
Abstract
Introduction
In the acute phase of COVID-19, elevated d-dimer levels indicate a hypercoagulable state putting the patients at increased risk for venous thromboembolic disease (VTE). It is unclear, if prior COVID-19 disease increases the risk for VTE after total joint arthroplasty (TJA) and if d-dimer levels can be used to identify patients at risk.
Materials and methods
d-Dimer levels of 313 consecutive SARS-CoV-2 IgG-positive and 2,053 -negative patients undergoing TJA between 05/20 and 12/20 were evaluated. d-Dimer levels were divided into three groups: < 200 ng/ml, 200–400 ng/ml, and > 400 ng/ml d-dimer units (DDU). 277 SARS-CoV-2 IgG-positive patients underwent a Doppler ultrasound to rule out deep-vein thrombosis (DVT) 4–6 weeks after TJA.
Results
d-Dimer levels did not differ significantly between SARS-CoV-2 IgG-positive and -negative patients (p value 0.53). Among SARS-CoV-2 IgG-negative patients, 1687 (82.17%) had d-dimer levels < 200 ng/ml, 256 (12.47%) between 200 and 400 ng/ml, and 110 (5.36%) > 400 ng/ml. Of the SARS-CoV-2 IgG-positive patients, 257 (83.71%) had d-dimer levels < 200 ng/ml, 34 (11.07%) between 200 and 400 ng/ml, and 16 (5.21%) > 400 ng/ml. A postoperative DVT was detected in nine patients (2.9%) in the SARS-CoV-2 IgG-positive group and a PE in one patient (0.3%). 7/229 patients with < 200 ng/ml (3.1%), 1/28 patients (3.6%) with 200–400 ng/ml and 1/9 patients (11.1%) with d-dimer levels > 400 ng/ml had a DVT or PE (p = 0.43).
Conclusions
The findings of this investigation suggest there is no difference in d-dimer levels between SARS-CoV-2 IgG-positive and -negative patients undergoing TJA. Although there is a trend for increased VTE rates with increased d-dimer levels, routine d-dimer testing is not recommended based on the current data. SARS-CoV-2 IgG-positive patients have a low risk of VTE in the current study.
Similar content being viewed by others


Introduction
Coronavirus Disease 2019 (COVID-19) has placed an immense strain on health care systems of the world, requiring postponement of elective orthopedic procedures during the pandemic. COVID-19 is caused by the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2). Besides pulmonary complications, patients with COVID-19 are at increased risk for thromboembolic events both in the arterial and the venous systems [6, 20, 21]. The induced hypercoagulable state is marked by platelet activation, vascular endothelial dysfunction and excessive inflammation [7, 12, 13, 15], though bleeding and thrombocytopenia have also been described [8, 9].
d-Dimer levels have been shown to be elevated during acute COVID-19 infection [5, 22, 30]. COVID-associated coagulopathy with evidence of microthrombi and macrothrombi in the venous and arterial systems can be diagnosed based on d-dimer elevations [14]. Elevated d-dimers are a predictor for mortality in individuals hospitalized for COVID-19 [4, 5, 17] and a cutoff of > 1070 ng/ml DDU (2.14 mg/L FEU) predicted in-hospital mortality with a sensitivity of 88.2% and specificity of 71.3% [30]. Comparing d-dimer levels in patients with active SARS-CoV-2 infection to healthy controls has shown substantially higher d-dimer values in SARS-CoV-2-positive patients [11].
In a small retrospective case series of four patients undergoing elective surgery during active COVID-19 infection, the perioperative course was complicated and resulted in a high fatality rate (50%) [1]. The mortality rate in active COVID-19 fracture patients in one recent systematic review was 36.6%, mostly due to respiratory failure [16].
The current study evaluates whether patients with a history of previous COVID-19 (SARS-CoV-2 IgG positive) present with elevated d-dimer levels, and whether they are at increased risk for symptomatic and/or asymptomatic lower extremity DVT following total knee and hip arthroplasty.
Patients and methods
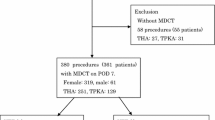
This study evaluates a consecutive series of patients undergoing elective TJA at the authors’ institution between May 2020 and December 2020. The study was approved by the Institutional Review Board. d-Dimer levels of a consecutive series of 313 SARS-CoV-2 IgG-positive patients undergoing joint arthroplasty were prospectively collected and retrospectively reviewed and compared to a series of 2053 SARS-CoV-2 IgG-negative patients undergoing TJA. The polymerase chain reaction (PCR) test for active COVID-19 infection was negative in all patients at the time of surgery and SARS-CoV-2 IgG-positive patients only had surgery, if they recovered from COVID-19 and subsequently tested negative on PCR test prior to their surgery.
d-Dimer levels as well as SARS-CoV-2 IgG antibodies were drawn during medical clearance routinely within 1–21 days prior to surgery.
