mitchell, H.; Baumgarten, M.; Raine-Fenning, N. The social and psychological impact of endometriosis on women’s lives: A critical narrative review. Hum. Reprod. Update 2013, 19, 625–639. [Google Scholar] [CrossRef] [Green Version]
- Tanaka, K.; Murata, S.; Nishigami, T.; Mibu, A.; Manfuku, M.; Shinohara, Y.; Tanabe, A.; Ono, R. The central sensitization inventory predict pain-related disability for musculoskeletal disorders in the primary care setting. Eur. J. Pain 2019, 23, 1640–1648. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kregel, J.; Schumacher, C.; Dolphens, M.; Malfliet, A.; Goubert, D.; Lenoir, D.; Cagnie, B.; Meeus, M.; Coppieters, I. Convergent Validity of the Dutch Central Sensitization Inventory: Associations with Psychophysical Pain Measures, Quality of Life, Disability, and Pain Cognitions in Patients with Chronic Spinal Pain. Pain Pract. 2018, 18, 777–787. [Google Scholar] [CrossRef] [PubMed]
- Walankar, P.P.; Panhale, V.P.; Patil, M.M. Psychosocial factors, disability and quality of life in chronic shoulder pain patients with central sensitization. Health Psychol. Res. 2020, 8, 79–83. [Google Scholar] [CrossRef] [PubMed]
- Dams, L.; Van der Gucht, E.; Haenen, V.; Lauwers, M.; De Pauw, S.; Steurs, T.; Devoogdt, N.; Smeets, A.; Bernar, K.; De Vrieze, T.; et al. Biopsychosocial risk factors for pain and pain-related disability 1 year after surgery for breast cancer. Support. Care Cancer 2022, 30, 4465–4475. [Google Scholar] [CrossRef]
- Turk, D.C.; Fillingim, R.B.; Ohrbach, R.; Patel, K.V. Assessment of Psychosocial and Functional Impact of Chronic Pain. J. Pain 2016, 17, T21–T49. [Google Scholar] [CrossRef]
- Pollard, C. Preliminary validity study of the pain disability index. Percept. Mot. Ski. 1984, 59, 974. [Google Scholar] [CrossRef]
- Tait, R.C.; Pollard, C.A.; Margolis, R.B.; Duckro, P.N.; Krause, S.J. The Pain Disability Index: Psychometric and validity data. Arch. Phys. Med. Rehabil. 1987, 68, 438–441. [Google Scholar]
- Evans, S.; Mikocka-Walus, A.; Olive, L.; Seidman, L.C.; Druitt, M.; Payne, L.A. Phenotypes of Women with and Without Endometriosis and Relationship with Functional Pain Disability. Pain Med. 2020, 22, 1511–1521. [Google Scholar] [CrossRef]
- Edwards, R.R. Age differences in the correlates of physical functioning in patients with chronic pain. J. Aging Health 2006, 18, 56–69. [Google Scholar] [CrossRef]
- Elliott, A.M.; Burton, C.D.; Hannaford, P.C. Resilience does matter: Evidence from a 10-year cohort record linkage study. BMJ Open 2014, 4, e003917. [Google Scholar] [CrossRef] [Green Version]
- Sharp, T.J.; Harvey, A.G. Chronic Pain and Posttraumatic Stress Disorder: Mutual Maintenance? Clin. Psychol. Rev. 2001, 21, 857–877. [Google Scholar] [CrossRef]
- Carbone, M.G.; Campo, G.; Papaleo, E.; Marazziti, D.; Maremmani, I. The Importance of a Multi-Disciplinary Approach to the Endometriotic Patients: The Relationship between Endometriosis and Psychic Vulnerability. J. Clin. Med. 2021, 10, 1616. [Google Scholar] [CrossRef] [PubMed]
- Vlaeyen, J.W.S.; Linton, S.J. Fear-avoidance and its consequences in chronic musculoskeletal pain: A state of the art. Pain 2000, 85, 317–332. [Google Scholar] [CrossRef] [Green Version]
- Müller, O.; Neuhann, F.; Razum, O. Epidemiology and control of COVID-19. Dtsch. Med. Wochenschr. 2020, 145, 670–674. [Google Scholar]
