
Diagnostic Efficiency of Three Fully Automated Serology Assays and Their Correlation with a Novel Surrogate Virus Neutralization Test in Symptomatic and Asymptomatic SARS-COV-2 Individuals

 , ,
, ,  ,
,  , , , ,
, , , ,  and
and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design, Ethical Approval, and Clinical Samples
2.2. Automated-IgG Assays
2.3. Neutralization Assay (sVNT)
2.4. Statistical Analysis
3. Results
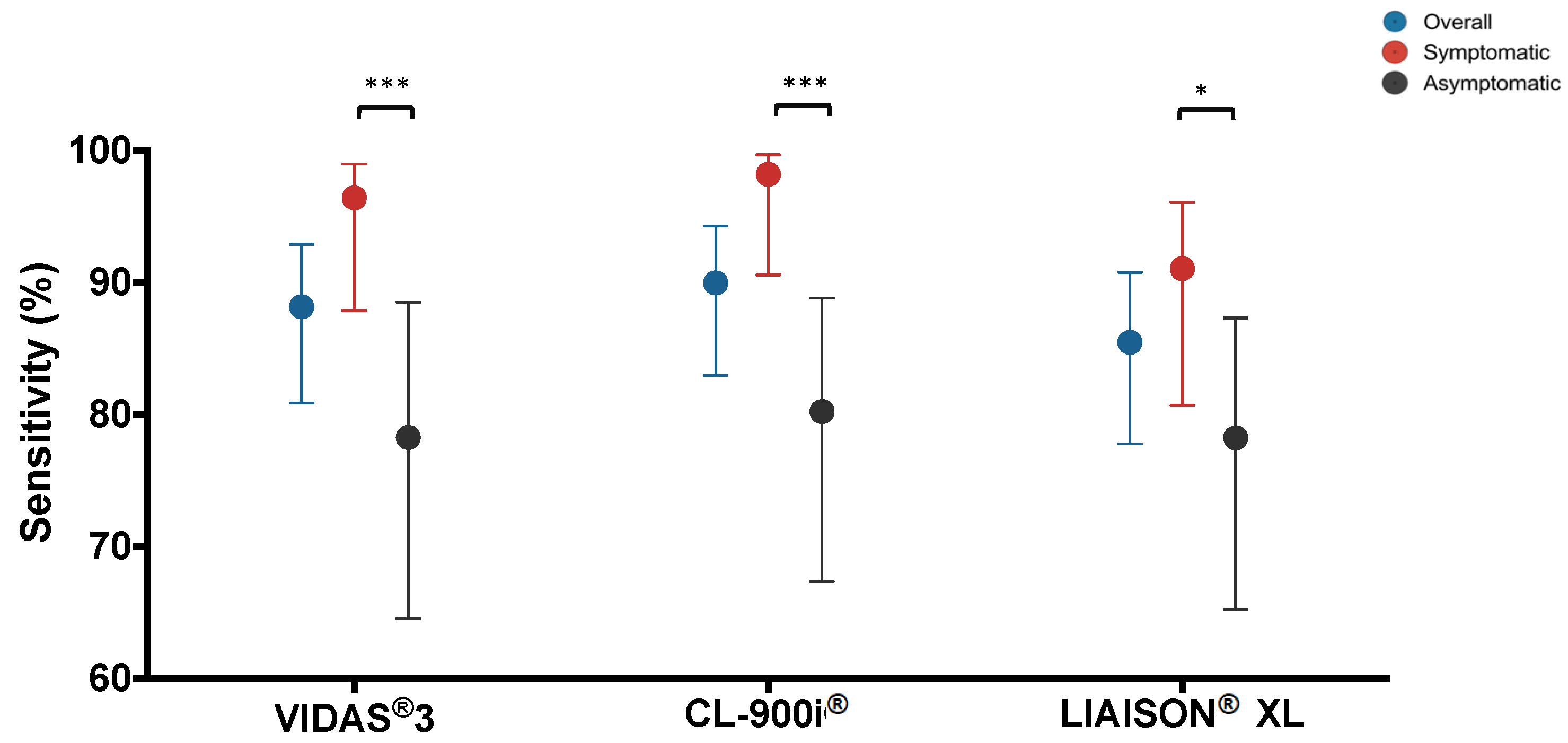
3.1. Diagnostic Performance Using RT-PCR as a Reference Test
3.2. Evaluation of Potential Cross-Reactivity with Other Viruses
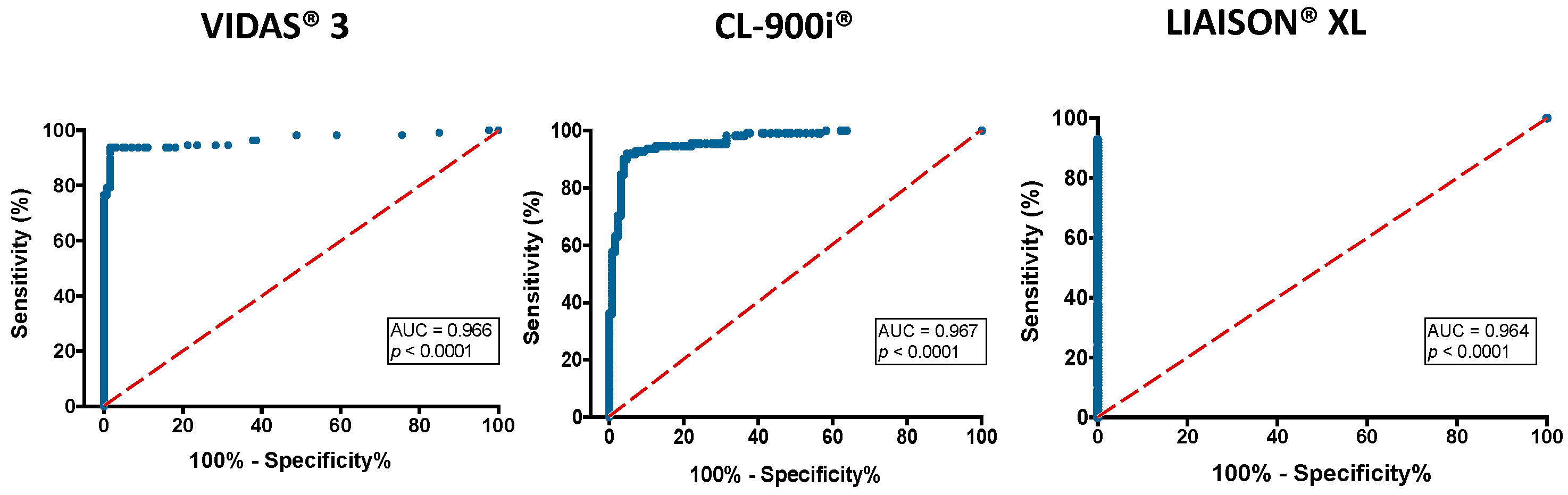
3.3. Receiver Operating Characteristics (ROC) Curve Analysis
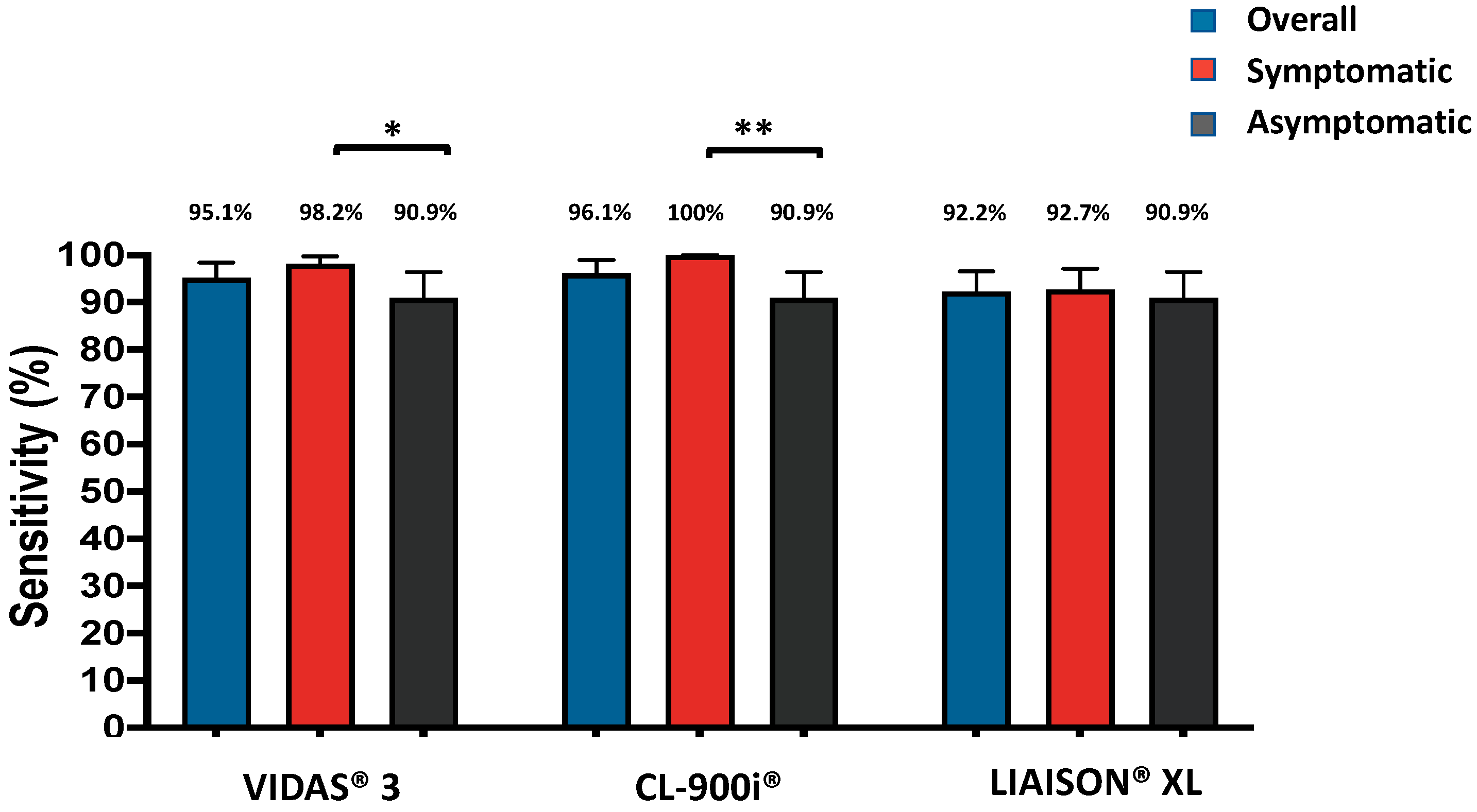
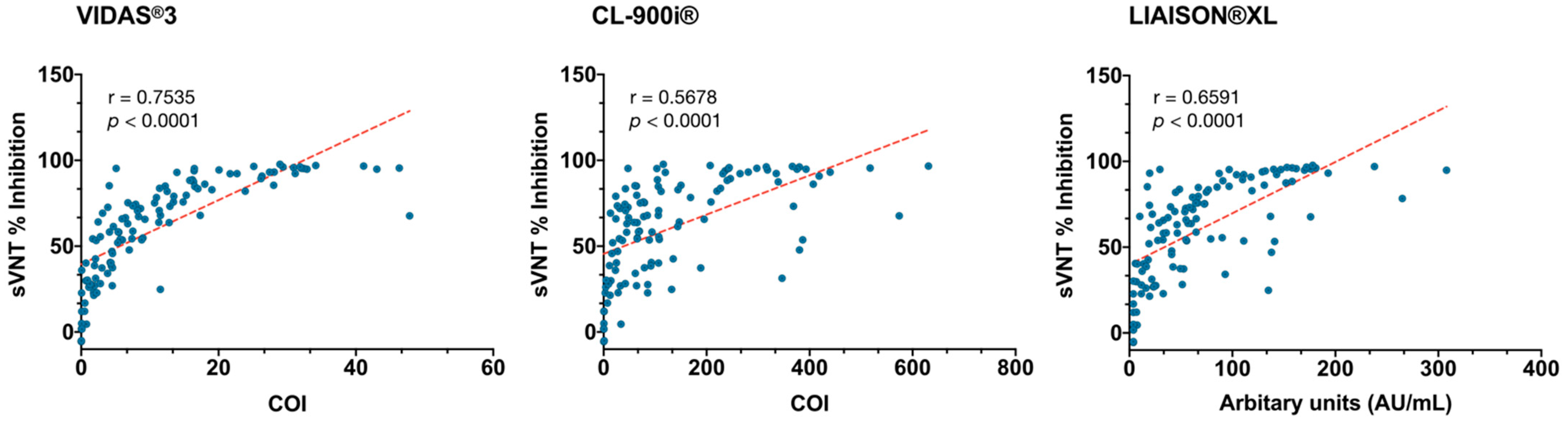
