 Rosina Malagrida1,2*
Rosina Malagrida1,2* Jessica Fernández1Jordi Casabona3,4Jacqueline E. W. Broerse2on behalf of the Sentinel School Network Study Group of Catalonia
Jessica Fernández1Jordi Casabona3,4Jacqueline E. W. Broerse2on behalf of the Sentinel School Network Study Group of Catalonia- 1Living Lab for Health, IrsiCaixa AIDS Research Institute, IGTP, Badalona, Spain
- 2Athena Institute, Vrije Universiteit Amsterdam, Amsterdam, Netherlands
- 3Centre d’Estudis Epidemiològics sobre les Infeccions de Transmissió Sexual i Sida de Catalunya (CEEISCAT), Barcelona, Spain
- 4Centro de Investigación Biomédica en Red de Epidemiología y Salud Pública (CIBERESP), Barcelona, Spain
Objectives: The European Centre for Disease Control (ECDC) COVID-19 guidelines for non-pharmaceutical interventions (NPI) identify safety, hygiene and physical distancing measures to control SARS-Cov-2 transmission in schools. Because their implementation requires complicated changes, the guidelines also include “accompanying measures” of risk communication, health literacy and community engagement. Although these are considered crucial, their implementation is complex. This study aimed to co-define a community partnership that a) identifies systemic barriers and b) designs recommendations on how to implement the NPI to improve SARS-Cov-2 prevention in schools.
Methods: We designed and piloted a System-Oriented Dialogue Model with the participation of 44 teachers and 868 students and their parents from six Spanish schools during 2021. The results were analysed using thematic analysis.
Results: Participants identified 406 items addressing issues related to system characteristics, which is indicative of the complexity of the challenge. Using a thematic analysis, we defined 14 recommendations covering five categories.
Conclusion: These findings could help in developing guidelines for initiating community engagement partnerships in schools to provide more integrated prevention interventions.
Introduction
The European Centre for Disease Prevention and Control (ECDC) stated in 2020 that closing schools to control the COVID-19 pandemic should be done as a last resort due to its negative impact on children’s physical and mental health and education as well as its broader economic impact on society. It therefore developed guidelines for non-pharmaceutical interventions (NPI) aimed at preventing and controlling SARS-Cov-2 transmission in school settings (1, 2). These include safety- and hygiene-related measures—such as using masks, appropriate ventilation and respiratory and hand hygiene; ensuring appropriate facility cleaning and promoting a “stay at home when sick” policy—and physical distancing measures—such as creating cohorts of classes and groups; ensuring physical distancing in the classroom; reducing class sizes; staggering arrival, meal and break times or holding classes outdoors. Schools are advised to adapt the physical distancing measures to the setting and age group and to balance preventing transmission with providing optimal learning and psychosocial environments. The ECDC also recommends that such measures be accompanied by risk communication, health literacy and community engagement, including the voices of the children and other stakeholders. These “accompanying measures” are considered crucial components of an effective response in school settings (1, 2). They are also being promoted by the WHO and UNESCO within an initiative called Health Promoting Schools (3, 4).
Although most of these measures have been implemented with a high degree of effectiveness that has allowed many EU countries to keep schools open for long periods during the pandemic (5), their practical implementation has been complex (6). Challenges include how to find the right balance between preventing transmission and providing children with optimal environments, how to implement the accompanying measures or how to respond to more practical issues such as coping with physical distancing in spaces that do not allow it (1, 2).
These challenges are also complex, and they will require systemic changes in schools (7), such as changes in a) current routines and ways of working, b) rules, policies, guidelines, power structures and distribution of resources and c) mental and cultural models used within a school setting, including norms, values, beliefs, attitudes and expectations. Such changes are often initially overlooked and may subsequently give rise to systemic barriers. This is because systems actively create barriers for interventions that are incompatible with the dominant cultures, structures and practices within them (7). If these systemic barriers are not adequately addressed, the prevention measures cannot be implemented effectively. The ECDC, WHO and UNESCO have therefore suggested a new model for health protection and promotion for use within community partnerships in which different social actors from the education community work together to design and implement effective solutions for the emerging challenges (1–4). However, there are no clear guidelines on how to set up participatory community partnerships while assuring they will lead to the identification and implementation of appropriate (accompanying) measures that consider the systemic barriers. Our research therefore aimed to design and pilot a System-Oriented Dialogue Model for a) identifying the systemic barriers to implementing NPI for SARS-Cov-2 prevention in schools and b) co-designing recommendations on how to address those barriers within community partnerships.
Methods
This research was conducted within the framework of the broader Sentinel Schools Study, which forms part of the Catalonia Ministry of Health’s COVID-19 prevention plan. The broader study aims to monitor and evaluate the COVID-19 pandemic in school settings and to identify barriers and facilitators for improving prevention measures. It is run by a consortium of experts in healthcare and in public health research who were consulted during different phases of the process.
