


The Future of Point-of-Care Nucleic Acid Amplification Diagnostics after COVID-19: Time to Walk the Walk


Abstract
:1. Introduction
2. RT-PCR as a Point-of-Care Tool

{kind=link}
{kind=link}
| Test | Targets | LoD (cp/mL) b | Run | Specimen c | n d | PPA/NPA (%) e | Devices | Samples per Run | Read-Out | Reference |
|---|---|---|---|---|---|---|---|---|---|---|
| Monoplex | ||||||||||
| Xpert Xpress CoV-2 plus | N2, E and ORF1ab | 70 | 30 min | NP swab NS swab | 164 111 | 100/96.5 100/100 | GeneXpert Dx GeneXpert Infinity | 4 48/80 | Real-time fluorescence | Cepheid [35] |
| Xpert Xpress SARS-CoV-2 test | N2 and E | 125 | 30 min | NS swab | 90 | 95.8/95.6 | GeneXpert Dx GeneXpert Infinity | 4 48/80 | Real-time fluorescence | Cepheid [36,37] |
| cobas SARS-CoV-2 | ORF1ab and N | 12 | 20 min | NP swab | 230 | 96.1/96.8 | cobas® 6800 cobas® 8800 | 96 every 3 h 96 every 3 h | Real-time fluorescence | Roche [38] |
| MicroGEM Sal6830 SARS-CoV-2 Saliva Test | N and E | 6.4 × 103 | 30 min | Saliva | 119 | 87.2/97.2 | MicroGEM Sal6830 PoC PCR System | 1 | Real-time fluorescence | MicroGEM [39] |
| DASH SARS-CoV-2/S Test | N1 and N2 | 7.5 × 103 | 16 min | NS swab | 313 | 95.9/98.5 | DASH Analyzer | 1 | Real-time fluorescence | Minute Molecular [40,41] |
| Visby Medical COVID-19 Point of Care Test | N1 | 1.1 × 103 | 30 min | NP swab | 95 | 100/95.3 | Visby COVID-19 Device | 1 | Lateral-flow | Visby Medical [42,43] |
| Accula SARS-CoV-2 Test | N | 150 | 30 min | NS swab | 50 | 95.8/100 | Accula Dock | 1 | Lateral-flow | Accula [44] |
| Multiplex | ||||||||||
| Xpert Xpress CoV-2/Flu/RSV plus | N2, E and ORF1ab | 138 | 30 min | NP swab | 279 | 100/100 | GeneXpert Dx GeneXpert Infinity | 4 48/80 | Real-time fluorescence | Cepheid [45] |
| Xpert Xpress SARS-CoV-2/Flu/RSV | N2 and E | 131 | 30 min | NP swab | 240 | 97.9/100 | GeneXpert Dx GeneXpert Infinity | 4 48/80 | Real-time fluorescence | Cepheid [46] |
| cobas SARS-CoV-2 & Influenza A/B Nucleic Acid Test | ORF1ab and N | 12 | 20 min | NP swab NS swab | 935 930 | 95.2/99.6 96.4/99.5 | Cobas® Liat® System | 1 | Real-time fluorescence | Roche [47] |
| BioFire Respiratory Panel 2.1-EZ (RP2.1-EZ) a | S and M | 500 | 45 min | NP swab | 98 | 98/100 | BioFire® FilmArray® System | 1 | Real-time fluorescence | BioFire [27] |
