1. Introduction
The SARS-CoV-2 2019 (COVID-19) pandemic has killed millions of people worldwide (
https://en.wikipedia.org/wiki/Template:COVID-19_pandemic_data (accessed on 25 August 2022). From a medical point of view, the situation in the Republic of Bulgaria was not that different from the rest of the world; however, the statistics reveal disturbing tendencies, i.e., the percentage of vaccinated people in Bulgaria has been one of the lowest in Europe and the mortality rate has been one of the biggest in the European Union [
1].
SARS-CoV-2 infection disproportionately affects patients with hypertension, diabetes mellitus, chronic kidney disease (CKD), and/or cardiovascular disease, as well as older people [
2,
3,
4]. Acute kidney injury (AKI) may be caused by many factors, including heart failure, sepsis, hemorrhage, nephro-toxic drugs, as well as by COVID-19. A recent review paper addressed COVID-19-associated AKI [
5]. It is now widely believed that AKI is a frequent and significant complication of COVID-19; however, there is significant variability in its reported incidence and outcomes.
For example, in 2020, Hirsh et al. reported a high prevalence of AKI among hospitalized patients with COVID-19 (36.6%) [
6]. In non-COVID-19 patients, it is estimated that 20% of hospitalized patients deteriorate to AKI and 10% of AKI patients require renal-replacement therapy (RRT). The mortality rate of patients requiring RRT is as high as 50%. Patients recovering from AKI have a higher risk of chronic kidney disease and even end-stage renal disease [
7,
8,
9,
10]. In those infected with COVID-19, major observational studies and meta-analyses have reported AKI incidence rates of 28–34% in inpatients and 46–77% in those in the intensive care unit (ICU). Nevertheless, the prevalence of more severe cases of AKI that require RRT in the ICU appears to have reduced over time: the data from England and Wales show that RRT has declined from 26% at the start of the pandemic to 14% in 2022 [
5].
The risk factors for AKI in COVID-19 are similar to those outside of COVID-19; the presence of underlying CKD is a particularly significant risk factor. Additionally, the existence of new-onset AKI in the ICU independently predicted higher mortality in more severely ill patients, but not in those who experienced the most severe sequential organ failure assessment (SOFA) scores [
11]. Thus, these findings show that the presence of hospital-acquired AKI serves as an early indicator of developing systemic multiorgan failure and of subsequent death. Recently, Sabaghian et al. published a systematic review (44 studies) on COVID-19 and AKI. They identified that the most prevalent comorbidities in patients with COVID-19 and suffering from AKI were diabetes, hypertension, and hyperlipidemia. Of the 44 included studies, twelve reported a history of chronic kidney disease (CKD). The most frequent underlying pathological conditions were focal segmental glomerulosclerosis and acute tubular necrosis. The average length of hospital stay was 19 days and the median duration of need for mechanical ventilation was three days. They concluded that AKI often complexed the COVID-19 hospitalization course and was associated with an increase in disease severity, prolonged duration of hospitalization, and poor outcome [
12].
Diagnosing AKI early and taking proper preventive and therapeutic measures can effectively improve recovery after AKI. At present, the standard for the diagnosis of AKI is based on the serum creatinine level and urine excretion volume, in accordance with the recommendations issued by the Kidney Disease Improving Global Outcomes (KDIGO) in 2012 [
13]. However, serum creatinine and urine output are unspecific and may be delayed, thus obscuring the early diagnosis of AKI. More effective and potential early biomarkers have been discovered with the in-depth studies of AKI pathology, such as neutrophil gelatinase-associated lipocalin (NGAL) in the blood (sNGAL) or urine (uNGAL), urinary kidney-injury molecule-1 (KIM-1), and interleukin-18 (IL-18), serum cystatin C (sCysC), plasma tissue inhibitor of metallo-proteinase 2 (TIMP-2), monocyte chemo-attractant protein (MCP-1), etc. Recently, Menez et al. evaluated 19 urinary biomarkers of injury, inflammation, and repair in 153 hospitalized COVID-19 patients. They found that a twofold higher level of NGAL, MCP-1, and KIM-1 was associated with the highest risk of sustaining a primary composite outcome, i.e., KDIGO stage 3 AKI, requirement for dialysis, or death within 60 days of hospital admission [
14]. In a series of 52 COVID-19 patients, of whom 22 developed AKI, and of which 8 required RRT, Pode Shakked et al. found that the serum creatinine and sCysC measured at presentation into an emergency department (ED) were both highly accurate predictors of AKI and the need for RRT, whereas sNGAL demonstrated an adequate diagnostic parameter [
15]. In a prospective observational study of 57 COVID-19 patients admitted into intensive care, Luther et al. assessed urinary albumin, NGAL, KIM-1, and plasma TIMP-2 at admission: the majority (89%) of patients developed AKI. They found that biomarkers in the urine were increased in the majority of patients, but they did not predict the KDIGO stage reliably [
16].
In this prospective, observational, non-interventional, single-center study, we assessed various plasma and urinary biomarkers of kidney injury (NGAL, KIM-1, IL-18); inflammation (IL-6, C-reactive protein [CRP]); and angiotensin-converting enzyme 2 (ACE2) in COVID-19 patients at ED admission, with the aim of correlating them with the outcomes (mortality, AKI). We also assessed these biomarkers in healthy volunteers and non-COVID-19 CKD patients.
2. Patients and Methods
This is a single-center study conducted at the Alexandrovska Hospital in Sofia (Bulgaria) between February 1 and March 31 2021. In summary, we enrolled consecutive patients who had positive COVID-19 infection and were admitted to the hospital after a positive PCR test for SARS-CoV-2. All cases were validated using a reverse transcription-polymerase chain reaction of combined throat/nose samples. In this study, we only included patients >18 years of age. Patients with coexisting urinary tract infection were excluded [
17].
Of the 120 patients enrolled into our study, 70 had a history of chronic kidney disease (i.e., impaired kidney function with an estimated glomerular-filtration [eGFR] rate of <60 mL/min, though >20 mL/min, i.e.) and none had end-stage renal disease. The eGFR was estimated using the chronic kidney-disease (CKD)-EPI 2021 formula. The other 50 patients had no history of kidney disease and had normal levels of serum creatinine (i.e., females 44–80 µmol/L; males 62–106 µmol/L; eGFR > 60 mL/min/1.73 m2); that group included five patients that had undergone renal transplantation (eGFR of >60 mL/min).