We used a Community-Based Participatory Research (CBPR) approach to co-design the recommendations for setting up community partnerships because both share the same principles: the participation and empowerment of different community members and the relevance and impact of research. In CBPR, research participants from a community are actively involved in the research process and the research is action oriented, which is especially useful when the goal is to achieve real-life change (8). For this project, we also used the Dialogue Model (9), as it describes a structured multistakeholder process for designing action agendas to address a problem. In addition, its principles are also aligned with those of CBPR: active engagement of stakeholders, respect for experiential knowledge and dialogue between stakeholders. The model provides clear prescriptive guidelines on how to consult with various stakeholders and integrate their perspectives, and it has been validated by numerous case studies on a wide range of health issues (10). It comprises the following phases: Exploration, Consultation, Prioritization, Integration, Programming and Implementation. We adapted the model in two ways. First, we swapped the order of the prioritization and integration phases so the priority-setting process would be based on all the results, although this phase and the programming and implementation phases were beyond the scope of our project. We also added a new phase—Dissemination—to follow integration because we considered it essential to validate and discuss the results with participants and then disseminate them to key stakeholders who could contribute to the last three phases of the model. Second, as the Dialogue Model does not explicitly use a systems approach, we included a systems analysis to ensure we could identify the systemic barriers. For this analysis, we applied Van Mierlo et al.’s (11) system analysis tool, which classifies the barriers to system transformation according to the different characteristics of a system. To fit our topic and actors, we added a new characteristic named “health,” renamed “market structure” as “economy” and added information to contextualize each of the characteristics (see Box 1).
BOX 1 | System characteristics to be analysed during the consultation phase (adapted from Van Mierlo et al’s, 2010, system analysis tool). System-Oriented Dialogue Model, Catalonia, Spain, 2021.
“Access to knowledge/information and research development”: education, communication, access to contrasted information, etc.
“Physical and virtual infrastructure”: school, family and leisure spaces, new technologies, etc.
“Legislation, regulation and compliance”: from the government and from the school and social environment, such as handwashing, ventilation, social distancing, etc.
“Roles and interaction and collaboration between different actors”: between teachers, students, families, administration, health sector, social environment, etc.
“Economy”: changes in families’ employment situations, resources to deal with the changes, etc.
“Health”: impact on physical and psycho-social health, agility of response with preventive measures, perception of risk by different social actors, willingness to be vaccinated, etc.
“Values, norms and symbols”: refers to a country’s, region’s or sector’s culture, its social norms and values and its political and economic climates. This characteristic is key because it generates problems and needs within the former system characteristics, which mostly refer to structures, patterns and events (12).
We called this novel methodology the System-Oriented Dialogue Model.
The System-Oriented Dialogue Model was implemented from January to June 2021 with six participating schools from the Sentinel School Network in Catalonia, Spain (including both primary and secondary schools) (see Figure 1). The schools were identified within a school sentinel surveillance network created within the Sentinel Schools Study and were selected considering socio-economic, rural-urban and private-public criteria to ensure a diverse sample. Below, we describe the activities in the different phases.
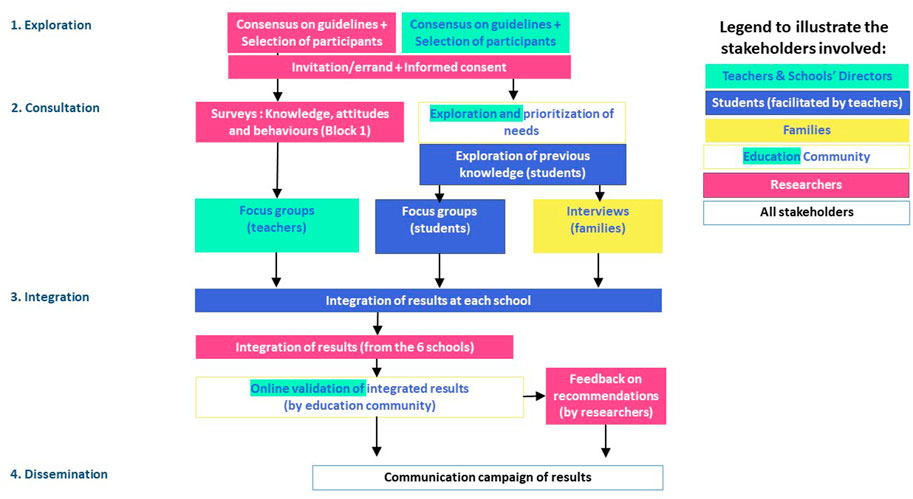
FIGURE 1. System-Oriented Dialogue Model workflow. System-Oriented Dialogue Model, Catalonia, Spain, 2021.
Phase 1: Exploration
In the exploration phase, we operationalized the System-Oriented Dialogue Model by defining guidelines and concrete activities for the different phases to be implemented with teachers, students (aged 10–17 years) and their parents. The guidelines described a) how researchers could engage teachers, students and parents, b) how researchers could conduct focus group discussions (FGDs) with teachers, c) how teachers could conduct FGDs with students, and d) how students could interview their parents. These guidelines also included complementary educational activities to stimulate students’ learning and optimal participation. All guidelines were designed to ensure that the group dynamics promoted collective deliberation.
Once the guidelines were validated by other researchers from the Sentinel Schools Study, we presented the project to schools via online meetings.These were followed by mailings to directors and teachers where they were invited to suggest changes. Their suggestions were used improve the final guidelines. These stakeholders were prioritized during this phase to ensure that the final design fitted their needs and expectations so as to facilitate their involvement in the implementation.
Phase 2: Consultation
This phase started with six online FGDs with teachers, one in each school. A total of 44 teachers from 7 primary and secondary schools participated. Each FGD began with a presentation of the project, its aims and methodology, followed by a presentation on the topic of COVID-19 prevention in schools. The teachers were then invited to follow the steps of the model’s guidelines. The FGDs lasted approximately 120 min.
After the FGDs, the teachers received the guidelines for organizing a consultation process with students and their parents. Of the 44 teachers who attended the online FGDs, 22 conducted FGDs with their students. Those who did not were teachers and school heads with no students in the designated age range for participation, and teachers that were not able to complete the work within the deadlines defined in the guidelines. The participating teachers used communication materials to introduce the project and invite their students to participate. These included a letter of invitation/errand in which researchers from the Sentinel Schools Study asked the students and their parents to participate as co-researchers together with the teachers.
