Article Text

Abstract
Objective To assess the impact of the COVID-19 outbreak on cardiovascular disease (CVD) related mortality and hospitalisation.
Design Community-based prospective cohort study.
Setting The UK Biobank.
Participants 421 372 UK Biobank participants who were registered in England and alive as of 1 January 2020.
Primary and secondary outcome measures The primary outcome of interest was CVD-related death, which was defined as death with CVD as a cause in the death register. We retrieved information on hospitalisations with CVD as the primary diagnosis from the UK Biobank hospital inpatient data. The study period was 1 January 2020 to June 30 2020, and we used the same calendar period of the three preceding years as the reference period. In order to control for seasonal variations and ageing of the study population, standardised mortality/incidence ratios (SMRs/SIRs) with 95% CIs were used to estimate the relative risk of CVD outcomes during the study period, compared with the reference period.
Results We observed a distinct increase in CVD-related deaths in March and April 2020, compared with the corresponding months of the three preceding years. The observed number of CVD-related deaths (n=218) was almost double in April, compared with the expected number (n=120) (SMR=1.82, 95% CI 1.58 to 2.07). In addition, we observed a significant decline in CVD-related hospitalisations from March onwards, with the lowest SIR observed in April (0.45, 95% CI 0.41 to 0.49).
Conclusions There was a distinct increase in the number of CVD-related deaths in the UK Biobank population at the beginning of the COVID-19 outbreak. The shortage of medical resources for hospital care and stress reactions to the pandemic might have partially contributed to the excess CVD-related mortality, underscoring the need of sufficient healthcare resources and improved instructions to the public about seeking healthcare in a timely way.
- cardiology
- COVID-19
- epidemiology
- health services administration & management
Data availability statement
Data used in this study was from the UK Biobank (http://www.ukbiobank.ac.uk/), which are available to all researchers on making an application. Part of this research was conducted using the UK Biobank Resource under Application 54803.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
The major merit of our study is the self-comparison analysis, which adjusted inherently for potential confounders that are constant over time, including genetic factors and many environmental factors that did not change greatly within the 4-year period.
Seasonal variation and ageing of the study population were well controlled by monthly based estimations and calculation of standardised expected numbers and standardised incidence ratios.
For the fact that accessibility to COVID-19 test was largely restricted to inpatients with symptoms before 27 April 2020 in the UK, we might have underestimated the number of deaths related to COVID-19 in March and April.
Introduction
Since the first reported case of COVID-19 in December 2019, the epidemic has spread rapidly all over the globe and has had a profound influence on the global economy and public health. The WHO declared COVID-19 a Public Health Emergency of International Concern on 30 January 2020, and later, on 11 March 2020, it was declared a pandemic.1 On 21 October 2020, the number of daily confirmed cases hit a new record of more than 600 000 worldwide, and this signalled the start of a second wave of the pandemic. As of 18 October 2020, COVID-19 had cumulatively affected around 40 million people and caused more than 1.1 million deaths.2
The COVID-19 pandemic has placed tremendous pressure on healthcare service systems worldwide. The healthcare demand created by the COVID-19 pandemic is far beyond the hospital surge capacity in many countries, including the UK.3 4 In addition to insufficient ascertainment and treatment of COVID-19, the severe shortage of medical resources might have considerable impact on patients with other severe diseases, such as cardiovascular disease (CVD). To prevent the rapid spread of COVID-19, the UK government advised people to practice social distancing on 16 March and implemented behavioural restrictions enforceable by law on 23 March.5 These measures might have induced stress reactions6 and prevented people from seeking health care.7 Indeed, since March, urgent 2-week wait cancer referrals were reported to have decreased by up to 80% in the UK.8
Despite its relatively low fatality rate, the COVID-19 crisis has led to high levels of stress in the population.9 Notable sources of stress include witnessing the rapid spread of the disease and an overwhelmed healthcare system, concerns about being infected and financial difficulties resulting from the pandemic.10 Accumulating evidence from epidemiological, clinical and experimental studies have revealed that psychological stress,11 including stressful life events12 13 and stress-related disorders,14 have an important influence on fatal cardiovascular events. However, it is unclear whether the severe psychological stress experienced in relation to COVID-19 is associated with changes in CVD-related mortality.
