
Lessons Learned from Developing Digital Teaching Modules for Medical Student Education in Neurosurgery during the COVID-19 Pandemic



Abstract
:1. Introduction
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
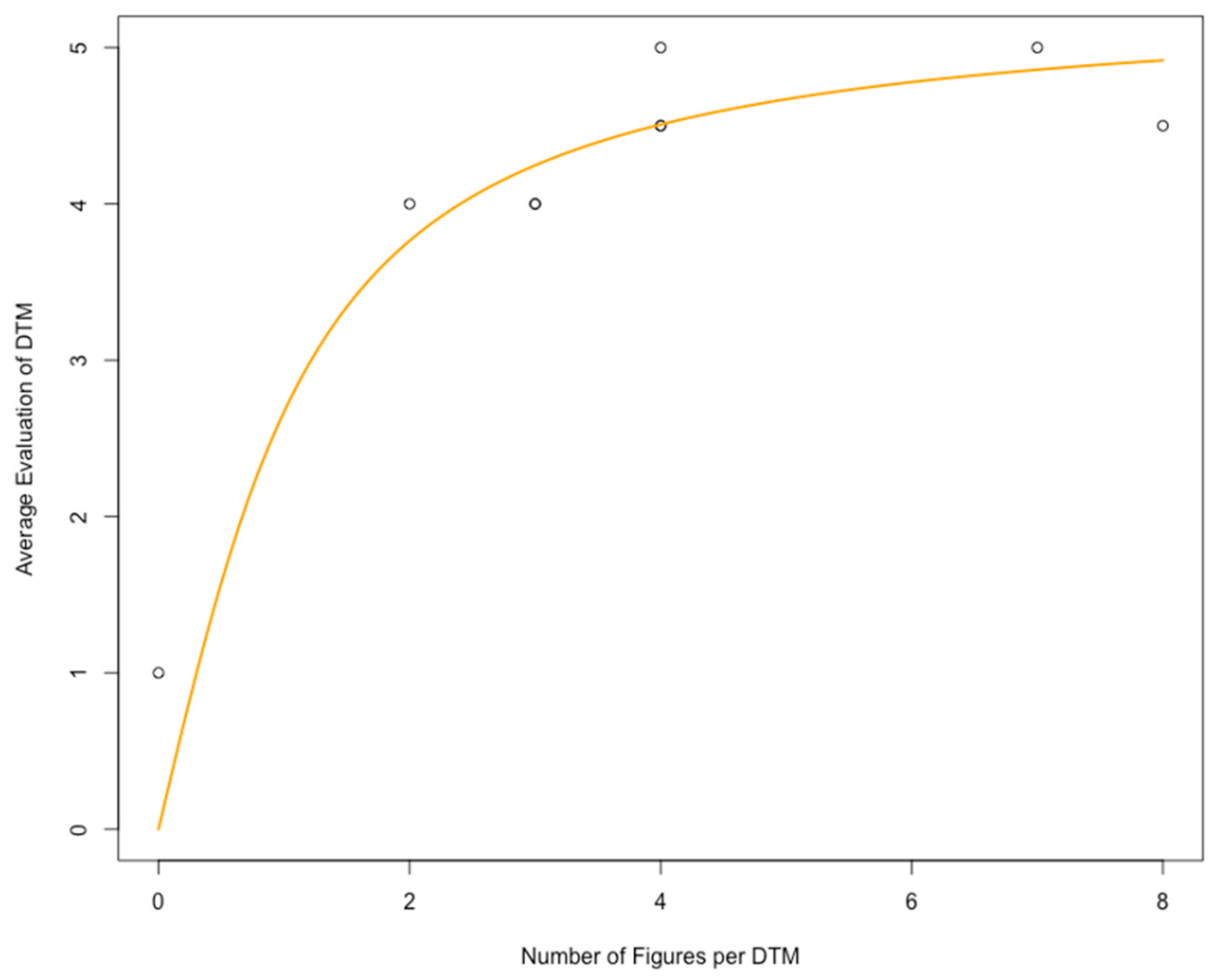
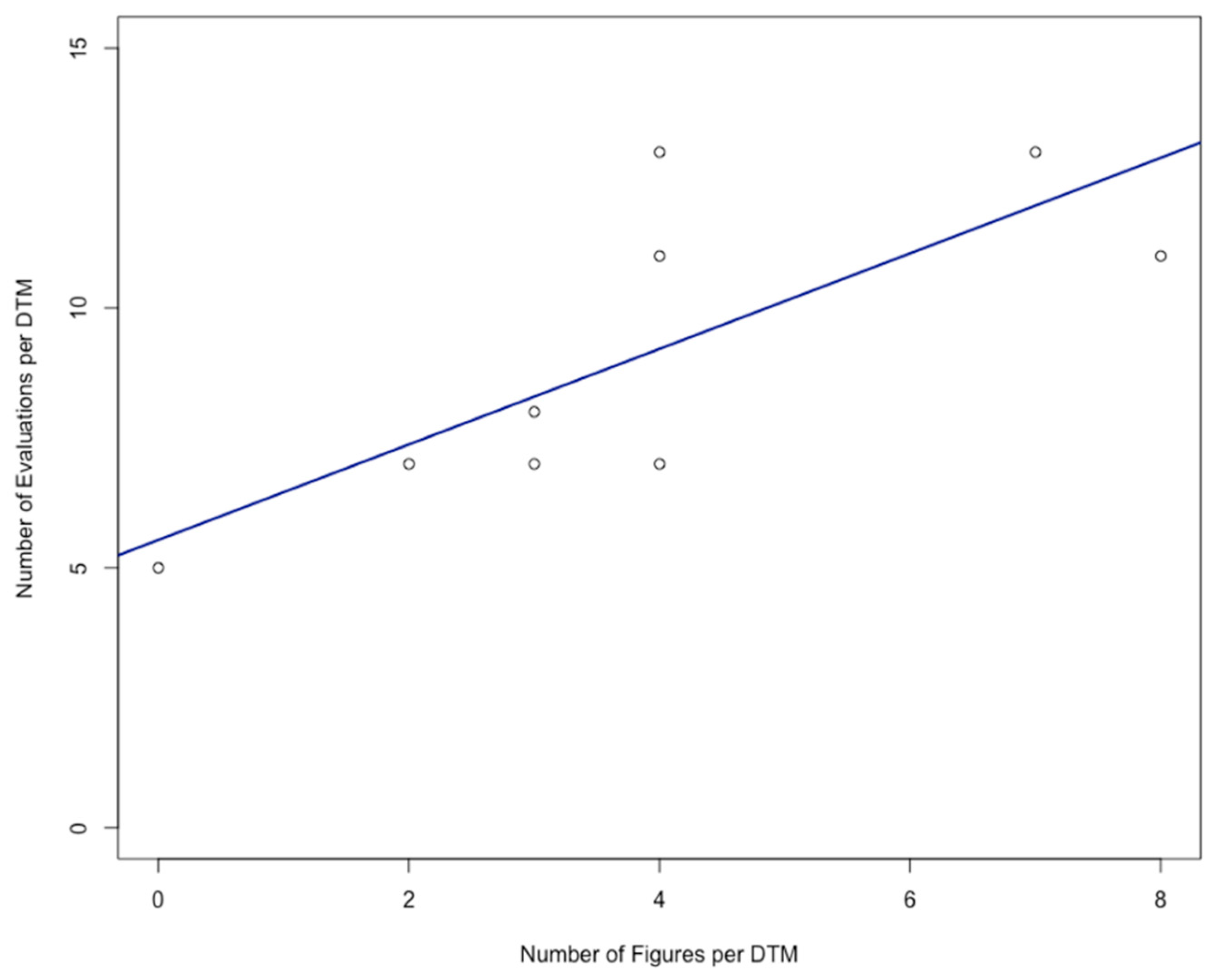
- (Interactive) figures and illustrative cases apparently foster students’ engagement with the content of the DTM; and
- To obtain valuable feedback from students, it is advised to offer low-threshold communication channels. These include a scoring option for each DTM, open survey questions, and provision of the e-mail address of a correspondent academic staff member.