The guidelines for students began with preparatory educational activities inviting students and their parents to familiarize themselves with the subject (e.g., by reading articles on the topic related with the different characteristics of the system analysis). After these preparatory tasks, the teachers conducted FGDs with their students. A total of 868 students participated: 122 in primary education, 648 in lower secondary education and 98 in upper secondary education (Table 1). Subsequently, the students interviewed their parents.
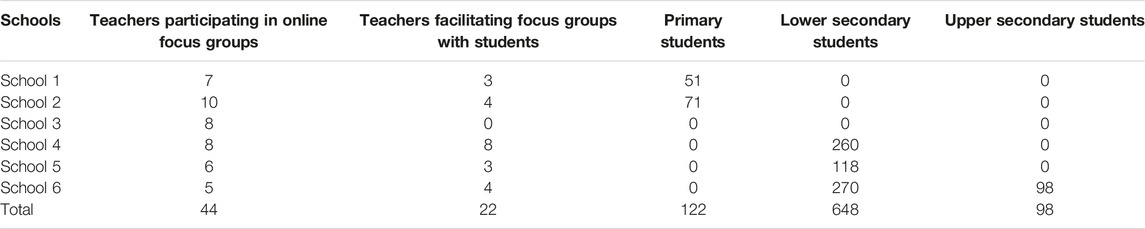
TABLE 1. Distribution of participating students across education levels and of teachers participating in online Focus Groups and facilitating Focus Groups with students. System-Oriented Dialogue Model, Catalonia, Spain, 2021.
Phase 3: Integration
Class specific FGDs and interview results were integrated during a session with each school class. In these teacher-facilitated sessions, the results from the students’ FGDs were integrated with the results from the parents’ interviews and those from the online FGD facilitated by researchers.
The integrated results from each school class were sent to the first two authors of this paper. They checked the submitted tables for completeness by comparing them with the results from the FGDs with teachers; any missing topics were added to the tables. The results from all classes were then integrated into one final preliminary list of problems, needs and recommendations. These were classified into five main categories and then further divided into clusters using a thematic analysis. The preliminary integrated and structured list of recommendations was sent back to the participants for final validation through an online questionnaire. In total, 280 responses were received from 21 teachers, 236 students and 23 parents. These resulted in some minor modifications before a final list of recommendations was obtained. Researchers from the Sentinel Schools consortium also shared feedback on the final recommendations; their comments were added as footnotes to the recommendation list.
We also conducted a frequency count to determine if the participatory system analysis had been effective at identifying key problems and needs in the system characteristics within each category, as these could act as systemic barriers. The frequency analysis is important because the number of characteristics mentioned per category and the weight of each is indicative of each category’s complexity. When there is high complexity, one-off interventions that address problems or needs in isolation (i.e., in one part of a category) are usually not effective enough (12). For this analysis, we calculated the percentage of items per cluster and assigned that percentage to each system characteristic covered by that cluster. Thus, the coverage of each characteristic was weighted against the percentage of items in that cluster compared to the other clusters in the same category. This allowed us to visualize the “weight” that each system characteristic had within each cluster and category.
Finally, a second thematic analysis was conducted and the results were classified into two categories—thematic and process-oriented recommendations—to facilitate moving towards the phases of prioritization, programming and implementation.
Phase 4: Dissemination
Students presented the edited list of recommendations to scientists and policymakers in June 2021 during an online congress attended by 241 students, 16 teachers, 15 researchers and healthcare providers and 3 policymakers. During the congress, the experts shared their views, based on scientific evidence, and added comments to the final list of recommendations, as described in Phase 3. The results were also disseminated to policymakers and to the education community through other channels.
As no personal data was collected for the study, no ethics approval or specific consent procedures were required.
Results
The items identified with the System-Oriented Dialogue Model were distributed into categories and clusters of problems, needs and recommendations using the thematic analysis. In this section, we first describe those problems and needs within each category that act as systemic barriers to the implementation of prevention measures and should therefore be addressed through accompanying measures. Then we present the analysis of how the items were distributed across the system characteristics. We finish by describing the clusters of priority recommendations within each category that should be addressed as accompanying recommendations. All the problem and needs, clusters, recommendations and recommendation clusters are presented in Supplementary File S1.
Identified Problems and Needs
A total of 406 items describing the problems and needs were collected and distributed into 40 clusters and 5 categories using thematic analysis (see Table 2). Brief descriptions of the categories are provided here.
1. Participation of the education community and other stakeholders: comprises problems related to transitioning towards a more open and inclusive model of governance of the pandemic and of research and innovation (R&I). The cluster with the most items (37) corresponds to the “Lack of participation in decision-making at political level and within schools and other environments to adapt regulations to each context, to promote co-responsibility and to reach consensus on the needs for R&I.”
2. Physical, mental and social health: includes problems and needs related to mental and social health (e.g., social relationships, loneliness) and to physical health (e.g., the pandemic’s impact on physical exercise, weight gain and obesity, skin condition, breathing and vocal cords). The main cluster (with 29 items) corresponds to the “Impact of COVID-19 on mental health,” followed by clusters on the “Inconveniences of using masks on communication, hygiene, breathing, pressure on ears and vocal cords, etc., for the different stakeholders” (18 items) and the “Impact of COVID-19 on social health of students outside school” (16 items).
3. Infrastructures and waste management: includes problems and needs in implementing ventilation and social distancing measures and problems involving the waste generated by control measures (e.g., masks and self-tests). The main cluster (12 items) corresponds to “Difficulties with effective implementation of ventilation measures”: for example, how to adapt those measures when it is noisy or cold outside or when the number of students per class is higher than recommended.
