
The Pandemic Puzzle—Reviewing the Existing Pieces, Searching for the Missing Ones


1
Department of Pneumology, Iuliu Hațieganu University of Medicine and Pharmacy, 400332 Cluj-Napoca, Romania
2
Public Health Department, Faculty of Dental Medicine, Carol Davila University of Medicine and Pharmacy, 050474 Bucharest, Romania
3
Department of Plastic Surgery and Reconstructive Microsurgery, Carol Davila University of Medicine and Pharmacy, 050474 Bucharest, Romania
*
Author to whom correspondence should be addressed.
Sustainability 2023, 15(6), 5214; https://doi.org/10.3390/su15065214
Submission received: 23 January 2023
/
Revised: 9 March 2023
/
Accepted: 11 March 2023
/
Published: 15 March 2023
(This article belongs to the Special Issue Public Health and Healthcare Services Technologies and Development in Post-COVID 19 Era)
Abstract
:The research carried out on socioeconomic implication models of (re)emerging infectious diseases triggering pandemics has shown us that these largely depended on infection transmission, conditioned by the type of pathogen and the human host. Also, these depended on certain external factors, such as the phenomenon of globalization, pollution, fragile health systems, modification of human behaviors, expansion of human habitat near the outbreaks, favorable vectors involved in the transmission and development of new pandemics and last but not least of wars or civil revolts. The present research attempts to provide some responses to the following questions: 1. What have been the most recent and important emerging infectious disease pandemics and what were the risk factors? 2. What was the socioeconomic impact generated by these pandemics and what important lessons did we learn/identify? 3. What measures and/or directions must be implemented/addressed to prevent/possibly stop a future wave of infections or a new pandemic? The answers to these questions are substantiated by different indicators (transmission potential and pathogen severity) through which we focused to offer some suggestions/directions regarding the way in which these pandemics could be anticipated or prevent, indicators that otherwise are already used by public authorities in the development and exploration of intervention strategies. However, through the elaboration and staged presentation of how these pandemics acted as well as the socioeconomic implications and human reactions, this research could be useful in leading to the development of new, effective ways to prevent the transmission of (re)emerging infectious diseases.
1. Introduction
The year 2020 was different from previous years. The world has changed, and the trigger was not a new industrial revolution, as we would have expected, but the emergence of an unknown pathogen agent from the wild that caused an unknown disease, which scientists predicted but did not evaluate it in totality [1]. This disease, known today as COVID-19, has reconfigured the society of the most evolved species on Earth and, despite the advances made in the medical field, has generated an unprecedented global crisis, the multiple effects of which are still being felt.
1.1. Theoretical Background—Mirroring the Present and the Future in the Context of (Re)emerging Infectious Diseases
There is a close causal relationship between high population mobility, the impact, severity, and mode of spread of new epidemics. Globalization, demography, climate changes, urban agglomerations, the coexistence of humans and animals and, finally, the delayed reactions of the international surveillance systems of risk areas contribute to increasing the risk of emerging infectious diseases and, at the same time, lead to the possibility the outbreak of new pandemics [2,3].
The past abounds in classic examples of infectious agents that have generated pandemics, such as smallpox, cholera, Spanish flu [4] as well as new emerging infectious agents, including the coronavirus family, Nipah virus, Hantavirus, Ebola virus, Crimean-Congo hemorrhagic fever, Rift Valley fever virus, Lassa fever virus, Zika virus, which have demonstrated their ability to become global threats [1,5].
Also, the continuous changing capacity of the microbial world represents a threat to the process of managing health crises. Developing, obtaining the necessary approvals and implementing new therapies within therapeutic protocols involves a lot of time, which in case of a pandemic caused by an unknown infectious agent, most of the time, can be insufficient. The most eloquent example was the COVID-19 pandemic, where changing the behaviors of individuals, the rapid development of computational tools for synthesizing and understanding epidemiological patterns, and collaboration on a global scale was desirable and at the same time showed us that we are still unprepared to face future threats [6].
1.2. Aim of the Research
This qualitative synthesis aims to identify some answers and possible hints regarding the method of mitigate/combat (re)emerging infectious diseases due to some viral or zoonotic infectious agents triggering pandemics. By understanding the model of evolution and dynamics of these pandemics and in conjunction with predictive mathematical models combined or not with effective machine learning models and based on lessons learned from past expertise, this research tries to offer some new solutions to face new possible threats.
2. Materials and Methods
2.1. Search Method
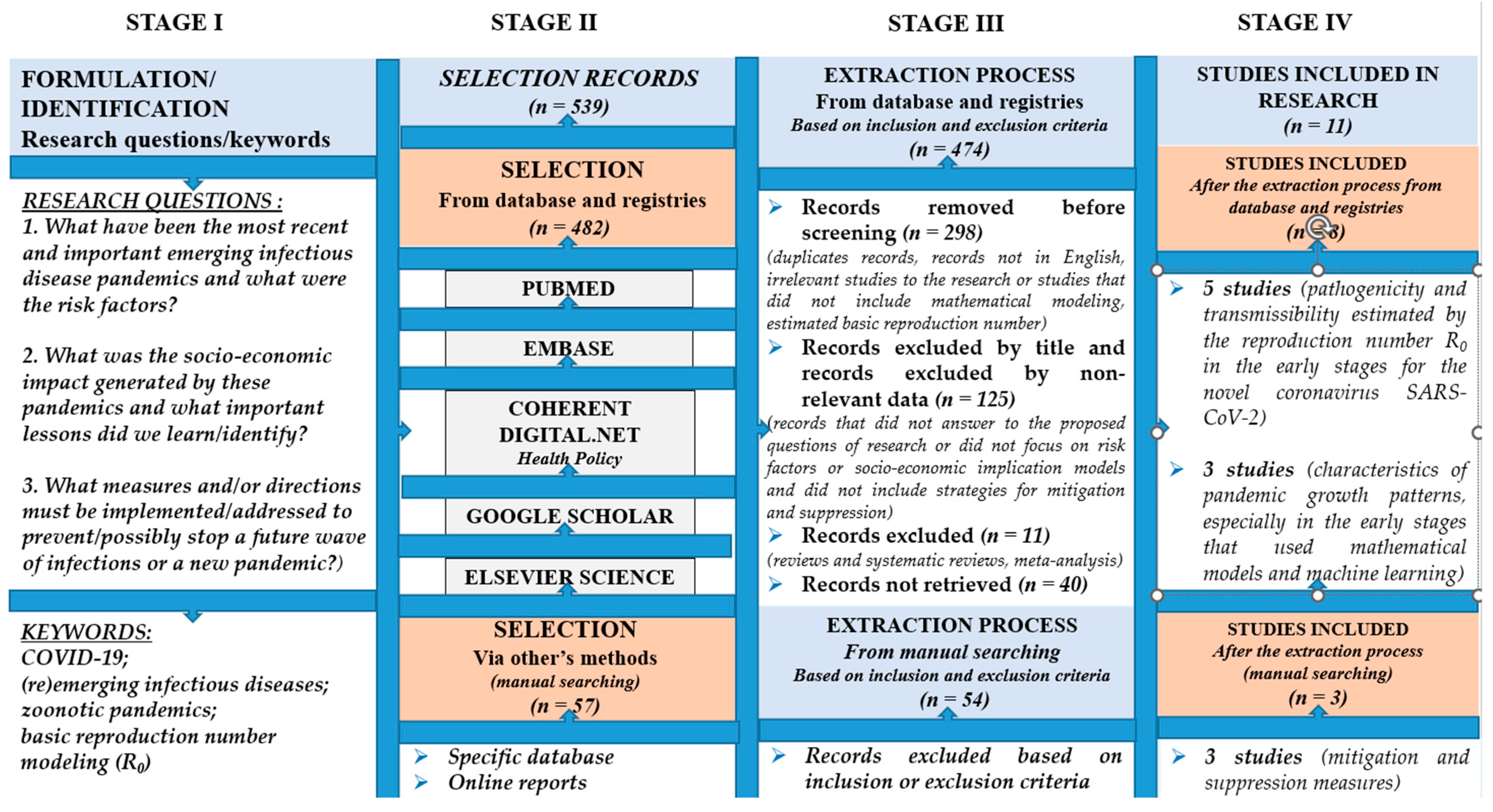
Following a review of the specialized literature, the preferred reporting items were selected from different databases: PubMed, Embase, Coherent digital.net—Community of Common Policies, Google Scholar, and Elsevier Science. Selected items ranged from January 2017 to December 2022 and followed the inclusion criteria such as studies that used mathematical models to track the parameters of transmissibility and severity of (re)emerging infectious diseases in early phases as well as the implications and prevention plans applied to prevent/combat these diseases. The research was realized in four stages.
