
Behavioral Economics in the Epidemiology of the COVID-19 Pandemic: Theory and Simulations


Abstract
:1. Introduction
2. Materials and Methods
2.1. SEIR Model, Game Theory, and Behavioral Economics
- 1.
- A SEIR-type epidemiological model that, in particular, considers asymptomatic transmission for the case of COVID-19.
- 2.
- A game-theoretical component in which individuals choose their level of responsible behavior (and thus the probability of contagion).
- 3.
- Mechanisms from behavioral economics, considering that individuals’ perceptions and beliefs might be biased, especially as applied to COVID-19 [1,2,7,8,19]. In particular, we consider the following channels (we provide additional details about these channels in Online Appendix D).
- (a)
- Optimism bias and overconfidence, by which people tend to be excessively optimistic about future events and excessively confident in their own beliefs and skills to face those events [20].
- (b)
- Availability heuristic, in which the probability of an unknown event (a severe pandemic COVID-19) is estimated using the probability of a known event (a severe pandemic of seasonal influenza).
- (c)
- Fallacy of lack of evidence, whereby an absence of evidence for an event is interpreted as evidence for the absence of that event [21].
- (d)
- Status quo bias, by which people tend to prefer the current baseline (or status quo) over any change in such a way that there is a risk of doing nothing in the face of such a novel event as the pandemic [22].
- (e)
- Social influences have been extensively studied as a critical element in their effect on people’s choices and behaviors [23], especially on health-related outcomes.
2.2. Calibration
3. Theory
3.1. SEAIRD Baseline Model
3.2. Individual Behavior
Solving the Baseline Model with No Lockdown
3.3. Lockdown
4. Results
4.1. Theoretical Results
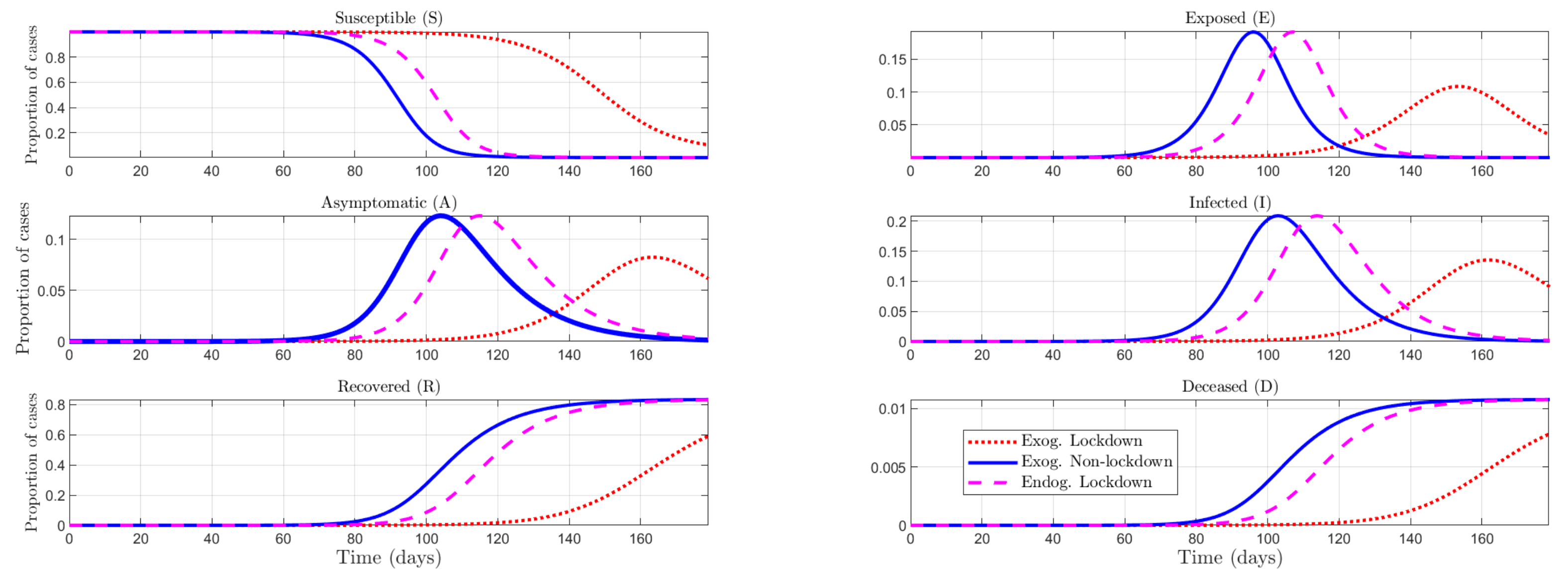