4. Communication and education for prevention: comprises problems and needs related to fragmented communication and education campaigns and to education models. It includes the need to better address pandemic-related competencies within formal and non-formal education, such as the ability to discern between evidence-based and non-evidence-based information or to increase citizenship responsibility. The main cluster (32 items) corresponds to “Ineffective communication: confusing, too focused on risks, contributing to stigma of certain age groups, non-transparent, non-evidence-based, overloading, inaccessible to certain groups.” This was followed by “Online classes are least effective and cause more fatigue” (31 items), which focused mostly on problems concerning the model of education, and the “Lack of awareness of the pandemic’s consequences to realize the importance of complying with regulations” (29 items).
5. Social inequalities: comprises problems and needs related to social and digital inequalities. The main cluster (35 items) corresponds to the “Impact of COVID-19 on social inequalities,” followed by the “Impact of digital divide during COVID-19” (29 items).
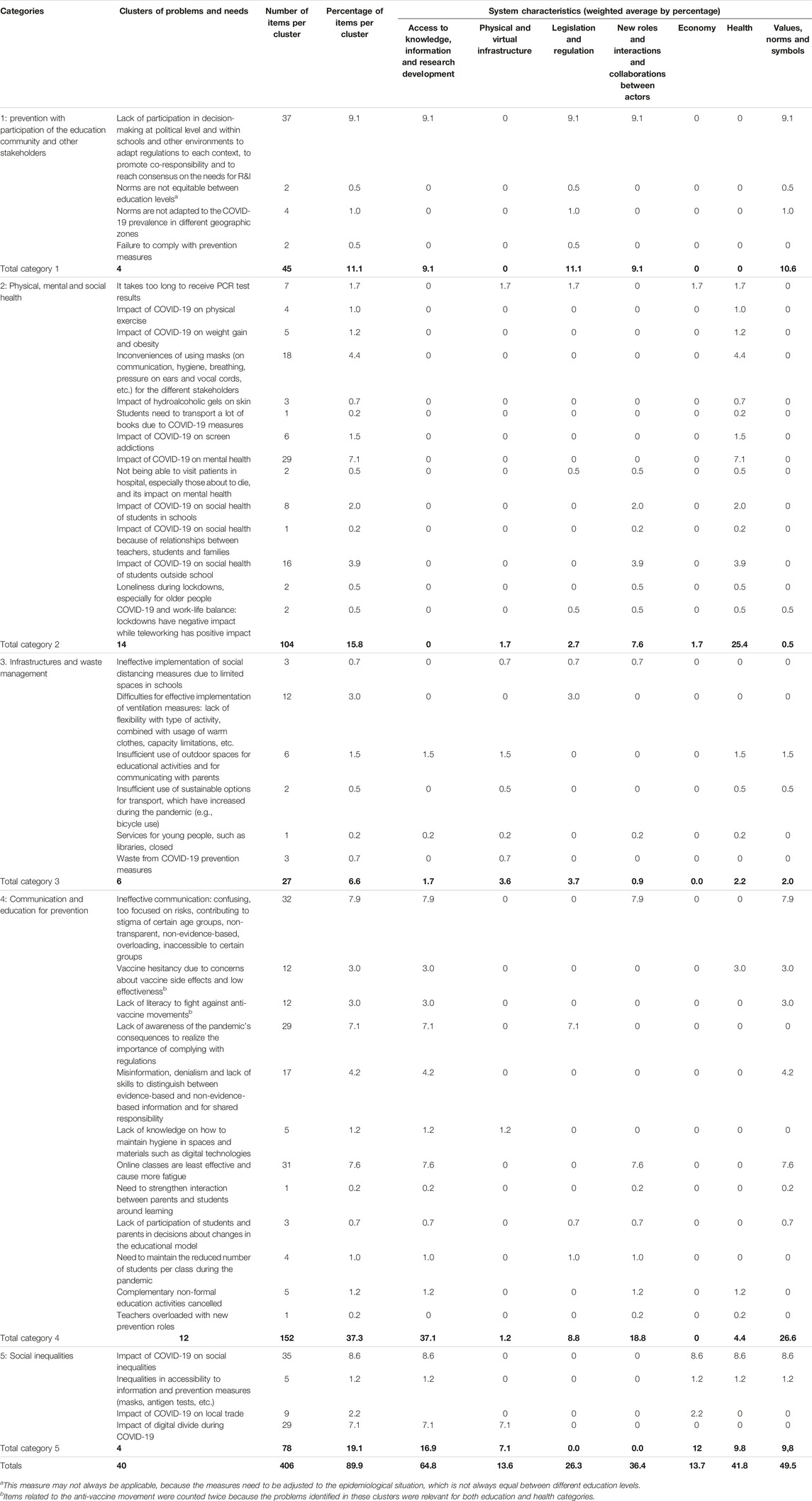
TABLE 2. Problems and needs categories and clusters, including the number and percentage of items per cluster and the weight of individual system characteristics within each cluster and category. System-Oriented Dialogue Model, Catalonia, Spain, 2021.
The categories in which participants identified the most issues were “Communication and education” (152 items) and “Physical, mental and social health” (104 items). The other categories ranked from “Social inequalities” (78 items) to “Participation of the education community and other stakeholders” (45 items) to “Infrastructures and waste management” (27 items).
The identified problems and needs covered the range of system characteristics. All categories had items in more than four characteristics, thus showing a relatively high complexity in every category (see Figure 2). Figure 2 also shows that the same system characteristics are key in several categories and they are therefore cross-cutting. For instance, in the category “Physical, mental and social health,” the cluster on the “Impact of COVID-19 on social health of students outside schools” has 16 items involving the system characteristic of “New roles and interactions and collaborations between actors.” This system characteristic is also important in the categories “Communication and education for prevention” and “Participation with the education community and other stakeholders.”