In the present study, we have used a community-based sample deposited in the UK Biobank, which contains timely and continuously updated longitudinal data on various health outcomes, to explore the potential impact of the COVID-19 pandemic on CVD-related death. Our aim was to investigate whether there was an increase in CVD-related mortality at the beginning of the COVID-19 pandemic in the UK and the possible reasons for this increase.
Methods
The UK Biobank recruited 502 507 participants aged 40–69 years who were registered with the National Health Service (NHS) and collected information about their sociodemographic, lifestyle and health-related factors with the help of questionnaires between 2006 and 2010.15 Health-related outcomes for all the UK Biobank participants were obtained through periodically linked data from multiple national datasets, with the participants’ consent.15 The inpatient hospital data were obtained through linked medical records, mapped across England, Scotland and Wales using the Hospital Episode Statistics in England, Scottish Morbidity Record and Patient Episode Database for Wales.16 The mortality data were obtained from death registers, that is, the NHS Digital and NHS Central Registry.17 The inpatient hospital and mortality data were updated on a monthly basis. To facilitate COVID-19 research, results of COVID-19 tests performed by real-time RT-PCR (RdRp gene assay) of oral swab samples obtained in England from 16 March 2020 onwards, have been made available, through cross-linkage to the Public Health England (PHE) microbiology database.18
Study design
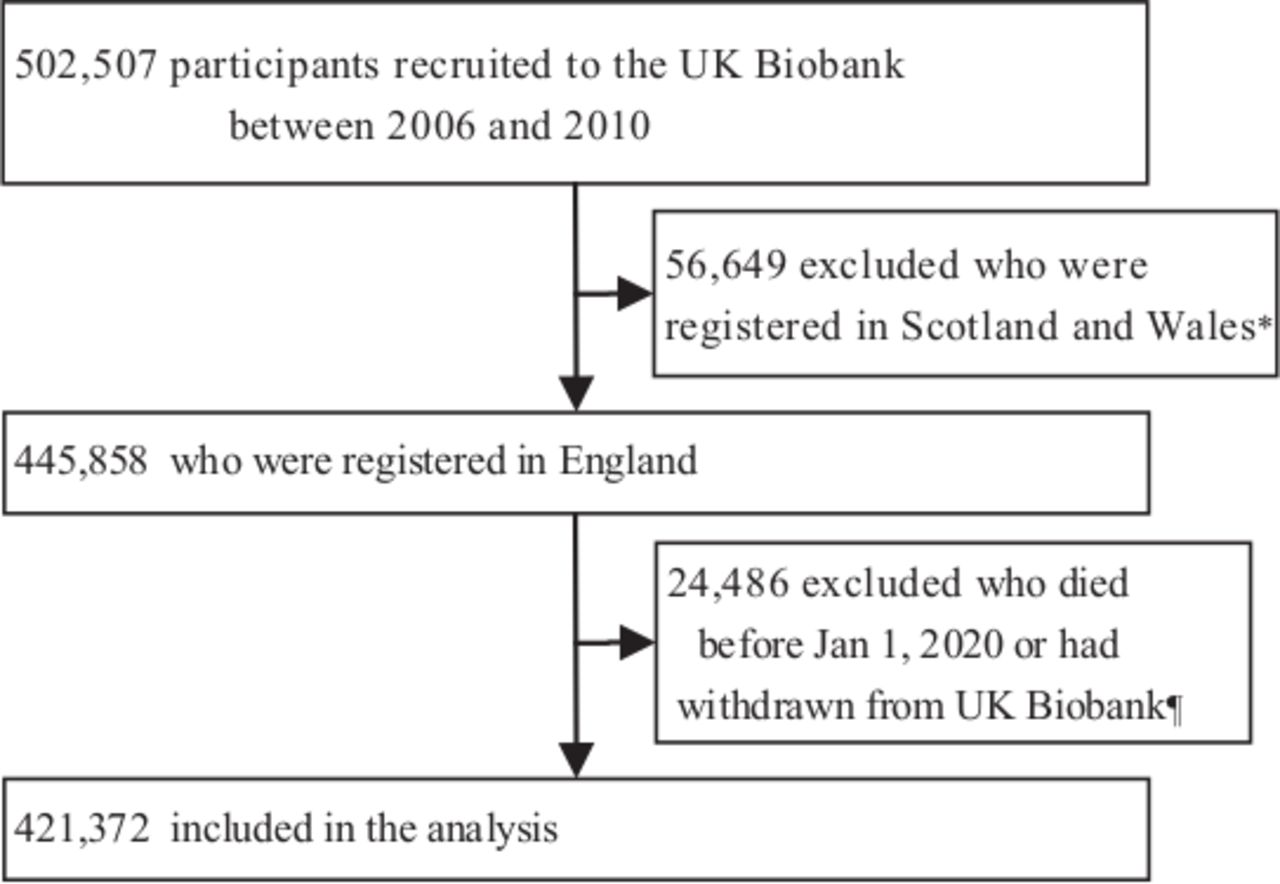
In the present study, we included participants (n=445 858) from the UK Biobank cohort who were registered in England, as inpatient hospital data during the COVID-19 outbreak were not available for participants in Scotland and Wales (figure 1). After excluding 24 486 individuals who died before 1 January or had withdrawn from the UK Biobank cohort, we included a total of 421 372 participants in the analyses (figure 1). The primary outcome of interest was CVD-related mortality during the COVID-19 outbreak, and the study period was 1 January 2019 to 30 June 2020. In order to account for seasonal variations in CVD-related mortality,19 we used the same calendar period of the three preceding years, as the reference period. In addition to CVD-related mortality, we also estimated all-cause mortality during the COVID-19 outbreak. As a proxy for access to healthcare for severe CVD, data on hospitalisations due to CVD were obtained and considered as the secondary outcome.