Data on sex, age, comorbidities, and laboratory results of blood drawn were collected on admission to the Emergency Department. The follow-up was performed at 7–10 days after admission. Medical comorbidities, i.e., hypertension, obesity (i.e., body mass index >30 kg/m2), diabetes mellitus, vascular disease, and CKD, which should have already been diagnosed along with the medical history, were recorded. When AKI was present, it was categorized according to the KDIGO criteria.
For all patients with a positive COVID-19 test, a chest CT-scan was performed to assess the disease severity and progression. We used simple chest computed-tomography (CT) scores to evaluate the severity of the lung involvement in COVID-19 patients. Each patient was classified between 0–5: score 0 (0% or none), score 1 (1–5% or minimal), score 2 (6–25% or mild), score 3 (26–49% or moderate), score 4 (50–74% or severe), and score 5 (≥75% or extensive) [
18].
Upon admission into the ED, the patients were informed of the protocol by one of us (R.F.) and, after they had given their informed consent and signed to give a blood sample, the blood and urinary samples were sent to the laboratory to be stored, frozen, until biomarker analyses.
In total, five different biomarkers were assessed: urinary NGAL, KIM-1, IL-18, serum IL-6, and angiotensin-converting enzyme 2 (ACE2). The determination of NGAL was performed with ELISA kits obtained from Thermo Fisher Scientific, while the assays for IL-6, IL-18, and ACE-2 were performed with ELISA kits obtained from BioVendor R and D. KIM-1 was assayed using ELISA kits from MyBioSource, Inc. All of the analyses were accomplished according to the producers’ instructions. For every biomarker, all the patients’ samples were thawed and assessed the same day by the same technician.
The biomarkers were also assessed in two control groups: 20 healthy volunteers taking no medication and 20 CKD patients. The latter patients needed to have a well-characterized CKD and were followed-up in our outpatient nephrology clinic. In addition, they needed to be in a stable condition. After having given their informed consent to participate in the study, both the healthy volunteers and CKD controls had a PCR-test for SARS-CoV-2 that had to be negative.
For testing ACE-2 (from serum), we used the following kit: Catalogue number RAG006R, produced by: BioVendor–Laboratorní medicína a.s. Karásek 1767/1, 621 00 Brno, Czech Republic. The normal ranges are 0.0625 ng/mL–4 ng/mL. For the IL-6 (from serum) assessment, a kit from Catalogue number RD194015200R (produced by BioVendor–Laboratorní medicína a.s. Karásek 1767/1, 621 00 Brno, Czech Republic) was used. Probes from all the healthy control patients were assessed: the lowest standard result was 1.25 pg/mL, and three samples were measured between 1.25 and 5 pg/mL. Regarding NGAL (from urine), we used the following kit: Catalogue number BMS2202, produced by Thermo Fisher Scientific, Campus Vienna Biocenter 2, 1030 Vienna, Austria. The measured values of our healthy controls were 21–48 ng/mL. With respect to KIM-1 (from urine), we used the kit from Catalogue number MBS020924, produced by: MyBioSource, Inc., San Diego, CA 92195-3308, USA. The measured values from our healthy controls were 1.5–2.1 ng/mL. Finally, for interleukin-18 (from urine), we used the kit from Catalogue number RAF143R, produced by: BioVendor–Laboratorní medicína a.s. Karásek 1767/1, 621 00 Brno, Czech Republic. The measured values from our healthy controls were 27.1–100.5 pg/mL plus one outlier (with a result of 189.7 pg/mL).
The study was conducted according to the guidelines of the Declaration of Helsinki and was approved by the ethical committee KENIMUS at the Medical University of Sofia, Bulgaria, with Protocol №12/31.05.2022. All of the data are available upon request from the corresponding author.
2.1. Statistical Analysis
Categorical parameters were described by absolute and relative (percentage) frequencies. Continuous parameters were described by arithmetic means and standard deviations (SD), and median, minimum, and maximum values. The distribution of the continuous parameters was checked for normality using the Shapiro–Wilk test.
2.2. Methods for Testing the Post hoc Hypotheses
To compare the continuous parameters in two related (paired) groups, the Wilcoxon two-sample test was applied, and the approximation of the Student’s t-statistic (t-approximation) with a continuity correction of 0.5 was used to determine statistical significance. In addition, the sign test was used where appropriate.
Comparisons between the independent (unrelated) groups (CKD vs. no CKD) were made after adjustment for baseline differences.
Due to the heterogeneity and non-normality of the data distribution, non-parametric ANOVA (Kruskal-Wallis) was used to compare more than two groups.
The linear association between the continuous normally distributed variables was estimated by Pearson’s correlation coefficient. For the continuous non-normal parameters, Spearman’s coefficient was used. Bi-serial coefficient was used to explore the relation between the non-metric variables.
2.3. Method Used for Data Modelling
Binary logistic regression was used to model the relationship between the output (COVID-19-related death) as a dependent variable and the main parameters. A model is presented for death. In addition, the odds ratios and forest plots are shown. For decision making, a significance level of 5% was used.
The SAS® package version 9.4 (SAS Institute Inc., SAS 9.4 Help and Documentation, Cary, NC, USA: SAS Institute Inc., 2015–2022) was used for the calculations and the graphical presentations.
3. Results
From the total of 160 persons, 75% were confirmed with COVID-19 (120 patients in total), of which 70 (58.3%) had a history of CKD. The other 40 persons (25%) that had no history of COVID-19 were used as controls and were divided into two separate groups: 20 patients (50%) had a history of CKD, whereas the other 20 (50%) were totally healthy (i.e., no history of CKD or any other type of co-morbidity).
The median age of the CKD patients that had a positive test for COVID-19 was 56.8 years, whereas for the non-CKD COVID-19 patients, it was 65.9 years. The gender ratio was 50% in both groups (see
Table 1). For the CKD patients without COVID-19, the median age was 66.1 years; the gender ratio was 11 females (55%) to 10 males (45%). For the healthy control group, the median age was 36.8 years, and the gender ratio was equal: 10 male and 10 female patients. Overall, in the COVID-19 patients, the serum-creatinine level on admission was 119.0 μmol/L (57.0–930.0 μmol/L) for the CKD group and 79.0 μmol/L (50.0–295.0 μmol/L) for the non-CKD group. In addition, it was elevated over the baseline in 58.3% of cases.