3.4. Diagnostic Performance Using sVNT as the Reference Test
3.5. Concordance Assessment among the SARS-CoV-2 IgG Automated Assays and the GenScript sVNT Test
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Zhou, P.; Yang, X.-L.; Wang, X.-G.; Hu, B.; Zhang, L.; Zhang, W.; Si, H.-R.; Zhu, Y.; Li, B.; Huang, C.-L.; et al. A pneumonia outbreak associated with a new coronavirus of probable bat origin. Nature 2020, 579, 270–273. [Google Scholar] [CrossRef] [Green Version]
- Gorbalenya, A.E.; Baker, S.C.; Baric, R.S.; de Groot, R.J.; Drosten, C.; Gulyaeva, A.A.; Haagmans, B.L.; Lauber, C.; Leontovich, A.M.; Neuman, B.W.; et al. The species Severe acute respiratory syndrome-related coronavirus: Classifying 2019-nCoV and naming it SARS-CoV-2. Nat. Microbiol. 2020, 5, 536–544. [Google Scholar] [CrossRef] [Green Version]
- Van Elslande, J.; Houben, E.; Depypere, M.; Brackenier, A.; Desmet, S.; André, E.; Van Ranst, M.; Lagrou, K.; Vermeersch, P. Diagnostic performance of seven rapid IgG/IgM antibody tests and the Euroimmun IgA/IgG ELISA in COVID-19 patients. Clin. Microbiol. Infect. 2020. [Google Scholar] [CrossRef]
- Ong, D.S.Y.; de Man, S.J.; Lindeboom, F.A.; Koeleman, J.G.M. Comparison of diagnostic accuracies of rapid serological tests and ELISA to molecular diagnostics in patients with suspected coronavirus disease 2019 presenting to the hospital. Clin. Microbiol. Infect. 2020. [Google Scholar] [CrossRef]
- World Health Organization. Coronavirus Disease (COVID-19) Dashboard. 2020. Available online: https://covid19.who.int/ (accessed on 1 December 2020).
