
SARS-CoV-2 Reinfection among Healthcare Workers in Mexico: Case Report and Literature Review

 ,
,
Abstract
:1. Introduction
2. Methods
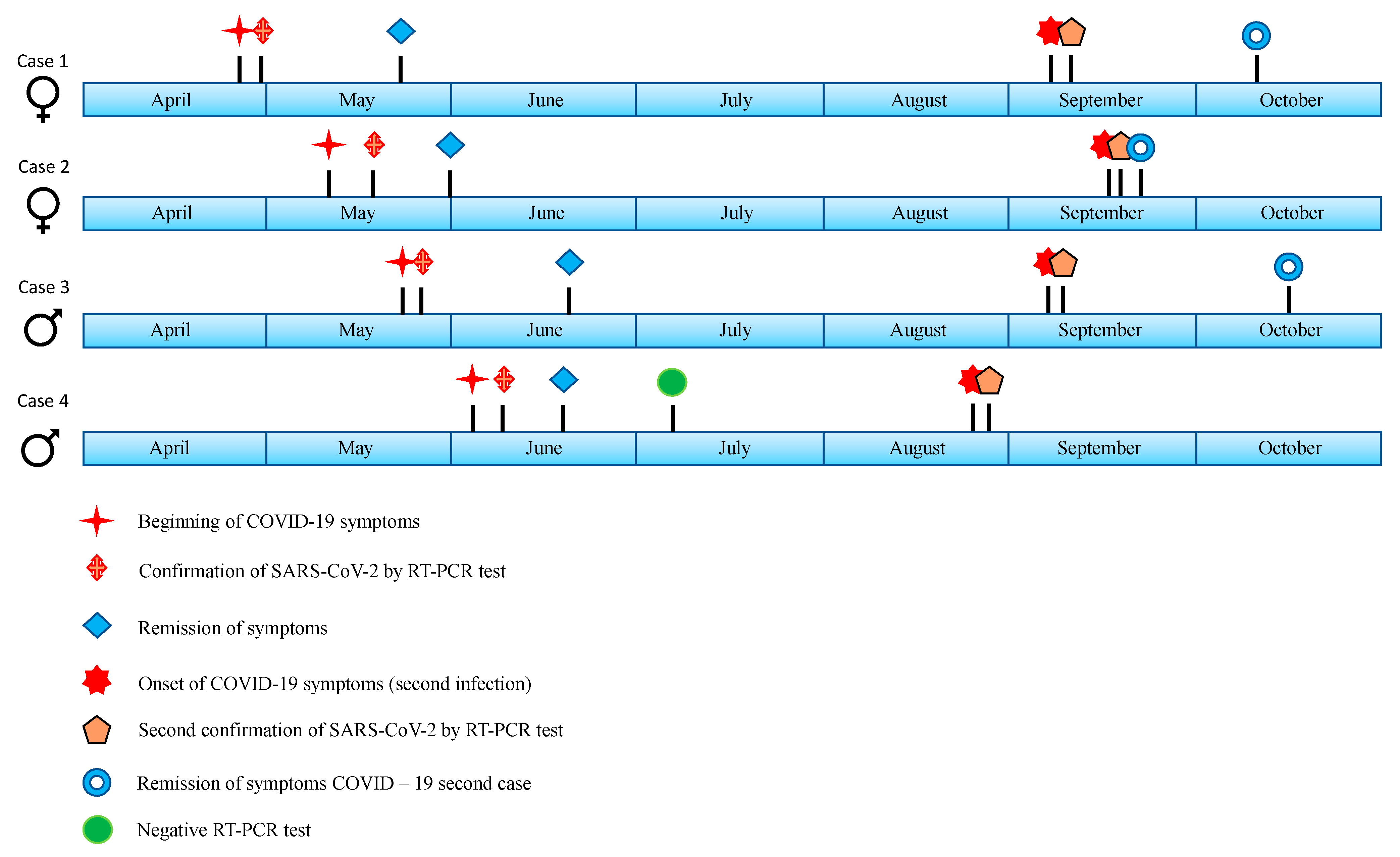
3. Case Reports
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Suárez, V.; Suarez Quezada, M.; Oros Ruiz, S.; Ronquillo De Jesús, E. Epidemiología de COVID-19 en México: Del 27 de febrero al 30 de abril de 2020. Rev. Clín. Esp. 2020, 220, 463–471. [Google Scholar] [CrossRef]
- Centro de Produccion CEPROPIE. Informe Diario Sobre Coronavirus COVID-19 en México. Secretaría de Salud. Martes 23 de Marzo [Internet]. 2021. Available online: https://www.youtube.com/watch?v=t4UraPe7bZc&ab_channel=CENTRODEPRODUCCIONCEPROPIE (accessed on 23 March 2021).