Flow chart of the study. *The inpatient hospital data during the COVID-19 outbreak were not available for participants in Scotland and Wales. ¶The first COVID-19 positive patient was diagnosed on 31 January 2020 in the UK.
CVD-related death and hospitalisation for CVD
CVD-related death was defined as death with CVD as a cause, according to the International Classification of Diseases version 10 (ICD-10) codes I00-I70, I730 and I74-I75,14 based on relevant data from the death registers. Because COVID-19 patients with cardiovascular comorbidity are more likely to experience fatal outcomes20 and infection of SARS-CoV-2 leads to cardiac injuries,21 we conducted a separate analysis in which individuals with confirmed COVID-19 who died of CVD were excluded. The ascertainment of COVID-19 status was mainly based on the PHE dataset, which contains information about specimen date, origin (inpatient or not) and result (positive or negative) for all COVID-19 tests performed in England since 16 March 2020.18 We further used the UK Biobank inpatient hospital data and mortality data, that is, any diagnosis or cause of death coded with ICD-10 code U07.1 and U07.2, as supplements for COVID-19 cases identification. Hospitalisation for CVD was defined as hospital admission with a primary diagnosis of CVD (ICD-10: I00-I70, I730 and I74-I75).
We also conducted several subanalyses in which we focused on the five major subtypes of CVD14: acute myocardial infraction (ICD-10: I21, I23-I24), arrhythmia (I47-I49), essential hypertension (I10), heart failure (I50) and stroke (I61- I64) (see online supplemental table 1).
Supplemental material
Covariates
Personal data, such as birth year and sex, were collected at baseline through questionnaires. Patients with CVD are more susceptible to COVID-19 and have a worse prognosis after infection20 21; additionally, patients with psychiatric disorders also have an increased risk of COVID-19 and COVID-19 related death.22 23 Therefore, we also extracted information about history of CVD and psychiatric disorders, defined as a primary diagnosis of CVD or psychiatric disorder (the ICD-10 codes are listed in online supplemental table 1) before 1 January 2020, from the UK Biobank inpatient hospital data.