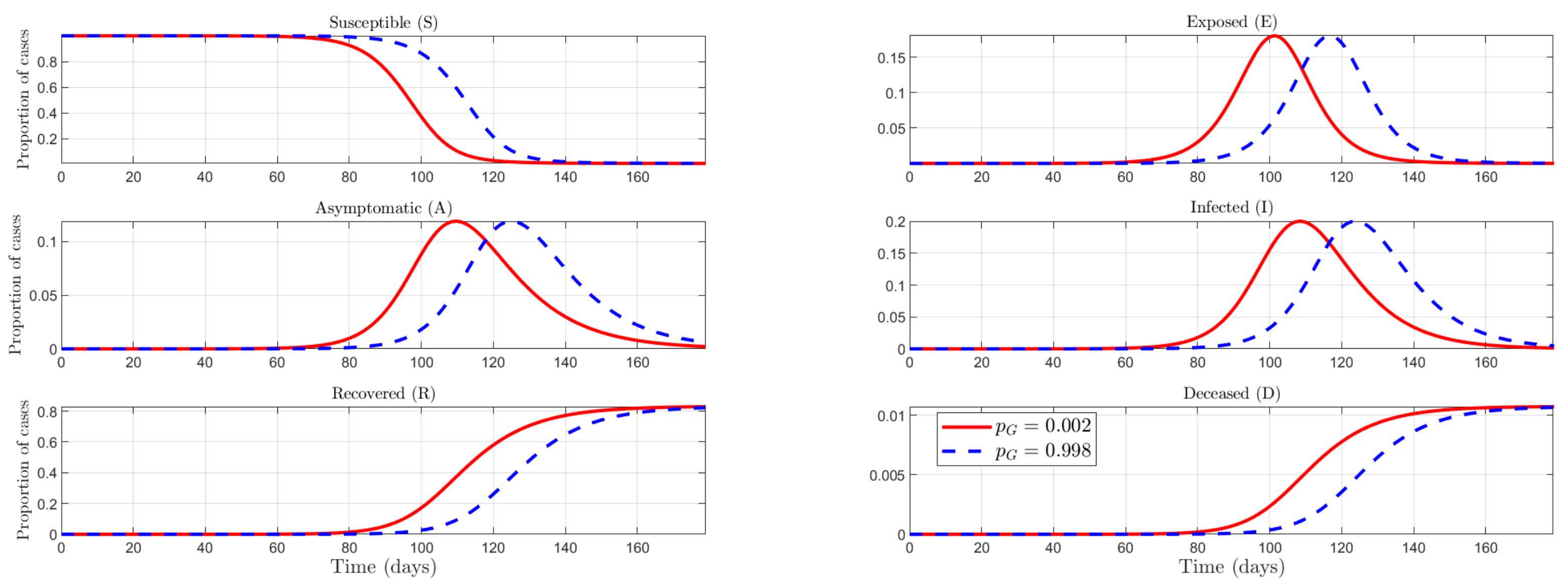
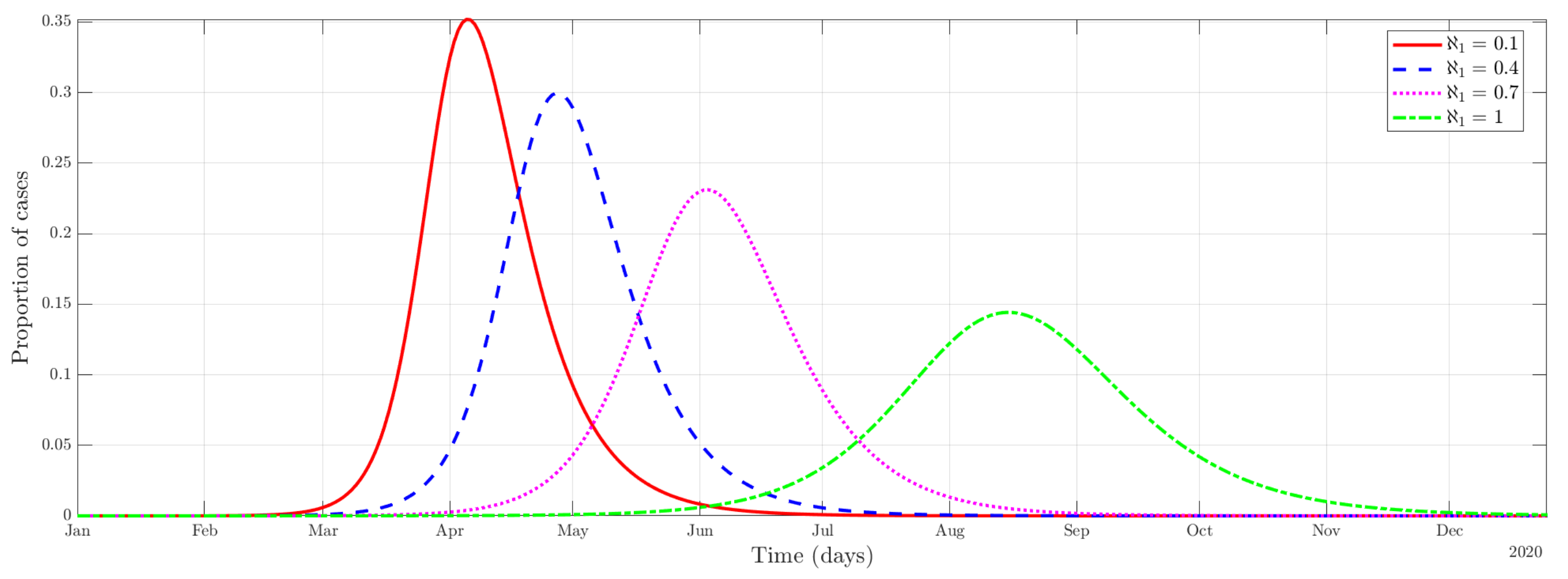
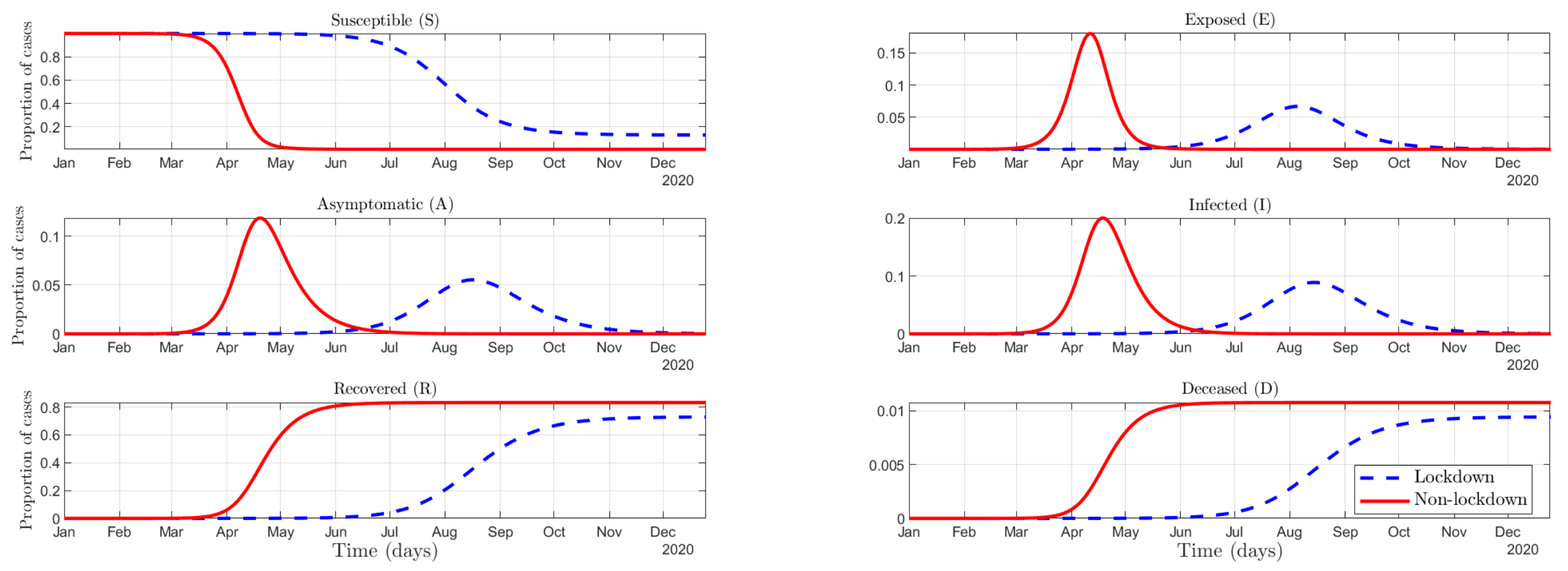
4.2. Numerical Results
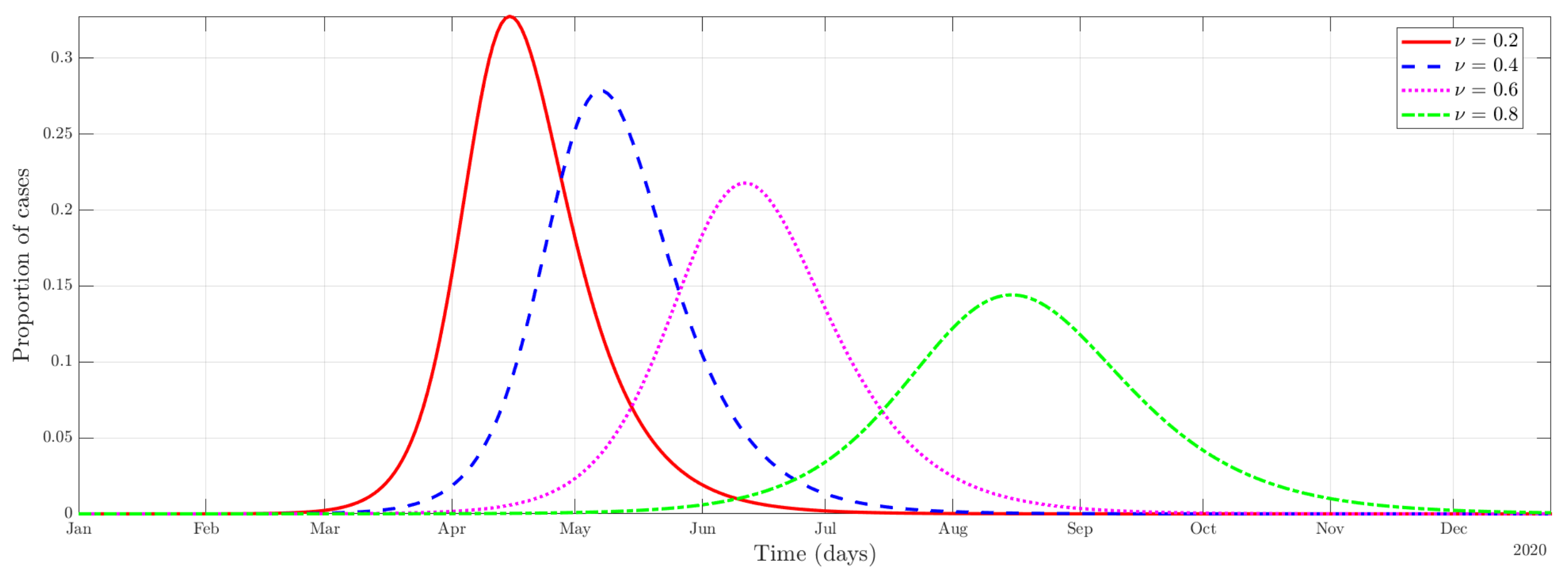
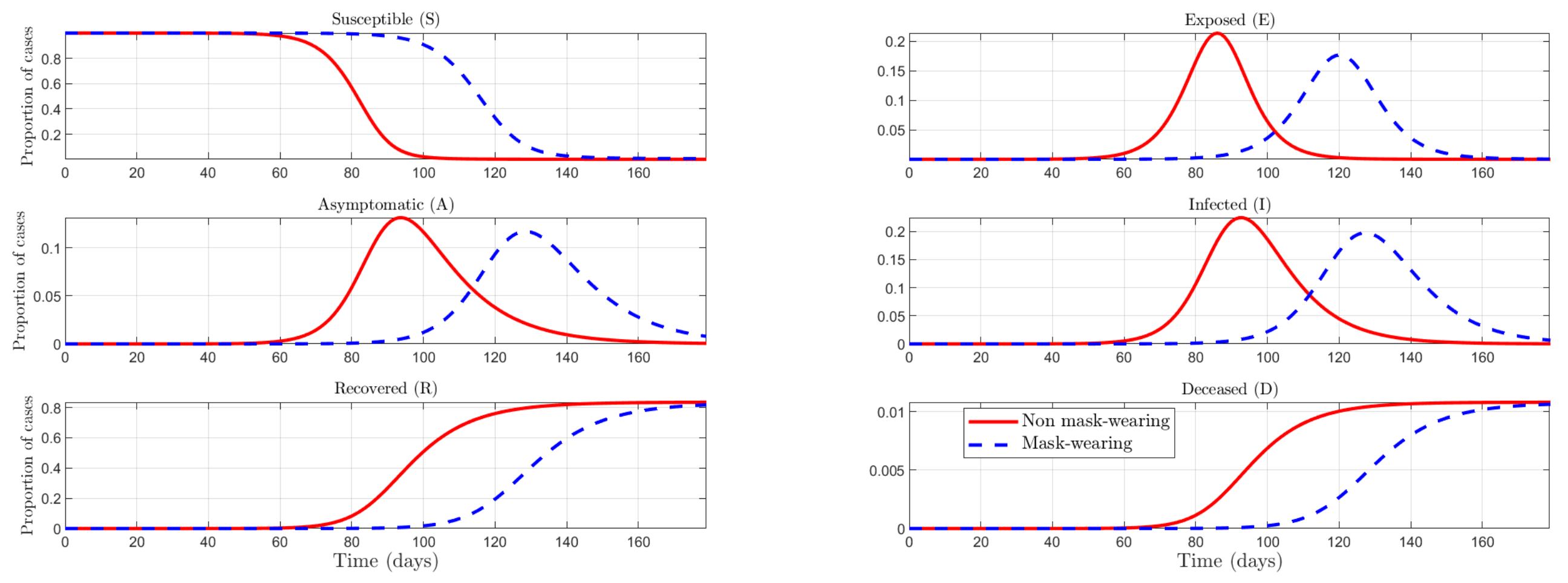
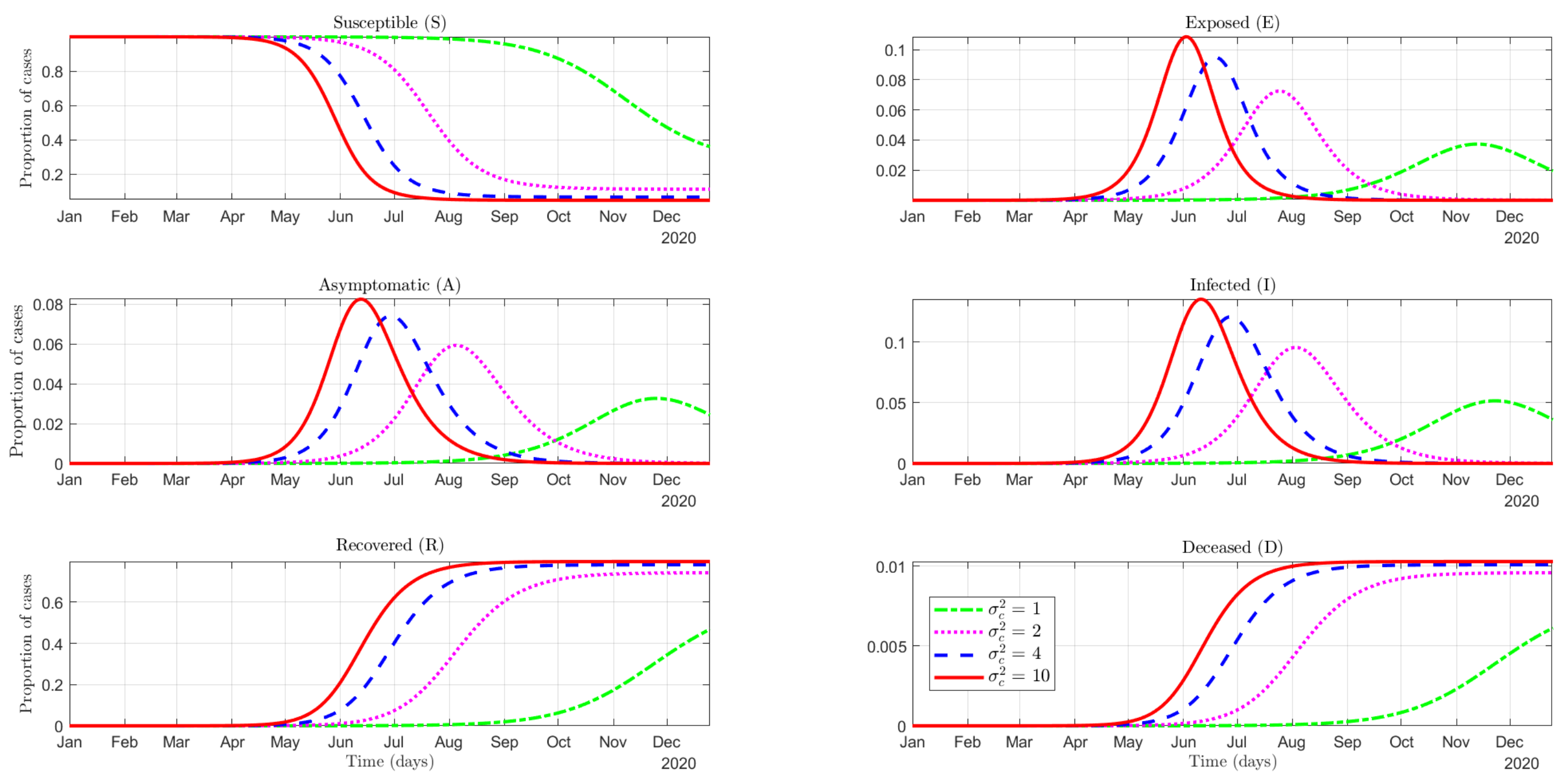
4.2.1. Effectiveness of the Use of Protective Measures
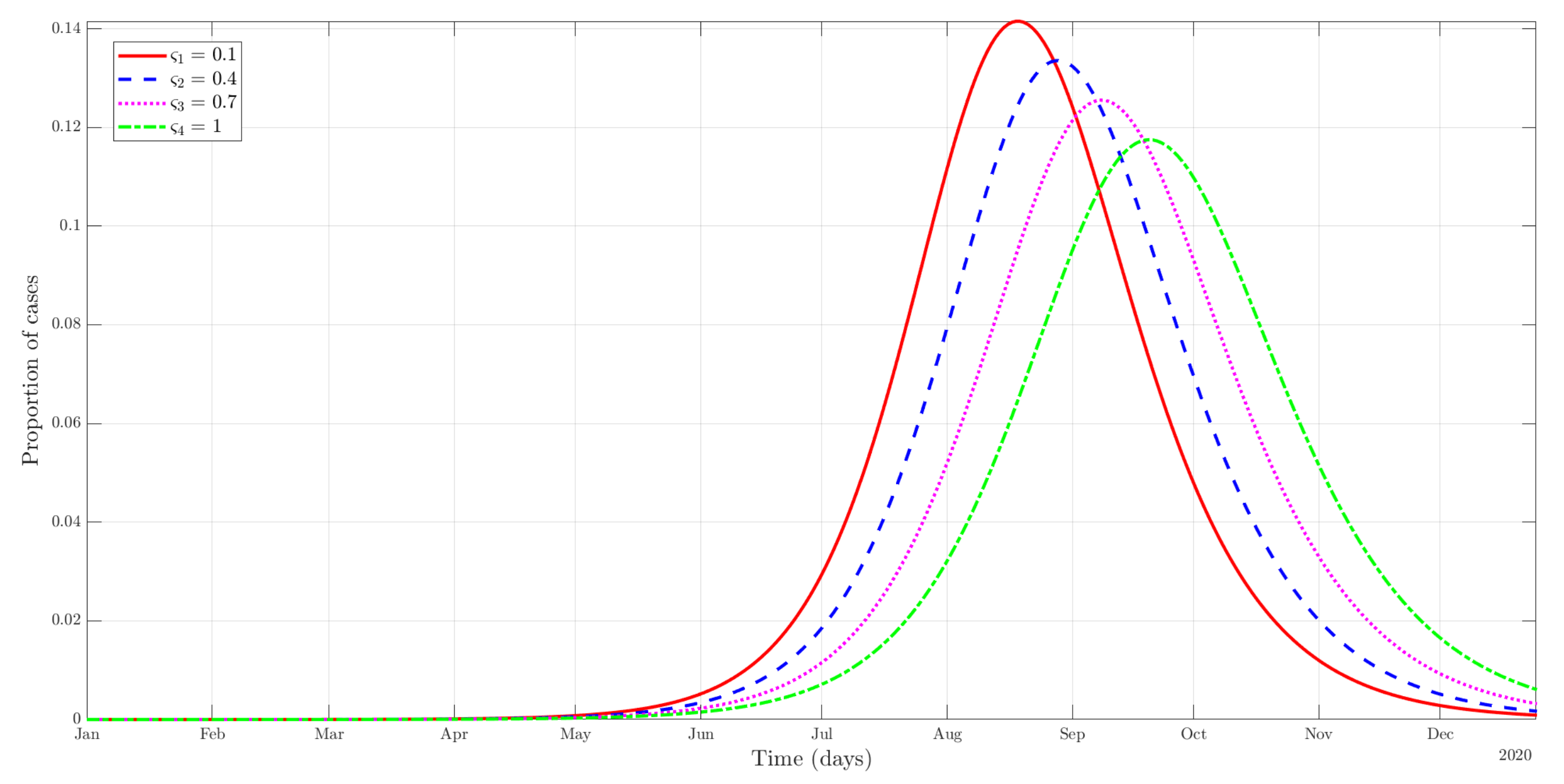
4.2.2. Social Norms
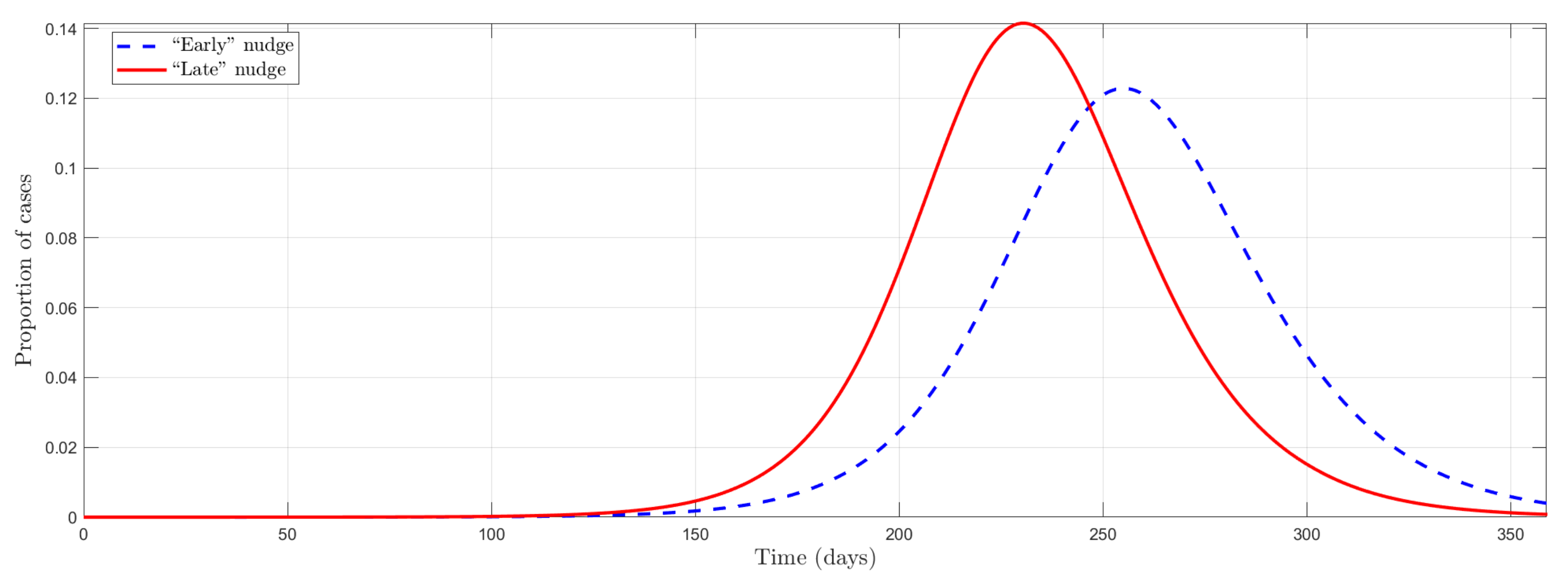
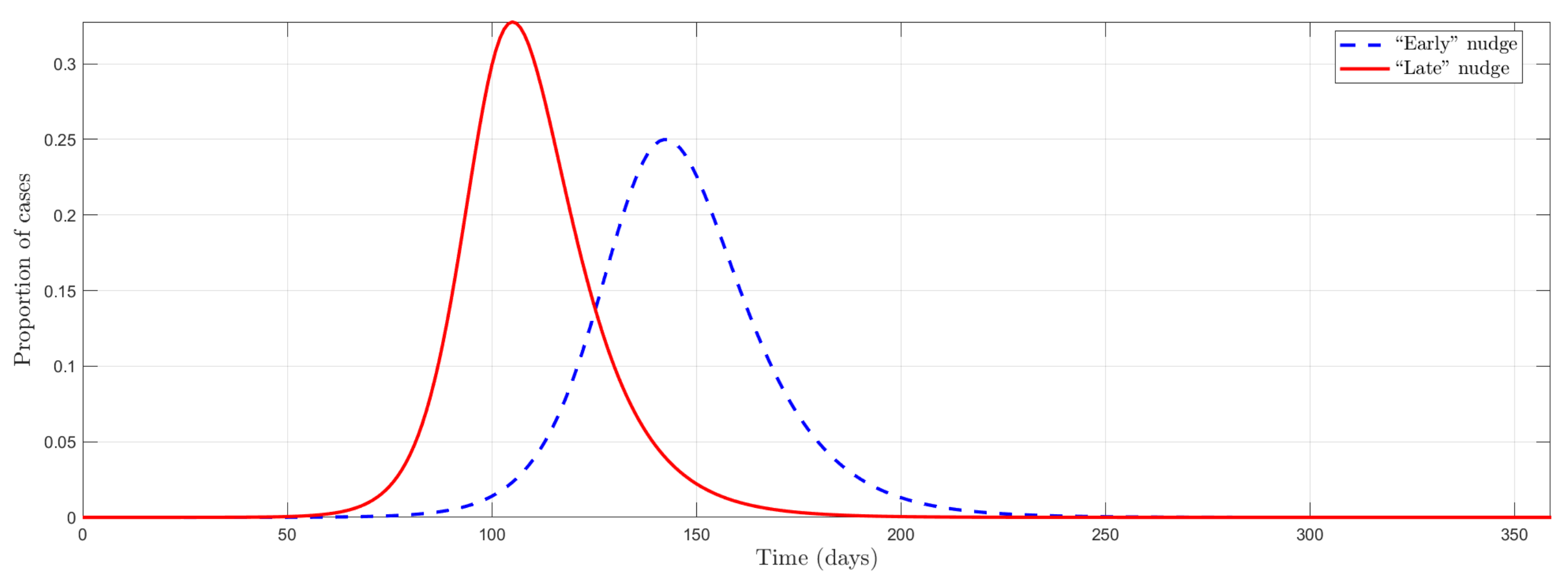
4.2.3. Mandates vs. Nudges to Fight COVID
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
Abbreviations
| SEIR | Susceptible-Exposed-Infectious-Removed |
| SEAIRD | Susceptible-Exposed-Asymptomatic-Infectious-Recovered-Deceased |
Appendix A. Initial Reaction to the Pandemic
| Protest | No Protest | |
| Democratic | 0 | |
| Authoritarian | 0 |
Appendix A.1. Government Equilibrium Behavior
- 1.
- Pooling equilibrium with Alarm, when: .
- 2.