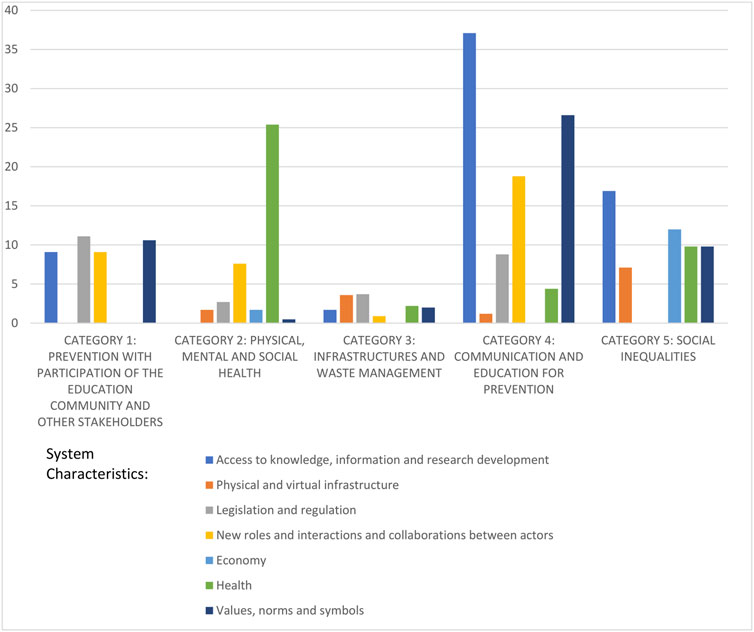
FIGURE 2. Weighted average by percentage of items in each system characteristic within each category. System-Oriented Dialogue Model, Catalonia, Spain, 2021.
The key characteristic “Values, norms and symbols” is present in all categories, although it was most prominent in the following clusters of Categories 1, 4 and 5.
• “Lack of participation in decision-making at political level and within schools and other environments to adapt regulations to each context, to promote co-responsibility and to reach consensus on the needs for R&I,” with norms regarding decision-making capacity—the administration’s versus the citizens’ role in decision making—and fragmented versus collaborative governance models among different system characteristics (9.1% weight in Category 1).
• “Ineffective communication: confusing, too focused on risks, contributing to stigma of certain age groups, non-transparent, non-evidence-based, overloading, inaccessible to certain groups,” with values and norms regarding the lack of critical analysis of information or to stigmas against certain age groups for not following the rules (7.9% weight in Category 4). “Online classes are less effective and cause more fatigue,” with norms regarding the education model being teacher-centred versus cooperative learning (7.6% weight in the same category).
• “Impact of COVID-19 on social inequalities,” with norms regarding fairness and social justice (8.6% weight in Category 5).
Recommendations
The first thematic analysis resulted in 47 recommendations. During the second thematic analysis, this was reduced to 8 thematic and 6 process-oriented final clusters of recommendations for the accompanying measures schools are supposed to address for more integrated prevention interventions (see Table 3).
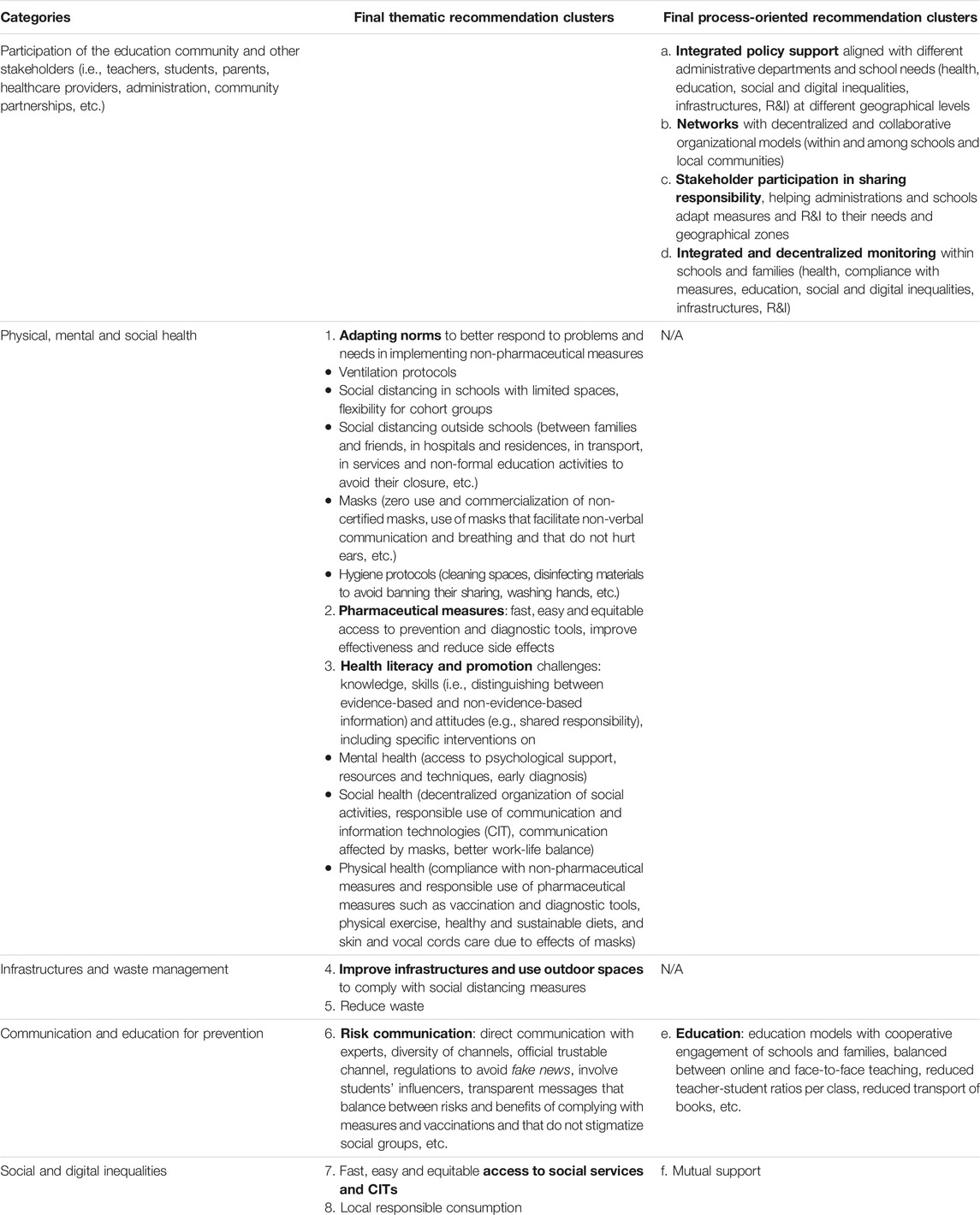
TABLE 3. Categories and final recommendation clusters for accompanying measures, including thematic and process-oriented clusters. System-Oriented Dialogue Model, Catalonia, Spain, 2021.