- CSSEGISandData. CSSEGISandData/COVID-19 [Internet]. 2021. Available online: https://github.com/CSSEGISandData/COVID-19 (accessed on 7 March 2021).
- Mehta, S.; Machado, F.; Kwizera, A.; Papazian, L.; Moss, M.; Azoulay, É.; Herridge, M. COVID-19: A heavy toll on health-care workers. Lancet Respir. Med. 2021, 9, 226–228. [Google Scholar] [CrossRef]
- Bandyopadhyay, S.; Baticulon, R.E.; Kadhum, M.; Alser, M.; Ojuka, D.K.; Badereddin, Y.; Kamath, A.; Parepalli, S.A.; Brown, G.; Iharchane, S.; et al. Infection and mortality of healthcare workers worldwide from COVID-19: A systematic review. BMJ Glob. Health 2020, 5, e003097. [Google Scholar] [CrossRef]
- Demos, E.; Martínez, Á.C. La Jornada—Enfermaron de Covid 195,558 Trabajadores de Salud en México [Internet]. Available online: https://www.jornada.com.mx (accessed on 15 March 2021).
- Agren, D. Understanding Mexican health worker COVID-19 deaths. Lancet 2020, 396, 807. [Google Scholar] [CrossRef]
- van Kampen, J.J.; van de Vijver, D.A.; Fraaij, P.L.; Haagmans, B.L.; Lamers, M.M.; Okba, N.; van den Akker, J.P.; Endeman, H.; Gommers, D.A.; Cornelissen, J.J.; et al. Duration and key determinants of infectious virus shedding in hospitalized patients with coronavirus disease-2019 (COVID-19). Nat. Commun. 2021, 12, 267. [Google Scholar] [CrossRef]
- Tomassini, S.; Kotecha, D.; Bird, P.W.; Folwell, A.; Biju, S.; Tang, J.W. Setting the criteria for SARS-CoV-2 reinfection—Six possible cases. J. Infect. 2021, 82, 282–287. [Google Scholar] [CrossRef]
- Yahav, D.; Yelin, D.; Eckerle, I.; Eberhardt, C.S.; Wang, J.; Cao, B.; Kaiser, L. Definitions for COVID-19 reinfection, relapse and PCR re-positivity. Clin. Microbiol. Infect. 2021, 27, 315–318. [Google Scholar] [CrossRef] [PubMed]
- Chen, D.; Xu, W.; Lei, Z.; Huang, Z.; Liu, J.; Gao, Z.; Peng, L. Recurrence of positive SARS-CoV-2 RNA in COVID-19: A case report. Int. J. Infect. Dis. 2020, 93, 297–299. [Google Scholar] [CrossRef] [PubMed]
- Ye, G.; Pan, Z.; Pan, Y.; Deng, Q.; Chen, L.; Li, J.; Li, Y.; Wang, X. Clinical characteristics of severe acute respiratory syndrome coronavirus 2 reactivation. J. Infect. 2020, 80, e14–e17. [Google Scholar] [CrossRef] [PubMed]
- Osman, A.A.; Al Daajani, M.M.; Alsahafi, A.J. Re-positive coronavirus disease 2019 PCR test: Could it be a reinfection? New Microbes New Infect. 2020, 37, 100748. [Google Scholar] [CrossRef]
- Li, J.; Zhang, L.; Liu, B.; Song, D. Case Report: Viral Shedding for 60 Days in a Woman with COVID-19. Am. J. Trop. Med. Hyg. 2020, 102, 1210–1213. [Google Scholar] [CrossRef]
- de Brito, C.A.A.; Lima, P.M.A.; de Brito, M.C.M.; de Oliveira, D.B. Second Episode of COVID-19 in Health Professionals: Report of Two Cases. Int. Med. Case Rep. J. 2020, 13, 471–475. [Google Scholar] [CrossRef]