The first stage consisted of formulating the questions (1. What have been the most recent and important emerging infectious disease pandemics and what were the risk factors? 2. What was the socioeconomic impact generated by these pandemics and what important lessons did we learn/identify? 3. What measures and/or directions must be implemented/addressed to prevent/possibly stop a future wave of infections or a new pandemic?) and identification of the relevant keywords of the research (COVID-19; (re)emerging infectious diseases; zoonotic pandemics; basic reproduction number modeling (R0)).
In the second stage, using the following keywords: ((COVID-19) OR (SARS-CoV-2) OR (2019 novel coronavirus) OR (severe acute respiratory syndrome coronavirus 2)) AND (((re)emerging infectious diseases) OR (zoonotic pandemics), AND (modeling basic reproduction number modeling (R0)) OR (estimated basic reproduction number (R0))), we identified from the database and registries 482 records appropriate to the aim of the research. To have a complete image of the evolution and impact on worldwide pandemics, a manual search was also carried out and we identified 57 initial records.
The third stage consisted of the extraction process, and after using the inclusion and exclusion criteria, we selected only the studies and reports that were suitable for this research. The fourth stage consisted of the coalescence of the data that resulted after the extraction process, and 11 studies were considered relevant and used in this qualitative synthesis; see Figure 1. Flow diagram of literature search, screening, inclusion and exclusion of studies and Table 1. Characteristics of the included studies in research.
From these 11 studies, 8 studies were based on data originated from countries located on the Asian continent, geographic area recognized as a considerable zoonotic tank with favorable vectors for transmitting (re)emerging infectious disease or performed by Asian researchers. More precisely, 5 studies focused on pathogenicity and transmissibility estimated by the reproduction number R0 in the early stages for the novel coronavirus SARS-CoV-2 and 3 studies were focused on characteristics of pandemic growth patterns, especially in the early stages that used mathematical models and machine learning. The other 3 studies that resulted from the manual searching carried out were considered suitable because of the correlation between transmission variations with risk factors, attenuation and suppression strategies, especially in the early stages of the disease on populations located in Europe, USA, UK, areas of the Middle East, North- and sub-Saharan Africa and areas of Asia and the Pacific; see Figure 1. Flow diagram of literature search, screening, inclusion and exclusion of studies and Table 1. Characteristics of the included studies in research.
Additionally, we tried to identify and evaluate the risk factors and socioeconomic impact of the most important and recent pandemics based on reports or data published online by expert groups into specific databases such as the World Health Organization (WHO), the Center for Disease Prevention and Control (CDC), the European Commission, the World Bank, and the International Monetary Fund. From these we selected only the relevant data that answered the research questions formulated in the first stage of the research, see the Table 2 Risk factors involved in the development of (re)emerging infectious disease and Table 3. Items of interest regarding pathogens that, through their characteristics, have influenced medical research.
2.2. Selection Criteria
Inclusion criteria were as follows:
- Studies published between January 2017 and December 2022.
- Relevant articles according to the year of publication, the name of the researcher, the category of the research, the title of the source and the list of journals.
- Studies published in English.
- Studies based on mathematical modeling to track the parameters of transmissibility (estimated by R0) and severity (health indicators) of (re)emerging infectious diseases in early phases of the outbreaks.
- Studies based on the implications and prevention plans applied to prevent/combat zoonotic pandemics (avian, porcine, those due to the Coronavirus family as well as some emerging viruses considered possible future threats (Ebola, Nipah and Hantavirus)).
- Studies focused on risk factors that can trigger pandemics.
- Studies regarding the evolution of (re)emerging infectious diseases and the socioeconomic implication models.
Exclusion criteria were as follows:
- Articles that were irrelevant to the research (symposia, books, workshops or discussion papers).
- Duplicates and articles that were not in English.
- Studies that did not include mathematical modeling or estimated of the basic reproduction number (R0) of (re)emerging infectious diseases in early phases of the outbreaks.
- Studies that did not answer the proposed research questions.
- Studies that did not focus on risk factors that can trigger pandemics or to evolution and socioeconomic implication models.
- Studies that did not include implications and prevention plans applied to prevent/combat zoonotic pandemics (avian, porcine, those due to the Coronavirus family as well as some emerging viruses considered possible future threats (Ebola, Nipah and Hantavirus)).
- Systematic reviews and meta-analysis.
3. Results
This research is a review on pandemics and the management of corresponding health crises. Based on characteristics and evolution of pandemics, growth patterns, especially in the early stages, we focused on two important indicators, namely the transmission potential (basic reproduction number of the infection (R0)) and the pathogen severity (virulence) estimated with the help of mathematical tools and machine learning, as well as the implications and strategic intervention plans applied by authorities.
We have also tried to highlight the importance of these tools in the fight against new (re)emerging disease by generating useful forecasts and allow rapid intervention by authorities to minimize/alter the rate of transmission especially in the early stages of outbreaks of pathogens potentially dangerous in triggering pandemics.
The initial research identified 482 records from database and registries and 57 using other methods (manual searching). After the extraction process by applying the inclusion and exclusion criteria, eight studies regarding characteristics of pandemic growth patterns, especially in the early stages that used mathematical models and machine learning were considered relevant to our research. After conducting the manual search, we considered another three studies suitable for our review regarding the strategies for mitigation and suppression especially in the early stages of these disease performed in high- and low-income countries. Thus, 11 studies were considered relevant and used in this qualitative synthesis; see Figure 1. Flow diagram of literature search, screening, inclusion and exclusion of studies and Table 1. Characteristics of the included studies in research.
In addition, we considered it appropriate for our research to identify the triggers that outbreak pandemics, see Table 2 Risk factors involved in the development of (re)emerging infectious disease add some data from online reports published by expert groups into specific databases such as: the World Health Organization (WHO), the Center for Disease Prevention and Control (CDC), the European Commission, the World Bank and the International Monetary Fund, which answered the research questions formulated in the first stage of this research; see Table 3. Items of interest regarding pathogens that, through their characteristics, have influenced medical research.
The conclusions of these studies and data reports analyzed in this research reinforced the idea, emphasized by us, that the impact of a pandemic on a population is different. The evolution and impact of a pandemic depend on the risk factors, evolution model, characteristics of the virus as well as human reactions.
In this fight against the triggers that cause the outbreak of pandemics or modify the impact and evolution of them (climate change, globalization, geographic variations, population distribution and age groups, zoonotic reservoir, as well as human actions and delay or lack of response by authorities), it is very important to be warned on time and to be able to modify the evolution of a new (re)emerging infectious disease starting from the early stages.