Statistical analysis
We first calculated the monthly number of CVD-related deaths between 1 January 2020 and 30 June 2020. We also calculated the mean number of CVD-related deaths in the corresponding 6 months during the three preceding years. To account for ageing of the cohort, we calculated the expected age-standardised monthly number of CVD-related deaths for the study period by multiplying the number of persons by the average age-specific (1-year strata), sex-specific and month-specific mortality rates derived from the same period of the previous 3 years (ie, the reference period), in the same population. The standardised mortality ratios (SMRs), that is, the ratio of the observed to the expected number of CVD-related deaths, along with their corresponding 95% CIs14 were then used to estimate the relative risk of CVD-related death, when the study period is compared with the reference period.
In addition to considering all CVDs as one group, we performed separate analyses for the five major subtypes of CVD. Furthermore, to explore the impact of history of CVD and psychiatric disorders on SMR, we conducted subgroup analyses according to history of CVD or psychiatric disorders (yes or no).
We then repeated all the above analyses, including calculations of SMRs for all-cause mortality and standardised incidence ratios (SIRs) for CVD-related hospitalisation. All analyses and graph drawings were carried out using R V.4.0.0. A two-sided p value of <0.05 was considered to indicate statistical significance.
Patient and public involvement
In this study, no participants were involved in setting research questions or outcome measures, nor were they involved in developing proposals for design or implementation. We are not going to directly disseminate the results of this study to involved participants or relevant participants communities but plan to disseminate them through publication of this study.
Results
The average monthly number of CVD-related deaths remained largely constant between January and June in 2017–2019 (reference period). In 2020, the number of CVD-related deaths was generally higher than that in the preceding years, and we observed a peak in CVD-related deaths in March and April (figure 2A and online supplemental table 2). Even when the ageing of the population was considered, an increase in the number of CVD-related deaths was found in March and April when the study period was compared with the reference period (figure 2B). For instance, in April, the observed number of CVD-related deaths (n=218) was almost double that of the expected number (n=120), and this corresponded to an SMR of 1.82 (95% CI 1.58 to 2.07) (orange line, figure 2C). After excluding CVD-related deaths in cases with confirmed COVID-19, we observed a diminished but statistically significant increase in March (the SMR decreased from 1.38 (95% CI 1.17 to 1.60) to 1.19 (95% CI 1.00 to 1.40)) but not in April (SMR=0.98, 95% CI 0.81 to 1.17) (blue dashed line, figure 2C). Additionally, we observed largely similar changes in all-cause mortality and CVD-related mortality, with slightly smaller SMRs (1.30 (95% CI 1.17 to 1.43) for March and 1.51 (95% CI 1.39 to 1.64) for April) for all-cause mortality than for CVD-related mortality (SMR: 1.38 (95% CI 1.17 to 1.60) for March and 1.82 (95% CI 1.58 to 2.07) for April) (online supplemental figure 1 and online supplemental table 3). We observed a significant decline in CVD-related hospitalisations from March onwards, and the lowest SIR was observed in April (0.45, 95% CI 0.41 to 0.49), when the study period was compared with the reference period (figure 2D–F and online supplemental table 4).

SMRs with 95% CI for CVD-related mortality and SIRS with 95% CI for CVD-related hospitalisation. *The expected monthly number for CVD-related deaths and hospitalisations during the study period was calculated by multiplying the number of persons by the average age-specific (1-year strata), sex-specific and month-specific mortality rates derived from the same period of the preceding 3 years (ie, the reference period), within the same population. CVD, cardiovascular disease; SIRS, standardised incidence ratios.
For both CVD-related death and hospitalisation, the observed temporal patterns did not vary significantly depending on whether the patients had a history of CVD (online supplemental figure 2 and online supplemental table 5) or psychiatric disorders (online supplemental figure 3 and online supplemental table 6).