Discussion
This study developed a System-Oriented Dialogue Model for designing future community partnerships that will facilitate participation while taking into account the systemic barriers for COVID-19 prevention in schools. The model, which is based on a structured participatory action-oriented process, includes a systems analysis to a) identify the key problems and (systemic) barriers that should be addressed and b) formulate recommendations for accompanying measures in order to achieve more integrated COVID-19 prevention that deals with the different system characteristics.
The problems and needs identified within each system characteristic illustrate the complexity of COVID-19 prevention. We classified the problems into five categories. Most issues fell into the “Communication and education” category, followed by the “Physical, mental and social health” and “Social inequalities” categories. Each category has a high degree of complexity, as evidenced by their having items related to at least four system characteristics. This complexity may explain why the categories of problems identified in our study have been persistent over a long period of time (13). These multifaceted and enduring—hence “wicked”—problems will require integrated interventions with coordinated approaches within and among all the categories. Single or multiple one-off interventions aimed at addressing problems in only one or some of these categories will simply not be effective enough (12).
Integrated interventions should consider the recommendations for each system barrier, including both the easily observable factors, such as “the lack of adapting NPI to each school reality,” and the less obvious ones, such as “values, norms and symbols” (e.g., norms regarding the education community’s role in the administration’s decision making processes). According to David Peter Stroh (14), the less obvious elements are key systemic factors that influence the more tangible elements.
Our study’s results also give insight into how schools can implement other international policy standards, such as those suggested by the WHO and UNESCO in “Global Standards and Indicators for Health Promoting Schools” (HPS) (3, 4).
Our System-Oriented Dialogue Model—a combination of the Dialogue Model and a systems analysis method—has been shown to be an effective methodology for including and integrating the experiential knowledge of teachers, students and their parents and for dealing with the complexity within the different problems and needs. To move towards the subsequent phases of our model that were not included in this study (i.e., prioritization, programming and implementation), we suggest that the community partnership should engage an even wider diversity of stakeholders at local and regional levels, including STEAM professionals in private and public organizations, policymakers, civil society organizations and the wider community with expertise in COVID-19 prevention and in the five problem categories. Stakeholders should be organized into different innovation or mission teams, each based on one of the final thematic recommendation clusters and all follow the final process-oriented recommendation clusters. The management structure should be defined with participatory methodologies. For the more complex clusters, such as the promotion of mental health, physical exercise or healthy and sustainable diets, stakeholders should conduct a new iteration of the System-Oriented Dialogue Model to deepen the system analysis and to validate the recommendations through broader collective transformation knowledge. The final output of this new iteration could be Research, Innovation and Action (RIA) plans with collaborative and decentralized approaches for implementing the most complex recommendations. Finally, the innovation teams could implement the resulting RIA plans with all stakeholders participating. However, further research is needed to explore how to improve: a) the system analysis to better consider the interactions between the different items and stakeholders, b) the involvement of the students and their parents in the different phases of the research process and c) the motivation of the participants for instances by introducing a theory of change. Further research involving more schools, both in our context and beyond, is also needed to validate our results, as some specificities may arise.
Policy Implications
Our results show the urgent need to establish community partnerships, as suggested by the ECDC, UNESCO and WHO, to adapt and implement integrated interventions that act simultaneously in the different categories.
However, implementing engagement processes such as our System-Oriented Dialogue Model is not straightforward. We therefore recommend that schools are provided clear guidelines for all the phases of our model, including those not addressed in this study. These should include participatory ideation processes that use system innovation methodologies for the programming and implementation phases (11, 12, 14, 15). The guidelines should be supported with training packages to enable schools to engage their students and key stakeholders in implementing recommendations as integrated interventions using collaborative and decentralized approaches. To ensure that schools dedicate efforts to implementing these guidelines, they must be designed with participatory approaches that not only improve health protection and promotion but also the learning of science (16). The Open Schooling movement has demonstrated that one key to improving science learning is promoting learning activities in which students collaborate with scientists, families and other stakeholders to contribute to solving social challenges through research. The guidelines should therefore be designed following these principles, and they should be adjustable and adaptable to local needs. This means they should be based on participatory research approaches. Besides contributing to learning and implementation, such approaches would allow the education community to participate in the necessary research to deal with the complexities within each category. The interaction between schools and scientists would also help the scientific community to better adapt their research to the needs and expectations of schools, which is a key policy priority of many governmental organizations willing to increase the impact of research (16–19).