- Ravioli, S.; Ochsner, H.; Lindner, G. Reactivation of COVID-19 pneumonia: A report of two cases. J. Infect. 2020, 81, e72–e73. [Google Scholar] [CrossRef] [PubMed]
- Popovici, J.; Pierce-Friedrich, L.; Kim, S.; Bin, S.; Run, V.; Lek, D.; Hee, K.H.D.; Lee Soon-U, L.; Cannon, M.V.; Serre, D.; et al. Recrudescence, Reinfection, or Relapse? A More Rigorous Framework to Assess Chloroquine Efficacy for Plasmodium vivax Malaria. J. Infect. Dis. 2019, 219, 315–322. [Google Scholar] [CrossRef]
- Gousseff, M.; Penot, P.; Gallay, L.; Batisse, D.; Benech, N.; Bouiller, K.; Collarino, R.; Conrad, A.; Slama, D.; Joseph, C.; et al. Clinical recurrences of COVID-19 symptoms after recovery: Viral relapse, reinfection or inflammatory rebound? J. Infect. 2020, 81, 816–846. [Google Scholar] [CrossRef] [PubMed]
- Korber, B.; Fischer, W.M.; Gnanakaran, S.; Yoon, H.; Theiler, J.; Abfalterer, W.; Hengartner, N.; Giorgi, E.E.; Bhattacharya, T.; Foley, B.; et al. Tracking Changes in SARS-CoV-2 Spike: Evidence that D614G Increases Infectivity of the COVID-19 Virus. Cell 2020, 182, 812–827. [Google Scholar] [CrossRef] [PubMed]
- Iwasaki, A. What reinfections mean for COVID-19. Lancet Infect. Dis. 2021, 21, 3–5. [Google Scholar] [CrossRef]
- To, K.K.W.; Hung, I.F.N.; Ip, J.D.; Chu, A.W.H.; Chan, W.M.; Tam, A.R.; Fong, C.H.Y.; Yuan, S.; Tsoi, H.W.; Ng, A.C.K.; et al. Coronavirus Disease 2019 (COVID-19) Re-infection by a Phylogenetically Distinct Severe Acute Respiratory Syndrome Coronavirus 2 Strain Confirmed by Whole Genome Sequencing. Clin. Infect. Dis. 2020. [Google Scholar] [CrossRef]
- Van Elslande, J.; Vermeersch, P.; Vandervoort, K.; Wawina-Bokalanga, T.; Vanmechelen, B.; Wollants, E.; Laenen, L.; André, E.; Van Ranst, M.; Lagrou, K.; et al. Symptomatic Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2) Reinfection by a Phylogenetically Distinct Strain. Clin. Infect. Dis. 2020. [Google Scholar] [CrossRef]
- Tillett, R.L.; Sevinsky, J.R.; Hartley, P.D.; Kerwin, H.; Crawford, N.; Gorzalski, A.; Laverdure, C.; Verma, S.C.; Rossetto, C.C.; Jackson, D.; et al. Genomic evidence for reinfection with SARS-CoV-2: A case study. Lancet Infect. Dis. 2021, 21, 52–58. [Google Scholar] [CrossRef]
- Prado-Vivar, B.; Becerra-Wong, M.; Guadalupe, J.J.; Marquez, S.; Gutierrez, B.; Rojas-Silva, P.; Grunauer, M.; Trueba, G.; Barragan, V.; Cardenas, P. COVID-19 Re-Infection by a Phylogenetically Distinct SARS-CoV-2 Variant, First Confirmed Event in South America. SSRN J. 2020. Available online: https://www.ssrn.com/abstract=3686174 (accessed on 21 April 2021). [CrossRef]