- Brooks, S.K.; Webster, R.K.; Smith, L.E.; Woodland, L.; Wessely, S.; Greenberg, N.; Rubin, G.J. The psychological impact of quarantine and how to reduce it: Rapid review of the evidence. Lancet 2020, 395, 912–920. [Google Scholar] [CrossRef] [Green Version]
- Rosielle, K.; Bergwerff, J.; Schreurs, A.M.F.; Knijnenburg, J.; De Bie, B.; Maas, J.W.M.; Nap, A.W.; van Wely, M.; Lambalk, C.B.; Goddijn, M.; et al. The impact of the COVID-19 pandemic on infertility patients and endometriosis patients in the Netherlands. Reprod. Biomed. Online 2021, 43, 747–755. [Google Scholar] [CrossRef]
- Nicolás, I.; Martínez-Zamora, M.Á.; Gracia, M.; Feixas, G.; Rius, M.; Carmona, F. Impact of SARS-COV2 Pandemic on Patients with Endometriosis and Their Health Care. J. Women’s Health 2022, 31, 480–486. [Google Scholar] [CrossRef]
- Ashkenazi, M.S.; Huseby, O.L.; Kroken, G.; Soto-Mota, A.; Pents, M.; Loschiavo, A.; Lewandowska, R.; Tran, G.; Kwiatkowski, S. COVID-19 pandemic and the consequential effect on patients with endometriosis. Hum. Reprod. Open 2022, 2022, hoac013. [Google Scholar] [CrossRef]
- Bäuerle, A.; Teufel, M.; Musche, V.; Weismüller, B.; Kohler, H.; Hetkamp, M.; Dörrie, N.; Schweda, A.; Skoda, E. Increased generalized anxiety, depression and distress during the COVID-19 pandemic: A cross-sectional study in Germany. J Public Health 2020, 42, 672–678. [Google Scholar] [CrossRef]
- Matos, M.; McEwan, K.; Kanovský, M.; Halamová, J.; Steindl, S.R.; Ferreira, N.; Linharelhos, M.; Rijo, D.; Asano, K.; Vilas, S.P.; et al. The role of social connection on the experience of COVID-19 related post-traumatic growth and stress. PLoS ONE 2021, 16, e0261384. [Google Scholar] [CrossRef]
- Killgore, W.D.S.; Cloonen, S.A.; Taylor, E.C.; Dailey, N.S. Loneliness: A Signature Mental Health Concern in the Era of COVID-19. Psychiatry Res. 2020, 290, 113117. [Google Scholar] [CrossRef] [PubMed]
- Verdolini, N.; Amoretti, S.; Montejo, L.; García-Rizo, C.; Hogg, B.; Mezquida, G.; Rabelo-da-Ponte, F.D.; Vallespir, C.; Radua, J.; Martinez-aran, A.; et al. Resilience and mental health during the COVID-19 pandemic. J. Affect Disord. 2021, 283, 156–164. [Google Scholar] [CrossRef] [PubMed]
- Kimhi, S.; Marciano, H.; Eshel, Y.; Adini, B. Resilience and demographic characteristics predicting distress during the COVID-19 crisis. Soc. Sci. Med. 2020, 265, 113389. [Google Scholar] [CrossRef] [PubMed]
- Arena, A.; Orsini, B.; Degli, E.; Raimondo, D.; Lenzi, J. Effects of the SARS-CoV-2 pandemic on women affected by endometriosis: A large cross-sectional online survey. Ann. Med. 2021, 53, 1924–1934. [Google Scholar] [CrossRef]
- Hawker, G.A.; Mian, S.; Kendzerska, T.; French, M. Measures of adult pain: Visual Analog Scale for Pain (VAS Pain), Numeric Rating Scale for Pain (NRS Pain), McGill Pain Questionnaire (MPQ), Short-Form McGill Pain Questionnaire (SF-MPQ), Chronic Pain Grade Scale (CPGS), Short Form-36 Bodily Pain Scale (SF-36 BPS), and Measure of Intermittent and Constant Osteoarthritis Pain (ICOAP). Arthritis Care Res. 2011, 63, S240–S252. [Google Scholar] [CrossRef]
- Tait, R.C.; Chibnall, J.T.; Krause, S. The Pain Disability Index: Psychometric properties. Pain 1990, 40, 171–182. [Google Scholar] [CrossRef]