Thus, using an equitable approach to countries with deficient healthcare systems and by developing mathematical tools and/or using machine learning, we could be better prepared to face new possible threats.
3.1. Brief History of Pathogens That Have Influenced Medical Research
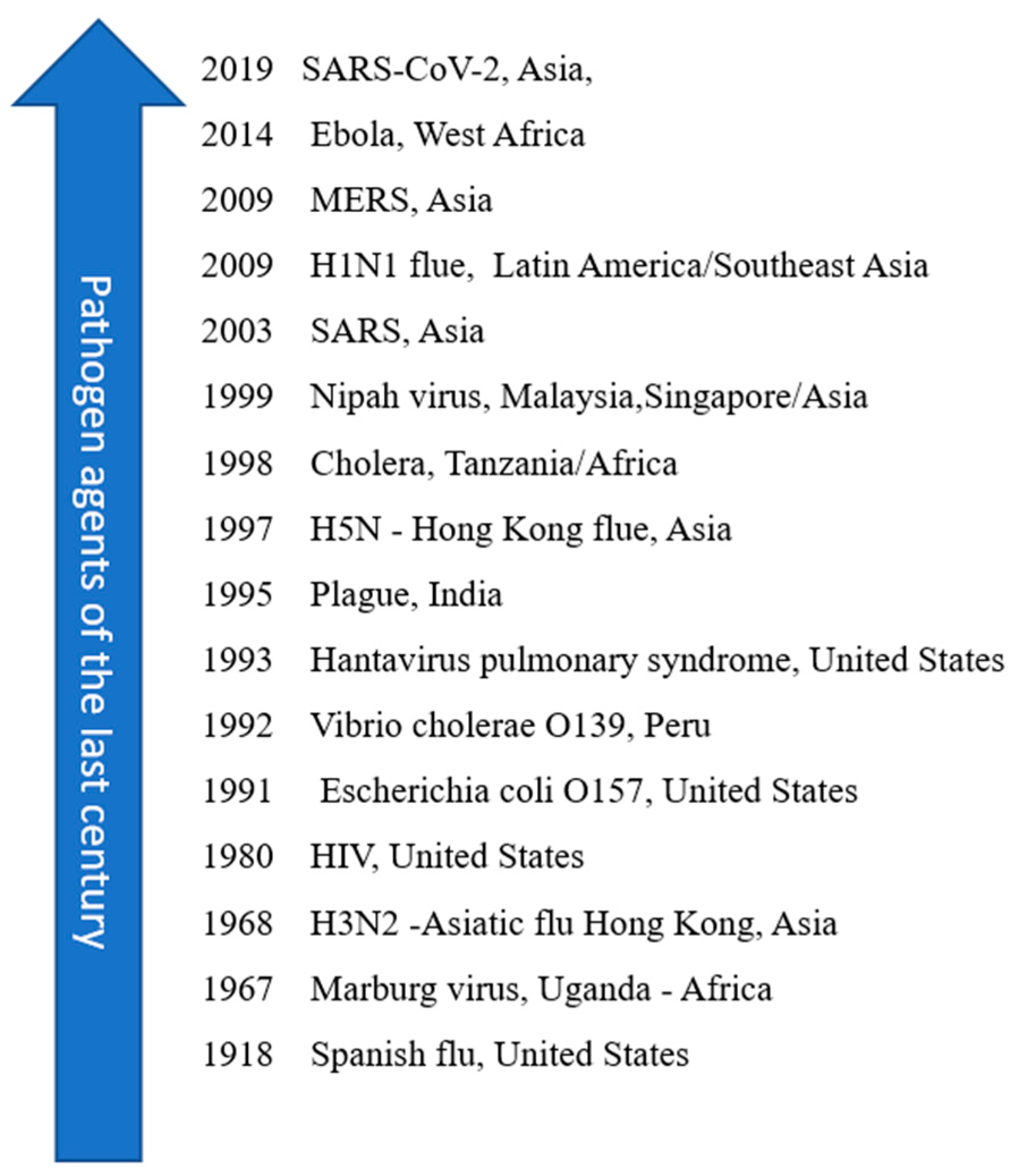
The WHO has developed a research and development plan to provide vaccines, drugs, and diagnostic tests for the most dangerous known pathogens so that we can act promptly and appropriately in case we must face an unknown infectious pathogen. Also, it has compiled a priority list of pathogens that require additional monitoring and urgent action. Most of the priority pathogens are not previously unknown viruses, but viruses that have already caused epidemics among humans, which have traveled and have adapted, which is especially worrying because we still have no cure. Their names are Crimean–Congo hemorrhagic fever, Rift Valley fever, Lassa fever, Zika virus, Nipah and Ebola, agents that have demonstrated their ability to become global threats [1,5]. (Figure 2. Pathogens that have generated epidemics in the modern world for each continent) The appearance of the new coronavirus, the previously unknown SARS-CoV-2 virus, demonstrated how vulnerable and unprepared we are in the face of these global threats and how important it is to invest in research and innovation programs, of unity and global cooperation to be able to provide a rapid and effective response to infectious agents that could present a threat to humanity. However, to face these future threats, we need significant investment to improve public health and time to deal with future health crises [18].
3.2. Risk Factors Involved in the Development of Emerging Infectious Diseases
The impact, severity and spread of new emerging infectious diseases and the possibility of generating pandemics is closely correlated with the internal factors related to the characteristics of the pathogen incriminated (incubation, transmissibility, stability or genetic variability, etc.) but also with the human host (human susceptibility, severity and the duration of the disease, the created immunity, the pattern and dynamics of the disease according to age and comorbidities) as well as the external factors that provide the opportunity for their appearance and development [19].
By globalization, we mean economic development and urbanization, which have led to greater mobility, including travel and the phenomenon of migration and the expansion of living space with the occupation of natural habitat and coexistence with animals (urban overcrowding) or expansion in cold climate or remote areas where exposure to the zoonotic reservoir is high (new, unknown infectious agents or exposure to transmission vectors). Also, the effect of urbanization has contributed to the occurrence of climate change due to environmental pollution and deforestation favoring habitats favorable to vectors (insects, animals, etc.) involved in the transmission and development of emerging/re-emerging infections. [20] The weakened public health infrastructure, failure to implement public health measures, war, civil revolts but also the change in individuals’ behavior (misunderstanding the seriousness of the risk presented by emerging infectious diseases, excessive consumption of anti-infectious drugs) are directly proportional to the increase in the risk of spreading favorable habitats and vectors involved in the transmission and development of new pandemics (Table 2. Risk factors involved in the development of (re)emerging infectious diseases).

{kind=link}
{kind=link}
| Risk Factors | Variables |
|---|---|
| Virus [19] |
|
| Human host [19] |
|
| External factors (medium) [20] |
|
3.3. The Characteristics of Pandemics and the Socioeconomic Implications Generated by (Re)emerging Infectious Disease
3.3.1. Characteristics
The impact of the pandemic on a population is different and is not fully characterized by the number of infections and deaths, so pandemics can be estimated in terms of transmissibility and severity of the disease, but also by the geographical area, by different moments and intensities, by human reactions as well as the prevention/combat strategies adopted by the authorities [21].
For example, we can quantify the basic reproduction number as a transmission potential parameter (R0, is the expected number of secondary cases produced by a primary case at the beginning of the infection (early phase of the outbreak); see “Sections 2 and 3 in [22] and Section 2 in [23] for the computation of the basic reproduction number in mathematical models of structured population dynamics (ecology and epidemiology)”. The pathogen severity can be quantified by health indicators (case fatality rate, (CFR%) death rate, number of deaths), with which we can quantify the severity of a pandemic [24,25].