For the non-COVID-19 CKD patients, the median serum creatinine was 109.1 μmol/L (62.0–188.0 μmol/L); it was elevated in 60% of cases. No patients in the healthy control group had creatinine levels over the baseline, i.e., normal ranges for males are 62–106 μmol/L and for females 44–80 μmol/L. The mean value of eGFR on admission was 80.4 mL/min/1.73 m2 for the non-CKD COVID-19 patients, whilst it was 47.9 mL/min/1.73 m2 for the CKD COVID-19 patients (p-values < 0.0001). For the CKD patients without COVID-19, the eGFR was 62.3 mL/min/1.73 m2, whilst the eGFR was at 111.1 mL/min/1.73 m2 for the healthy control group.
There were significant differences (<0.0001) between the CRP values across the four groups. All of the COVID-19 patients had elevated CRP levels: 75.7 mg/L (SD = 73.7) in the CKD group and 53.9 mg/L (SD = 59.5) in the non-CKD group. For the COVID-19-negative patients, CRP was at 7.0 mg/L (SD = 6.7) in the CKD group and 1.7 mg/L (SD =1.6) in the healthy controls. The upper limit for CRP was ~5 mg/L.
The five biomarkers statistically differed across the four subgroups (see
Table 2); thus, we made comparisons between each subgroup using paired Kruskal-Wallis analysis.
We found the following statistically significant changes:
- -
CKD and COVID-19 vs. healthy controls—significant changes for IL-6, ACE2 enzyme, NGAL, and IL-18
- -
Non-CKD and COVID-19 vs. healthy controls—significant changes for IL-6, NGAL, and IL-18
- -
CKD only vs. healthy controls—significant changes for IL-6, ACE2 enzyme, and IL-18
- -
CKD and COVID-19 vs. CKD only—significant changes for ACE2 enzyme and NGAL
Acute kidney injury was a frequent event, i.e., it occurred in 38 patients (27.3%), but was registered only in the COVID-19 positive patients, of whom 31 were in the CKD group (44.3%), and 7 (14%) were in the non-CKD group (p-value = 0.0006). All of the patients that had AKI could be divided into three stages, using the KDIGO criteria: from all the patients with AKI, 30 patient (i.e., 78.9%) had AKI Stage 3; 4 patients had AKI Stage 2 (10.5%); while the remainder (3 patients or 7.8%) had AKI stage 1. From our analysis, the AKI was assessed as a risk factor in connection to the mortality rate: overall, the hospital mortality was 14.4% (23 patients) of the 160 patients in our group, of which 19 patients, or 82.6% (p = 0.009), had AKI (any stage by KDIGO).
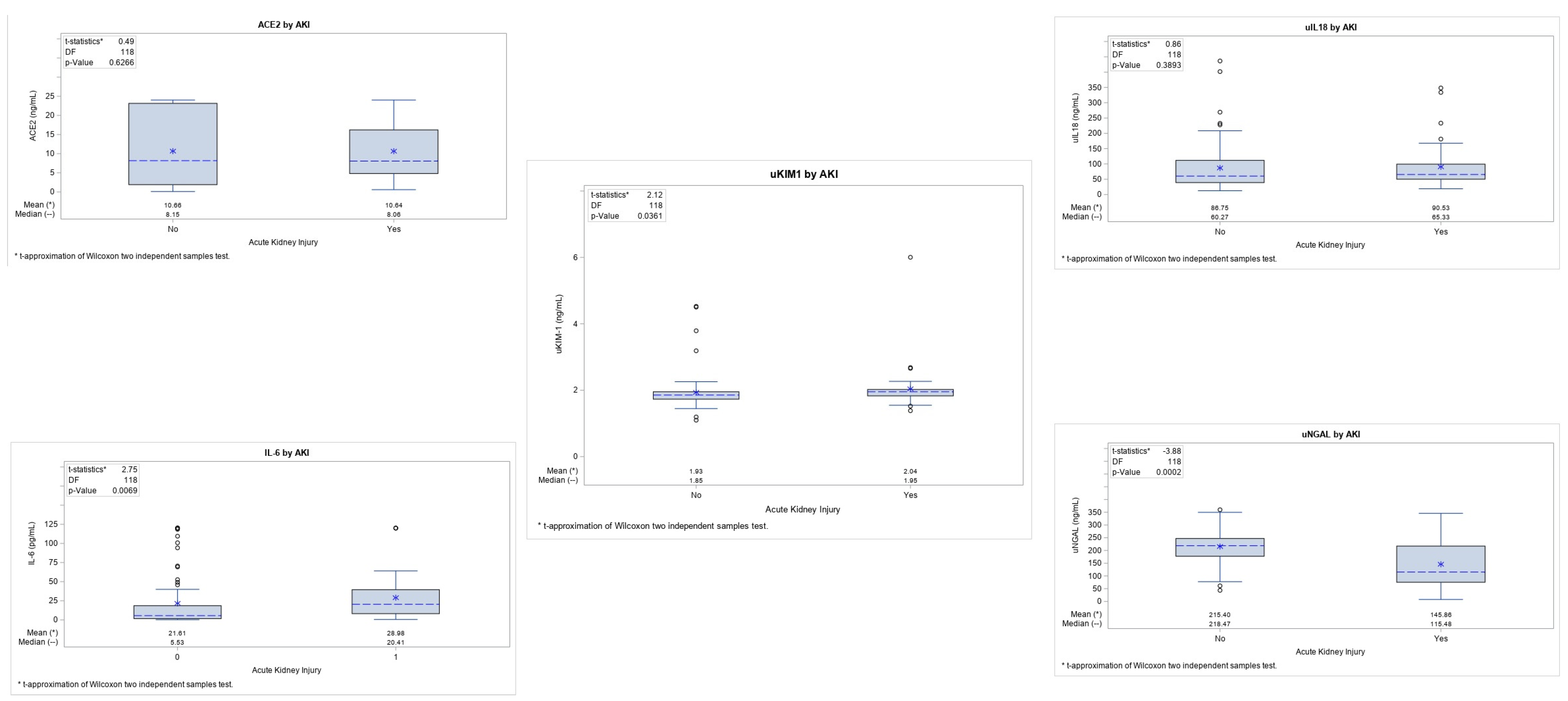
Analysis was performed to assess the correlations between the biomarkers and the incidence of AKI in each of the COVID-19 groups. Amongst the biomarkers, we found that the levels of IL-6 (
p = 0.006) and uKIM-1 (
p = 0.03) were significantly higher in those patients that presented with AKI, whilst the results for the uNGAL were significantly lower (
p-value = 0.0002). Conversely, there was no significance for the other two biomarkers: ACE2 enzyme (
p = 0.62) and uIL-18 (
p = 0.38) (
Figure 2). However, none of the biomarkers were able to predict AKI.