- Löwe, B.; Wahl, I.; Rose, M.; Spitzer, C.; Glaesmer, H.; Wingenfeld, K.; Schneider, A.; Brähler, E. A 4-item measure of depression and anxiety: Validation and standardization of the Patient Health Questionnaire-4 (PHQ-4) in the general population. J. Affect Disord. 2010, 122, 86–95. [Google Scholar] [CrossRef]
- Furukawa, T.; Kessler, R.; Slade, T.; Andrews, G. The performance of the K6 and K10 screening scales for psychological distress in the Australian National Survey of Mental Health and Well-Being. Psychol. Med. 2003, 33, 357–362. [Google Scholar] [CrossRef]
- Löwe, B.; Kroenke, K.; Gräfe, K. Detecting and monitoring depression with a two-item questionnaire (PHQ-2). J. Psychosom. Res. 2005, 58, 163–171. [Google Scholar] [CrossRef]
- Gilbody, S.; Richards, D.; Brealey, S.; Hewitt, C. Screening for depression in medical settingswith the Patient HealthQuestionnaire (PHQ): A diagnostic meta-analysis. J. Gen. Intern. Med. 2007, 22, 1596–1602. [Google Scholar] [CrossRef] [Green Version]
- Kroenke, K.; Spitzer, R.L.; Williams, J.B.W.; Löwe, B. An Ultra-Brief Screening Scale for Anxiety and Depression: The PHQ–4. Psychosomatics 2009, 50, 613–621. [Google Scholar] [CrossRef] [PubMed]
- Kroenke, K.; Spitzer, R.L.; Williams, J.B.W. The patient health questionnaire-2: Validity of a two-item depression screener. Med. Care 2003, 41, 1284–1292. [Google Scholar] [CrossRef] [PubMed]
- Kroenke, K.; Spitzer, R.L.; Williams, J.B.W.; Monahan, P.O.; Löwe, B. Anxiety Disorders in Primary Care: Prevalence, Impairment, Comorbidity, and Detection. Ann. Intern. Med. 2007, 146, 317–325. [Google Scholar] [CrossRef]
- Smith, B.W.; Dalen, J.; Wiggins, K.; Tooley, E.; Christopher, P.; Bernard, J. The Brief Resilience Scale: Assessing the Ability to Bounce Back. Int. J. Behav. Med. 2008, 15, 194–200. [Google Scholar] [CrossRef]
- Smith, B.W.; Tooley, E.M.; Christopher, P.J.; Kay, V.S. Resilience as the ability to bounce back from stress: A neglected personal resource? J. Posit. Psychol. 2010, 5, 166–176. [Google Scholar] [CrossRef]
- Chmitorz, A.; Wenzel, M.; Stieglitz, R.D.; Kunzler, A.; Bagusat, C.; Helmreich, I.; Gerlicher, A.; Kampa, M.; Kubiak, T.; Kalisch, R.; et al. Population-based validation of a German version of the Brief Resilience Scale. PLoS ONE 2018, 13, e0192761. [Google Scholar] [CrossRef] [Green Version]
- Hawryluck, L.; Gold, W.L.; Robinson, S.; Pogorski, S.; Galea, S.; Styra, R. SARS control and psychological effects of quarantine, Toronto, Canada. Emerg. Infect. Dis. 2004, 10, 1206–1212. [Google Scholar] [CrossRef]
- Bursac, Z.; Gauss, C.H.; Williams, D.K.; Hosmer, D.W. Purposeful selection of variables in logistic regression. Source Code Biol. Med. 2008, 3, 17. [Google Scholar] [CrossRef] [Green Version]
- Bursac, Z.; Gauss, C.; Williams, D.K.; Hosmer, D. A purposeful selection of variables macro for logistic regression. SAS Glob. Forum Proc. 2007, 173, 1–5. [Google Scholar]
- Mewes, R.; Rief, W.; Stenzel, N.; Glaesmer, H.; Martin, A.; Brähler, E. What is “normal” disability? An investigation of disability in the general population. Pain 2009, 142, 36–41. [Google Scholar] [CrossRef]
- Nilges, P.; Deuker, N.; Kirschner, P. Schmerz, Funktionsbehinderung, psychische Beeinträtichtigung und Behandlungsverlauf bei Patienten mit Hüftgelenk-Prothesen. In Bericht über den 38. KongreB der Deutschen Gesellschaft für Psychologie in Trier; Montada, L., Ed.; Gesellschaft für Psychologie: Trier, Germany, 1992; p. 532. [Google Scholar]