- Separating equilibrium in which the democratic government chooses Wait, and the authoritarian government chooses Alarm, when:
- 3.
- Pooling equilibrium with Waiting, when
Appendix A.2. The Economic versus Health Trade-Off

Appendix A.3. Unexpected versus Expected Pandemic

Appendix B. Mathematical Proofs
- (1)
- Pooling equilibrium with Alarm: in this case, , and therefore and it must be the case that This is the condition for the democratic government, which implies the condition for the authoritarian government.
- (2)
- Separating equilibrium in which the democratic government chooses Wait, and the authoritarian government chooses Alarm. In this case and , what implies :
- (3)
- Pooling equilibrium in Waiting. In this case, , . The type that has the most incentives to deviate is authoritarian, so this equilibrium exists whenever
Appendix C. Additional Simulations




Appendix D. Behavioral Channels
References
- Soofi, M.; Najafi, F.; Karami-Matin, B. Using Insights from Behavioral Economics to Mitigate the Spread of COVID-19. Appl. Health Econ. Health Policy 2020, 18, 345–350. [Google Scholar] [CrossRef] [PubMed]
- Haushofer, J.; Metcalf, J.C.E. Combining Behavioral Economics and Infectious Disease Epidemiology to Mitigate the COVID-19 Outbreak; Princeton University: Princeton, NJ, USA, 2020; Volume 6, pp. 1–10. [Google Scholar]
- Abellán Perpiñán, J.M.; Jimenez-Gomez, D.; del Llano-Señarís, J. La gestión de la pandemia de SARS-CoV-2 según la economía del comportamiento. In Economía de la Salud (y más) de la COVID-19; Asociación de Economía de la Salud (Barcelona): Barcelona, Spain, 2020. [Google Scholar]
- Karing, A. Social signaling and childhood immunization: A field experiment in Sierra Leone. University of California Berkeley. 2018. Available online: https://economics.yale.edu/sites/default/files/jmp_socialsignaling.pdf (accessed on 1 May 2020).