3. Loop-Mediated Isothermal Amplification (LAMP) as a Point-of-Care Tool
4. Recombinase Polymerase Amplification (RPA) and Recombinase-Aided Amplification (RAA) as Point-of-Care Tools
5. Other Isothermal Amplification Techniques as Point-of-Care Tools
| Test | Use a | Targets | LoD (cp/mL) c | Run | Specimen d | n e | PPA/NPA (%) f | Device | Samples per Run | Readout g | Reference |
|---|---|---|---|---|---|---|---|---|---|---|---|
| LAMP | |||||||||||
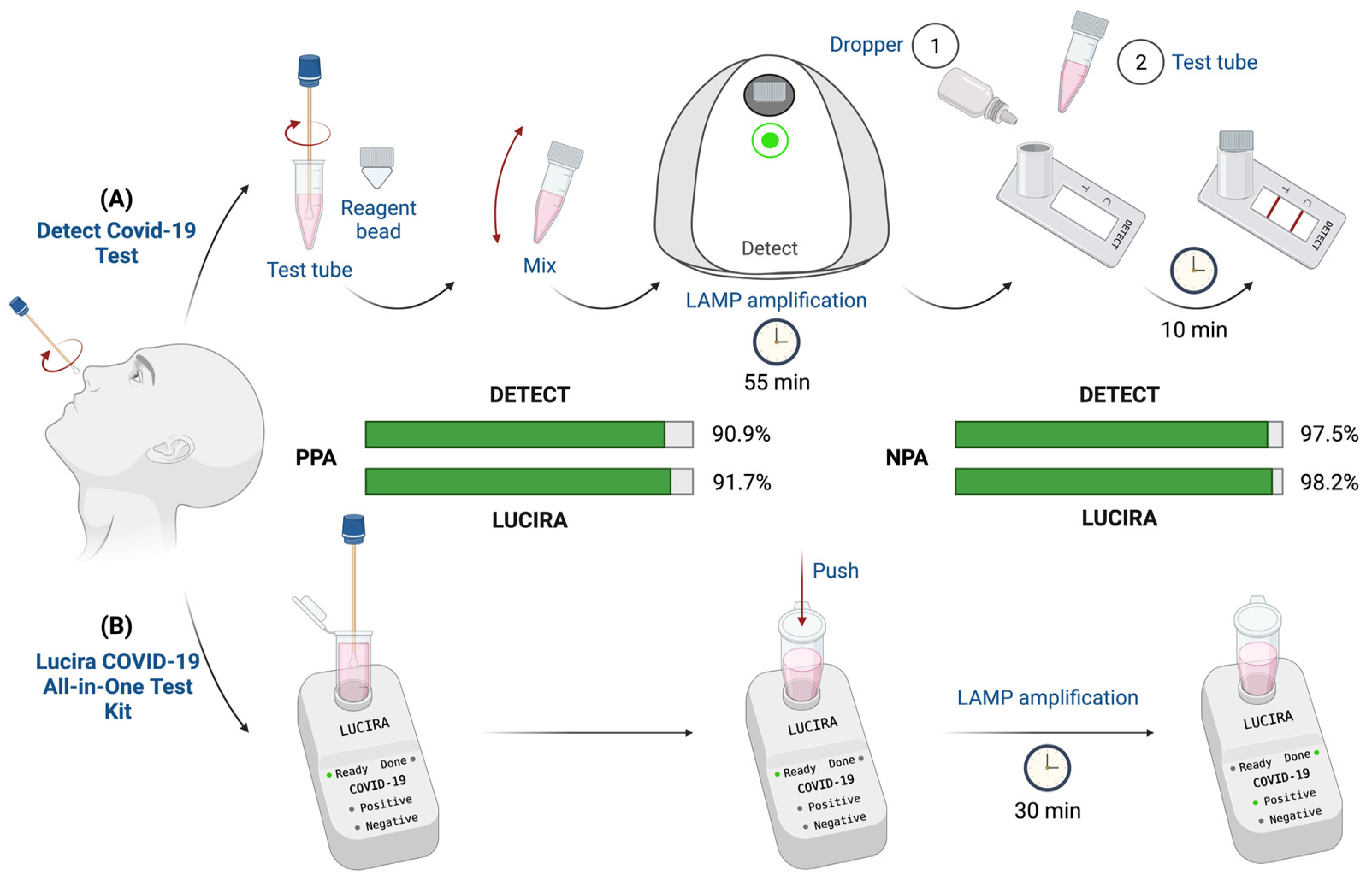
| Detect COVID-19 Test | POC Home | ORF1ab | 800 | 55 min | NP swab | 112 | 90.9/97.5 | Detect Hub | 1 | Lateral flow App | Detect [64] |
| Lucira COVID-19 All-in-One Test Kit | POC Home | N | 900 | 30 min | NS swab | 404 | 91.7/98.2 | Lucira Test Unit | 1 | Color change-LED detector | Lucira Health [66] |
| UOL COVID-19 Test | POC | N/D b | 2.6 × 103 | 40 min | NP swab | 207 | 87.7/100 | UOL COVID-19 Instrument | 1 | Fluorescence App | Uh-Oh LABS [101] |
| DxLab COVID-19 Test | POC | M | 6 × 104 | 25 min | NS swab | 139 | 86/100 | DxHub Instrument | 8 | Fluorescence | DxLab [102] |
| NEAR | |||||||||||
| ID NOW COVID-19 | POC | ORF1ab | 125 | 13 min | NP swab NS swab | 207 | 94.5/99.3 | ID NOW Intstrument | 1 | FLMB | Abbott [90,103] |
| ID NOW COVID-19 2.0 | POC | ORF1ab | 500 | 12 min | NP swab NS swab | 438 430 | 92.5/98.4 94.0/98.6 | ID NOW Intstrument | 1 | FLMB | Abbott [91] |
| Qualitative Isothermal NAAT | |||||||||||
| Cue COVID-19 Test for Home and OTC Use | POC Home | N | 1.3 × 103 | 20 min | NS swab | 273 | 97.4/99.1 | Cue Instrument | 1 | App | Cue Health [104] |
| Talis One COVID-19 Test System | POC | ORF1ab N | 500 | 27 min | NS swab | 98 | 100/100 | Talis One | 1 | Probe-specific fluorescence | Talis [105] |
6. Nucleic Acid Amplification Combined with CRISPR Diagnostics, a New Point-of-Care Approach
7. Point-of-Care SARS-CoV-2 Variant Diagnostic Challenge
8. Perspectives
9. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Liang, S.T.; Liang, L.T.; Rosen, J.M. COVID-19: A comparison to the 1918 influenza and how we can defeat it. Postgrad. Med. J. 2021, 97, 273–274. [Google Scholar] [CrossRef] [PubMed]
- Kilbourne, E.D. Influenza pandemics of the 20th century. Emerg. Infect. Dis. 2006, 12, 9–14. [Google Scholar] [CrossRef]