- Petherick, A. Developing antibody tests for SARS-CoV-2. Lancet 2020, 395, 1101–1102. [Google Scholar] [CrossRef]
- Younes, N.; Al-Sadeq, D.W.; Al-Jighefee, H.; Younes, S.; Al-Jamal, O.; Daas, H.I.; Yassine, H.M.; Nasrallah, G.K. Challenges in Laboratory Diagnosis of the Novel Coronavirus SARS-CoV-2. Viruses 2020, 12, 582. [Google Scholar] [CrossRef]
- Yassine, H.M.; Al-Jighefee, H.; Al-Sadeq, D.W.; Dargham, S.R.; Younes, S.N.; Shurrab, F.; Marei, R.M.; Hssain, A.A.; Taleb, S.; Alhussain, H.; et al. Performance evaluation of five ELISA kits for detecting anti-SARS-COV-2 IgG antibodies. Int. J. Infect. Dis. 2021, 102, 181–187. [Google Scholar] [CrossRef]
- Okba, N.; Müller, M.A.; Li, W.; Wang, C.; GeurtsvanKessel, C.H.; Corman, V.M.; Haagmans, B.L. Severe acute respiratory syndrome coronavirus 2-specific antibody responses in coronavirus disease 2019 patients. Emerg. Infect. Dis. 2020, 26, 1478–1488. [Google Scholar] [CrossRef]
- Ng, K.W.; Faulkner, N.; Cornish, G.H.; Rosa, A.; Harvey, R.; Hussain, S.; Ulferts, R.; Earl, C.; Wrobel, A.G.; Benton, D.J.; et al. Preexisting and de novo humoral immunity to SARS-CoV-2 in humans. Science 2020, 370, 1339–1343. [Google Scholar] [CrossRef]
- Bryant, J.E.; Azman, A.S.; Ferrari, M.J.; Arnold, B.F.; Boni, M.F.; Boum, Y.; Hayford, K.; Luquero, F.J.; Mina, M.J.; Rodriguez-Barraquer, I.; et al. Serology for SARS-CoV-2: Apprehensions, opportunities, and the path forward. Sci. Immunol. 2020, 5, eabc6347. [Google Scholar] [CrossRef]
- Choe, P.G.; Perera, R.; Park, W.B.; Song, K.-H.; Bang, J.H.; Kim, E.S.; Kim, H.B.; Ko, L.W.R.; Park, S.W.; Kim, N.-J. MERS-CoV antibody responses 1 year after symptom onset, South Korea, 2015. Emerging infect. dis. 2017, 23, 1079. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Planning and Statistics Authority- State of Qatar. Qatar Monthly Statistics. Available online: https://www.psa.gov.qa/en/pages/default.aspx (accessed on 26 May 2020).
- Planning and Statistics Authority-State of Qatar. The Simplified Census of Population, Housing & Establishments. Available online: https://www.psa.gov.qa/en/statistics/Statistical%20Releases/Population/Population/2018/Population_social_1_2018_AE.pdf (accessed on 2 April 2020).
- World Population Review. Qatar Population (Live). Available online: https://worldpopulationreview.com/countries/qatar-population/ (accessed on 23 April 2020).
- Priya Dsouza Communications. Population of Qatar by Nationality–2019 Report. Available online: https://priyadsouza.com/population-of-qatar-by-nationality-in-2017/ (accessed on 15 August 2019).
- Nasrallah, G.K.; Al Absi, E.S.; Ghandour, R.; Ali, N.H.; Taleb, S.; Hedaya, L.; Ali, F.; Huwaidy, M.; Husseini, A. Seroprevalence of hepatitis E virus among blood donors in Qatar (2013–2016). Transfusion 2017, 57, 1801–1807. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Smatti, M.K.; Yassine, H.M.; AbuOdeh, R.; AlMarawani, A.; Taleb, S.A.; Althani, A.A.; Nasrallah, G.K. Prevalence and molecular profiling of Epstein Barr virus (EBV) among healthy blood donors from different nationalities in Qatar. PLoS ONE 2017, 12, e0189033. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Humphrey, J.M.; Al-Absi, E.S.; Hamdan, M.M.; Okasha, S.S.; Al-Trmanini, D.M.; El-Dous, H.G.; Dargham, S.R.; Schieffelin, J.; Abu-Raddad, L.J.; Nasrallah, G.K. Dengue and chikungunya seroprevalence among Qatari nationals and immigrants residing in Qatar. PLoS ONE 2019, 14, e0211574. [Google Scholar] [CrossRef] [PubMed]
- Al-Qahtani, A.A.; Alabsi, E.S.; AbuOdeh, R.; Thalib, L.; El Zowalaty, M.E.; Nasrallah, G.K. Prevalence of anelloviruses (TTV, TTMDV, and TTMV) in healthy blood donors and in patients infected with HBV or HCV in Qatar. Virol. J. 2016, 13, 208. [Google Scholar] [CrossRef] [Green Version]
- Dargham, S.R.; Nasrallah, G.K.; Al-Absi, E.S.; Mohammed, L.I.; Al-Disi, R.S.; Nofal, M.Y.; Abu-Raddad, L.J. Herpes Simplex Virus Type 2 Seroprevalence Among Different National Populations of Middle East and North African Men. Sex. Transm. Dis. 2018, 45, 482–487. [Google Scholar] [CrossRef]
- Nasrallah, G.K.; Dargham, S.R.; Mohammed, L.I.; Abu-Raddad, L.J. Estimating seroprevalence of herpes simplex virus type 1 among different Middle East and North African male populations residing in Qatar. J. Med. Virol. 2018, 90, 184–190. [Google Scholar] [CrossRef]
- Smatti, M.K.; Nasrallah, G.K.; Al Thani, A.A.; Yassine, H.M. Measuring influenza hemagglutinin (HA) stem-specific antibody-dependent cellular cytotoxicity (ADCC) in human sera using novel stabilized stem nanoparticle probes. Vaccine 2020, 38, 815–821. [Google Scholar] [CrossRef]
- Al Kahlout, R.A.; Nasrallah, G.K.; Farag, E.A.; Wang, L.; Lattwein, E.; Muller, M.A.; El Zowalaty, M.E.; Al Romaihi, H.E.; Graham, B.S.; Al Thani, A.A.; et al. Comparative Serological Study for the Prevalence of Anti-MERS Coronavirus Antibodies in High- and Low-Risk Groups in Qatar. J. Immunol. Res. 2019, 2019, 1386740. [Google Scholar] [CrossRef] [Green Version]
- Nasrallah, G.K.; Dargham, S.R.; Sahara, A.S.; Elsidiq, M.S.; Abu-Raddad, L.J. Performance of four diagnostic assays for detecting herpes simplex virus type 2 antibodies in the Middle East and North Africa. J. Clin. Virol. 2019, 111, 33–38. [Google Scholar] [CrossRef]
- Corman, V.M.; Landt, O.; Kaiser, M.; Molenkamp, R.; Meijer, A.; Chu, D.K.; Bleicker, T.; Brünink, S.; Schneider, J.; Schmidt, M.L.; et al. Detection of 2019 novel coronavirus (2019-nCoV) by real-time RT-PCR. Euro Surveill. 2020, 25, 2000045. [Google Scholar] [CrossRef] [Green Version]
- Mindray. SARS-CoV-2 IgG(CLIA). Available online: https://www.mindray.com/en/product/CL-900i.html (accessed on 25 January 2020).