Further correlation analyses were performed with all five biomarkers in relation to the inflammation biomarkers and the degree of lung involvement, thus determining whether any of these criteria were associated with a fatal outcome (
Table 4).
The most significant results were found for IL-6, which correlated with the number of leukocytes and neutrophils, and with the degree of lung involvement (as assessed by the Severity Score, ventilation, and mortality). The only non-significant result for IL-6 was with CRP. The biomarkers KIM-1 and CRP also showed a significant correlation. IL-18 showed an association with the neutrophil count and the extent of lung involvement.
We observed that having high baseline IL-6 levels was associated with subsequent ventilation requirement. Indeed, the patients that required subsequent ventilation had IL-6 levels ranging between 25 and 120 pg/mL (median 45.2 pg/mL); there were two outliers under 25 pg/mL. In the COVID-19 patients, 27 patients had IL-6 results of >25 pg/mL on admission and, later, 19 required mechanical ventilation (70.4%).
All of the patients that did not survive the SARS-CoV-2 infection were in the ICU and died from advanced pneumonia; none of these patients had a history of any kind of cardiovascular incident while in the ICU.
All of the COVID-19 patients had received a chest CT-scan upon AD admission. Every CT-scan was graded according to the severity score (0–5). For our patients, the results ranged between 0–4. We grouped the patients into two categories: 0–2 score (n = 102) and 3–4 (n = 18).
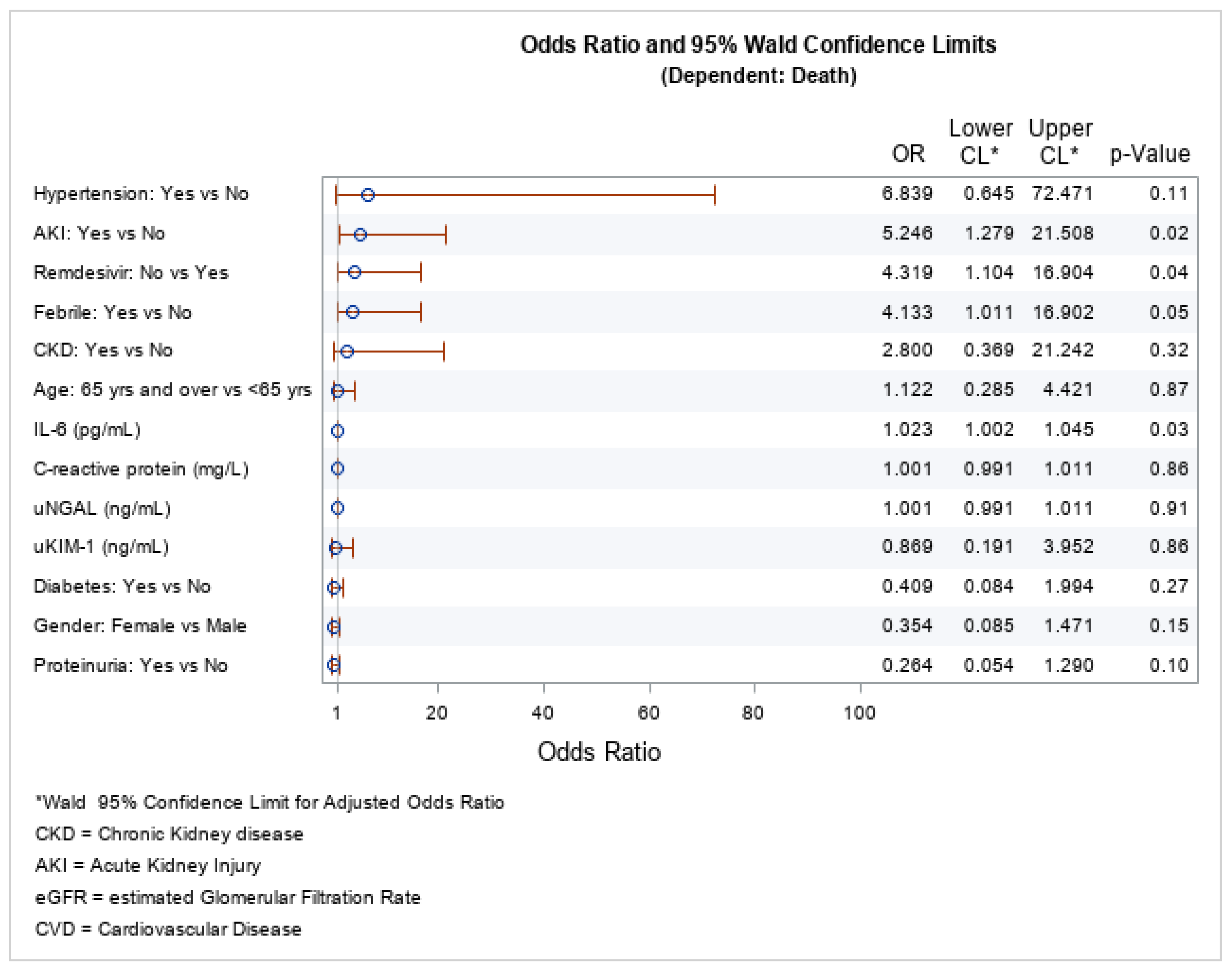
We included the following factors in the logistic regression model as important: Gender, Hypertension, AKI, Treatment with Remdesivir, Febrile, CKD, age, IL-6, CRP, uNGAL, uKIM-1, Diabetes, and Proteinuria.
The logistic regression for the mortality risk factors showed that the statistically significant factors were AKI, IL-6 levels, and not being treated with remdesivir (see
Figure 3). AKI was a negative prognostic factor for COVID-19 infection, i.e., it increased the mortality [OR = 5.246 (95% CI: 1.279–21.508);
p = 0.02], as was not being treated with remdesevir [OR = 4.319 (95% CI: 1.104–16.904);
p = 0.04] and having increased levels of IL-6 [OR = 1.023 (95% CI: 1.002–1.045);
p = 0.03]. The other biomarkers (KIM-1, and NGAL) included in the model did not predict death.