In line with these, many countries have explored several strategies, from mitigation strategies (from hygiene measures and practices, to physical distancing measures, mobility or travel restrictions to full quarantine-like isolation) [17] to suppression strategies that were influenced by the transmissibility parameter (basic reproduction number—R0) obtained following the use of dynamic mathematical models used for forecasting the epidemiological evolution of emerging/re-emerging infectious diseases in different scenarios [21]. A value of R0 greater than 1 indicates that the infection may increase or persist in the population, while a value of R0 less than 1 indicates that the infection will decrease in the population, although there are exceptions. These R0 values are also important in the development and application of risk mitigation strategies by public authorities, as well as R0 also representing the difference between epidemics that are manageable and cause moderate illness and those that cause a significant number of illnesses and require intervention strategies [16,17]. Unfortunately, this parameter cannot measure the effects of public health interventions [26]. The COVID-19 pandemic has revived researchers’ interest in understanding how (re)emerging infectious diseases evolve and spread, but also interest in the use of predictive mathematical models to make predictions about the extent and impact of diseases, especially in early stages for better planning and management of interventions to mitigate these infections. Hence, the interest in these tools, which are being used more and more often, as they can express the extent and impact of (re)emerging infectious diseases both on short and long term. There are several models, from one that can make weekly estimates to models that can make regional estimates for simulating policy options, including vaccination, to models that are used for global modeling [27], but the SIR (susceptible, infectious, and/or recovered) for spread of disease model was mostly used for the evolution of the last months of the COVID-19 pandemic [28]. As we can see in Table 1. Characteristics of included studies in research, the estimation of the reproduction number proved to be very useful, providing an estimate of the susceptible population more precisely and the extent of transmission [29]. The variation of the reproduction number is directly related to the risk factors and effectiveness of infection mitigation/combat interventions. Thus, its high value—above 1—indicating a greater risk of spreading the disease and the need to implement new policies and programs to minimize infection. The results of these studies highlighted the need for the application of fast and targeted interventions, from the early stages, which can modify/alter the rate of transmission of the infectious agent and implicitly the evolution of the disease [17].
From a dynamism point of view, the size of the susceptible population dictates the force of infection, the process of contact and the history of disease [28]. At the beginning of the COVID-19 pandemic, the susceptible population was represented by elderly and those with existing comorbidities, but during the pandemic, new vulnerable people were considered due to the phenomenon of continuous mutation and dynamics of virus. This phenomenon has also contributed other factors such as geographical variation, immigration, the loss of immunity, the differences in surveillance, behaviors, the access to healthcare assistance and distribution by age groups [21].
Starting from this principle with Table 3. Elements of interest regarding pathogens that, through their characteristics, have influenced medical research, we can compare and capture the epidemic growth profiles within the outbreaks of Ebola, SARS, MERS, flu pandemic, and the outbreaks produced by viruses that could constitute future threats (Nipah, Hantavirus, etc.); see also, Table 1. Characteristics of included studies in research. Based on transmission and severity parameters from reports and data provided by the WHO, CDC, World Bank, and a group of experts (Imperial College London’s COVID-19 Response Team), this research attempts to summarize the most important and recent pandemics as well as the socioeconomic impact generated by (re)emerging infectious diseases and strategic interventions to mitigate their spread.
Thus, we can observe that, from the point of view of the transmission potential parameter (R0) and common characteristics, the COVID-19 pandemic was very similar to influenza pandemics (Spanish flu, Hong Kong flu and swine flu) spread around the world. The factors that favored this spread were the phenomenon of globalization, urbanization, mobilization and increasing severity for people with chronic diseases. In fact, the evolution model remains constant, the major triggers in development of pandemics being common elements, such as the way of transmission (respiratory tract and in some cases through contact with fluids), socioeconomic factors, globalization (Asia) or poverty (Africa) being the major triggers in the development of pandemics [17,19].
From the data presented by the World Bank in the 2019 pandemic preparedness report, we can see that in terms of severity (the number of deaths) the 1918 “Spanish flu” was the most devastating pandemic, killing more than 50 million people, while the 2009 H1N1 flu pandemic killed more than 18,000 people and the 2013–2016 Ebola outbreak killed 1300 people in Sierra Leone, Liberia and Guinea and more than 2000 people in the Republic of Congo [26]. Regarding the family of Coronaviruses, the new SARS-CoV-2 coronavirus with its viral variants, in terms of death, is the leader by far. It generated an unprecedented crisis with 6,679,319 deaths reported at the time of reporting [30], while for MERS (2012) were reported 935 of deaths, of which 854 deaths occurred in Saudi Arabia alone [31], and for SARS (2003) 800 deaths were reported worldwide [32,33] see in Table 3. Elements of interest on pathogens that, through their characteristics, have influenced medical research.
Table 3.
Elements of interest regarding pathogens that, through their characteristics, have influenced medical research.
Table 3.
Elements of interest regarding pathogens that, through their characteristics, have influenced medical research.
| Years | Virus/ Continent/ Epicentre | Items of Interest | Severity Criteria/ Risk of Spread (R0) | Estimated Costs |
|---|---|---|---|---|
| 2019 | Coronavirus SARS-CoV-2/Asia (China) | Member of the Coronaviridae Family. Origin: bats. Transmission: respiratory droplets and aerosol. Vulnerable groups: elderly | R0: 3.3–5.5 [9] R0: 3.6–4.0 [10] R0: 4.71(2019) and 2.08 (2020) [11] CFR: 3%; R0: 1.4–5.5 [12] 6,679,319 deaths worldwide [30] | €40.5 billion [18] |
| 2012–2015 | Coronavirus MERS-Co-V/Asia (Saudi Arabia) | Origin: bats. Coronaviridae family. Transmission: respiratory droplets. Vulnerable groups: elderly | CFR: 40%; 2502 cases and R0 < 1 [12] 2193 cases of infections, 858 deaths alone in Saudi Arabia and 2600 of cases with 935 deaths in 27 countries, CFR 34.4% [31] | $US 2.6 billion in lost tourism revenue [26] |
| 2003 | Coronavirus SARS-CoV-1/Asia (China) | Spread in 29 countries on 5 continents. The main factor that led to the spread of the virus was the high mobility of the population and the lack of measures to isolate the outbreak. Transmission: respiratory droplets. Vulnerable groups: elderly | R0: 2–5 and CFR 10% [12] 800 deaths worldwide and CFR 9–10% [32,33] | $US 6 billion [26] close to $40 billion [33] |
| 2001–2008 | Nipah virus/Asia (Malaysia and Singapore) | Paramyxoviridae family related to Hendra virus. Origin: bats. Transmission: bodily fluids, contaminate food. People can also develop asymptomatic infection. Symptoms include moderate to severe respiratory infection, and inflammation of the brain. | CFR: 40–70% and 700 cases from 1999–2018 WHO Southeast Asia [34] | |
| 1999 | Nipah virus/Asia (Bangladesh and India) | |||
| 2014-2016 | Ebola virus/ Africa (Sierra Leone, Guinea, Congo) | Member of the Filoviridae family Origin: Fruits bats, porcupines, and non-human primates. Transmission: bodily fluids. Vulnerable groups: health workers, women, and young children | R0: 1.5–2.5; CFR 70% [12] R0: 1.2–2.5 [35] CFR: 50%; Over 30,000 cases and 2100 deaths [36] | $US 4.3 billion to fight outbreaks. [18,36] |
| 1993 | Hantavirus/ US | Exposure to certain types of infected rodents can lead to infectious diseases. Pulmonary syndrome—detected in United States. Transmission: respiratory droplets and bodily fluids | 27 cases; R0 = 1.2 (0.8–1.6) [37] | |