Between May and July 2020, all patients underwent d-dimer testing, after July 2020, only SARS-CoV-2 IgG-positive patients were tested on the day of their surgery in the holding area before the procedure.
Inclusion criteria were patients undergoing elective TJA including total knee arthroplasty (TKA), total hip arthroplasty (THA), unicondylar knee arthroplasty (UKA) and hip resurfacing. Exclusion criteria were patients with periprosthetic infection, revision or trauma cases.
d-Dimer levels were categorized semi-quantitatively as by the institution’s normal range: normal values were < 200 ng/ml d-dimer units (DDU), elevated d-dimer levels were classified as data within the ranges from 200 to 400 ng/ml, and over 400 ng/ml DDU.
The SARS-CoV-2 IgG-positive group consisted of 173 female and 140 male patients, the SARS-CoV-2 IgG-negative group of 1203 female and 850 male patients. Patients in the SARS-CoV-2 IgG-positive group were younger and had a greater BMI than their SARS-CoV-2 IgG-negative counterparts (Table 1).
In the SARS-CoV-2 IgG-positive group, 145 patients underwent primary THA, 139 patients primary TKA, 13 patients hip resurfacing, and 9 patients UKA. In addition, five patients had bilateral TKAs and two patients bilateral THAs.
In the SARS-CoV-2 IgG-negative group, 1071 patients underwent primary THA, 802 patients primary TKA, 78 patients hip resurfacing, 56 patients UKA, 30 patients bilateral TKAs, 14 patients bilateral THAs, 1 patient bilateral resurfacings, and 1 patient bilateral UKAs.
A bilateral lower extremity Doppler ultrasound 6 weeks postoperatively to rule out asymptomatic DVT was performed in 277 patients as part of hospital protocols. There was no difference in SARS-CoV-2 IgG-positive patients receiving a Doppler ultrasound to those who did not have a Doppler ultrasound. Patients, who missed the ultrasound missed it for organizational reasons, like follow-up at a location without ultrasound access, timed constrained limited ability to do an ultrasound or patients did not want another test at the hospital.
Postoperative DVT prophylaxis was indicated based on patient’s comorbidities. Patients with atrial fibrillation, history of DVT or pulmonary embolism (PE) in the past received either Warfarin, Apixaban or Rivaroxaban, as per the surgeon’s preference or established treatment. Standard DVT prophylaxis at the senior author’s institution is Aspirin (ASA) 325 mg BID.
Statistical analysis
Variables were assessed for normalcy; comparisons between and within cohorts were made using Wilcoxon rank-sum tests and Wilcoxon signed-rank tests, respectively. Categorical variables were assessed using Chi-square or Fisher exact tests. For regression modeling, continuous and ordinal variables were explored using Pearson and Spearman’s correlation coefficient, respectively. Measurements which differed between the primary and comparative cohorts, and variables correlated/associated with those measurements, were included in the logistic regression modeling. A power-analysis was conducted for d-dimer levels. There is 85% power to detect a twofold increase in d-dimer proportion above 400. This is based on a cohort estimate of 5% above 400 ng/ml and 10% in the SARS-CoV-2 IgG-positive group.
All statistical tests were two sided with a significance level of 0.05. Analyses were conducted using SAS software version 9.4 (SAS Institute Inc., Carey, NC).
Results
d-Dimer levels did not differ significantly between SARS-CoV-2 IgG-negative patients and SARS-CoV-2 IgG-positive patients (p = 0.5261). d-Dimer levels are reported in Table 2.
For the 277 SARS-CoV-2 IgG-positive patients who had a postoperative Doppler ultrasound performed at 4–6 weeks, the DVT prophylaxis and d-dimer levels are reported in Table 3.