- Luka-Krausgrill, U.; Wurmthaler, C.; Becker, T. Die Beziehung zwischen Schmerzbewältigung, Beeinträchtigung und Depression bei chronischem Schmerz. In Psychotherapeutische Medizin bei Chronischem Schmerz; Deutscher Ärzteverlag: Köln, Germany, 1994; p. 157. [Google Scholar]
- Saile, H.; Dieterich, A. Familiäre und schmerzbezogene Merkmale aus der Sicht von chronischen Schmerzpatienten und deren Partnern. Psychother. Psychosom. Med. Psychol. 1992, 42, 273–278. [Google Scholar] [PubMed]
- Saile, H.; Schmitz, U. Zur Oberprüfung des Circumplex-Modells: Familiäre Adaptabilität und Kohäsion bei chronischen Schmerzpatienten. Syst. Fam. 1991, 4, 223–225. [Google Scholar]
- Bień, A.; Rzońca, E.; Zarajczyk, M.; Wilkosz, K.; Wdowiak, A.; Iwanowicz-Palus, G. Quality of life in women with endometriosis: A cross-sectional survey. Qual. Life Res. 2020, 29, 2669–2677. [Google Scholar] [CrossRef] [PubMed]
- Ruokolainen, O.; Auvinen, J.; Linton, S.J.; Herrala, S.; Eskola, P.; Paananen, M.; Korpelainen, R.; Karppinen, J. ÖMPSQ-Short Score and determinants of chronic pain: Cross-sectional results from a middle-aged birth cohort. Eur. J. Phys. Rehabil. Med. 2017, 54, 34–40. [Google Scholar] [CrossRef]
- Kaniasty, K. Social support, interpersonal, and community dynamics following disasters caused by natural hazards. Curr. Opin. Psychol. 2020, 32, 105–109. [Google Scholar] [CrossRef]
- Gloster, A.T.; Lamnisos, D.; Lubenko, J.; Presti, G.; Squatrito, V.; Constantinou, M.; Nicolaou, C.; Papacostas, S.; Aydın, G.; Chong, Y.Y.; et al. Impact of COVID-19 pandemic on mental health: An international study. PLoS ONE 2020, 15, e024480. [Google Scholar] [CrossRef]
- Sturgeon, J.; Zautra, A.J. Social pain and physical pain: Shared paths to resilience. Pain Manag. 2016, 6, 63–74. [Google Scholar] [CrossRef]
- López-Martínez, A.E.; Esteve-Zarazaga, R.; Ramírez-Maestre, C. Perceived Social Support and Coping Responses Are Independent Variables Explaining Pain Adjustment Among Chronic Pain Patients. J. Pain 2008, 9, 373–379. [Google Scholar] [CrossRef]
- Sippel, L.M.; Pietrzak, R.H.; Charney, D.S.; Mayes, L.C.; Southwick, S.M. How does social support enhance resilience in the trauma-exposed individual? Ecol. Soc. 2015, 20, 10. [Google Scholar] [CrossRef]
- Huang, Z.; Wu, S. Acceptance of disability, coping style, perceived social support and quality of life among patients with chronic lymphedema: A cross-sectional study. Support. Care Cancer 2022, 30, 4099–4108. [Google Scholar] [CrossRef]
- Oliveira, V.C.; Ferreira, M.L.; Morso, L.; Albert, H.B.; Refshauge, K.M.; Ferreira, P.H. Patients’ perceived level of social isolation affects the prognosis of low back pain. Eur. J. Pain 2015, 19, 538–545. [Google Scholar] [CrossRef] [PubMed]
- Ortiz-Calvo, E.; Martínez-Alés, G.; Mediavilla, R.; González-Gómez, E.; Fernández-Jiménez, E.; Bravo-Ortiz, M.F.; Moreno-Küstner, B. The role of social support and resilience in the mental health impact of the COVID-19 pandemic among healthcare workers in Spain. J. Psychiatr. Res. 2022, 148, 181–187. [Google Scholar] [CrossRef] [PubMed]