| 2009 | Influenza virus—H1N1/ latin america (Mexico) | Origin: pig; Risk factors for the emergence of influenza viruses in humans are urban agglomerations (like South China Southeast Asia), where people live near animals. Transmission: Respiratory droplets. Vulnerable groups: teenagers, young adults. | CFR 0.03%; R0 = 1.2–1.6 [12] More than 150,000 people died into the first year and between 0.001–0.007% of the world’s population died due to respiratory problems in the first year the virus circulated [38] | $US 2.8 billion [26] |
| 1968-1969 | Influenza virus—H3N2 Hong Kong/Asia | Origin: porcin; Hong Kong Influenza A H2N2; Transmission: respiratory droplets. Vulnerable groups: elderly. | 1.1 million deaths 0.03 CFR [38] | |
| 1957-1958 | Influenza Influenza virus—H2N2 Asia (Southern China) | Origin: avian; bird flu; Influenza A H3N2. Transmission: respiratory droplets. Vulnerable groups: children and elderly | 1 million deaths 0.03 CFR [38,39] | |
| 1918–1919 | Influenza virus—H1N1 US | Origin: avian; bird flu. Influenza A H1N1. Transmission: respiratory droplets. Vulnerable groups: adults and pregnant women | CFR: 3%; R0: 1.4–3.8 [12] Over 50 million deaths and 3%CFR [38,40] |
In accordance with the data collected in the Table 3 Elements of interest regarding pathogens that, through their characteristics, have influenced medical research, if we compare the evolution pattern of emerging infectious diseases by means of the transmission potential and pathogen severity, we can observe that for those spread by direct or indirect contact such as: Nipah virus [34], Ebola virus [35,36] Hantavirus [37] MERS-CoV virus [31] and SARS-CoV-1 virus [32,33] tend to have a higher lethality (Nipah virus 40–70% [34], Ebola virus [35] 50%, SARS 10% [12,32,33], MERS 40% [12]) demonstrated their ability to develop global threats by severity. The virulence severity parameter (CFR) is higher when transmissibility is lower, meaning that although they were more severe (increased mortality) they did not have the ability to spread (R0 having values of/or below 1). Instead if we take into account the estimation R0 values and lethality values for respiratory viruses such as: H1N1/H5N1 (2009) [12,38], the H2N2 virus [38,39], the H1N1 1819 [12,38,40] and the new coronavirus SARS-CoV-2 [9,10,11,12], we can notice that respiratory viruses tend to have a higher R0 value than those spread by direct or indirect contact and demonstrated their ability to develop global threats through high transmission and potential for spread, see the estimated R0 value for each (value significantly greater than 1).
Based on the experience gained from outbreaks of Ebola, SARS and flu pandemics, using mathematical modelling, a group of experts from Imperial College in the United Kingdom predicted that, in the absence of social distancing measures and adequate treatment with antivirals or vaccines, in the case of the COVID-19 pandemic, there will be at least several hundred thousand casualties in UK alone. Also, by using mathematical modelling, the same group of experts estimated that, in the absence of interventions, people living in poverty with limited access to healthcare or limited access to running water and populations whose jobs do not allow social distancing, the probability of death from COVID-19 increases by 32%, 12.4%, 9.2% and 6%, respectively, for populations where social distancing is not possible [15]. Another estimate using mathematical models predicted that 20 million lives could be saved by carrying out interventions and through vaccination 30.7 million lives could be saved [16]. At the same time, Professor Neil Ferguson emphasized that the team’s work went beyond the center (Imperial College) and highlighted the need for international collaboration and the continuation of research in the medical and technological fields, even if vaccination and the fight against new viral variants have begun, because only by understanding the virus and its mode of transmission we will be able to control it [29].
3.3.2. The Measures Implemented and the Socioeconomic Implications
Zoonotic pandemics are very costly, from direct costs (those related to healthcare) to indirect costs (loss of productivity—jobless and care of sick relatives, quarantine and closing school, social distancing measures and the temporary closing of shopping malls, institutions and local or international transport companies) as well as intangible costs such as loss of human life, so anticipating and preventing emerging/re-emerging infectious diseases is necessary and cost effective.
Severe acute respiratory syndrome (SARS) was a good example of an emerging infection with severe indirect costs, as it was responsible for considerable economic losses and insecurity in financial markets in Asia and around the world. In a single outbreak, severe acute respiratory syndrome virus wiped between 10 and 50 billion US dollars (USD) off Asian stock markets due to trade disruption [26,33] compared to MERS in 2009, when 2.6 billion USD was lost in tourism revenue or 4.3 billion USD for interventions to reduce the impact of the Ebola outbreak in 2014 [18,36].
The 2019 joint report by the World Health Organization and the World Bank estimated that losses from a severe influenza pandemic could reach approximately 3 trillion USD per year [26] and the International Monetary Fund highlighted that middle-income and lower-income countries are more vulnerable to an outbreak than high-income countries, and losses are disproportionately due to poverty, poor access to healthcare and unaffordability. The COVID-19 pandemic has created an unprecedented global crisis, with the European Union launching support initiatives for countries with fragile healthcare systems (“Team Europe” on 8 April 2020) and mobilizing 40.5 billion euros. [26] Also, the EU established an EU recovery plan after the COVID-19 pandemic, allocating a total budget of EUR 1824 billion for the period 2021–2027 to support the development of digital infrastructures. The COVID-19 pandemic was differentiated from previous pandemics by the digital strategies applied against the background of the crisis, economic and social activities are increasingly accessed through digital infrastructures, allowing us to learn, work and socialize. Also, the use of contact tracing and population warning applications regarding self-isolation, testing, contact tracing and the use of artificial intelligence in detecting the spread patterns of the coronavirus have allowed public health sectors to develop rapid reactions and effective strategies against the coronavirus [41].
To anticipate and prevent(re)emerging infectious diseases we must prepare for future health crises by investing in the research and development of technologies capable of providing an adapting rapid and effective response against new global threats.
At the same time, there must be a unified and equitable approach that provides support to countries with fragile healthcare systems, an approach that has also proven cost-effective and effective in recent Ebola outbreaks [36] by strengthening the response capacities and preparedness for providing treatments, vaccines, medical supplies and equipment [42].
4. Discussion
What have we learned about how we should control or address these pandemics? It remains an open question.
Developing strategies to mitigate the severity of a new pandemic is now a top global public health priority. The penetration of the wildlife habitat, due to globalization and economic development, and exposure to the zoonotic reservoir and vectors involved in the transmission and development of (re)emerging infections, shows that new microbial threats will continue to emerge at an accelerated rate [42].
The COVID-19 pandemic has revived interest in the estimation of the basic reproduction number as a potentially extremely important transmission parameter in forecasting the magnitude and impact of a pandemic in the early phase of an outbreak. A high value of this indicating that the risk of increasing infection is high and requires investments, policies and intervention strategies, a fact also confirmed by the high costs [18] and the application of targeted strategies from the early stages, thus changing the evolution of the disease [29]. Pandemics also cannot be solved unless global inequality is considered and there is no unified and equitable international approach for countries with fragile health systems, the goal being to achieve sustainable and equitable health [43].
Limitations: the selection of the population of each considered study may hide some biases as well as not be fully representative. This revision has some limitations in that studies sometimes do not fully specify prevention measures and countries may have different levels of healthcare; therefore, the response to stress and crisis may vary.