- Nuccetelli, M.; Pieri, M.; Grelli, S.; Ciotti, M.; Miano, R.; Andreoni, M.; Bernardini, S. SARS-CoV-2 infection serology: A useful tool to overcome lockdown? Cell Death Discov. 2020, 6, 38. [Google Scholar] [CrossRef]
- BIOMÉRIEUX. VIDAS® SARS-COV-2. Available online: https://www.biomerieux-diagnostics.com/vidas-sars-cov-2 (accessed on 20 December 2020).
- Wolff, F.; Dahma, H.; Duterme, C.; Van den Wijngaert, S.; Vandenberg, O.; Cotton, F.; Montesinos, I. Monitoring antibody response following SARS-CoV-2 infection: Diagnostic efficiency of 4 automated immunoassays. Diagn. Microbiol. Infect. Dis. 2020, 98, 115140. [Google Scholar] [CrossRef]
- DiaSorin. LIAISON® SARS-CoV-2 S1/S2 IgG; DiaSorin S.p.A.: Via Crescentino snc, Saluggia, Italy, 2020; Volume 2020. [Google Scholar]
- GeneScript. SARS-CoV-2 Surrogate Virus Neutralization Test (sVNT) Kit; GeneScript USA Inc.: Piscataway, NJ, USA, 2020. [Google Scholar]
- Tan, C.W.; Chia, W.N.; Qin, X.; Liu, P.; Chen, M.I.C.; Tiu, C.; Hu, Z.; Chen, V.C.-W.; Young, B.E.; Sia, W.R.; et al. A SARS-CoV-2 surrogate virus neutralization test based on antibody-mediated blockage of ACE2–spike protein–protein interaction. Nat. Biotechnol. 2020, 38, 1073–1078. [Google Scholar] [CrossRef]
- Meyer, B.; Torriani, G.; Yerly, S.; Mazza, L.; Calame, A.; Arm-Vernez, I.; Zimmer, G.; Agoritsas, T.; Stirnemann, J.; Spechbach, H.; et al. Validation of a commercially available SARS-CoV-2 serological Immunoassay. medRxiv 2020. [Google Scholar] [CrossRef]
- Simundic, A.M. Measures of diagnostic accuracy: Basic definition. Ejifcc 2016, 19, 203–211. [Google Scholar]
- Youden, W.J. Index for rating diagnostic tests. Cancer 1950, 3, 32–35. [Google Scholar] [CrossRef]
- Kirch, W. (Ed.) Kappa CoefficientKappa coefficient. In Encyclopedia of Public Health; Springer: Dordrecht, The Netherlands, 2008; pp. 821–822. [Google Scholar]
- Michael, J.C.; Swinscow, T.D.V. Statistics at Square One, 11th ed.; Wiley: Hoboken, NJ, USA; Available online: https://www.wiley.com/en-ao/Statistics+at+Square+One%2C+11th+Edition-p-9781405191005 (accessed on 23 December 2020).