The scientific community could act as a facilitator by a) supporting the use of system-oriented participatory research approaches and b) using such approaches to monitor the process, the knowledge generated and the learning and changes within each category. This would enable reflexivity and help participants deal with uncertainties and conflicts while challenging current practices and related institutions (20). At the same time, it would allow the integration and management of research data at different levels: class, school, local, regional.
Implementations should be supported by national and regional policies or strategies “that recognise Health Promoting Schools as key vehicles to achieve national development goals through education and provide a framework for nation-wide promotion of these schools” (3, 4). They should also be coordinated with key international policies in other fields, such as those of the ECDC (2), Open Schooling (21, 22) and organizations willing to increase the impact of research (18). This requires “dedicated resources for true partnerships” (2).
Conclusion
The current model of health protection and promotion in schools needs to use more systemic and collaborative approaches that could be designed with the System-Oriented Dialogue Model described here. This model been useful in designing strategies that community partnerships can use to implement NPI for COVID-19 prevention, including the ECDC’s “accompanying measures.” As we discussed, our results are aligned with international policy standards for Health Promoting Schools and Open Schooling. However, for effective and sustainable implementation, coordinated policy support is required at different geographical levels with dedicated resources to achieve evidence-based impacts on both health promotion and education.
Ethics Statement
This study was approved on 17 December 2020 by the Ethical Committee of the Foundation University Institute for Research in Primary Health Care Jordi Gol i Gurina (IDIAPJGol) (code 20/192-PCV). Written informed consent from the participants' legal guardian/next of kin was not required to participate in this study in accordance with the national legislation and the institutional requirements.
Author Contributions
RM has substantially contributed to the design of the work and the writing of the manuscript. RM and JF have contributed to the acquisition, analysis and interpretation of data. JC has significantly contributed to data acquisition. JB has contributed to supervise all the process and has significantly contributed to the revision of the paper. All have given final approval of the version to be published.
Group Members of the Sentinel School Network Study Group of Catalonia
Principal investigators: Jordi Casabona [Centre d’Estudis Epidemiològics sobre les Infeccions de Transmissió Sexual i Sida de Catalunya (CEEISCAT)-CIBERESP], Josep Basora (Institut Universitari d'Investigació en Atenció Primària (IDIAP Jordi Gol). Project manager: Anna Bordas (CEEISCAT). Technical committee: Jordi Casabona (CEEISCAT), Jordi Sunyer (ISGlobal), Antoni Soriano (Hospital Universitari Vall d’Hebron), Rosina Malagrida (Living lab for Health, IRSICaixa) as Work Package coordinators. Cinta Folch, Pol Romano, Cristina Sánchez, Esteve Muntada, Anna Bordas, Andreu Colom-Cadena i Jordi Casabona (CEEISCAT), Mireia Gascón, Maria Subirana, Jordi Sunyer (ISGlobal), Rosina Malagrida, Jessica Fernández (Living lab for Health at IrsiCaixa), Antoni Soriano (Hospital Universitari Vall d’Hebron). Microbiology laboratories: Tomàs Pumarola, Andrés Antón, Cristina Andrés, Juliana Esperalba, Albert Blanco (Hospital Universitari Vall d’Hebron), Ignacio Blanco, Pere-Joan Cardona, Maria Victoria González, Gema Fernández, Cristina Esteban (Hospital Universitari Germans Trias i Pujol) Data Management and statistical analysis: Yesika Díaz, Lucia Alonso, Jordi Aceiton, Marcos Montoro (CEEISCAT). Data Protection Officer and Technical Support: Esteve Muntada (CEEISCAT). Communication manager: Pol Romano, Cristina Sánchez (CEEISCAT). Field team: Maria Subirana (ISGlobal), Jessica Fernández (Living Lab for Health, IRSICaixa), Andreu Colom-Cadena, Isabel Martínez, Marina Herrero, Alba García, Juan Rus, Paula Ribas, Alba Blanco (CEEISCAT). Community Paediatricians: Esperança Macià i Silvia Burgaya (CAP Manlleu), Ma Teresa Riera-Bosch, Elisabet Sola (EAP Vic Nord), Lidia Aulet, Maria Mendoza, Lidia Busquets (EAP Vic Sud), Xavier Perramon, Júlia Sebastià (EAP Eixample Dret), Ana Moreno (Cap Ripollet), Xavier Duran, Belen Pérez (EAP Can Gibert del Pla), Anna Gatell (Equip Territorial de Pediatria Alt Penedès), Maria Coma (Hospital Universitari Joan XXIII). Epidemiology suveillance services: Marc Olivella, Irene Barrabeig, Ignacio Parro’n, Mònica Carol, Núria Bes, Pere Godoy, Sofia Minguell, Maria Rosa Sala.
Funding
This work received funding from the CONNECT project, funded by the EU’s Horizon 2020 research and innovation programme under grant agreement no. 872814. It also received support from the Sentinel School Network Study Group of Catalonia, coordinated by CEEISCAT, led by the Ministers of Health and Education (Generalitat de Catalunya) and funded by the CERCA Programme/Generalitat de Catalunya, Spain (grant number 2017 SGR 252).
Conflict of Interest
The authors declare that they do not have any conflicts of interest.