Nine patients had a DVT on ultrasound (3.2%). There were two (0.6%) symptomatic DVTs in the SARS CoV-2 IgG-positive group and seven (2.5%) asymptomatic DVTs, and one PE (0.3%). Seven of 214 patients (3.3%) receiving ASA for DVT prophylaxis, 3 of the 8 patients (37.5%) receiving Warfarin had a DVT or PE, respectively; no DVT or PE was detected in patients treated with Apixaban or Rivaroxaban (p ≤ 0.0001). The occurrence of DVT or PE in accordance with d-dimer levels was 7 of 229 (3.1%) patients with d-dimer levels < 200 ng/ml, 1 of 28 patients (3.6%) with d-dimer levels 200–400 ng/mL, and 1 of 9 patients (11.1%) with d-dimer levels > 400 ng/mL, respectively (p = 0.43). One patient, who developed a DVT, did not have a blood draw for d-dimer levels.
Patients, who developed a DVT/PE, are shown in Table 4.
There was no difference in age between patients with d-dimer levels of 200–400 ng/mL and > 400 ng/mL (p = 0.40). At 64.4 ± 10.2 years, patients with d-dimer levels < 200 ng/ml were significantly younger than those with higher d-dimer levels (p ≤ 0.0001). There was no difference in BMI for different d-dimers levels (p = 0.40). The association between d-dimer levels and SARS-CoV-2 IgG status, when controlling for age at time of surgery and BMI, was not significant (p = 0.74). However, in the same model, age was significantly associated with d-dimer levels (p ≤ 0.0001) with an odds ratio of 0.97 (95% confidence interval (CI) 0.959, 0.980). BMI showed a borderline significant association with d-dimer levels (p = 0.047) with an odds ratio of 0.982 (95% CI 0.964, 1.000).
Discussion
This prospective study of 2366 consecutive patients undergoing elective TJA reports that (1) d-dimer levels at the time of surgery are not significantly different between SARS-CoV-2 IgG-positive and SARS-CoV-2 IgG-negative patients and (2) there is a postoperative symptomatic PE rate of 0.3% among patients that are SARS-CoV-2 IgG positive and the 6 weeks asymptomatic VTE rate is 2.5%.
The postoperative symptomatic DVT rate among patients with SARS-CoV-2 IgG positivity is comparable to the postoperative DVT rate for patients in the TJA literature. In a study by Warren et al., the incidence for symptomatic DVT in a database including 363,530 patients after THA was 0.4% and 1.4% after TKA [28]. In a meta-analysis, 6% of patients undergoing TKA and THA using Rivaroxaban for DVT prophylaxis presented with a DVT diagnosed by venography [19]. In a study by Westrich et al., ascending venography detected a postoperative DVT in 33% of patients undergoing TKA [29]. Parvizi et al. analyzed 4651 primary total joint arthroplasty cases and found a symptomatic DVT rate of 0.1% when using 81 mg ASA and of 0.3% when using 325 mg ASA [24]. In a study by Bala et al., Factor Xa inhibitors (1.7%) and aspirin (1.7%) had the lowest incidence of symptomatic DVT at 90 days, followed by enoxaparin (2.6%), and warfarin (3.7%) [3]. The later study showed a higher rate of symptomatic postoperative DVT compared to the current group of SARS-CoV-2 IgG-positive patients.
The results of our study indicate that preoperative d-dimer levels are similar among SARS-CoV-2 IgG-positive and -negative TJA patients. This is an important finding which, in conjunction with the reported low DVT rate among SARS-CoV-2 IgG-positive patients, suggests patients with history of COVID-19 infection do not continue at a hypercoagulability state throughout the duration of antibody positivity. Given these patients may no longer be in a hypercoagulable state, the study suggests there does not appear an elevated risk for DVT in TJA patients.
d-Dimer elevation in SARS-CoV-2 IgG-negative patients can be due to various causes: infection [18], malignancy [26], trauma [25, 27], pregnancy [10] age [23] or recent surgery [2]. Since a d-dimer elevation is very non-specific, routine DVT prophylaxis does not seem necessary for SARS-CoV-2 IgG-negative patients not undergoing surgery [26]. There is a lack of recommendations in the literature as to whether DVT prophylaxis should be increased in patients with elevated d-dimer levels undergoing surgery.
The current study has the following limitations. (1) No patient died during the follow-up, however, other complications were not evaluated in this study; (2) we are unpowered to detect differences in the rate of PE; (3) patients with elevated d-dimer levels might have been placed on more potent DVT prophylaxis, than patients with d-dimer levels < 200 ng/ml DDU; (4) the severity of the initial COVID-19 infection was not evaluated for the SARS-CoV-2 IgG-positive patients. A more severe initial course with hospitalization might increase the risk for VTE in this group of patients; (5) the current study focuses on an early period following the initial outbreak in New York (NY, USA), suggesting a less than 6-month interval between COVID-19 infection and TJA surgery. The current study does not report data on the time interval and its impact on d-dimer levels.