5. Future Suggestions and Lessons for the Future Pandemics
As a lesson from the past but also as a strategy for the future, the existence of international solidarity (the existence of international conventions and regulations), equity regarding access to tests, treatments and vaccines and multisectoral monitoring is necessary to achieve a quick, unified and adapted global response [43]. Global inequality, lack of education, poverty and community infrastructure can facilitate new emerging infectious diseases or favor the return of old ones that humanity considers eradicated [44].
6. Conclusions
The COVID-19 pandemic response differentiated itself from other pandemics by using artificial intelligence to detect the spread patterns of the coronavirus that allowed the healthcare sectors to develop effective strategies and rapid reactions in the fight against COVID-19 while also raising an alarm signal indicating that the fight against emerging/re-emerging infectious diseases is far from being won, and without investment in research and development of new intervention strategies we may find ourselves unprepared for a new threat.
Based on the results of this qualitative synthesis, we can now provide some answers to the questions proposed at the beginning of our review.
What were the most important emerging/re-emerging infectious disease pandemics and what were the risk factors?
The importance of pandemics is shown by the implications they generate, the degree of transmissibility and severity as well as human reactions and the capacity of public healthcare systems to react to them. As this research shows, depending on the characteristics of the pathogens and the parameters studied, each pandemic is important. Menaces of the future (Nipah virus, Hantavirus and the coronavirus family) have demonstrated their ability to develop global threats, being possible triggers in the development of important pandemics in future, which is why we must assign special importance to all of them and prepare through an intensification of investments in research and development of technologies by establishing international agreements to provide support to countries with deficient healthcare systems because an infectious pathogen that we may not yet be aware of, or consider eradicated [44], could trigger a new pandemic.
What have the socioeconomic implications of emerging/re-emerging infectious diseases been and what important lessons have we learned from them?
The socioeconomic implications of (re)emerging infectious diseases are multiple, from direct costs to indirect costs and intangible costs such as loss of human life, so the anticipation and prevention of pandemics is effective but also cost-effective. To anticipate and prevent these pandemics, we need to deepen the characteristics of epidemic/pandemic growth patterns, especially in the early stages, to generate useful forecasts for decision-making by authorities and to intervene quickly to minimize/alter the transmission rate of potentially dangerous pathogens in triggering pandemics [18].
What future clues or lessons should be implemented to prevent/stop a new pandemic based on experience?
After comparing the characteristics of transmission and severity, we found out that the most recent pandemics had the same pattern of evolution and other common characteristics. To deal with new threats, humanity must have a mechanism that provides international solidarity, equity in treatments and vaccines as well as investing in the development of innovative technologies that allow monitoring of risk areas and identify new pathogens to anticipate certain future threats [41].
How does a virus spread and what is the progression of the disease?
This is still an open question; the history of pandemics shows us that the evolution and impact of a pandemic depend on the risk factors, the evolution model, the characteristics of the virus as well as human reactions. The complexity of this struggle is also contributed to by climate change, globalization, geographical variations, population and age group distribution, coexistence with animals (zoonotic reservoir) as well as human actions and the late response or lack of response from the authorities.
Author Contributions
Conceptualization: G.-V.B.E., D.A.T., A.B. and D.M.; Methodology: G.-V.B.E., D.A.T., A.B. and D.M.; Project administration: G.-V.B.E. and D.A.T.; Validation: G.-V.B.E., D.A.T., A.B. and D.M.; Writing—original draft preparation G.-V.B.E., D.A.T., A.B. and D.M.; Writing—review and editing: G.-V.B.E. and D.A.T. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Being a qualitative narrative review synthesis, data were collected from the literature following our original search method described in the manuscript so that, the data being from studies or reports published online, neither ethical approval nor individual consent was required.
Conflicts of Interest
The author declares no conflict of interest.
References
- WHO. Prioritizing Diseases for Research and Development in Emergency Contexts. 2018. Available online: https://www.who.int/activities/prioritizing-diseases-for-research-and-development-in-emergency-contexts (accessed on 21 April 2020).
- Burkle, F.M., Jr. Globalization and Disasters: Issues of Public Health, State Capacity and Political Action. J. Int. Aff. 2006, 59, 241–265. [Google Scholar]
- Jones, K.E.; Patel, N.G.; Levy, M.A.; Storeygard, A.; Balk, D.; Gittleman, J.L.; Daszak, P. Global trends in emerging infectious diseases. Nature 2008, 451, 990–993. [Google Scholar] [CrossRef] [PubMed]
- Akin, L.; Gözel, M.G. Understanding dynamics of pandemics. Turk. J. Med. Sci. 2020, 50, 515–519. Available online: http://journals.tubitak.gov.tr/medical/ (accessed on 8 April 2020). [CrossRef] [PubMed]
- Schar, D.L.; Yamey, G.M.; Machalaba, C.C.; Karesh, W. A framework for stimulating economic investments to prevent emerging diseases. Bull. World Health Organ. 2017, 96, 138–140. [Google Scholar] [CrossRef]
- Heesterbeek, H.; Anderson, R.M.; Andreasen, V.; Bansal, S.; De Angelis, D.; Dye, C.; Eames, K.T.D.; Edmunds, W.J.; Frost, S.D.W.; Funk, S.; et al. Threats. Science 2015, 347, aaa4339. [Google Scholar] [CrossRef] [Green Version]
- Li, Q.; Guan, X.; Wu, P.; Wang, X.; Zhou, L.; Tong, Y.; Ren, R.; Leung, K.S.M.; Lau, E.H.Y.; Wong, J.Y.; et al. Early transmission dynamics in Wuhan, China, of novel coronavirus–infected pneumonia. N. Engl. J. Med. 2020, 382, 1199–1207. [Google Scholar] [CrossRef]
- Bi, Q.; Wu, Y.; Mei, S.; Ye, C.; Zou, X.; Zhang, Z.; Liu, X.; Wei, L.; Truelove, S.A.; Zhang, T.; et al. Epidemiology and Transmission of COVID-19 in Shenzhen China: Analysis of 391 Cases and 1286 of Their Close Contacts. 2020. Available online: https://www.medrxiv.org/content/10.1101/2020.03.03.20028423v3 (accessed on 8 April 2020).
- Zhao, S.; Lin, Q.; Ran, J.; Musa, S.S.; Yang, G.; Wang, W.; Lou, Y.; Gao, D.; Yang, L.; He, D.; et al. Preliminary estimation of the basic reproduction number of novel coronavirus (2019-nCoV) in China, from 2019 to 2020: A data-driven analysis in the early phase of the outbreak. bioRxiv 2020. [Google Scholar] [CrossRef] [Green Version]
- Read, J.M.; Bridgen, J.R.; Cummings, D.A.; Ho, A.; Jewell, C.P. Novel coronavirus 2019-nCoV: Early estimation of epidemiological parameters and epidemic predictions. medRixiv 2020. [Google Scholar] [CrossRef] [Green Version]
- Shen, M.; Peng, Z.; Xiao, Y. Modelling the epidemic trend of the 2019 novel coronavirus outbreak in China. bioRxiv 2020, in press. [Google Scholar] [CrossRef]
- Chen, J. Pathogenicity and transmissibility of 2019-nCoV-A quick overview and comparison with other emerging viruses. Microbes Infect. 2020, 22, 69–71. [Google Scholar] [CrossRef]
- Wu, J.T.; Leung, K.; Bushman, M.; Kishore, N.; Niehus, R.; de Salazar, P.M.; Cowling, B.J.; Lipsitch, M.; Leung, G.M. Estimating clinical severity of COVID-19 from the transmission dynamics in Wuhan, China. Nat. Med. 2020, 26, 506–510. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Feng, S.; Feng, Z.; Ling, C.; Chang, C.; Feng, Z. Prediction of the COVID-19 epidemic trends based on SEIR and AI models. PLoS ONE 2021, 16, e0245101. [Google Scholar] [CrossRef] [PubMed]
- Winskill, P.; Whittaker, C.; Walker, P.; Watson, O.; Laydon, D.; Imai, N.; Cuomo-Dannenburg, G.; Ainslie, K.; Baguelin, M.; Bhatt, S. Equity in Response to the COVID-19 Pandemic: An Assessment of the Direct and Indirect Impacts on Disadvantaged and Vulnerable Populations in Low- and Lower Middle-Income Countries. Imperial College London (12-05-2020). Available online: https://spiral.imperial.ac.uk/handle/10044/1/78965 (accessed on 18 December 2022).