4. Discussion
In this observational, prospective study that included COVID-19 patients with or without CKD, we evaluated the added value of blood and urinary biomarkers assessed at hospital admission with the aim to determine whether they could predict subsequent death and AKI. These biomarkers included urinary NGAL, KIM-1, IL-18, and serum IL-6, CRP, and ACE2. Only the IL-6 level was independently associated with death. A recent systematic review and meta-analysis has shown that IL-6 significantly increases the risk of COVID-19 severity (adjusted OR = 1.0284; 95% CI 1.0130–1.0441;
p = 0.0003) and mortality (aOR = 1.0076; 95% CI 1.0004–1.0148;
p = 0.04; adjusted hazard ratio (aHR) = 1.0036; 95% CI 1.0010–1.0061;
p = 0.006) [
19]. Another systematic review of 147 studies has shown that deceased COVID-19 patients had 42.1 times higher mean concentrations of IL-6 than patients that survived. The IL-6 level was significantly increased in those that died (MD: 42.11;
p < 0.001; 95% CI: 36.86, 47.36) [
20].
We also found that not giving remdesivir therapy upon admission into the ED independently increased the risk of death by more than four-fold (OR = 4.319; 95% CI. 1.104–16.904;
p = 0.04). Indeed, a recent randomized controlled trial has demonstrated that among non-hospitalized COVID-19 patients that had a high risk for its progression, a three day course of remdesivir had an acceptable safety profile and resulted in an 87% lower risk of hospitalization or death than a placebo [
21]. In addition, a recent systematic review and meta-analysis has shown that there is a high probability that remdesivir reduces mortality for nonventilated patients with COVID-19 and that require supplemental oxygen therapy [
22]. However, the World Health Organization (WHO) Solidarity Trial Consortium has demonstrated that remdesivir has no significant effect on patients with COVID-19 who were already being ventilated [
23].
We found that AKI independently increased, by more than 5-fold (OR 5.246 (95%CI 1.279–21.508);
p = 0.02), the risk of COVID-19-associated death. A recent study from the United States (US) has shown that out of a total cohort of 306,061 COVID-19 patients, 126,478 (41.0 %) had AKI. The AKI patients had higher mortality compared to those without AKI; the incidence of AKI was highest at the beginning of the pandemic (49.3%), but later reduced (40.6%). The severity of AKI was also associated with mortality [
24]. Similarly, the incidence of more severe AKI that requires renal-replacement therapy in an ICU appears to have declined over time: the data from England and Wales show that RRT declined from 26% at the start of the pandemic to 14% in 2022 [
5].
In our study, we also looked for early biomarkers that might predict COVID-19-associated AKI. Urinary interleukin-18 (uIL-18), as well as ACE2, were not associated with AKI. A recent systematic review evaluated the value of uIL-18 to predict AKI. The estimated sensitivity and specificity of uIL-18 for the diagnosis of AKI were 0.64 (95% confidence interval (CI): 0.54–0.73) and 0.77 (95%CI: 0.71–0.83), respectively. Subgroup analysis showed that uIL-18 in pediatric patients was more effective at predicting AKI than in adults [
25]. Saygili et al. assessed uIL-18 in 71 COVID-19 children, of whom 12 had AKI. Compared to healthy control children, uIL-18 was significantly increased; however, only 4 of 12 AKI children had increased levels of uIL-18 [
26]. The actions of angiotensin-converting enzyme 2 (ACE2) oppose those of the renin-angiotensin-aldosterone system. The SARS-CoV-2 cellular entry receptor is ACE2. ACE2 may be a cytoprotectant in some tissues. It has been shown that renal ACE2 expression is decreased in ischemic AKI [
27]. We found that the ACE2 blood levels were significantly higher in the COVID-19 patients compared to the non-COVID-19 patients and healthy volunteers. In addition, amongst the CKD patients, the ACE2 levels were significantly higher in the COVID-19 positive group compared to the COVID-19-negative patients.
We found that the IL-6 levels were significantly higher in the COVID-19 patients and in the non-COVID-19 CKD patients compared to the healthy volunteers. In the COVID-19 patients, those that had AKI had significantly higher IL-6 levels compared to those that had no AKI (20.4 vs. 5.53 pg/mL). Wang et al. have shown that the L-6 level had significant positive correlations with serum creatinine and blood urea nitrogen [
28]. In the patients with COVID-19, the serum levels of IL-6 were elevated in those with AKI [
29]. In addition, the serum levels of IL-6 can also predict the clinical outcomes of AKI as it is significantly reduced in those where AKI is eliminated after effective treatment [
30]. Finally, levels of IL-6 of >35 pg/mL may indicate a risk of respiratory failure [
31] in the context of a COVID-19 infection. Herein, we confirm that result, i.e., out of 27 COVID-19 patients that had IL-6 results of >25 pg/mL at admission, later, 19 (70.4%) of these required mechanical ventilation.
KIM1 expression is dramatically up-regulated in kidney post-ischaemia/reperfusion injury in rats, as well as in rodent models of drug-induced AKI. Its expression is mainly upregulated in proximal tubule cells, both in rodents and in man. KIM-1 plays an important role in kidney recovery and tubular regeneration [
32]. In a prospective study, 19 urinary biomarkers were assessed to predict AKI in COVID-19 patients; among them, twofold higher levels of NGAL (HR, 1.34 [95% CI, 1.14–1.57]), monocyte chemoattractant protein (MCP-1) (HR, 1.42 [95% CI, 1.09–1.84]), and KIM-1 (HR, 2.03 [95% CI, 1.38–2.99]) were associated with the highest risk of sustaining a primary composite outcome (KDIGO stage 3 AKI, requirement for dialysis, or death within 60 days of hospital admission) (14). However, individual biomarkers provided moderate discrimination, and biomarker combinations improved the discrimination from the primary outcome. We observed that uKIM1 in the COVID-19 patients was significantly higher in those that had AKI versus the others; however, the absolute difference was very small (1.95 vs. 1.85 ng/mL
p = 0.03).
Neutrophil gelatinase-associated lipocalin (NGAL) concentrations in urine or plasma may identify patients with a high risk for AKI in clinical research and practice [
33]. A recent systematic review has shown that NGAL appeared to have a predictive value irrespective of age, from newborn to 78 years. NGAL levels can accurately predict the outcome and severity of AKI occurring in several disease processes, including contrast-induced AKI during cardiac surgery, kidney-transplant rejection, chronic heart failure, and systemic inflammation in critically ill patients, even though the significance of NGAL is highly variable across studies [
34]. In the setting of COVID-19 patients, a prospective cohort observational study consisting of 444 consecutive patients evaluated uNGA at hospital admission. They found that the levels were associated with AKI diagnosis (267 ± 301 vs. 96 ± 139 ng/mL,
p < 0.0001) and staging; uNGAL levels >150 ng/mL had 80% specificity and 75% sensitivity to diagnose AKI stages 2 to 3. At admission, the uNGAL level was quantitatively associated with prolonged AKI, dialysis, shock, prolonged hospitalization, and in-hospital death, even when the admission serum-creatinine level was not elevated [
35].