Conclusion
The current study did not observe a difference in d-dimer levels between SARS-CoV-2 IgG-negative and SARS-CoV-2 IgG-positive patients undergoing TJA and does not support routine d-dimer testing prior to elective TJA. Within a 6-week follow-up, the rate of symptomatic DVT in SARS-CoV-2 IgG-positive patients was 0.6% compared to 6% in SARS-CoV-2 IgG-negative patients in the literature [19, 28]. The asymptomatic DVT rate of 2.5% is within the range of data published in the literature.
References
Aminian A, Safari S, Razeghian-Jahromi A, Ghorbani M, Delaney CP (2020) COVID-19 outbreak and surgical practice: unexpected fatality in perioperative period. Ann Surg 272(1):e27–e29
An TJ, Engstrom SM, Oelsner WK, Benvenuti MA, Polkowski GG, Schoenecker JG (2016) Elevated d-dimer is not predictive of symptomatic deep venous thrombosis after total joint arthroplasty. J Arthroplasty 31(10):2269–2272
Bala A, Murasko MJ, Burk DR et al (2020) Venous thromboprophylaxis after total hip arthroplasty: aspirin, warfarin, enoxaparin, or factor Xa inhibitors? Hip Int 30(5):564–571
Cheng A, Hu L, Wang Y et al (2020) Diagnostic performance of initial blood urea nitrogen combined with D-dimer levels for predicting in-hospital mortality in COVID-19 patients. Int J Antimicrob Agents 56:106110
Cho ES, McClelland PH, Cheng O et al (2020) Utility of d-dimer for diagnosis of deep vein thrombosis in coronavirus disease-19 infection. J Vasc Surg Venous Lymphat Disord 9:47–53
de Roquetaillade C, Chousterman BG, Tomasoni D et al (2020) Unusual arterial thrombotic events in Covid-19 patients. Int J Cardiol 323:281–284
Del Turco S, Vianello A, Ragusa R, Caselli C, Basta G (2020) COVID-19 and cardiovascular consequences: is the endothelial dysfunction the hardest challenge? Thromb Res 196:143–151
Görlinger K, Dirkmann D, Gandhi A, Simioni P (2020) COVID-19 associated coagulopathy and inflammatory response: what do we know already and what are the knowledge gaps? Anesth Analg 131:1324–1333
Grobler C, Maphumulo SC, Grobbelaar LM et al (2020) Covid-19: the rollercoaster of fibrin(Ogen), D-dimer, von willebrand factor, P-selectin and their interactions with endothelial cells, platelets and erythrocytes. Int J Mol Sci 21(14):5168
Gutiérrez García I, Pérez Cañadas P, Martínez Uriarte J, García Izquierdo O, Angeles Jódar Pérez M, de Guadiana G, Romualdo L (2018) D-dimer during pregnancy: establishing trimester-specific reference intervals. Scand J Clin Lab Invest 78(6):439–442
Han H, Yang L, Liu R et al (2020) Prominent changes in blood coagulation of patients with SARS-CoV-2 infection. Clin Chem Lab Med 58(7):1116–1120
Hottz ED, Azevedo-Quintanilha IG, Palhinha L et al (2020) Platelet activation and platelet-monocyte aggregate formation trigger tissue factor expression in patients with severe COVID-19. Blood 136(11):1330–1341
Iba T, Levy JH, Connors JM, Warkentin TE, Thachil J, Levi M (2020) The unique characteristics of COVID-19 coagulopathy. Crit Care 24(1):360
Jayarangaiah A, Kariyanna PT, Chen X, Jayarangaiah A, Kumar A (2020) COVID-19-associated coagulopathy: an exacerbated immunothrombosis response. Clin Appl Thromb Hemost 26:1076029620943293
Klok FA, Kruip M, van der Meer NJM et al (2020) Incidence of thrombotic complications in critically ill ICU patients with COVID-19. Thromb Res 191:145–147
Kumar Jain V, Lal H, Kumar Patralekh M, Vaishya R (2020) Fracture management during COVID-19 pandemic: a systematic review. J Clin Orthop Trauma 11(Suppl 4):S431-s441
Laguna-Goya R, Utrero-Rico A, Talayero P et al (2020) IL-6-based mortality risk model for hospitalized patients with COVID-19. J Allergy Clin Immunol 146:799-807.e9
Lippi G, Bonfanti L, Saccenti C, Cervellin G (2014) Causes of elevated D-dimer in patients admitted to a large urban emergency department. Eur J Intern Med 25(1):45–48
Liu J, Zhao J, Yan Y, Su J (2019) Effectiveness and safety of rivaroxaban for the prevention of thrombosis following total hip or knee replacement: a systematic review and meta-analysis. Medicine (Baltimore) 98(9):e14539