- Nie, J.; Li, Q.; Wu, J.; Zhao, C.; Hao, H.; Liu, H.; Zhang, L.; Nie, L.; Qin, H.; Wang, M.; et al. Establishment and validation of a pseudovirus neutralization assay for SARS-CoV-2. Emerg. Microbes Infect. 2020, 9, 680–686. [Google Scholar] [CrossRef] [Green Version]
- Wu, F.; Wang, A.; Liu, M.; Wang, Q.; Chen, J.; Xia, S.; Ling, Y.; Zhang, Y.; Xun, J.; Lu, L.; et al. Neutralizing antibody responses to SARS-CoV-2 in a COVID-19 recovered patient cohort and their implications. medRxiv 2020. [Google Scholar] [CrossRef] [Green Version]
- Tang, M.S.; Hock, K.G.; Logsdon, N.M.; Hayes, J.E.; Gronowski, A.M.; Anderson, N.W.; Farnsworth, C.W. Clinical Performance of Two SARS-CoV-2 Serologic Assays. Clin. Chem. 2020, 66, 1055–1062. [Google Scholar] [CrossRef] [PubMed]
- Chen, S.-Y.; Lee, Y.-L.; Lin, Y.-C.; Lee, N.-Y.; Liao, C.-H.; Hung, Y.-P.; Lu, M.-C.; Wu, J.-L.; Tseng, W.-P.; Lin, C.-H.; et al. Multicenter evaluation of two chemiluminescence and three lateral flow immunoassays for the diagnosis of COVID-19 and assessment of antibody dynamic responses to SARS-CoV-2 in Taiwan. Emerg. Microbes Infect. 2020, 9, 2157–2168. [Google Scholar] [CrossRef] [PubMed]
- Wu, J.; Liang, B.; Chen, C.; Wang, H.; Fang, Y.; Shen, S.; Yang, X.; Wang, B.; Chen, L.; Chen, Q.; et al. SARS-CoV-2 infection induces sustained humoral immune responses in convalescent patients following symptomatic COVID-19. medRxiv 2020. [Google Scholar] [CrossRef]
- Zhao, J.; Yuan, Q.; Wang, H.; Liu, W.; Liao, X.; Su, Y.; Wang, X.; Yuan, J.; Li, T.; Li, J.; et al. Antibody responses to SARS-CoV-2 in patients of novel coronavirus disease 2019. Clin. Infect. Dis. Off. Publ. Infect. Dis. Soc. Am. 2020, ciaa344. [Google Scholar] [CrossRef]
- Mooney, M.; Perera, N.K.P.; Broderick, C.; Saw, R.; Wallett, A.; Drew, M.; Waddington, G.; Hughes, D. A deep dive into testing and management of COVID-19 for Australian high performance and professional sport. J. Sci. Med. Sport 2020, 23, 664–669. [Google Scholar] [CrossRef] [PubMed]
- Basile, K.; Maddocks, S.; Kok, J.; Dwyer, D.E. Accuracy amidst ambiguity: False positive SARS-CoV-2 nucleic acid tests when COVID-19 prevalence is low. Pathology 2020, 52, 809–811. [Google Scholar] [CrossRef]
- Katz, A.P.; Civantos, F.J.; Sargi, Z.; Leibowitz, J.M.; Nicolli, E.A.; Weed, D.; Moskovitz, A.E.; Civantos, A.M.; Andrews, D.M.; Martinez, O.; et al. False-positive reverse transcriptase polymerase chain reaction screening for SARS-CoV-2 in the setting of urgent head and neck surgery and otolaryngologic emergencies during the pandemic: Clinical implications. Head Neck 2020, 42, 1621–1628. [Google Scholar] [CrossRef]
- Bryan, A.; Pepper, G.; Wener, M.H.; Fink, S.L.; Morishima, C.; Chaudhary, A.; Jerome, K.R.; Mathias, P.C.; Greninger, A.L. Performance Characteristics of the Abbott Architect SARS-CoV-2 IgG Assay and Seroprevalence in Boise, Idaho. J. Clin. Microbiol. 2020, 58, e00920–e00941. [Google Scholar] [CrossRef]
- Kohmer, N.; Westhaus, S.; Rühl, C.; Ciesek, S.; Rabenau, H.F. Brief clinical evaluation of six high-throughput SARS-CoV-2 IgG antibody assays. J. Clin. Virol. 2020, 129, 104480. [Google Scholar] [CrossRef]
- Public Health England. Evaluation of Roche Elecsys AntiSARS-CoV-2 Serology Assay for the Detection of anti-SARS-CoV-2 Antibodies. Available online: https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/891598/Evaluation_of_Roche_Elecsys_anti_SARS_CoV_2_PHE_200610_v8.1_FINAL.pdf (accessed on 5 June 2020).
- Coste, A.T.; Jaton, K.; Papadimitriou-Olivgeris, M.; Greub, G.; Croxatto, A. Comparison of SARS-CoV-2 serological tests with different antigen targets. medRxiv 2020. [Google Scholar] [CrossRef]
- Chia, W.N.; Tan, C.W.; Foo, R.; Kang, A.E.Z.; Peng, Y.; Sivalingam, V.; Tiu, C.; Ong, X.M.; Zhu, F.; Young, B.E.; et al. Serological differentiation between COVID-19 and SARS infections. Emerg. Microbes Infect. 2020, 9, 1497–1505. [Google Scholar] [CrossRef]