- Hu, J.; Huang, Y.; Liu, J.; Zheng, Z.; Xu, X.; Zhou, Y.; Wang, J. COVID-19 Related Stress and Mental Health Outcomes 1 Year After the Peak of the Pandemic Outbreak in China: The Mediating Effect of Resilience and Social Support. Front. Psychiatry 2022, 13, 828379. [Google Scholar] [CrossRef]
- Hou, T.; Zhang, T.; Cai, W.; Song, X.; Chen, A.; Deng, G.; Ni, C. Social support and mental health among health care workers during Coronavirus Disease 2019 outbreak: A moderated mediation model. PLoS ONE 2020, 15, e0233831. [Google Scholar] [CrossRef] [PubMed]
- Ramírez-Maestre, C.; Esteve, R.; López, A.E. Cognitive appraisal and coping in chronic pain patients. Eur. J. Pain 2008, 12, 749–756. [Google Scholar] [CrossRef]
- Rossi, H.R.; Uimari, O.; Arffman, R.; Vaaramo, E.; Kujanpää, L.; Ala-Mursula, L.; Piltonen, T.T. The association of endometriosis with work ability and work life participation in late forties and lifelong disability retirement up till age 52: A Northern Finland Birth Cohort 1966 study. Acta Obstet. Gynecol. Scand. 2021, 100, 1822–1829. [Google Scholar] [CrossRef]
- Leuenberger, J.; Kohl Schwartz, A.S.; Geraedts, K.; Haeberlin, F.; Eberhard, M.; von Orellie, S.; Imesch, P.; Leeners, B. Living with endometriosis: Comorbid pain disorders, characteristics of pain and relevance for daily life. Eur. J. Pain United Kingd. 2022, 26, 1021–1038. [Google Scholar] [CrossRef]
- Jones, G.; Jenkinson, C.; Kennedy, S. The impact of endometriosis upon quality of life: A qualitative analysis. J. Psychosom. Obstet. Gynecol. 2004, 25, 123–133. [Google Scholar] [CrossRef]
- Moradi, M.; Parker, M.; Sneddon, A.; Lopez, V.; Ellwood, D. Impact of endometriosis on women’s lives: A qualitative study. BMC Womens. Health 2014, 14, 123. [Google Scholar] [CrossRef] [Green Version]
- Gilmour, J.A.; Huntington, A.; Wilson, H.V. The impact of endometriosis on work and social participation. Int. J. Nurs. Pract. 2008, 14, 443–448. [Google Scholar] [CrossRef]
- Miller, L. Neurosensitization: A model for persistent disability in chronic pain, depression, and posttraumatic stress disorder following injury. NeuroRehabilitation 2000, 14, 25–32. [Google Scholar] [CrossRef] [PubMed]
- Soliman, A.M.; Coyne, K.S.; Zaiser, E.; Castelli-Haley, J.; Fuldeore, M.J. The burden of endometriosis symptoms on health-related quality of life in women in the United States: A cross-sectional study. J. Psychosom. Obstet. Gynecol. 2017, 38, 238–248. [Google Scholar] [CrossRef] [PubMed]
- Banks, S.M.; Kerns, R.D. Explaining high rates of depression in chronic pain: A diathesis-stress framework. Psychol. Bull. 1996, 119, 95. [Google Scholar] [CrossRef]
- Orr, N.L.; Wahl, K.J.; Lisonek, M.; Joannou, A.; Noga, H.; Albert, A.; Bedaiwy, M.A.; Williams, C.; Allaire, C.; Yong, P.J. Central sensitization inventory in endometriosis. Pain 2022, 163, E234–E245. [Google Scholar] [CrossRef]
- Woolf, C.J. Central sensitization: Implications for the diagnosis and treatment of pain. Pain 2011, 152, S2–S15. [Google Scholar] [CrossRef]
- Hu, T.; Zhang, D.; Wang, J. A meta-analysis of the trait resilience and mental health. Pers. Individ. Differ. 2015, 76, 18–27. [Google Scholar] [CrossRef]
- Casale, R.; Sarzi-Puttini, P.; Botto, R.; Alciati, A.; Batticciotto, A.; Marotto, D.; Torta, R. Fibromyalgia and the concept of resilience. Clin. Exp. Rheumatol. 2019, 37, 105–113. [Google Scholar]