Lodigiani C, Iapichino G, Carenzo L et al (2020) Venous and arterial thromboembolic complications in COVID-19 patients admitted to an academic hospital in Milan, Italy. Thromb Res 191:9–14
Manolis AS, Manolis TA, Manolis AA, Papatheou D, Melita H (2021) COVID-19 infection: viral macro- and micro-vascular coagulopathy and thromboembolism/prophylactic and therapeutic management. J Cardiovasc Pharmacol Ther 26(1):12–24
Martín-Rojas RM, Pérez-Rus G, Delgado-Pinos VE et al (2020) COVID-19 coagulopathy: an in-depth analysis of the coagulation system. Eur J Haematol 105:741–750
Olson JD (2015) D-dimer: an overview of hemostasis and fibrinolysis, assays, and clinical applications. Adv Clin Chem 69:1–46
Parvizi J, Huang R, Restrepo C et al (2017) Low-dose aspirin is effective chemoprophylaxis against clinically important venous thromboembolism following total joint arthroplasty: a preliminary analysis. J Bone Jt Surg Am 99(2):91–98
Rizoli S, Nascimento B Jr, Key N et al (2011) Disseminated intravascular coagulopathy in the first 24 hours after trauma: the association between ISTH score and anatomopathologic evidence. J Trauma 71(5 Suppl 1):S441-447
Schutte T, Thijs A, Smulders YM (2016) Never ignore extremely elevated D-dimer levels: they are specific for serious illness. Neth J Med 74(10):443–448
Verni CC, Davila A, Sims CA, Diamond SL (2020) D-dimer and fibrin degradation products impair platelet signaling: plasma D-dimer is a predictor and mediator of platelet dysfunction during trauma. J Appl Lab Med 5:1253–1264
Warren JA, Sundaram K, Anis HK, Kamath AF, Higuera CA, Piuzzi NS (2020) Have venous thromboembolism rates decreased in total hip and knee arthroplasty? J Arthroplasty 35(1):259–264
Westrich GH, Allen ML, Tarantino SJ et al (1998) Ultrasound screening for deep venous thrombosis after total knee arthroplasty. 2-year reassessment. Clin Orthop Relat Res 356:125–133
Yao Y, Cao J, Wang Q et al (2020) D-dimer as a biomarker for disease severity and mortality in COVID-19 patients: a case control study. J Intensive Care 8:49
Acknowledgements
The authors thank Rachelle Hornick, MPH, for her help with the statistics and Michael Alexiades MD, Michael Ast MD, Mathias Bostrom MD, Robert Buly MD, Alberto Carli MD, Michael Cross MD, Fred Cushner MD, Mark Figgie MD, Steven Haas MD, Allen Inglis MD, Seth Jerabek MD, David Mayman MD, Douglas Padgett MD, Michael Parks MD, Jose Rodriguez MD, Eduardo Salvati MD, Peter Sculco MD, Thomas Sculco MD, Edwin Su MD, Jonathan Vigdorchik MD, and Russell Windsor MD from the ARJR service for contributing patients to the current study.
Funding
No funding was received to assist with the preparation of this manuscript.
Author information
Authors and Affiliations
Contributions
All the authors contributed to the study conception and design. Material preparation, data collection and analysis were performed by AJ-W. The first draft of the manuscript was written by AJ-W and all the authors commented on previous versions of the manuscript. All the authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Conflict of interest
FB reports royalties from Orthodevelopment and Smith and Nephew and compensation from Orthodevelopment, Smith and Nephew, Depuy and Medtronic, unrelated to this research. AGDV receives royalties from Orthodevelopment and Orthosensor and compensation by Johnson & Johnson and Link Bio, unrelated to this research. JB reports compensation by 3M, KCI and Aceity, unrelated to this research.
Ethical approval
The study was approved by the institutional review board.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Jungwirth-Weinberger, A., Bendich, I., Hanreich, C. et al. History of COVID-19 infection is not associated with increased d-dimer levels and risk of deep-vein thrombosis in total joint arthroplasty. Arch Orthop Trauma Surg 143, 785–789 (2023). https://doi.org/10.1007/s00402-021-04181-8
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00402-021-04181-8