- Jääskeläinen, A.J.; Kuivanen, S.; Kekäläinen, E.; Ahava, M.J.; Loginov, R.; Kallio-Kokko, H.; Vapalahti, O.; Jarva, H.; Kurkela, S.; Lappalainen, M. Performance of six SARS-CoV-2 immunoassays in comparison with microneutralisation. J. Clin. Virol. 2020, 129, 104512. [Google Scholar] [CrossRef] [PubMed]
- Bonelli, F.; Sarasini, A.; Zierold, C.; Calleri, M.; Bonetti, A.; Vismara, C.; Blocki, F.; Pallavicini, L.; Chinali, A.; Campisi, D.; et al. Clinical And Analytical Performance Of An Automated Serological Test That Identifies S1/S2 Neutralizing IgG In Covid-19 Patients Semiquantitatively. bioRxiv 2020. [Google Scholar] [CrossRef] [PubMed]
- Perkmann, T.; Perkmann-Nagele, N.; Breyer, M.-K.; Breyer-Kohansal, R.; Burghuber, O.C.; Hartl, S.; Aletaha, D.; Sieghart, D.; Quehenberger, P.; Marculescu, R.; et al. Side-by-Side Comparison of Three Fully Automated SARS-CoV-2 Antibody Assays with a Focus on Specificity. Clin. Chem. 2020, 66, 1405–1413. [Google Scholar] [CrossRef] [PubMed]
- Winter, A.K.; Hegde, S.T. The important role of serology for COVID-19 control. Lancet Infect. Dis. 2020, 20, 758–759. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Automated Analyzer | Detection Method | Targeted Antigen(s) a | Sample Volume | Result Interpretation | Reported Sensitivity | Reported Specificity | Reference |
|---|---|---|---|---|---|---|---|
| VIDAS®3 | ELFA | S1 RBD | 100 μL (including the dead volume) | <1 AU/mL: Negative ≥1 AU/mL: Positive | 100% (≥15 days) | 98.5% | [29,30] |
| CL-900i® | CLIA | S and N proteins | 10 μL (this volume does not include the dead volume) | <10 AU/mL: Negative ≥10 AU/mL: Positive | 100% (≥15 days) | 94.9% | [27,28] |
| LIAISON®XL | CLIA | S1/S2 | 170 μL of specimen (20 μL specimen +150 μL dead volume) | <12 AU/mL: Negative 12–15 AU/mL: Borderline >15 AU/mL: Positive | 97.5% (≥15 days) | 98.2% | [30,31] |
| RT-PCR | Overall Percent Agreement | Sensitivity | Specificity | Cohen’s Kappa Statistic | ||||
|---|---|---|---|---|---|---|---|---|
| Positive | Negative | Total | % (95% CI) | % (95% CI) | % (95% CI) | k (95% CI) | ||
| (A) | ||||||||
| Negative | 11 | 121 | 132 | |||||
| Total | 111 | 127 | 238 | |||||
| VIDAS®3 assay | Positive | 98 | 2 | 100 | 93.7 (89.9–96.2) | 88.3 (81.0–93.0) | 98.4 (94.5–99.6) | 0.87 (0.83–0.92) |
| Negative | 13 | 125 | 138 | |||||
| Total | 111 | 127 | 238 | |||||
| CL-900i® assay | Positive | 100 | 6 | 106 | 92.9 (88.9–95.5) | 90.1 (83.1–94.4) | 95.3 (90.1–97.8) | 0.86 (0.81–0.90) |
| Negative | 11 | 121 | 132 | |||||
| Total | 111 | 127 | 238 | |||||
| LIAISON®XL assay | Positive | 95 | 0 | 95 | 93.3 (89.4–95.8) | 85.6 (77.9–90.9) | 100 (97.1–100) | 0.86 (0.82–0.91) |
| Negative | 16 | 127 | 143 | |||||
| Total | 111 | 127 | 238 | |||||
| (B) | ||||||||
| VIDAS®3 assay | Positive | 54 | 2 | 56 | 97.8 (94.5–99.1) | 96.4 (87.9–99.0) | 98.4 (94.5–99.6) | 0.95 (0.92–0.98) |
| Negative | 2 | 125 | 127 | |||||
| Total | 56 | 127 | 183 | |||||
| CL-900i® assay | Positive | 55 | 6 | 61 | 96.2 (92.3–98.1) | 98.2 (90.6–99.7) | 95.3 (90.1–97.8) | 0.91 (0.87–0.95) |
| Negative | 1 | 121 | 122 | |||||
| Total | 56 | 127 | 183 | |||||
| LIAISON®XL assay | Positive | 51 | 0 | 51 | 97.3 (93.8–98.8) | 91.1 (80.7–96.1) | 100 (97.1–100) | 0.93 (0.90–0.97) |
| Negative | 5 | 127 | 132 | |||||
| Total | 56 | 127 | 183 | |||||
| (C) | ||||||||
| Negative | 10 | 121 | 131 | |||||
| Total | 51 | 127 | 178 | |||||
| VIDAS®3 assay | Positive | 40 | 2 | 42 | 92.7 (89.8–96.2) | 78.4 (64.7–88.7) | 98.4 (94.5–99.6) | 0.81 (0.75–0.87) |
| Negative | 11 | 125 | 136 | |||||
| Total | 56 | 127 | 178 | |||||
| CL-900i® assay | Positive | 41 | 6 | 47 | 91.0 (85.9–94.4) | 80.4 (67.5–89.0) | 95.3 (90.1–97.8) | 0.77 (0.71–0.84) |
| Negative | 10 | 121 | 131 | |||||
| Total | 51 | 127 | 178 | |||||