Acknowledgments
A special acknowledgement goes to the partners of the projects CONNECT and Sentinel School Network Study Group of Catalonia and especially to Antonio Soriano from the Hospital Universitari Vall d’Hebron and to the ISGlobal research group led by Jordi Sunyer for their valuable contribution of scientific perspectives on the recommendations. The authors also acknowledge the project participants from all the schools for their contributions to the ideas underpinning this paper. The opinions expressed in this article do not reflect those of the EC, which is not responsible for how the information in this article is used.
Supplementary Material
The Supplementary Material for this article can be found online at: https://www.ssph-journal.org/articles/10.3389/ijph.2023.1605624/full#supplementary-material
References
1.European Centre for Disease Prevention and Control. COVID-19 in Children and the Role of School Settings in COVID-19 Transmission. Stockholm: Ecdc (2020).
2.European Centre for Disease Control. COVID-19 in Children and the Role of School Settings in COVID-19 Transmission-Second Update. Stockholm: Ecdc (2021).
3. Sawyer, SM, Raniti, M, and Aston, R. Making Every School a Health-Promoting School, 5. The Lancet Child and Adolescent Health (2021).
4. World Health Organization, . Global Standards for Health Promoting Schools. Available at: https://cdn.who.int/media/docs/default-source/health-promoting-schools/global-standards-for-health-promoting-schools-who-unesco.pdf (Accessed November 24, 2022) (2018).
5. Katerina, V, Aslanoglou, K, Hilton-Boon, M, Phalkey, R, Leonardi-Bee, J, Magiorkinis, G, et al. Effectiveness of Non-pharmaceutical Measures (NPIs) on COVID-19 in Europe: A Systematic Literature Review (2021). Vol. NA, NA.
6. Krishnaratne, S, Pfadenhauer, LM, Coenen, M, Geffert, K, Jung-Sievers, C, Klinger, C, et al. Measures Implemented in the School Setting to Contain the COVID-19 Pandemic: A Scoping Review. Cochrane Database Syst Rev (2020) 12(12):CD013812. doi:10.1002/14651858.CD013812
7. Schuitmaker, TJ, and Haar-van Twillert, Eter. Unraveling Persistent Problems through Analyzing Innovative Practices in Healthcare. In: Toward Sustainable Transitions in Healthcare Systems (2017).
8. Israel, BA, Schulz, AJ, Parker, EA, and Becker, AB. Review of Community-Based Research: Assessing Partnership Approaches to Improve Public Health, 19. Annual Review of Public Health (1998).
9. Abma, TA, and Broerse, JEW. Patient Participation as Dialogue: Setting Research Agendas. Health Expectations (2010).
10. Schölvinck, AFM, Pittens, CACM, and Broerse, JEW. Patient Involvement in Agenda-Setting Processes in Health Research Policy: A Boundary Work Perspective. Sci Public Pol (2020) 47(2):246–55. doi:10.1093/scipol/scaa001
11. van Mierlo, B, Regeer, B, van Amstel, M, Arkesteijn, M, Beekman, V, Bunders, J, et al. Reflexive Monitoring in Action: A Guide for Monitoring System Innovation Projects. In: Wageningen/Amsterdam: Communication and Innovation Studies, WUR. VU: Athena Institute (2010).
12. Stroh, DP. In: J Praded, editor. Systems Thinking for Social Change. Vermont: Chelsea Green Publishing (2015).
13. Klasche, B. After COVID-19: What Can We Learn about Wicked Problem Governance? Social Sci Humanities Open (2021) 4(1):100173. doi:10.1016/j.ssaho.2021.100173
14. Meadows, DH. Places to Intervene in a System (In Increasing Order of Effectiveness). Whole Earth (1997)(91).
16. Malagrida, R, Klaassen, P, Ruiz-Mallén, I, and Broerse, JEW. Towards Competencies and Methods to Support Responsible Research and Innovation within STEAM Secondary Education–The Case of Spain. Research in Science and Technological Education (2022).
17. von Schomberg, R. Prospects for Technology Assessment in a Framework of Responsible Research and Innovation. SSRN (2014).
18. Owen, R, Macnaghten, P, and Stilgoe, J. Responsible Research and Innovation: From Science in Society to Science for Society, with Society. Sci Public Pol (2012).
19. Stilgoe, J, Owen, R, and Macnaghten, P. Developing a Framework for Responsible Innovation. Res Pol (2013).
20. van Mierlo, B, Arkesteijn, M, and Leeuwis, C. Enhancing the Reflexivity of System Innovation Projects with System Analyses. Am J Eval (2010) 31(2):143–61. doi:10.1177/1098214010366046
21. Okada, A, and Sherborne, T. Equipping the Next Generation for Responsible Research and Innovation with Open Educational Resources, Open Courses, Open Communities and Open Schooling: An Impact Case Study in Brazil. J Interactive Media Educ (2018) 2018(1):1–15. [Internet]. doi:10.5334/jime.482
Keywords: COVID-19 prevention, system analysis, community-based participatory research (CBPR), integrated intervention, community partnership, engagement
Citation: Malagrida R, Fernández J, Casabona J and Broerse JEW (2023) A System-Oriented Dialogue Model to Design Community Partnerships for More Effective Sars-Cov-2 Prevention in Schools: The Case of Spain. Int J Public Health 68:1605624. doi: 10.3389/ijph.2023.1605624
Received: 24 November 2022; Accepted: 02 March 2023;
Published: 02 May 2023.
Edited by:
Erica Di Ruggiero, University of Toronto, CanadaReviewed by:
Margaret Haworth-Brockman, Max Rady College of Medicine, University of Manitoba, CanadaCopyright © 2023 Malagrida, Fernández, Casabona and Broerse. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Rosina Malagrida, rmalagrida@irsicaixa.es