- Walker, P.; Whittaker, C.; Watson, O.; Baguelin, M.; Ainslie, K.; Bhatia, S.; Bhatt, S.; Boonyasiri, A.; Boyd, O.; Cattarino, L.; et al. The Global Impact of COVID-19 and Strategies for Mitigation and Suppression. Imperial College London (26-03-2020). Available online: https://spiral.imperial.ac.uk/handle/10044/1/77735 (accessed on 18 December 2022).
- Ferguson, N.; Laydon, D.; Nedjati Gilani, G.; Imai, N.; Ainslie, K.; Baguelin, M.; Bhatia, S.; Boonyasiri, A.; Cucunuba Perez, Z.; Cuomo-Dannenburg, G.; et al. Impact of Non-Pharmaceutical Interventions (NPIs) to Reduce COVID-19 Mortality and Healthcare Demand. Imperial College London (16-03-2020). Available online: https://spiral.imperial.ac.uk/handle/10044/1/77482 (accessed on 18 December 2022).
- European Council. Coiuncil of the European Union. Global Solidarity during the COVID-19 Pandemic. Available online: https://www.consilium.europa.eu/en/policies/coronavirus/global-solidarity/ (accessed on 3 August 2022).
- Van Damme, W.; Dahake, R.; Delamou, A.; Ingelbeen, B.; Wouters, E.; Vanham, G.; Van De Pas, R.; Dossou, J.-P.; Ir, P.; Abimbola, S.; et al. The COVID-19 pandemic diverse contexts; different epidemics-how and why? BMJ Glob. Health 2020, 5, e003098. [Google Scholar] [CrossRef] [PubMed]
- Findlater, A.; Bogoch, I.I. Human Mobility and the Global Spread of Infectious Diseases: A Focus on Air Travel. Trends Parasitol. 2018, 34, 772–783. [Google Scholar] [CrossRef]
- Heffernan, J.M.; Smith, R.J.; Wahl, L.M. Perspectives on the basic reproductive ratio. J. R. Soc. Interface R. Soc. 2005, 2, 281–293. [Google Scholar] [CrossRef] [PubMed]
- Barril, C.; Calsina, A.; Ripoll, J. A practical approach to R0 in continuous-time ecological models. Math. Meth. Appl. Sci. 2017, 41, 8432–8445. [Google Scholar] [CrossRef]
- Breda, D.; Florian, F.; Ripoll, J.; Vermiglio, R. Efficient numerical computation of the basic reproduction number for structured populations. J. Comput. Appl. Math. 2021, 384, 113165. [Google Scholar] [CrossRef]
- Last, J.M. (Ed.) . A Dictionary of Epidemiology, 4th ed.; Oxford University Press: New York, NY, USA, 2001. [Google Scholar]
- Mercer, G.; Glass, K.; Beckers, N. Effective reproduction numbers are commonly overestimated early in a disease outbreak. Stat. Med. 2011, 30, 984–994. [Google Scholar] [CrossRef]
- European Parliamentary Research Service. Economic Impact of Epidemics and Pandemics. Available online: https://www.europarl.europa.eu/thinktank/en/document/EPRS_BRI(2020)646195 (accessed on 3 August 2022).
- Imperial College COVID-19 Response Team. Available online: http://www.imperial.ac.uk/mrc-global-infectious-disease-analysis/covid-19/ (accessed on 18 December 2022).
- Lessler, J.; Azman, A.S.; Grabowski, M.K.; Salje, H.; Rodriguez-Barraquer, I. Trends in the mechanistic and dynamic modeling of infectious diseases. Curr. Epidemiol. Rep. 2016, 3, 212–222. [Google Scholar] [CrossRef] [Green Version]
- Centers for Disease Control and Prevention. Prioritizing COVID-19 Contact Tracing Mathematical Methods and Findings. Available online: www.cdc.gov/coronavirus/2019-ncov/php/contact-tracing/contact-tracingresources.htm (accessed on 8 August 2022).
- Worldmater. COVID-19 Coronavirus Pandemic. Available online: https://www.worldometers.info/coronavirus/ (accessed on 16 December 2022).
- World Health Organization. Middle East Respiratory Syndrome Coronavirus (MERS-CoV). Available online: https://www.who.int/emergencies/disease-outbreak-news/item/2022-DON422 (accessed on 16 December 2022).
- Saywell, T.; Fowler, G.A.; Crispin, S.W.; Borsuk, R.; Cohen, M. The cost of SARS: $11 billion and rising. Dow Jones Far East. Econ. Rev. 2003, 166, 12–17. [Google Scholar]
- Flu Outbreaks Reminder of Pandemic Threat; The World Bank: Washington, DC, USA, 2013; Available online: https://www.worldbank.org/en/news/feature/2013/03/05/flu-outbreaks-reminder-of-pandemic-threat (accessed on 18 April 2020).
- World Health Organization. Health Topics. Nipah Virus Infection, Overview. Symptoms. Treatment. Available online: https://www.who.int/health-topics/nipah-virus-infection#tab=tab_1 (accessed on 3 August 2022).
- Van Kerkhove, M.D.; Bento, A.I.; Mills, H.L.; Ferguson, N.M.; Donnelly, C.A. A review of epidemiological parameters from Ebola outbreaks to inform early public health decision-making. Sci. Data 2015, 2, 150019. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Bank. Pandemics. Brief. Ebola outbreak in Democratic Republic of Congo. Available online: https://www.worldbank.org/en/topic/pandemics/brief/fact-sheet-world-bank-support-to-10th-ebola-outbreak-in-democratic-republic-of-congo (accessed on 18 April 2021).
- Centers for Disease Control and Prevention. Hantavirus. Reportet Cases of Hantavirius. Available online: https://www.cdc.gov/hantavirus/index.html (accessed on 20 December 2022).
- Centers for Disease Control and Prevention. 2009 H1N1 Pandemic. (H1N1 pdm09 Virus). Available online: https://www.cdc.gov/flu/pandemic-resources/2009-h1n1-pandemic.html (accessed on 20 December 2022).
- Centers for Disease Control and Prevention 1957–1958 Pandemic (H2N2 Virus). Available online: https://www.cdc.gov/flu/pandemic-resources/1957-1958-pandemic.html (accessed on 20 December 2022).
- Centers for Disease Control and Prevention. History of 1918 Flu Pandemics. Available online: https://www.cdc.gov/flu/pandemic-resources/1918-commemoration/1918-pandemic-history.htm (accessed on 20 December 2022).