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Hu, B.; Guao, H.; Zhou, P.; Shi, Z.L. Characteristics of SARS-CoV-2 and COVID-19. Nat. Rev. Microbiol. 2021, 19, 141–154. [Google Scholar] [CrossRef]
- Sorci, G.; Faivre, B.; Morand, S. Explaining among-country variation in COVID-19 case fatality rate. Sci. Rep. 2020, 10, 18909. [Google Scholar] [CrossRef]
- Meyerowitz-Katz, G.; Merone, L. A systematic review and meta-analysis of published research data on COVID-19 infection fatality rates. Int. J. Infect. Dis. 2020, 101, 138–148. [Google Scholar] [CrossRef]
- Haug, N.; Geyrhofer, L.; Londei, A.; Dervic, E.; Desvars-Larrive, A.; Loreto, V.; Pinior, B.; Thurner, S.; Klimek, P. Ranking the effectiveness of worldwide COVID-19 government interventions. Nat. Hum. Behav. 2020, 4, 1303–1312. [Google Scholar] [CrossRef] [PubMed]
- Pozo, J.I.; Pérez Echeverria, M.P.; Cabellos, B.; Sánchez, D.L. Teaching and Learning in Times of COVID-19: Uses of Digital Technologies During School Lockdown. Front. Psychol. 2021, 12, 656776. [Google Scholar] [CrossRef]
- Motte-Signoret, E.; Labbé, A.; Benoist, G.; Linglart, A.; Gajdos, V.; Lapillonne, A. Perception of medical education by learners and teachers during the COVID-19 pandemic: A cross-sectional survey of online-teaching. Med. Educ. Online 2021, 26, 1919042. [Google Scholar] [CrossRef]
- Asgari, S.; Trajkovic, J.; Rahmani, M.; Zhang, W.; Lo, R.C.; Sciortino, A. An observational study of engineering online education during the COVID-19 pandemic. PLoS ONE 2021, 16, e0250041. [Google Scholar] [CrossRef] [PubMed]
- ILIAS. Available online: https://www.ilias.de (accessed on 27 June 2021).
- k-MED. Available online: https://kmed.uni-giessen.de (accessed on 27 June 2021).
- Besprechung der Bundeskanzlerin mit den Regierungschefinnen und Regierungschefs der Länder am 12. März 2020. Available online: https://www.bundesregierung.de/breg-de/themen/coronavirus/beschluss-zu-corona-1730292 (accessed on 27 June 2021).
- Alsoufi, A.; Alsuyihili, A.; Msherghi, A.; Elhadi, A.; Atiyah, H.; Ashini, A.; Ashwieb, A.; Ghula, M.; Ben Hasan, H.; Abudabuos, S.; et al. Impact of the COVID-19 pandemic on medical education: Medical students’ knowledge, attitudes, and practices regarding electronic learning. PLoS ONE 2020, 15, e0242905. [Google Scholar] [CrossRef]
- Atreya, A.; Acharya, J. Distant virtual medical education during COVID-19: Half a loaf of bread. Clin. Teach. 2020, 17, 418–419. [Google Scholar] [CrossRef]
- Jones, N.; Sanchez Tapia, I.; Baird, S.; Guglielmi, S.; Oakley, E.; Yadete, W.A.; Sultan, M.; Pincock, K. Intersecting barriers to adolescents’ educational access during COVID-19: Exploring the role of gender, disability and poverty. Int. J. Educ. Dev. 2021, 85, 102428. [Google Scholar] [CrossRef]
- Maity, S.; Sahu, T.N.; Sen, N. Panoramic view of digital education in COVID-19: A new explored avenue. Rev. Educ. 2021, 9, 405–423. [Google Scholar] [CrossRef]
- Chen, T.; Peng, L.; Yin, X.; Rong, J.; Yang, J.; Cong, G. Analysis of user satisfaction with online education platforms in China during the COVID-19 pandemic. Healthcare 2020, 8, 200. [Google Scholar] [CrossRef] [PubMed]
- Ramos, J.L.; Cattaneo, A.A.P.; de Jong, F.P.C.M.; Espadeiro, R.G. Pedagogical models for the facilitation of teacher professional development via video-supported collaborative learning. A review of the state of the art. J. Res. Technol. Educ. 2021. [Google Scholar] [CrossRef]
- Katz, N.; Nandi, N. Social media and medical education in the context of the COVID-19 pandemic: Scoping review. JMIR Med. Educ. 2021, 7, e25892. [Google Scholar] [CrossRef]
- Corell-Almuzara, A.; Lopez-Belmonte, J.; Marin-Marin, J.-A.; Moreno-Guerrero, A.-J. COVID-19 in the field of education: State of the art. Sustainability 2021, 13, 5452. [Google Scholar] [CrossRef]
- The R Project. Available online: https://www.r-project.org (accessed on 30 June 2021).