Figure 3 and online supplemental tables 7 and 8 show the results for the five major subtypes of CVD. In general, consistent with the main analyses, an increase in deaths due to these specific CVDs was mainly observed in March and April. In March, we found an increase in deaths caused by essential hypertension (a 72.00% increase, compared with the age-standardised expected number), arrhythmia (114.29% increase) and stroke (29.63% increase) (orange and black lines, figure 3A). The increase in deaths was lower but did not disappear after deaths with confirmed COVID-19 were excluded (blue dashed lines, figure 3A). However, the decrease in hospitalisations for the subtypes of CVD was smaller in magnitude in March, especially for essential hypertension (14.29% decrease) and stroke (7.38% decrease) (figure 3B). In April, compared with March, we observed a further increase in mortality caused by essential hypertension, arrhythmia and stroke, as well as an additional increase in deaths caused by heart failure, but all these increases disappeared after excluding deaths with confirmed COVID-19 (blue dashed lines, figure 3A). Finally, the decrease in hospitalisations for the different subtypes was similar in April and March (figure 3B).

{kind=link}
{kind=link}
{kind=link}
The number of deaths and hospitalisations for five major types of CVD. *The expected monthly number for deaths and hospitalisations during the study period was calculated by multiplying the number of persons by the average age-specific (1-year strata), sex-specific and month-specific mortality rates derived from the same period of the preceding 3 years (ie, the reference period), within the same population. CVD, cardiovascular disease.
Discussion
Our analyses of a large community-based cohort from the UK Biobank showed that in March and April 2020, there was a considerably higher risk of CVD-related deaths that was accompanied by a significantly reduced rate of CVD-related hospitalisations. This pattern matches the exponential growth pattern of COVID-19 cases in the UK during the time (eg, from 35 to 25 521 from the beginning to the end of March). These findings indicate that the shortage of healthcare resources for regular CVD care might have partially contributed to the excess CVD-related mortality. In addition, when COVID-19 cases were excluded from the analysis, the number of CVD-related deaths was significantly reduced. These findings may indicate the substantial impact of COVID-19 on the cardiovascular system. Additionally, because mortality increase was mainly observed in March when COVID-19 cases were excluded, whereas the decrease in CVD-related hospitalisations was greater in April than in March. This implies that the transient inflation in the number of CVD-related deaths may also be attributed to other reasons, such as severe emotional stress reactions experienced at the beginning of the pandemic, which has been demonstrated as a potent trigger for fatal CVD.14
Increase in deaths due to CVD during the COVID-19 outbreak have been described previously,24–26 but limited effort had been directed towards exploring the underlying reasons. In the USA, between March and April 2020, CVD-related deaths increased by 89% in the five states with the highest number of COVID-19 related deaths.26 Similarly, according to death registers in England and Wales, 2085 more deaths were caused by acute CVD between 2 March and 30 June 2020, compared with the same period of the previous 6 years.25 In the present study, we expanded these previous findings by showing that the increase in all-cause mortality was similar, although of slightly smaller magnitude, to the increase in CVD-related mortality. This indicates that a higher-than-expected increase in CVD-related mortality relative to mortality due to other causes.
Our finding about decreased healthcare capabilities for CVD during the COVID-19 pandemic among UK Biobank participants is in line with reports from other investigators, but previous studies did not provide data on the subtypes of CVD.27 28 In an analysis of data from Akershus University Hospital in Norway, Myhre et al29 showed a reduction in hospitalisations for CVD during the first wave of the pandemic, which continued up to the first few weeks after the restriction was eased. Additionally, analyses of hospital admissions in England revealed a substantial reduction in the weekly number of patients with acute coronary syndrome who were admitted to hospitals in England between the end of March and the end of May 2020.28 A similar decrease in hospital admissions for stroke was also observed during the pandemic.27
Other explanations for the observed increase in CVD-related mortality may include fear of seeking healthcare by patients in need30 and delayed recognition of symptoms and treatment due to social isolation. A register study from France indicated that a marked decrease in hospital admissions for acute myocardial infarction was observed immediately after the nationwide lockdown.31 Individuals with a history of CVD are expected to rely more on CVD-related hospital care or CVD-specific regular medical services; however, we found a similar change in patterns even among participants who did not have a history of CVD. It is therefore unlikely that such concern can fully explain our findings. As another explanation, severe SARS-CoV-2 infection has been associated with cardiac injuries,21 which may contribute to the increase in CVD-related mortality. However, after the exclusion of deaths with COVID-19, the increase in CVD-related mortality remained statistically significant in March. Additionally, the null result obtained for April might reflect the greater spread of COVID-19 among individuals who were more prone to fatal cardiovascular events in April than March.