Conversely, low uNGAL levels at admission ruled out stages 2–3 AKI (negative predictive value: 0.95, 95% CI: 0.92–0.97) and the need for dialysis (negative predictive value: 0.98, 95% CI: 0.96–0.99). In contrast, in a prospective cohort of 153 COVID-19 patients, Menez et al. evaluated the utility of urinary biomarkers such as NGAL, KIM1, MCP1 to predict AKI. They observed that individual biomarkers provided moderate discrimination and biomarker combinations improved the discrimination for the primary outcome [
14]. In our study, we found that the uNGAL in healthy controls and in non-COVID-19 patients was very similar; however, it was almost five times higher in those with COVID-19. However, surprisingly, the uNGAL was significantly lower in those that will develop AKI as compared to those that will not (115.48 vs. 218.47 ng/mL;
p = 0.0002). We have no explanation for this unexpected result.
We looked at whether the biomarkers we evaluated were associated with the chest-CT severity score (CTSS). Valk et al. found that, despite a poor prognostic capacity, CTSS was associated with ICU mortality [
36]. Almasi Nokiani et al. found that CTSS is an excellent tool in triage and prognostication in patients with COVID-19 aged ≥65 years, but is of limited value for younger patients [
37]. Some studies have found a positive correlation between the extent of CT lung involvement and short-term mortality [
38,
39]. In addition, there was a significant association between the CTSS and hospital admission, ICU admission, and 30 day mortality [
40]. In addition, patients with a score of three had a higher risk for complications and a fatal outcome [
41]. In our study, we found that the patients with COVID-19 at admission with a CTSS score of —between three and four had a mortality rate of 88.9%, compared to only 6.8% in those where the CTSS was —between zero and two (
p-value < 0.0001). In addition, we found that some biomarkers were significantly associated with the CTSS score, i.e., uIL-18, uNGAL, and serum IL-6. In the literature, we were not able to find other such correlations. Herold et al. reported that the maximal level of IL-6, followed by the CRP level, was highly predictive for the need of mechanical ventilation, but these patients did not have a chest CT-scan at admission [
31]. Therefore, taking into account all of our results, we found that patients that had higher IL-6 levels on admission and had a chest CT severity score of >3 had a much greater risk of needing mechanical ventilation. Sadly, all of the ventilated patients from our group have passed away.
Our study has some limitations: we only had 120 COVID-19 patients; however, they were very well phenotyped. In addition, the biomarkers were only assessed at admission in the ED, but not subsequently; this would have been of interested in order to study their kinetics. This might explain, in particular, why they were of very limited value, except with the IL-6 levels.
5. Conclusions
In this prospective case-series of 120 COVID-19 patients, the assessment at ED admission of the urinary biomarkers for kidney injury (NGAL, KIM-1, IL-18) was of limited value to predict AKI. Conversely, serum IL-6 was an independent predictor of death. Finally, IL-6 levels were associated with needing ventilation.
Author Contributions
Conceptualization, R.F. and L.R.; Methodology, R.F. and L.R.; Software, L.R. and K.K.; Validation, R.F. and L.R.; Formal analysis, R.F. and L.R.; Investigation, R.F., L.R., M.L., B.B., J.H. and D.S.; Resources, R.F. and L.R.; Data curation, R.F., L.R. and K.K.; Writing—original draft preparation, R.F.; writing—review and editing, L.R.; Visualization, R.F., M.L., B.B., J.H. and D.S.; supervision, L.R.; project administration, R.F. and L.R.; funding acquisition, R.F. and L.R. All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded by “SANTÉ ET ESPOIR” FRANCE-BULGARIE, Published on: February 3, 2007, with publication №: 20070005, with registered office: 2, rue du Congo, 31500 Toulouse, with new address: 6, chemin Pouciquot, 31520 Ramonville Saint-Agne, France.
Institutional Review Board Statement
The research was approved from the ethical committee KENIMUS of the Medical University of Sofia, Bulgaria with Protocol №12/31.05.2022.
Informed Consent Statement
Informed consent was obtained from all of the subjects involved in the study.
Data Availability Statement
The data are available upon request.
Conflicts of Interest
The authors declare no conflict of interest.
References
- National Statistical Institute of Republic of Bulgaria; COVID-19 Statistical Data. Available online: https://www.nsi.bg/en/content/18120/basic-page/covid-19 (accessed on 1 July 2022).