- Keifenheim, K.E.; Teufel, M.; Ip, J.; Speiser, N.; Leehr, E.J.; Zipfel, S.; Herrmann-Werner, A. Teaching history taking to medical students: A systematic review. BMC Med. Educ. 2015, 15, 159. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lerchenfeldt, S.; Mi, M.; Eng, M. The utilization of peer feedback during collaborative learning in undergraduate medical education: A systematic review. BMC Med. Educ. 2019, 19, 321. [Google Scholar] [CrossRef] [Green Version]
- O’Doherty, D.; Dromey, M.; Lougheed, J.; Hannigan, A.; Last, J.; McGrath, D. Barriers and solutions to online learning in medical education—An integrative review. BMC Med. Educ. 2018, 18, 130. [Google Scholar] [CrossRef] [Green Version]
- Singal, A.; Bansal, A.; Chaudhary, P.; Singh, H.; Patra, A. Anatomy education of medical and dental students during COVID-19 pandemic: A reality check. Surg. Radiol. Anat. 2021, 43, 515–521. [Google Scholar] [CrossRef]
- Lau, E.J.S.; Aslam, A.; Arshad, Z. How have digital resources been utilised in times of COVID-19? Opinions of medical students based in the United Kingdom. Can. Med. Educ. J. 2021, 12, e115–e117. [Google Scholar] [CrossRef]
- Capsule. Available online: https://www.capsule.ac.uk (accessed on 27 June 2021).
- Eurorad. Available online: https://www.eurorad.org (accessed on 27 June 2021).
- Kyaw, B.M.; Posadzki, P.; Paddock, S.; Car, J.; Campbell, J.; Car, L.T. Effectiveness of Digital Education on Communication Skills Among Medical Students: Systematic Review and Meta-Analysis by the Digital Health Education Collaboration. J. Med. Internet Res. 2019, 21, e12967. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Turkdogan, S.; Schnitman, G.; Wang, T.; Gotlieb, R.; How, J.; Gotlieb, W.H. Development of a Digital Patient Education Tool for Patients with Cancer During the COVID-19 Pandemic. JMIR Cancer 2021, 7, e23637. [Google Scholar] [CrossRef] [PubMed]
- Pubmed Search for the Term “Digital Learning Management System”. Available online: https://pubmed.ncbi.nlm.nih.gov/?term=digital+learning+management+system (accessed on 27 June 2021).