- Greaney, A.J.; Loes, A.N.; Crawford, K.H.D.; Starr, T.N.; Malone, K.D.; Chu, H.Y.; Bloom, J.D. Comprehensive mapping of mutations in the SARS-CoV-2 receptor-binding domain that affect recognition by polyclonal human plasma antibodies. Cell Host Microbe. 2021, 29, 463–476.e6. [Google Scholar] [CrossRef]
- Sabino, E.C.; Buss, L.F.; Carvalho, M.P.; Prete, C.A.; Crispim, M.A.; Fraiji, N.A.; Pereira, R.H.; Parag, K.V.; da Silva Peixoto, P.; Kraemer, M.U.; et al. Resurgence of COVID-19 in Manaus, Brazil, despite high seroprevalence. Lancet 2021, 397, 452–455. [Google Scholar] [CrossRef]
- Ringlander, J.; Nilsson, S.; Westin, J.; Lindh, M.; Martner, A.; Hellstrand, K. Low Incidence of Reinfection With Endemic Coronaviruses Diagnosed by Real-Time PCR. J. Infect. Dis. 2020. [Google Scholar] [CrossRef] [PubMed]
- Taboada, B.; Vazquez-Perez, J.A.; Muñoz-Medina, J.E.; Ramos-Cervantes, P.; Escalera-Zamudio, M.; Boukadida, C.; Sanchez-Flores, A.; Isa, P.; Mendieta-Condado, E.; Martínez-Orozco, J.A.; et al. Genomic Analysis of Early SARS-CoV-2 Variants Introduced in Mexico. J. Virol. 2020, 94, e01056-20. [Google Scholar] [CrossRef]
- Goldman, J.; Wang, K.; Röltgen, K.; Nielsen, S.; Roach, J.; Naccache, S.; Yang, F.; Wirz, O.; Yost, K.; Lee, J.; et al. Reinfection with SARS-CoV-2 and Failure of Humoral Immunity: A case report. MedRxiv 2020. [Google Scholar] [CrossRef]
- Kellam, P.; Barclay, W. The dynamics of humoral immune responses following SARS-CoV-2 infection and the potential for reinfection. J. Gen. Virol. 2020, 101, 791–797. [Google Scholar] [CrossRef] [PubMed]
- Bonifácio, L.P.; Pereira, A.P.S.; Balbão, V.D.M.P.; Fonseca, B.A.L.D.; Passos, A.D.C.; Bellissimo-Rodrigues, F. Are SARS-CoV-2 reinfection and Covid-19 recurrence possible? A case report from Brazil. Rev. Soc. Bras. Med. Trop. 2020, 53, e20200619. [Google Scholar] [CrossRef]
- Alizargar, J. Risk of reactivation or reinfection of novel coronavirus (COVID-19). J. Formos. Med. Assoc. 2020, 119, 1123. [Google Scholar] [CrossRef]
- Ibarrondo, F.J.; Fulcher, J.A.; Goodman-Meza, D.; Elliott, J.; Hofmann, C.; Hausner, M.A.; Ferbas, K.G.; Tobin, N.H.; Aldrovandi, G.M.; Yang, O.O. Rapid Decay of Anti–SARS-CoV-2 Antibodies in Persons with Mild Covid-19. N. Engl. J. Med. 2020, 383, 1085–1087. [Google Scholar] [CrossRef]
- Channappanavar, R.; Fett, C.; Zhao, J.; Meyerholz, D.K.; Perlman, S. Virus-Specific Memory CD8 T Cells Provide Substantial Protection from Lethal Severe Acute Respiratory Syndrome Coronavirus Infection. J. Virol. 2014, 88, 11034–11044. [Google Scholar] [CrossRef] [Green Version]
- Orientaciones Provisionales para la Detección de Casos de Reinfección por SARS-CoV-2—OPS/OMS|Organización Panamericana de la Salud [Internet]. Available online: https://www.paho.org/es/documentos/orientaciones-provisionales-para-deteccion-casos-reinfeccion-por-sars-cov-2 (accessed on 8 March 2021).