- Wang, X.; Fang, X.; Cai, Z.; Wu, X.; Gao, X.; Min, J.; Wang, F. Comorbid Chronic Diseases and Acute Organ Injuries Are Strongly Correlated with Disease Severity and Mortality among COVID-19 Patients: A Systemic Review and Meta-Analysis. Research 2020, 2020, 2402961. [Google Scholar] [CrossRef] [Green Version]
- Shahid, Z.; Kalayanamitra, R.; McClafferty, B.; Kepko, D.; Ramgobin, D.; Patel, R.; Aggarwal, C.S.; Vunnam, R.; Sahu, N.; Jain, R.; et al. COVID-19 and Older Adults: What We Know. J. Am. Geriatr. Soc. 2020, 68, 926–929. [Google Scholar] [CrossRef] [Green Version]
- Chung, E.Y.; Palmer, S.C.; Natale, P.; Krishnan, A.; Cooper, T.E.; Saglimbene, V.M.; Ruospo, M.; Au, E.; Jayanti, S.; Liang, A.; et al. Incidence and Outcomes of COVID-19 in People With CKD: A Systematic Review and Meta-analysis. Am. J. Kidney Dis. 2021, 78, 804–815. [Google Scholar] [CrossRef]
- Matsumoto, K.; Prowle, J.R. COVID-19-associated AKI. Curr. Opin. Crit. Care 2022, 28, 630–637. [Google Scholar] [CrossRef]
- Hirsch, J.S.; Ng, J.H.; Ross, D.W.; Sharma, P.; Shah, H.H.; Barnett, R.L.; Hazzan, A.D.; Fishbane, S.; Jhaveri, K.D.; on behalf of theNorthwell COVID-19 Research Consortium and theNorthwell Nephrology COVID-19 Research Consortium. Acute kidney injury in patients hospitalized with COVID-19. Kidney Int. 2020, 98, 209–218. [Google Scholar] [CrossRef] [PubMed]
- Wen, Y.; Parikh, C.R. The Aftermath of AKI: Recurrent AKI, Acute Kidney Disease, and CKD Progression. J. Am. Soc. Nephrol. 2021, 32, 2–4. [Google Scholar] [CrossRef] [PubMed]
- Koyner, J.L. Subclinical Acute Kidney Injury Is Acute Kidney Injury and Should Not Be Ignored. Am. J. Respir. Crit. Care Med. 2020, 202, 786–787. [Google Scholar] [CrossRef]
- Kellum, J.A.; Romagnani, P.; Ashuntantang, G.; Ronco, C.; Zarbock, A.; Anders, H.-J. Acute kidney injury. Nat. Rev. Dis. Prim. 2021, 7, 52. [Google Scholar] [CrossRef] [PubMed]
- Huang, C.-T.; Liu, K.D. Exciting developments in the field of acute kidney injury. Nat. Rev. Nephrol. 2020, 16, 69–70. [Google Scholar] [CrossRef]
- Regolisti, G.; Maggiore, U.; Di Mario, F.; Gentile, M.; Benigno, G.D.; Gandolfini, I.; Pistolesi, V.; Morabito, S.; Barbagallo, M.; Picetti, E.; et al. The Association of New-Onset Acute Kidney Injury and Mortality in Critically Ill Patients With COVID-19 With Less Severe Clinical Conditions at Admission: A Moderation Analysis. Front. Med. 2022, 9, 799298. [Google Scholar] [CrossRef]
- Sabaghian, T.; Kharazmi, A.B.; Ansari, A.; Omidi, F.; Kazemi, S.N.; Hajikhani, B.; Vaziri-Harami, R.; Tajbakhsh, A.; Omidi, S.; Haddadi, S.; et al. COVID-19 and Acute Kidney Injury: A Systematic Review. Front. Med. 2022, 9, 705908. [Google Scholar] [CrossRef]
- Ostermann, M.; Bellomo, R.; Burdmann, E.A.; Doi, K.; Endre, Z.H.; Goldstein, S.L.; Kane-Gill, S.L.; Liu, K.D.; Prowle, J.R.; Shaw, A.D.; et al. Controversies in acute kidney injury: Conclusions from a Kidney Disease: Improving Global Outcomes (KDIGO) Conference. Kidney Int. 2020, 98, 294–309. [Google Scholar] [CrossRef] [PubMed]
- Menez, S.; Moledina, D.G.; Thiessen-Philbrook, H.; Wilson, F.P.; Obeid, W.; Simonov, M.; Yamamoto, Y.; Corona-Villalobos, C.P.; Chang, C.; Garibaldi, B.T.; et al. Prognostic Significance of Urinary Biomarkers in Patients Hospitalized With COVID-19. Am. J. Kidney Dis. 2022, 79, 257–267.e1. [Google Scholar] [CrossRef]
- Shakked, N.P.; de Oliveira, M.H.S.; Cheruiyot, I.; Benoit, J.L.; Plebani, M.; Lippi, G.; Benoit, S.W.; Henry, B.M. Early prediction of COVID-19-associated acute kidney injury: Are serum NGAL and serum Cystatin C levels better than serum creatinine? . Clin. Biochem. 2022, 102, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Luther, T.; Bülow-Anderberg, S.; Larsson, A.; Rubertsson, S.; Lipcsey, M.; Frithiof, R.; Hultström, M. COVID-19 patients in intensive care develop predominantly oliguric acute kidney injury. Acta Anaesthesiol. Scand. 2020, 65, 364–372. [Google Scholar] [CrossRef]
- Filev, R.; Rostaing, L.; Lyubomirova, M.; Bogov, B.; Kalinov, K.; Svinarov, D. COVID-19 Infection in Chronic Kidney Disease Patients in Bulgaria: Risk Factors for Death and Acute Kidney Injury. J. Pers. Med. 2022, 12, 1676. [Google Scholar] [CrossRef]
- Abdel-Tawab, M.; Basha, M.A.A.; Mohamed, I.A.I.; Ibrahim, H.M. A simple chest CT score for assessing the severity of pulmonary involvement in COVID-19. Egypt. J. Radiol. Nucl. Med. 2021, 52, 149. [Google Scholar] [CrossRef]
- Halim, C.; Mirza, A.F.; Sari, M.I. The Association between TNF-α, IL-6, and Vitamin D Levels and COVID-19 Severity and Mortality: A Systematic Review and Meta-Analysis. Pathogens 2022, 11, 195. [Google Scholar] [CrossRef]
- Jafrin, S.; Aziz, A.; Islam, M.S. Elevated Levels of Pleiotropic Interleukin-6 (IL-6) and Interleukin-10 (IL-10) are Critically Involved With the Severity and Mortality of COVID-19: An Updated Longitudinal Meta-Analysis and Systematic Review on 147 Studies. Biomark. Insights 2022, 17, 11772719221106600. [Google Scholar] [CrossRef]
- Gottlieb, R.L.; Vaca, C.E.; Paredes, R.; Mera, J.; Webb, B.J.; Perez, G.; Oguchi, G.; Ryan, P.; Nielsen, B.U.; Brown, M.; et al. Early Remdesivir to Prevent Progression to Severe COVID-19 in Outpatients. N. Engl. J. Med. 2022, 386, 305–315. [Google Scholar] [CrossRef]
- Angamo, M.T.; Mohammed, M.A.; Peterson, G.M. Efficacy and safety of remdesivir in hospitalised COVID-19 patients: A systematic review and meta-analysis. Infection 2022, 50, 27–41. [Google Scholar] [CrossRef]