| LIAISON®XL assay | Positive | 40 | 0 | 40 | 93.8 (89.3–96.5) | 78.4 (65.4–87.5) | 100 (97.1–100) | 0.84 (0.78–0.90) |
| Negative | 11 | 121 | 131 | |||||
| Total | 51 | 127 | 178 | |||||
| Subgroup with IgG/IgM Antibodies Against: | No. of Samples | VIDAS®3 | CL-900i® | LIAISON®XL |
|---|---|---|---|---|
| % (95% CI) | % (95% CI) | % (95% CI) | ||
| Other human CoVs (SARS-CoV, MERS-CoV, HCoV-229E, NL63, OC43, and HKU1) | 18 | 18/18; 100 (82.4–100) | 12/18; 66.7 (43.8–83.7) | 18/18; 100 (82.4–100) |
| Non-CoV respiratory viruses (Influenza A and RSV) | 38 | 37/38; 97.4 (86.5–99.5) | 38/38; 100 (90.8–100) | 38/38; 100 (90.8–100) |
| Non-respiratory viruses (HEV, HGV, HCV, HBV, DENV, WNV, CHIKV, B19, HSV-1, HSV-2, EBV, HHV-6, and HHV-8) | 65 | 65/65; 100 (94.4–100) | 65/65; 100 (94.4–100) | 65/65; 100 (94.4–100) |
| Antinuclear antibodies (ANAs) | 6 | 5/6; 83.3 (43.7–97.0) | 6/6; 100 (61.0–100) | 6/6; 100 (61.0–100) |
| Overall specificity | 127 | 125/127; 98.4 (94.5–99.6) | 121/127; 95.3 (90.1–97.8) | 127/127; 100 (97.1–100) |
| Test | Compared to | Overall Percent Agreement | Positive Percent Agreement | Negative Percent Agreement | Cohen’s Kappa Statistic |
|---|---|---|---|---|---|
| % (95% CI) | % (95% CI) | % (95% CI) | k (95% CI) | ||
| sVNT | VIDAS®3 | 106/111; 95.5 (89.9–98.1) | 98/103; 95.1 (89.1–97.9) | 8/8; 100 (67.6–100) | 0.74 (0.65–0.83) |
| CL-900i® | 106/111; 95.5 (89.9–98.1) | 99/103; 96.1 (90.4–98.5) | 7/8; 87.5 (52.9–97.8) | 0.71 (0.62–0.81) | |
| LIAISON®XL | 103/111; 92.8 (86.4–96.3) | 95/103; 92.2 (85.4–96.0) | 8/8; 100 (67.6–100) | 0.63 (0.52–0.74) | |
| VIDAS®3 | sVNT | 106/111; 95.5 (89.9–98.1) | 98/98; 100 (92.3–100) | 8/13; 61.5 (35.5–82.3) | 0.74 (0.65–0.83) |
| CL-900i® | 105/111; 94.6 (88.7–97.5) | 96/98; 98.0 (92.5–99.4) | 9/13; 69.2 (42.4–87.3) | 0.72 (0.62–0.82) | |
| LIAISON®XL | 106/111; 95.5 (89.9–98.1) | 94/98; 95.9 (90.0–98.4) | 12/13; 92.3 (66.7–98.6) | 0.80 (0.72–0.88) | |
| CL-900i® | sVNT | 106/111; 95.5 (89.9–98.1) | 99/100; 99.0 (94.6–99.8) | 7/11; 63.6 (35.4–84.8) | 0.71 (0.62–0.81) |
| VIDAS®3 | 105/111; 94.6 (88.7–97.5) | 96/100; 96.0 (90.2–98.4) | 9/11; 81.8 (52.3–94.9) | 0.72 (0.62–0.82) | |
| LIAISON®XL | 104/111; 93.7 (87.6–96.9) | 94/100; 94.0 (87.5–97.2) | 10/11; 90.9 (62.3–98.4) | 0.71 (0.61–0.80) | |
| LIAISON®XL | sVNT | 103/111; 92.8 (86.4–96.3) | 95/95; 100 (96.1–100) | 8/16; 50.0 (28.0–72.0) | 0.63 (0.52–0.74) |
| CL-900i® | 104/111; 93.7 (87.6–96.9) | 94/95; 98.9 (94.3–99.8) | 10/16; 62.5 (38.6–81.5) | 0.71 (0.61–0.80) | |
| VIDAS®3 | 106/111 95.5 (89.9–98.1) | 94/95; 98.9 (94.3–99.8) | 12/16; 75.0 (50.5–89.8) | 0.80 (0.72–0.88) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Younes, S.; Al-Jighefee, H.; Shurrab, F.; Al-Sadeq, D.W.; Younes, N.; Dargham, S.R.; Al-Dewik, N.; Qotba, H.; Syed, M.; Alnuaimi, A.; et al. Diagnostic Efficiency of Three Fully Automated Serology Assays and Their Correlation with a Novel Surrogate Virus Neutralization Test in Symptomatic and Asymptomatic SARS-COV-2 Individuals. Microorganisms 2021, 9, 245. https://doi.org/10.3390/microorganisms9020245
Younes S, Al-Jighefee H, Shurrab F, Al-Sadeq DW, Younes N, Dargham SR, Al-Dewik N, Qotba H, Syed M, Alnuaimi A, et al. Diagnostic Efficiency of Three Fully Automated Serology Assays and Their Correlation with a Novel Surrogate Virus Neutralization Test in Symptomatic and Asymptomatic SARS-COV-2 Individuals. Microorganisms. 2021; 9(2):245. https://doi.org/10.3390/microorganisms9020245
Chicago/Turabian StyleYounes, Salma, Hadeel Al-Jighefee, Farah Shurrab, Duaa W. Al-Sadeq, Nadin Younes, Soha R. Dargham, Nader Al-Dewik, Hamda Qotba, Mohamed Syed, Ahmed Alnuaimi, and et al. 2021. "Diagnostic Efficiency of Three Fully Automated Serology Assays and Their Correlation with a Novel Surrogate Virus Neutralization Test in Symptomatic and Asymptomatic SARS-COV-2 Individuals" Microorganisms 9, no. 2: 245. https://doi.org/10.3390/microorganisms9020245