- Ledford, H. Coronavirus reinfections: Three questions scientists are asking. Nature 2020, 585, 168–169. [Google Scholar] [CrossRef]
- Lafaie, L.; Célarier, T.; Goethals, L.; Pozzetto, B.; Grange, S.; Ojardias, E.; Annweiler, C. Recurrence or Relapse of COVID-19 in Older Patients: A Description of Three Cases. J. Am. Geriatr. Soc. 2020, 68, 2179–2183. [Google Scholar] [CrossRef]
- Arafkas, M.; Khosrawipour, T.; Kocbach, P.; Zielinski, K.; Schubert, J.; Mikolajczyk, A.; Celinska, M.; Khosrawipour, V. Current meta-analysis does not support the possibility of COVID-19 reinfections. J. Med. Virol. 2021, 93, 1599–1604. [Google Scholar] [CrossRef] [PubMed]
- Sun, J.; Xiao, J.; Sun, R.; Tang, X.; Liang, C.; Lin, H.; Zeng, L.; Hu, J.; Yuan, R.; Zhou, P.; et al. Prolonged Persistence of SARS-CoV-2 RNA in Body Fluids. Emerg. Infect. Dis. 2020, 26, 1834–1838. [Google Scholar] [CrossRef] [PubMed]
- Alvarez-Moreno, C.A.; Rodríguez-Morales, A.J. Testing Dilemmas: Post negative, positive SARS-CoV-2 RT-PCR—Is it a reinfection? Travel Med. Infect. Dis. 2020, 35, 101743. [Google Scholar] [CrossRef]
- Malkov, E. Simulation of coronavirus disease 2019 (COVID-19) scenarios with possibility of reinfection. Chaos Solitons Fractals 2020, 139, 110296. [Google Scholar] [CrossRef] [PubMed]
- Duggan, N.M.; Ludy, S.M.; Shannon, B.C.; Reisner, A.T.; Wilcox, S.R. Is novel coronavirus 2019 reinfection possible? Interpreting dynamic SARS-CoV-2 test results. Am. J. Emerg. Med. 2021, 39, e256.e1–e256.e3. [Google Scholar] [CrossRef] [PubMed]
- Roy, S. COVID-19 Reinfection: Myth or Truth? SN Compr. Clin. Med. 2020, 2, 710–713. [Google Scholar] [CrossRef]
- Chaturvedi, R.; Naidu, R.; Sheth, S.; Chakravarthy, K. Efficacy of Serology Testing in Predicting Reinfection in Patients with SARS-CoV-2. Disaster Med. Public Health Prep. 2020, 1–3. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Case 1 | Case 2 | Case 3 | Case 4 | |||||
|---|---|---|---|---|---|---|---|---|
| Age in years | 40 | 49 | 53 | 52 | ||||
| Gender | Female | Female | Male | Male | ||||
| Occupation | Nurse | Nurse | Pharmacy assistant | Internist | ||||
| Comorbidities | Yes | No | No | |||||
| First Infection | Second Infection | First Infection | Second Infection | First Infection | Second Infection | First Infection | Second Infection | |
| Onset of symptoms | 26 April 2020 | 07 September 2020 | 10 May 2020 | 16 September 2020 | 22 May 2020 | 06 September 2020 | 03 June 2020 | 24 August 2020 |
| Symptom remission | 22 May 2020 | 10 October 2020 | 30 May 2020 | 21 September 2020 | 20 June 2020 | 15 October 2020 | 18 June 2020 | 17 November 2020 |
| Time between the onset of the first and second infection | 134 days | 129 days | 107 days | 82 days | ||||
| Time between remission of first infection and onset of second infection | 108 days | 109 days | 78 days | 67 days | ||||
| Symptoms | ||||||||
| Fever | Yes | Yes | Yes | Yes | ||||