The major merit of our study is the self-comparison analysis, in which the number and rate of CVD-related deaths and hospitalisations during the study period (COVID-19 pandemic) were compared with the corresponding data for a reference period (the same calendar period of the three preceding years) in the same study population (ie, the UK Biobank population). This analysis adjusted inherently for potential confounders that are constant over time, including genetic factors and many environmental factors that did not change greatly within the 4-year period. In addition, other influential factors, such as seasonal variation and ageing of the study population, were well controlled by monthly-based estimations and calculation of standardised expected numbers and SIRs.
Limitations
The notable limitations of this study include the fact that accessibility to the COVID-19 test was largely restricted to inpatients with symptoms before 27 April 2020 in the UK. Consequently, we might have underestimated the number of deaths related to COVID-19 in March and April. In addition, we used hospitalisation for CVD as a proxy for healthcare resources for care of severe CVD. However, we did not have access to cases that did not require admission, including emergency care. This precludes the possibility to separately study CVD-related deaths that occurred outside a hospital, which would have provided a measure of potentially reduced access to healthcare during the COVID-19 pandemic. Finally, the UK Biobank recruited only 5.5% of the target population, and therefore, the cohort may not be entirely representative of the UK population. Moreover, the sample size of this study was relatively small considering that the aim was to measure the impact of the COVID-19 outbreak on cause-specific mortality. Given all these limitations, caution must be exercised when generalising our findings to the entire UK population or other populations.
Conclusions
In conclusion, in the UK Biobank population, we observed a distinct increase in CVD-related deaths at the beginning of the COVID-19 outbreak. In addition to CVD-associated complications of SARS-CoV-2 infections, the reduced hospital capacity and stress reactions to the COVID-19 outbreak might have contributed to the observed increase in CVD-related deaths. Our findings underscore the need for sufficient healthcare resources for CVD and improved instructions from the government to the public about timely healthcare seeking behaviours in the context of public health emergencies, such as the COVID-19 pandemic.
Data availability statement
Data used in this study was from the UK Biobank (http://www.ukbiobank.ac.uk/), which are available to all researchers on making an application. Part of this research was conducted using the UK Biobank Resource under Application 54803.
Ethics statements
Ethics approval
The UK Biobank has full ethical approval from the National Health Service National Research Ethics Service (reference number: 16/NW/0274), and this study was also approved by the biomedical research ethics committee of West China Hospital (reference number: 2020.661).
Acknowledgments
We would like to thank the team members of the West China Biomedical Big Data Center for Disease Control and Prevention for their support.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
FF and HS contributed equally.
Contributors HS and FF were responsible for the study’s concept and design. JW, HY, YH, YS, ZY and YQ were responsible for data and project management. JW, JZ and HY performed the data cleaning and analysis. JW, JZ, HY, UV, FF and HS interpreted the data. JW, JZ, HY, YH, YS, UV, UV, FF and HS drafted and revised the manuscript. All the authors approved the final manuscript as submitted and agree to be accountable for all aspects of the work.
Funding This work is supported by the National Science Foundation of China (No. 81971262 to HS), West China Hospital COVID-19 Epidemic Science and Technology Project (No. HX-2019-nCoV-014 to HS), Sichuan University Emergency Grant (No. 2020scunCoVyingji10002 to HS), EU Horizon2020 Research and Innovation Action Grant (847776 to UV and FF) and NordForsk grant (105668 to UV and FF).
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.