- Hassett, A.L.; Finan, P.H. The role of resilience in the clinical management of chronic pain. Curr. Pain Headache Rep. 2016, 20, 39. [Google Scholar] [CrossRef]
- Southwick, S.M.; Charney, D.S. The Science of Resilience: Implications for the Prevention and Treatment of Depression. Science 2012, 338, 79–82. [Google Scholar] [CrossRef]
- Sturgeon, J.A.; Zautra, A.J. Resilience: A new paradigm for adaptation to chronic pain. Curr. Pain Headache Rep. 2010, 14, 105–112. [Google Scholar] [CrossRef]
- Greenberg, J.; Mace, R.A.; Bannon, S.M.; Kulich, R.J.; Vranceanu, A.M. Mind-body activity program for chronic pain: Exploring mechanisms of improvement in patient-reported, performance-based and ambulatory physical function. J. Pain Res. 2021, 14, 359. [Google Scholar] [CrossRef] [PubMed]
- Cutter, S.L.; Barnes, L.; Berry, M.; Burton, C.; Evans, E.; Tate, E.; Webb, J. A place-based model for understanding community resilience to natural disasters. Glob. Environ. Chang. 2008, 18, 598–606. [Google Scholar] [CrossRef]
- Mao, W.; Agyapong, V.I.O. The Role of Social Determinants in Mental Health and Resilience After Disasters: Implications for Public Health Policy and Practice. Front. Public Health 2021, 9, 551. [Google Scholar] [CrossRef]
- Lara-Cabrera, M.L.; Betancort, M.; Muñoz-Rubilar, C.A.; Novo, N.; De las Cuevas, C. The Mediating Role of Resilience in the Relationship between Perceived Stress and Mental Health. Int. J. Environ. Res. Public Health 2021, 18, 9762. [Google Scholar] [CrossRef]
- Nelson, P.J.; Tucker, S. Developing an Intervention to Alter Catastrophizing in Persons With Fibromyalgia. Orthop. Nurs. 2006, 25, 205–214. [Google Scholar] [CrossRef] [PubMed]
- Dimitriadis, Z.; Kapreli, E.; Strimpakos, N.; Oldham, J. Do psychological states associate with pain and disability in chronic neck pain patients? J. Back Musculoskelet. Rehabil. 2015, 28, 797–802. [Google Scholar] [CrossRef]
- Badcock, L.J.; Lewis, M.; Hay, E.M.; McCarney, R.; Croft, P.R. Chronic shoulder pain in the community: A syndrome of disability or distress? Ann. Rheum. Dis. 2002, 61, 128–131. [Google Scholar] [CrossRef] [Green Version]
- Major, D.H.; Røe, Y.; Småstuen, M.C.; Windt, D.V.D.; Sandbakk, T.B. Fear of movement and emotional distress as prognostic factors for disability in patients with shoulder pain: A prospective cohort study. BMC Musculoskelet. Disord. 2022, 23, 183. [Google Scholar] [CrossRef]
- Lee, H.; Hübscher, M.; Moseley, G.L.; Kamper, S.J.; Traeger, A.C.; Mansell, G.; Mcauley, J.H. How does pain lead to disability? A systematic review and meta-analysis of mediation studies in people with back and neck pain. Pain 2015, 156, 988–997. [Google Scholar] [CrossRef]
- Varela, A.J.; Van Asselt, K.W. The relationship between psychosocial factors and reported disability: The role of pain self-efficacy. BMC Musculoskelet. Disord. 2022, 23, 21. [Google Scholar] [CrossRef]
- Aziz, Q.; Giamberardino, M.A.; Barke, A.; Korwisi, B.; Baranowski, A.P.; Wesselmann, U.; Rief, W.; Treede, R.D. The IASP classification of chronic pain for ICD-11: Chronic secondary visceral pain. Pain 2019, 160, 69–76. [Google Scholar] [CrossRef] [PubMed]