- Remdesivir and three other drugs for hospitalised patients with COVID-19: Final results of the WHO Solidarity randomised trial and updated meta-analyses. Lancet 2022, 399, 1941–1953. [CrossRef]
- Masthead; Yoo, Y.J.; Wilkins, K.J.; Alakwaa, F.; Liu, F.; Torre-Healy, L.A.; Krichevsky, S.; Hong, S.S.; Sakhuja, A.; Potu, C.K.; et al. COVID-19-associated AKI in hospitalized US patients: Incidence, temporal trends, geographical distribution, risk factors and mortality. medRxiv 2022. [Google Scholar] [CrossRef]
- Qin, Z.; Li, H.; Jiao, P.; Jiang, L.; Geng, J.; Yang, Q.; Liao, R.; Su, B. The value of urinary interleukin-18 in predicting acute kidney injury: A systematic review and meta-analysis. Ren. Fail. 2022, 44, 1717–1731. [Google Scholar] [CrossRef]
- Saygili, S.; Canpolat, N.; Cicek, R.Y.; Agbas, A.; Yilmaz, E.K.; Sakalli, A.A.K.; Aygun, D.; Akkoc, G.; Demirbas, K.C.; Konukoglu, D.; et al. Clinical and subclinical acute kidney injury in children with mild-to-moderate COVID-19. Pediatr. Res. 2022, 7, 1–7. [Google Scholar] [CrossRef]
- Nath, K.A.; Singh, R.D.; Grande, J.P.; Garovic, V.D.; Croatt, A.J.; Ackerman, A.W.; Barry, M.A.; Agarwal, A. Expression of ACE2 in the Intact and Acutely Injured Kidney. Kidney360 2021, 2, 1095–1106. [Google Scholar] [CrossRef]
- Wang, J.; Yang, X.; Li, Y.; Huang, J.-A.; Jiang, J.; Su, N. Specific cytokines in the inflammatory cytokine storm of patients with COVID-19-associated acute respiratory distress syndrome and extrapulmonary multiple-organ dysfunction. Virol. J. 2021, 18, 117. [Google Scholar] [CrossRef]
- Joseph, A.; Zafrani, L.; Mabrouki, A.; Azoulay, E.; Darmon, M. Acute kidney injury in patients with SARS-CoV-2 infection. Ann. Intensive Care. 2020, 10, 117. [Google Scholar] [CrossRef]
- Villa, G.; Romagnoli, S.; De Rosa, S.; Greco, M.; Resta, M.; Montin, D.P.; Prato, F.; Patera, F.; Ferrari, F.; Rotondo, G.; et al. Blood purification therapy with a hemodiafilter featuring enhanced adsorptive properties for cytokine removal in patients presenting COVID-19: A pilot study. Crit. Care 2020, 24, 605. [Google Scholar] [CrossRef]
- Herold, T.; Jurinovic, V.; Arnreich, C.; Lipworth, B.J.; Hellmuth, J.C.; von Bergwelt-Baildon, M.; Klein, M.; Weinberger, T. Elevated levels of IL-6 and CRP predict the need for mechanical ventilation in COVID-19. J. Allergy Clin. Immunol. 2020, 146, 128–136.e4. [Google Scholar] [CrossRef]
- Schrezenmeier, E.V.; Barasch, J.; Budde, K.; Westhoff, T.; Schmidt-Ott, K.M. Biomarkers in acute kidney injury—Pathophysiological basis and clinical performance. Acta Physiol. 2017, 219, 556–574. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Albert, C.; Zapf, A.; Haase, M.; Röver, C.; Pickering, J.W.; Albert, A.; Bellomo, R.; Breidthardt, T.; Camou, F.; Chen, Z.; et al. Neutrophil Gelatinase-Associated Lipocalin Measured on Clinical Laboratory Platforms for the Prediction of Acute Kidney Injury and the Associated Need for Dialysis Therapy: A Systematic Review and Meta-analysis. Am. J. Kidney Dis. 2020, 76, 826–841.e1. [Google Scholar] [CrossRef] [PubMed]
- Marakala, V. Neutrophil gelatinase-associated lipocalin (NGAL) in kidney injury—A systematic review. Clin. Chim. Acta 2022, 536, 135–141. [Google Scholar] [CrossRef] [PubMed]
- Xu, K.; Shang, N.; Levitman, A.; Corker, A.; Kudose, S.; Yaeh, A.; Neupane, U.; Stevens, J.; Sampogna, R.; Mills, A.M.; et al. Elevated Neutrophil Gelatinase-Associated Lipocalin Is Associated With the Severity of Kidney Injury and Poor Prognosis of Patients With COVID-19. Kidney Int. Rep. 2021, 6, 2979–2992. [Google Scholar] [CrossRef]
- Valk, C.M.; Zimatore, C.; Mazzinari, G.; Pierrakos, C.; Sivakorn, C.; Dechsanga, J.; Grasso, S.; Beenen, L.; Bos, L.D.J.; Paulus, F.; et al. The RALE Score Versus the CT Severity Score in Invasively Ventilated COVID-19 Patients—A Retrospective Study Comparing Their Prognostic Capacities. Diagnostics 2022, 12, 2072. [Google Scholar] [CrossRef]
- Almasi Nokiani, A.; Shahnazari, R.; Abbasi, M.A.; Divsalar, F.; Bayazidi, M.; Sadatnaseri, A. CT-severity score in COVID-19 patients: For whom is it applicable best? Caspian J. Intern. Med. 2022, 13 (Suppl. S3), 228–235. [Google Scholar] [CrossRef]
- Colombi, D.; Bodini, F.C.; Petrini, M.; Maffi, G.; Morelli, N.; Milanese, G.; Silva, M.; Sverzellati, N.; Michieletti, E. Well-aerated Lung on Admitting Chest CT to Predict Adverse Outcome in COVID-19 Pneumonia. Radiology 2020, 296, E86–E96. [Google Scholar] [CrossRef] [Green Version]
- Gervaise, A.; Bouzad, C.; Peroux, E.; Helissey, C. Acute pulmonary embolism in non-hospitalized COVID-19 patients referred to CTPA by emergency department. Eur. Radiol. 2020, 30, 6170–6177. [Google Scholar] [CrossRef]
- Lieveld, A.W.E.; Azijli, K.; Teunissen, B.P.; van Haaften, R.M.; Kootte, R.S.; Van Den Berk, I.A.H.; van der Horst, S.F.B.; de Gans, C.; van de Ven, P.M.; Nanayakkara, P.W.B. Chest CT in COVID-19 at the ED: Validation of the COVID-19 Reporting and Data System (CO-RADS) and CT Severity Score: A Prospective, Multicenter, Observational Study. Chest 2021, 159, 1126–1135. [Google Scholar] [CrossRef]
- Machnicki, S.; Patel, D.; Singh, A.; Talwar, A.; Mina, B.; Oks, M.; Makkar, P.; Naidich, D.; Mehta, A.; Hill, N.S.; et al. The Usefulness of Chest CT Imaging in Patients With Suspected or Diagnosed COVID-19: A Review of Literature. Chest 2021, 160, 652–670. [Google Scholar] [CrossRef]
| Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).


 ,
, 




{kind=link}
{kind=link}
{kind=link}