- Darras, K.E.; Spouge, R.J.; de Bruin, A.B.H.; Sedlic, A.; Hague, C.; Forster, B.B. Undergraduate Radiology Education During the COVID-19 Pandemic: A Review of Teaching and Learning Strategies. Can. Assoc. Radiol. J. 2021, 72, 194–200. [Google Scholar] [CrossRef]
- Heinzmann, A.; Bode, S.; Forster, J.; Berger, J. Interactive, case-based seminars in the digitized pediatrics block internship from the students’ perspective. GMS J. Med. Educ. 2021, 38, Doc24. [Google Scholar] [CrossRef]
- Langewitz, W.; Pleines Dantas Seixas, U.; Hunziker, S.; Becker, C.; Fischer, M.R.; Benz, A.; Otto, B. Doctor-patient communication during the Corona crisis—Web-based interactions and structured feedback from standardized patients at the university of Basel and the LMU Munich. GMS J. Med. Educ. 2021, 38, Doc81. [Google Scholar] [CrossRef] [PubMed]
- Smith, E.; Boscak, A. A virtual emergency: Learning lessons from remote medical student education during the COVID-19 pandemic. Emerg. Radiol. 2021, 28, 445–452. [Google Scholar] [CrossRef]
- Vielsmeier, V.; Auerswald, S.; Marienhagen, J.; Keil, S.; Müller, N. Digital teaching with interactive case presentations of ENT diseases—Discussion of utilization and motivation of students. GMS J. Med. Educ. 2020, 37, Doc100. [Google Scholar] [CrossRef]
- He, M.; Tang, X.-Q.; Zhang, H.-N.; Luo, Y.-Y.; Tang, Z.-C.; Gao, S.-G. Remote clinical training practice in the neurology internship during the COVID-19 pandemic. Med. Educ. Online 2021, 26, 1899642. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Topic | Average Evaluation | Number of Evaluations | Number of Accesses | Number of Figures | Number of Inter-Active Figures * | Number of Questions | Number of Cases | Number of Linked Papers |
|---|---|---|---|---|---|---|---|---|
| Aneurysmal Subarachnoid Hemorrhage | 4.5 | 13 | 90 | 4 | 0 | 2 | 1 | 1 |
| Impairment of Consciousness | 4.5 | 11 | 162 | 4 | 0 | 5 | 1 | 2 |
| Elective Neurosurgery During the COVID-19 Pandemic | 4.0 | 7 | 77 | 3 | 0 | 2 | 1 | 1 |
| Fluorescence-Guided Glioma Surgery | 1.0 | 5 | 85 | 0 ** | 0 | 2 | 1 | 3 |
| Intracranial Pressure | 5.0 | 13 | 98 | 7 | 0 | 6 | 1 | 0 |
| Brain Death | 4.0 | 7 | 126 | 2 | 0 | 4 | 0 | 2 |
| Hydrocephalus | 4.5 | 11 | 134 | 8 | 3 | 1 | 1 | 0 |
| Lumbar Disc Hernia | 4.0 | 8 | 109 | 3 | 0 | 4 | 2 | 0 |
| Cervical Disc Hernia | 5.0 | 7 | 91 | 4 | 1 | 2 | 1 | 0 |
| Module Popularity Measure | Number of Figures per Module | Number of Interactive Figures per Module | Number of Cases per Module | Number of Questions per Module | Number of Linked Papers per Module |
|---|---|---|---|---|---|
| Number of accesses per module | 0.4 (0.286) | 0.25 (0.5147) | −0.09 (0.8153) | 0.34 (0.3692) | −0.13 (0.7354) |
| Number of evaluations per module | 0.78 (0.0137) * | −0.01 (0.9762) | 0.19 (0.6294) | 0.29 (0.4465) | −0.43 (0.2449) |
| Average evaluation per module | 0.85 (0.0037) * | 0.45 (0.2232) | 0 (1) | 0.17 (0.6653) | −0.62 (0.0743) |
| Feedback Channel | Threshold | Feedback Quantity | Feedback Quality |
|---|---|---|---|
| Scoring bar | (+) | (+++) | (+++) |
| Survey, closed questions | (+++) | (++) | (+) |
| Survey, open questions | (++) | (+) | (++) |
| Individual response by e-mail | (++) | (+) | (++) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rupa, R.; Pojskic, M.; Nimsky, C.; Voellger, B. Lessons Learned from Developing Digital Teaching Modules for Medical Student Education in Neurosurgery during the COVID-19 Pandemic. Healthcare 2021, 9, 1141. https://doi.org/10.3390/healthcare9091141
Rupa R, Pojskic M, Nimsky C, Voellger B. Lessons Learned from Developing Digital Teaching Modules for Medical Student Education in Neurosurgery during the COVID-19 Pandemic. Healthcare. 2021; 9(9):1141. https://doi.org/10.3390/healthcare9091141
Chicago/Turabian StyleRupa, Rosita, Mirza Pojskic, Christopher Nimsky, and Benjamin Voellger. 2021. "Lessons Learned from Developing Digital Teaching Modules for Medical Student Education in Neurosurgery during the COVID-19 Pandemic" Healthcare 9, no. 9: 1141. https://doi.org/10.3390/healthcare9091141