- Pop-Eleches, C.; Thirumurthy, H.; Habyarimana, J.P.; Zivin, J.G.; Goldstein, M.P.; De Walque, D.; MacKeen, L.; Haberer, J.; Kimaiyo, S.; Sidle, J.; et al. Mobile phone technologies improve adherence to antiretroviral treatment in a resource-limited setting: A randomized controlled trial of text message reminders. Aids 2011, 25, 825–834. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Banerjee, A.V.; Duflo, E.; Glennerster, R.; Kothari, D. Improving immunisation coverage in rural India: Clustered randomised controlled evaluation of immunisation campaigns with and without incentives. BMJ 2010, 340. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van Bavel, J.J.; Boggio, P.; Capraro, V.; Cichocka, A.; Cikara, M.; Crockett, M.; Crum, A.; Douglas, K.; Druckman, J.; Drury, J.; et al. Using social and behavioural science to support COVID-19 pandemic response. Nat. Hum. Behav. 2020, 4, 460–471. [Google Scholar] [CrossRef]
- Halpern, S.D.; Miller, F.G. The Urge to Build More Intensive Care Unit Beds and Ventilators: Intuitive but Errant. Ann. Int. Med. 2020, 173, 302–303. [Google Scholar] [CrossRef]
- Murray, E.J. Epidemiology’s Time of Need: COVID-19 Calls for Epidemic-Related Economics. J. Econ. Perspect. 2020, 34, 105–120. [Google Scholar] [CrossRef]
- Geoffard, P.Y.; Philipson, T. Rational epidemics and their public control. Int. Econ. Rev. 1996, 37, 603–624. [Google Scholar] [CrossRef]
- Kremer, M. Integrating behavioral choice into epidemiological models of AIDS. Q. J. Econ. 1996, 111, 549–573. [Google Scholar] [CrossRef]
- Greenwood, J.; Kircher, P.; Santos, C.; Tertilt, M. An equilibrium model of the African HIV/AIDS epidemic. Econometrica 2019, 87, 1081–1113. [Google Scholar] [CrossRef] [Green Version]
- Auld, M.C. Choices, beliefs, and infectious disease dynamics. J. Health Econ. 2003, 22, 361–377. [Google Scholar] [CrossRef] [Green Version]
- Eichenbaum, M.S.; Rebelo, S.; Trabandt, M. The Macroeconomics of Epidemics; Technical Report; National Bureau of Economic Research: Cambridge, MA, USA, 2020. [Google Scholar]
- Garibaldi, P.; Moen, E.R.; Pissarides, C.A. Modelling contacts and transitions in the SIR epidemics model. Covid Econ. 2020, 5, 1–21. [Google Scholar]
- Jones, C.J.; Philippon, T.; Venkateswaran, V. Optimal Mitigation Policies in a Pandemic: Social Distancing and Working from Home; Technical Report; National Bureau of Economic Research: Cambridge, MA, USA, 2020. [Google Scholar]
- Reluga, T.C. Game Theory of Social Distancing in Response to an Epidemic. PLoS Comput. Biol. 2010, 6, e1000793. [Google Scholar] [CrossRef]
- Eksin, C.; Paarporn, K.; Weitz, J.S. Systematic biases in disease forecasting—The role of behavior change. Epidemics 2019, 27, 96–105. [Google Scholar] [CrossRef]
- OECD. Regulatory Policy and COVID-19: Behavioural Insights for Fast-Paced Decision Making; Technical Report November; 2020. Available online: https://www.oecd.org/coronavirus/policy-responses/regulatory-policy-and-covid-19-behavioural-insights-for-fast-paced-decision-making-7a521805/ (accessed on 14 April 2021).
- Lovallo, D.; Kahneman, D. Delusions of success. Harv. Bus. Rev. 2003, 81, 56–63. [Google Scholar]
- Altman, D.G.; Bland, J.M. Statistics notes: Absence of evidence is not evidence of absence. BMJ 1995, 311, 485. [Google Scholar] [CrossRef] [Green Version]
- Redelmeier, D.A.; Shafir, E. Pitfalls of judgment during the COVID-19 pandemic. Lancet Public Health 2020, 5, e306–e308. [Google Scholar] [CrossRef]
- Becker, G.S.; Murphy, K.M. Social Economics; Harvard University Press: Cambridge, MA, USA, 2009. [Google Scholar]
- Davies, N.G.; Kucharski, A.J.; Eggo, R.M.; Gimma, A.; Edmunds, W.J.; Jombart, T.; O’Reilly, K.; Endo, A.; Hellewell, J.; Nightingale, E.S.; et al. Effects of non-pharmaceutical interventions on COVID-19 cases, deaths, and demand for hospital services in the UK: A modelling study. Lancet Public Health 2020, 5, E375–E385. [Google Scholar] [CrossRef]
- Iwata, K.; Miyakoshi, C. A Simulation on Potential Secondary Spread of Novel Coronavirus in an Exported Country Using a Stochastic Epidemic SEIR Model. J. Clin. Med. 2020, 9, 944. [Google Scholar] [CrossRef] [Green Version]
- WHO. Modes of Transmission of Virus Causing COVID-19: Implications for IPC Precaution Recommendations; Technical Report; World Health Organization: Geneve, Switzerland, 2020. [Google Scholar]
- Nishiura, H.; Kobayashi, T.; Miyama, T.; Suzuki, A.; mok Jung, S.; Hayashi, K.; Kinoshita, R.; Yang, Y.; Yuan, B.; Akhmetzhanov, A.R.; et al. Estimation of the asymptomatic ratio of novel coronavirus infections (COVID-19). Int. J. Infect. Dis. 2020, 94, 154–155. [Google Scholar] [CrossRef]
- Peng, L.; Yang, W.; Zhang, D.; Zhuge, C.; Hong, L. Epidemic Analysis of COVID-19 in China by Dynamical Modeling. medRxiv 2020. [Google Scholar] [CrossRef] [Green Version]
- Backer, J.A.; Klinkenberg, D.; Wallinga, J. Incubation period of 2019 novel coronavirus (2019- nCoV) infections among travellers from Wuhan, China, 20 28 January 2020. Eurosurveillance 2020, 25, 2000062. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Prem, K.; Liu, Y.; Russell, T.W.; Kucharski, A.J.; Eggo, R.M.; Davies, N.; Flasche, S.; Clifford, S.; Pearson, C.A.; Munday, J.D.; et al. The effect of control strategies to reduce social mixing on outcomes of the COVID-19 epidemic in Wuhan, China: A modelling study. Lancet Public Health 2020, 5, e261–e270. [Google Scholar] [CrossRef] [Green Version]