| Dry cough | Yes | Yes | Yes | Yes | Yes | Yes | Yes | |
| Headache | Yes | Yes | Yes | Yes | ||||
| Rhinorrhea | Yes | Yes | Yes | |||||
| General malaise | Yes | Yes | Yes | Yes | Yes | |||
| Anosmia | Yes | Yes | Yes | |||||
| Chills | Yes | Yes | ||||||
| Odynophagia | Yes | Yes | Yes | |||||
| Dyspnea | Minimum efforts | Medium efforts | Medium efforts | Medium efforts | Minimum efforts | |||
| Myalgia | Yes | Yes | Yes | Yes | Yes | |||
| Arthralgia | Yes | Yes | Yes | Yes | Yes | |||
| Decrease in oxygen saturation | Yes | Yes | Yes | |||||
| Exanthema | Maculopapular on upper and lower limbs, thorax, face and neck | Diffuse fine maculopapular | ||||||
| Dysgeusia | Yes | Yes | Yes | |||||
| Treatment | Paracetamol, nebulizations with budesonide plus ipratropium bromide, salmetol/fluticasone, salbutamol spray, loratadine. | Paracetamol, Salmeterol/ fluticasone, salbutamol spray, montelukast. | Paracetamol y azithromycin. | Budesonide/ formoterol and paracetamol. | Azithromycin, oseltamivir, paracetamol, prednisone, hydroxychloroquinine. | Azithromycin, ivermectin, paracetamol, benzonatate beads, prednisone, indomethacin, beclomethasone spray. | Lopinavir/ritonavir, dexamethasone, azithromycin. | Tocilizumab, linezolid, piperacillin/ tazobactam, enoxaparin, methylprednisolone, dexmedetomidine. |
| Pneumonia on the second event identified by imaging. | Yes | Yes | ||||||
| Supplemental oxygen requirement | Yes | Yes | Yes | |||||
| Hospital stay | Yes | Yes | ||||||
| Intensive care unit (ICU) stay | Yes | |||||||
| Assisted mechanical ventilation | Yes (11 days) | |||||||
| Clinical course | Exacerbation/Improvement | Discharged/Pulmonary sequela with postinfectious bullae | Improvement | Improvement | Improvement | Improvement | Improvement | Bilateral interstitial pneumonia/Improvement |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Garduño-Orbe, B.; Sánchez-Rebolledo, J.M.; Cortés-Rafael, M.; García-Jiménez, Y.; Perez-Ortiz, M.; Mendiola-Pastrana, I.R.; López-Ortiz, E.; López-Ortiz, G. SARS-CoV-2 Reinfection among Healthcare Workers in Mexico: Case Report and Literature Review. Medicina 2021, 57, 442. https://doi.org/10.3390/medicina57050442
Garduño-Orbe B, Sánchez-Rebolledo JM, Cortés-Rafael M, García-Jiménez Y, Perez-Ortiz M, Mendiola-Pastrana IR, López-Ortiz E, López-Ortiz G. SARS-CoV-2 Reinfection among Healthcare Workers in Mexico: Case Report and Literature Review. Medicina. 2021; 57(5):442. https://doi.org/10.3390/medicina57050442
Chicago/Turabian StyleGarduño-Orbe, Brenda, Juan Manuel Sánchez-Rebolledo, Mustafá Cortés-Rafael, Yuliana García-Jiménez, Marcelina Perez-Ortiz, Indira Rocío Mendiola-Pastrana, Eduardo López-Ortiz, and Geovani López-Ortiz. 2021. "SARS-CoV-2 Reinfection among Healthcare Workers in Mexico: Case Report and Literature Review" Medicina 57, no. 5: 442. https://doi.org/10.3390/medicina57050442