- Thornton, L.; Batterham, P.J.; Fassnacht, D.B.; Kay-Lambkin, F.; Calear, A.L.; Hunt, S. Recruiting for health, medical or psychosocial research using Facebook: Systematic review. Internet Interv. 2016, 4, 72–81. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nunnink, S.; Meana, M. Remembering the pain: Accuracy of pain recall in endometriosis. J. Psychosom. Obstet. Gynecol. 2007, 28, 201–208. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| M (PDI Level) | SD | n | p-Value | |
|---|---|---|---|---|
| Current study | 31.61 | 15.82 | 277 | n.a. |
| Mewes et al. [60] | 6.9 | 11.1 | 1368 | <0.001 |
| Nilges et al. [61] | 37.03 | 13.73 | 42 | 0.036 |
| Luka-Krausgrill et al. [62] | 31.5 | 15.39 | 154 | 0.944 |
| Saile and Dieterich [63] | 30.5 | 13.9 | 40 | 0.674 |
| Saile and Schmitz [64] | 32.58 | 15.13 | 82 | 0.622 |
| High Pain-Induced Disability (PDI ≥ 32) | Very High Pain-Induced Disability (PDI ≥ 43) | |||
|---|---|---|---|---|
| p-Value | OR (95% CI) | p-Value | OR (95% CI) | |
| Dysmenorrhea prior to i/q | ||||
| VASP | 0.001 | 1.015 (1.006–1.024) | 0.013 | 1.013 (1.003–1.023) |
| VASPM (co: VASPL) | 0.589 | 1.221 (0.591–2.2524) | 0.982 | 1.011 (0.402–2.543) |
| VASCS (co: VASPL) | <0.001 | 3.664 (1.899–7.071) | 0.010 | 2.769 (1.277–6.004) |
| Noncyclic pain prior to i/q | ||||
| VASP | <0.001 | 1.021 (1.011–1.031) | <0.001 | 1.023 (1.012–1.035) |
| VASPM (co: VASPL) | <0.001 | 3.026 (1.713–5.344) | 0.002 | 2.876 (1.455–5.685) |
| VASCS (co: VASPL) | 0.001 | 2.890 (1.505–5.548) | 0.002 | 3.281 (1.548–6.956) |
| Dyspareunia prior to i/q | ||||
| VASP | 0.005 | 1.011 (1.003–1.019) | 0.008 | 1.012 (1.003–1.021) |
| VASPM (co: VASPL) | 0.028 | 1.910 (1.074–3.397) | 1.182 | 1.578 (0.807–3.086) |
| VASCS (co: VASPL) | 0.021 | 2.174 (1.121–4.213) | 0.016 | 2.423 (1.181–4.972) |
| Dysuria prior to i/q | ||||
| VASP | <0.001 | 1.021 (1.011–1.031) | 0.002 | 1.015 (1.006–1.025) |
| VASPM (co: VASPL) | 0.005 | 2.824 (1.378–5.788) | 0.041 | 2.132 (1.030–4.413) |
| VASCS (co: VASPL) | 0.005 | 4.008 (1.529–10.512) | 0.013 | 3.015 (1.265–7.188) |
| Dyschezia prior to i/q | ||||
| VASP | <0.001 | 1.015 (1.007–1.024) | <0.001 | 1.018 (1.009–1.028) |
| VASPM (co: VASPL) | 0.055 | 1.824 (0.988–3.370) | 0.001 | 3.018 (1.543–5.903) |
| VASCS (co: VASPL) | 0.005 | 2.656 (1.348–5.233) | 0.007 | 2.667 (1.305–5.449) |
| Lower back pain prior to i/q | ||||
| VASP | <0.001 | 1.021 (1.012–1.029) | <0.001 | 1.020 (1.011–1.030) |
| VASPM (co: VASPL) | 0.650 | 1.159 (0.613–2.193) | 0.405 | 1.417 (0.625–3.213) |
| VASCS (co: VASPL) | <0.001 | 3.895 (2.176–6.971) | <0.001 | 3.930 (2.006–7.701) |
| Global pain experience prior to i/q | ||||
| VASP | <0.001 | 1.048 (1.030–1.066) | <0.001 | 1.045 (1.025–1.066) |
| VASPM (co: VASPL) | <0.001 | 4.347 (2.370–7.973) | 0.003 | 3.218 (1.498–6.912) |
| VASCS (co: VASPL) | 0.001 | 7.845 (2.376–25.897) | <0.001 | 11.857 (3.802–36.976) |
| Current dysmenorrhea | ||||
| VASC | <0.001 | 1.021 (1.013–1.030) | <0.001 | 1.029 (1.017–1.041) |
| VASCM (co: VASCL) | 0.327 | 1.421 (0.704–2.872) | 0.402 | 1.566 (0.548–4.476) |
| VASCS (co: VASCL) | <0.001 | 5.577 (2.951–10.539) | <0.001 | 7.510 (3.176–17.757) |
| Current noncyclic pain | ||||
| VASC | <0.001 | 1.027 (1.018–1.037) | <0.001 | 1.032 (1.020–1.044) |
| VASCM (co: VASCL) | <0.001 | 2.977 (1.638–5.410) | 0.037 | 2.380 (1.056–5.366) |
| VASCS (co: VASCL) | <0.001 | 7.031 (3.620–13.658) | <0.001 | 9.199 (4.263–19.850) |
| Current dyspareunia | ||||
| VASC | <0.001 | 1.017 (1.009–1.024) | <0.001 | 1.016 (1.007–1.024) |