- Giannitsarou, C.; Kissler, S.; Toxvaerd, F. Waning immunity and the second wave: Some projections for SARS-CoV-2. Am. Econ. Rev. Insights 2021, 3, 321–338. [Google Scholar] [CrossRef]
- Berger, D.W.; Herkenhoff, K.F.; Mongey, S. An SEIR Infectious Disease Model with Testing and Conditional Quarantine; Technical Report; National Bureau of Economic Research: Cambridge, MA, USA, 2020. [Google Scholar]
- Manski, C.F.; Molinari, F. Estimating the COVID-19 infection rate: Anatomy of an inference problem. J. Econ. 2021, 220, 181–192. [Google Scholar] [CrossRef] [PubMed]
- Atkeson, A. What Will Be the Economic Impact of COVID-19 in the US? Rough Estimates of Disease Scenarios; NBER Working Paper Series; Technical Report; National Bureau of Economic Research: Cambridge, MA, USA, 2020; p. 25. [Google Scholar]
- Stock, J.H. Data Gaps and the Policy Response to the Novel Coronavirus; Technical Report; National Bureau of Economic Research: Cambridge, MA, USA, 2020. [Google Scholar]
- Avery, C.; Bossert, W.; Clark, A.; Ellison, G.; Ellison, S.F. An Economist’s Guide to Epidemiology Models of Infectious Disease. J. Econ. Perspect. 2020, 34, 79–104. [Google Scholar] [CrossRef]
- Ferguson, N.; Laydon, D.; Nedjati Gilani, G.; Imai, N.; Ainslie, K.; Baguelin, M.; Bhatia, S.; Boonyasiri, A.; Cucunuba Perez, Z.; Cuomo-Dannenburg, G.; et al. Report 9: Impact of Non-Pharmaceutical Interventions (NPIs) to Reduce COVID19 Mortality and Healthcare Demand; Imperial College COVID-19 Response Team London: London, UK, 2020. [Google Scholar]
- Acemoglu, D.; Chernozhukov, V.; Werning, I.; Whinston, M.D. A Multi-Risk SIR Model with Optimally Targeted Lockdown. Am. Econ. Rev. Insights 2021, 3, 487–502. [Google Scholar] [CrossRef]
- Bonell, C.; Michie, S.; Reicher, S.; West, R.; Bear, L.; Yardley, L.; Curtis, V.; Amlôt, R.; Rubin, G.J. Harnessing behavioural science in public health campaigns to maintain ’social distancing’ in response to the COVID-19 pandemic: Key principles. J. Epidemiol. Community Health 2020, 74, 617–619. [Google Scholar] [CrossRef]
- Mitze, T.; Kosfeld, R.; Rode, J.; Wälde, K. Face masks considerably reduce COVID-19 cases in Germany. Proc. Natl. Acad. Sci. USA 2020, 117, 32293–32301. [Google Scholar] [CrossRef]
- Pfattheicher, S.; Nockur, L.; Böhm, R.; Sassenrath, C.; Petersen, M.B. The emotional path to action: Empathy promotes physical distancing and wearing of face masks during the COVID-19 pandemic. Psychol. Sci. 2020, 31, 1363–1373. [Google Scholar] [CrossRef]
- Betsch, C.; Korn, L.; Sprengholz, P.; Felgendreff, L.; Eitze, S.; Schmid, P.; Böhm, R. Social and behavioral consequences of mask policies during the COVID-19 pandemic. Proc. Natl. Acad. Sci. USA 2020, 117, 21851–21853. [Google Scholar] [CrossRef]
- Goldberg, M.; Gustafson, A.; Maibach, E.; van der Linden, S.; Ballew, M.T.; Bergquist, P.; Kotcher, J.; Marlon, J.R.; Rosenthal, S.; Leiserowitz, A. Social norms motivate COVID-19 preventive behaviors. PsyArXiv 2020. [Google Scholar] [CrossRef]
- Barceló, J.; Sheen, G.C.H. Voluntary adoption of social welfare-enhancing behavior: Mask-wearing in Spain during the COVID-19 outbreak. PLoS ONE 2020, 15, e0242764. [Google Scholar] [CrossRef]
- Bokemper, S.E.; Cucciniello, M.; Rotesi, T.E.; Pin, P.; Malik, A.A.; Willebrand, K.; Paintsil, E.E.; Omer, S.B.; Huber, G.A.; Melegaro, A. Beliefs about Mask Efficacy and the Effect of Social Norms on Mask Wearing Intentions for COVID-19 Risk Reduction. PLoS ONE 2021, 16, e0258282. [Google Scholar] [CrossRef]
- Howard, J.; Huang, A.; Li, Z.; Tufekci, Z.; Zdimal, V.; van der Westhuizen, H.M.; von Delft, A.; Price, A.; Fridman, L.; Tang, L.H.; et al. An evidence review of face masks against COVID-19. Proc. Natl. Acad. Sci. USA 2021, 118, e2014564118. [Google Scholar] [CrossRef]
- Wang, X.; Ferro, E.G.; Zhou, G.; Hashimoto, D.; Bhatt, D.L. Association between universal masking in a health care system and SARS-CoV-2 positivity among health care workers. JAMA 2020, 324, 703–704. [Google Scholar] [CrossRef]
- Wang, Y.; Tian, H.; Zhang, L.; Zhang, M.; Guo, D.; Wu, W.; Zhang, X.; Kan, G.L.; Jia, L.; Huo, D.; et al. Reduction of secondary transmission of SARS-CoV-2 in households by face mask use, disinfection and social distancing: A cohort study in Beijing, China. BMJ Glob. Health 2020, 5, e002794. [Google Scholar] [CrossRef]
- Clapp, P.W.; Sickbert-Bennett, E.E.; Samet, J.M.; Berntsen, J.; Zeman, K.L.; Anderson, D.J.; Weber, D.J.; Bennett, W.D. Evaluation of cloth masks and modified procedure masks as personal protective equipment for the public during the COVID-19 pandemic. JAMA Int. Med. 2021, 181, 463–469. [Google Scholar] [CrossRef]
- World Health Organization. Advice on the Use of Masks in the Context of COVID-19: Interim Guidance; Technical Report; World Health Organization: Geneve, Switzerland, 2020; Available online: https://apps.who.int/iris/handle/10665/332293 (accessed on 26 May 2022).