- European Council. Council of the European Union. EU’s Response to COVID-19. An International Treaty on Pandemic, Prevention, and Preparedness. Available online: https://www.consilium.europa.eu/en/policies/coronavirus/pandemic-treaty/ (accessed on 3 August 2022).
- WHO Director-General’s Opening Remarks at the Global Preparedness Monitoring Board (GPMB) Board Meeting Hosted/Organised by: GPMB Secretariat. Available online: https://www.who.int/director-general/speeches/detail/who-director-general-s-opening-remarks-at-the-global-preparedness-monitoring-board-(gpmb)-board-meetinghosted-organised-by--gpmb-secretariat (accessed on 30 September 2022).
- Remarks of General Secretary of ONU, Summit 26 March 2020. Available online: www.un.org/sg/en/content/sg/statement/2020-03-26/secretary-generals-remarks-g-20-virtual-summit-the-covid-19-pandemic (accessed on 18 April 2021).
- Carrol, D.; Watson, B.; Togami, E.; Daszak, P.; Mczet, J.A.; Chrisman, C.J.; Rubin, E.M.; Wolfe, N.; Morel, C.M.; Gao, G.F.; et al. Building a global atlas of zoonotic viruses. Bull. World Health Organ. 2018, 96, 292–294. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Flow diagram of literature search, screening, inclusion and exclusion of studies.

Figure 2.
Pathogens that have caused epidemics in the modern world for each continent.

Table 1.
Characteristics of the included studies in research.
| Authors/References | Virus/Year | Type of Study/Contribution/Results |
|---|---|---|
| Li Q, Guan X et al., 2020 [7] | SARS-CoV-2 (2019) | 425 cases with confirmed pneumonia, with average age of 59 years from which 56% were men; 55% of cases with onset before 1 January 2020, associated with epicenter Wuhan Seafood Market, Hubei, China R0 = 2.2 (95% CI 1.4–3.9), mean 7.5 days (95% CI, 5.3–19). Prevention and transmission reduction measures should be implemented in the population at risk |
| Bi Qifang, Yong Sheng Wu et al., 2020 [8] | SARS-CoV2 (2019) | Data collected from Shenzhen Center for Disease Control and Prevention, Hubei, China from 14 January to 12 February 2020. From 391 confirmed cases, 204 were women and 187 men with average age of 45 years; 91% of cases with moderate clinical signs; cases were isolated on average 4.6 days after the development of symptoms. R0 = 0.4 |
| Zaho S et al., 2020 [9] | SARS-CoV-2 (2019) | Modeling the epidemic curve, China, 10–24 January 2020; have demonstrated the high potential to generate outbreaks of infection. Mean R0 ranged from 2.24 (95% CI 1.96–2.55) to 3.58 (95% CI 2.89–4.39) in the early phases, values significantly greater than 1. |
| Read J et al., 2020 [10] | SARS-CoV-2 (2019) | Early estimate of reproductive rate and case fatality rate (CFR%) for cases in Wuhan, China R0 = 3.1 (95%CI; 2.39–4.13) 58–76% transmission should be prevented to decrease risk of infection; the R0 estimates were comparable to SARS and MERS in the early periods. |
| Shen et al., 2020 [11] | SARS-CoV-2 (2019) | Diagnosis and the establishment of non-pharmacological interventions are essential in controlling the epidemic curve. R0 = 4.71 (4.50–4.92) at the beginning of the pandemic then decreased to 2.08 (1.99–2.18) on 22 January 2020 Comparing SARS and MERS had similar values for SARS (4.91) in Beijing, China (2003) and 3.5–6.7 for MERS in Saudi Arabia (2014). |
| Chen et al., 2020 [12] | SARS-CoV-2 (2019) | SEIR model, Pathogenicity and transmissibility of 2019-nCoV- compared to other emerging viruses. CFRSARS-CoV-2 = 3, R0 = 1.4–5.5 |
| SARS-CoV (2003) | CFR 10%; R0 = 2–5. | |
| MERS-CoV (2009) | CFR 40%; R0 < 1. | |
| H5N1/H1N1 (2009) | CFR 0.03%; R0 = 1.2–1.6. | |
| H1N1 (1918) | CFR 3%; R0 = 1.4–3.8. | |
| Ebola virus (2014) | CFR 70%; R0 = 1.5–2.5 | |
| Wu JT et al., 2020 [13] | SARS-CoV-2 (2019) | SEIR model, sensitivity analysis to understand infectious spread trend for China. R0 = 2.7, 95% CI, for Wuhan, China. CFR 1.4% (95% CI 0.9%–2.1%); the risk of symptomatic infections increases with age |
| S. Feng, Z. Feng [14] | SARS-CoV-2 (2019) | Prediction trends epidemics of COVID-19 on the basis SEIR and AI models Estimate transmission rates and death rates |
| Peter Winskill, Charlie Whittaker, Patrick Walker et al. Imperial College London (12 May 2020) [15] | SARS-CoV-2 (2019) | Report 22: Equity as a response the direct and indirect impact due to evolution the COVID-19 pandemic, on populations vulnerable in the countries with low and moderate incomes. The growth probability of death through COVID-19 by 32% in the poor population, with 12.4% for the populations that had limited access to medical services, with 9.2% for those with limitation to running water and by 6% due to their job—unable to social distancing. |
| Patrick GT Walker, Charles Whittaker, Oliver Watson et al. Imperial College London (26 March 2020) [16] | SARS-CoV-2 (2019) | Report 12: The Global Impact of COVID-19 and Strategies for Mitigation and Suppression The research combine data on age-specific contact patterns and COVID-19 severity to project the health impact in 202 countries (in the countries with low-income the risk profile for COVID-19 could be different from that observed in China, Europe, and North America). It was estimated that without interventions there would be 7.0 billion infections and 40 million deaths worldwide in one year and with interventions based on decreasing transmission such as a 40% decrease in social contacts, 20 million lives could be saved and through the early introduction of isolation, quarantine, testing and vaccination measures, 30.7 million lives could be saved. |
| Neil M Ferguson, Daniel Laydon, Gemma Nedjati-Gilani et al. Imperial College London (16 March 2020) [17] | SARS-CoV-2 (2019) | Report 9: microsimulation model performed in UK (Great Britain) and US: Impact of Non-Pharmaceutical Interventions (NPIs) on Reducing COVID-19 Mortality and Healthcare Demand. Two fundamental strategies were debated: -mitigation using NPIs (isolation, quarantine, social distancing), strategy adopted by some US cities in 1918, and by the world in 1957, 1968 and 2009 influenza pandemic, which, according to estimates, would lead to a 50% decrease in requests for medical assistance and -suppression (decrease R0 to 1 or below 1, as for SARS or Ebola) to reduce cases and implicitly eliminate human-to-human transmission, which should be maintained until immunity is obtained or until the virus circulates. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Ene, G.-V.B.; Mănuc, D.; Bordianu, A.; Todea, D.A. The Pandemic Puzzle—Reviewing the Existing Pieces, Searching for the Missing Ones. Sustainability 2023, 15, 5214. https://doi.org/10.3390/su15065214
AMA Style
Ene G-VB, Mănuc D, Bordianu A, Todea DA. The Pandemic Puzzle—Reviewing the Existing Pieces, Searching for the Missing Ones. Sustainability. 2023; 15(6):5214. https://doi.org/10.3390/su15065214
Chicago/Turabian StyleEne, Gianina-Valentina Băcescu, Daniela Mănuc, Anca Bordianu, and Doina Adina Todea. 2023. "The Pandemic Puzzle—Reviewing the Existing Pieces, Searching for the Missing Ones" Sustainability 15, no. 6: 5214. https://doi.org/10.3390/su15065214
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.