| VASCM (co: VASCL) | 0.003 | 2.468 (1.348–4.516) | 0.248 | 1.538 (0.741–3.194) |
| VASCS (co: VASCL) | <0.001 | 3.250 (1.703–6.201) | <0.001 | 4.091 (2.049–8.168) |
| Current dysuria | ||||
| VASC | <0.001 | 1.023 (1.014–1.033) | <0.001 | 1.018 (1.009–1.027) |
| VASCM (co: VASCL) | 0.002 | 3.033 (1.507–6.105) | 0.009 | 2.576 (1.264–5.250) |
| VASCS | <0.001 | 4.892 (2.008–11.923) | 0.003 | 3.300 (1.490–7.305) |
| Current dyschezia | ||||
| VASC | <0.001 | 1.025 (1.016–1.034) | <0.001 | 1.027 (1.017–1.037) |
| VASCM (co: VASCL) | <0.001 | 2.911 (1.597–5.306) | <0.001 | 3.474 (1.736–6.952) |
| VASCS (co: VASCL) | <0.001 | 6.262 (2.876–13.634) | <0.001 | 6.645 (3.142–14.056) |
| Current lower back pain | ||||
| VASC | <0.001 | 1.023 (1.015–1.031) | <0.001 | 1.023 (1.013–1.033) |
| VASCM (co: VASCL) | 0.718 | 1.135(0.571–2.257) | 0.652 | 1.240 (0.487–3.156) |
| VASCS (co: VASCL) | <0.001 | 5.862 (3.208–10.713) | <0.001 | 4.909 (2.411–9.997) |
| Current global pain experience | ||||
| VASC | <0.001 | 1.057 (1.040–1.075) | <0.001 | 1.056 (1.036–1.077) |
| VASCM (co: VASCL) | <0.001 | 4.562 (2.507–8.303) | 0.003 | 3.233 (1.495–6.990) |
| VASCS (co: VASCL) | <0.001 | 51.806 (6.685–401.457) | <0.001 | 30.436 (9.433–98.206) |
| High Pain-Induced Disability (PDI ≥ 32) | Very High Pain-Induced Disability (PDI ≥ 43) | |||
|---|---|---|---|---|
| p-Value | OR (95% CI) | p-Value | OR (95% CI) | |
| PHQ-2 cv | <0.001 | 1.754 (1.469–2.094) | <0.001 | 1.525 (1.286–1.810) |
| PHQ-2 ≥ 3 | <0.001 | 5.896 (3.476–10.002) | <0.001 | 4.229 (2.343–7.633) |
| PHQ-2 ≥ 5 | <0.001 | 6.453 (3.098–13.433) | 0.002 | 2.643 (1.433–4.878) |
| GAD-2 cv | <0.001 | 1.413 (1.223–1.633) | <0.001 | 1.319 (1.134–1.535) |
| GAD-2 ≥ 3 | <0.001 | 2.780 (1.696–4.558) | 0.003 | 2.331 (1.335–4.071) |
| GAD-2 ≥ 5 | 0.001 | 2.685 (1.482–4.866) | 0.006 | 2.290 (1.263–4.152) |
| PHQ-4 cv | <0.001 | 1.310 (1.198–1.433) | <0.001 | 1.232 (1.127–1.348) |
| PHQ-4 ≥ 6 | <0.001 | 4.536 (2.702–7.615) | <0.001 | 3.125 (1.777–5.495) |
| PHQ-4 ≥ 9 | <0.001 | 5.813 (2.925–11.554) | <0.001 | 3.550 (1.949–6.465) |
| BRS cv | 0.002 | 0.611 (0.449–0.833) | 0.018 | 0.657 (0.464–0.930) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Schwab, R.; Stewen, K.; Kottmann, T.; Theis, S.; Elger, T.; Hamoud, B.H.; Schmidt, M.W.; Anic, K.; Brenner, W.; Hasenburg, A. Determinants of Pain-Induced Disability in German Women with Endometriosis during the COVID-19 Pandemic. Int. J. Environ. Res. Public Health 2022, 19, 8277. https://doi.org/10.3390/ijerph19148277
Schwab R, Stewen K, Kottmann T, Theis S, Elger T, Hamoud BH, Schmidt MW, Anic K, Brenner W, Hasenburg A. Determinants of Pain-Induced Disability in German Women with Endometriosis during the COVID-19 Pandemic. International Journal of Environmental Research and Public Health. 2022; 19(14):8277. https://doi.org/10.3390/ijerph19148277
Chicago/Turabian StyleSchwab, Roxana, Kathrin Stewen, Tanja Kottmann, Susanne Theis, Tania Elger, Bashar Haj Hamoud, Mona W. Schmidt, Katharina Anic, Walburgis Brenner, and Annette Hasenburg. 2022. "Determinants of Pain-Induced Disability in German Women with Endometriosis during the COVID-19 Pandemic" International Journal of Environmental Research and Public Health 19, no. 14: 8277. https://doi.org/10.3390/ijerph19148277