- Mahikul, W.; Chotsiri, P.; Ploddi, K.; Pan-Ngum, W. Evaluating the impact of intervention strategies on the first wave and predicting the second wave of COVID-19 in thailand: A mathematical modeling study. Biology 2021, 10, 80. [Google Scholar] [CrossRef]
- Chernozhukov, V.; Kasahara, H.; Schrimpf, P. Causal impact of masks, policies, behavior on early covid-19 pandemic in the U.S. J. Econ. 2021, 220, 23–62. [Google Scholar] [CrossRef]
- Summers, J.; Cheng, H.Y.; Lin, H.H.; Barnard, L.T.; Kvalsvig, A.; Wilson, N.; Baker, M.G. Potential lessons from the Taiwan and New Zealand health responses to the COVID-19 pandemic. Lancet Reg. Health West. Pac. 2020, 4, 100044. [Google Scholar] [CrossRef]
- Zhou, R.; Li, F.; Chen, F.; Liu, H.; Zheng, J.; Lei, C.; Wu, X. Viral dynamics in asymptomatic patients with COVID-19. Int. J. Infect. Dis. 2020, 96, 288–290. [Google Scholar] [CrossRef]
- Abellán Perpiñán, J.M.; Cierco, C.; Jimenez-Gomez, D. Nudges y la pandemia: Un análisis desde la economía y el derecho conductual. Gac. Sanit. 2022, 36, 93–96. [Google Scholar] [CrossRef] [PubMed]
- Laibson, D. Golden eggs and hyperbolic discounting. Q. J. Econ. 1997, 112, 443–478. [Google Scholar] [CrossRef] [Green Version]
- European Centre for Disease Prevention and Control. Risk Factors and Risk Groups. 2021. Available online: https://www.ecdc.europa.eu/en/covid-19/latest-evidence/risk-factors-risk-groups (accessed on 1 May 2021).
- Aumann, R.J. Agreeing to Disagree. Ann. Stat. 1976, 4, 1236–1239. [Google Scholar] [CrossRef]
- Pulejo, Massimo; Querubín, Pablo Electoral concerns reduce restrictive measures during the COVID-19 pandemic. J. Public Econ. 2021, 198, 104387. [CrossRef] [PubMed]
- Sly, L. Stirrings of Unrest around the World could Portend Turmoil as Economies Collapse. 2020. Available online: https://www.washingtonpost.com/world/coronavirus-protests-lebanon-india-iraq/2020/04/19/1581dde4-7e5f-11ea-84c2-0792d8591911_story.html (accessed on 17 May 2021).
- Morris, S.; Shin, H.S. Global Games: Theory and Applications. In Advances in Economics and Econometrics. Theory and Applications, Eighth World Congress (Seattle 2000); Dewatripont, M., Hansen, L.P., Turnovsky, S.J., Eds.; Econometric Society; Cambridge University Press: Cambridge, UK, 2003; Volume 1, Chapter 3; pp. 56–103. [Google Scholar]
- Chilton, S.; Nielsen, J.S.; Wildman, J. Beyond COVID-19: How the “dismal science” can prepare us for the future. Health Econ. 2020, 29, 851–853. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.; Saltman, R.B. Policy lessons from early reactions to the COVID-19 virus in China. Am. J. Public Health 2020, 110, 1145–1148. [Google Scholar] [CrossRef]
- Lai, S.; Ruktanonchai, N.W.; Zhou, L.; Prosper, O.; Luo, W.; Floyd, J.R.; Wesolowski, A.; Santillana, M.; Zhang, C.; Du, X.; et al. Effect of non-pharmaceutical interventions to contain COVID-19 in China. Nature 2020, 585, 410–413. [Google Scholar] [CrossRef]
- Matjasko, J.L.; Cawley, J.H.; Baker-Goering, M.M.; Yokum, D.V. Applying behavioral economics to public health policy: Illustrative examples and promising directions. Am. J. Prevent. Med. 2016, 50, S13–S19. [Google Scholar] [CrossRef] [Green Version]
- An, S. Antidepressant direct-to-consumer advertising and social perception of the prevalence of depression: Application of the availability heuristic. Health Commun. 2008, 23, 499–505. [Google Scholar] [CrossRef]
- Folkes, V.S. The availability heuristic and perceived risk. J. Consum. Res. 1988, 15, 13–23. [Google Scholar] [CrossRef]
- Esparza, J. Lessons From History: What Can We Learn From 300 Years of Pandemic Flu That Could Inform the Response to COVID-19? Am. J. Public Health 2020, 110, 1160–1161. [Google Scholar] [CrossRef]
- Kahneman, D.; Knetsch, J.L.; Thaler, R.H. The endowment effect, loss aversion, and status quo bias. J. Econ. Perspect. 1991, 5, 193–206. [Google Scholar] [CrossRef] [Green Version]
- DeCicca, P.; Kenkel, D.; Mathios, A.; Shin, Y.J.; Lim, J.Y. Youth smoking, cigarette prices, and anti-smoking sentiment. Health Econ. 2008, 17, 733–749. [Google Scholar] [CrossRef] [Green Version]
- Hsieh, C.S.; van Kippersluis, H. Smoking initiation: Peers and personality. Quant. Econ. 2018, 9, 825–863. [Google Scholar] [CrossRef]
- Fletcher, J.M.; Ross, S.L. Estimating the effects of friends on health behaviors of adolescents. Health Econ. 2018, 27, 1450–1483. [Google Scholar] [CrossRef]
- Marin-Lopez, B.A. Risky Behavior Initiation with Behavioral Agents and Social Interactions. 2021. Available online: https://ssrn.com/abstract=3915368 (accessed on 17 May 2021).





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter | Value Used | Range | Description | Reference |
|---|---|---|---|---|
| 0.5 | - | Subclinical infectious rate A vs. I | [24] | |
| 0.65 | 0.1–1 | (Baseline) Transmission rate | [25] | |
| 1/14 | - | Recovery rate for mild infections | [26] | |
| 1/3 | 0.05–0.6 | Proportion of subclinical cases | [27] | |
| 0.021 | 0.005–0.03 | Death rate | [28] | |
| 1/6.4 | - | Incubation rate | [29] |
| Parameter | Value Used | Theoretical Range | Description | Behavioral Interpretation |
|---|---|---|---|---|
| 0.5 | Citizen’s and government’s prior |
| ||
| −0.5 | Disutility of contracting COVID-19 | – | ||
| c | Economic/psychological cost | – | ||
| 0 | Population mean of the cost c | |||
| 1 | Population variance of the cost c | |||
| 0.5 | Extra “moral” utility (for I) | – | ||
| , | Lockdown efficacy | – | ||
| 0.8 | Protective measures efficacy (for S and I) | Wrong beliefs : Availability heuristic | ||
| 0 | Strength of social norms | Social/Country norms |
| Protect | Don’t Protect | |
|---|---|---|
| I | 0 | |
| R | 0 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Marin-Lopez, B.A.; Jimenez-Gomez, D.; Abellán-Perpiñán, J.-M. Behavioral Economics in the Epidemiology of the COVID-19 Pandemic: Theory and Simulations. Int. J. Environ. Res. Public Health 2022, 19, 9557. https://doi.org/10.3390/ijerph19159557
Marin-Lopez BA, Jimenez-Gomez D, Abellán-Perpiñán J-M. Behavioral Economics in the Epidemiology of the COVID-19 Pandemic: Theory and Simulations. International Journal of Environmental Research and Public Health. 2022; 19(15):9557. https://doi.org/10.3390/ijerph19159557
Chicago/Turabian StyleMarin-Lopez, Blas A., David Jimenez-Gomez, and José-María Abellán-Perpiñán. 2022. "Behavioral Economics in the Epidemiology of the COVID-19 Pandemic: Theory and Simulations" International Journal of Environmental Research and Public Health 19, no. 15: 9557. https://doi.org/10.3390/ijerph19159557