- Fineberg, H.V. Pandemic preparedness and response—Lessons from the H1N1 Influenza of 2009. N. Engl. J. Med. 2014, 370, 1335–1342. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kucharski, A.J.; Edmunds, W.J. Case fatality rate for Ebola Virus disease in West Africa. Lancet 2014, 384, 1260–1261. [Google Scholar] [CrossRef] [Green Version]
- Peeri, N.C.; Shrestha, N.; Siddikur Rahman, M.; Zaki, R.; Tan, Z.; Bibi, S.; Baghbanzadeh, M.; Aghamohammadi, N.; Zhang, W.; Haque, U. The SARS, MERS and novel coronavirus (COVID-19) epidemics, the newest and biggest global health threats: What lessons have we learned? Int. J. Epidemiol. 2021, 49, 717–726. [Google Scholar] [CrossRef] [Green Version]
- Yan, Y.; Chang, L.; Wang, L. Laboratory testing of SARS-CoV, MERS-CoV, and SARS-CoV-2 (2019-nCoV): Current status, challenges, and countermeasures. Rev. Med. Virol. 2020, 30, e2106. [Google Scholar] [CrossRef] [PubMed]
- Wagner-Carena, J. Preparing for the next pandemic. Nat. Med. 2021, 27, 357. [Google Scholar]
- Au, W.Y.; Hang Cheung, P.P. Diagnostic performances of common nucleic acid tests for SARS-CoV-2 in hospitals and clinics: A systematic review and meta-analysis. Lancet Microbe 2021, 2, e704–e714. [Google Scholar] [CrossRef]
- Bi, Q.; Wu, Y.; Mei, S.; Ye, C.; Zou, X.; Zhang, Z.; Liu, X.; Wei, L.; Truelove, S.A.; Zhang, T.; et al. Epidemiology and transmission of COVID-19 in 391 cases and 1286 of their close contacts in Shenzhen, China: A retrospective cohort study. Lancet Infect. Dis. 2020, 20, 911–919. [Google Scholar] [CrossRef]
- De Felice, M.; De Falco, M.; Zappi, D.; Antonacci, A.; Scognamiglio, V. Isothermal amplification-assisted diagnostics for COVID-19. Biosens. Bioelectron. 2022, 205, 114101. [Google Scholar] [CrossRef]
- Mercer, T.R.; Salit, M. Testing at scale during the COVID-19 pandemic. Nat. Rev. Genet. 2021, 22, 415–426. [Google Scholar] [CrossRef] [PubMed]
- Guglielmi, G. Rapid Coronavirus tests: A guide for the perplexed. Nature 2021, 590, 202–205. [Google Scholar] [CrossRef] [PubMed]
- Boum, Y.; Eyangoh, S.; Okomo, M.-C. Beyond COVID-19—Will self-sampling and testing become the norm? Lancet Infect. Dis. 2021, 3099, 3–4. [Google Scholar] [CrossRef]
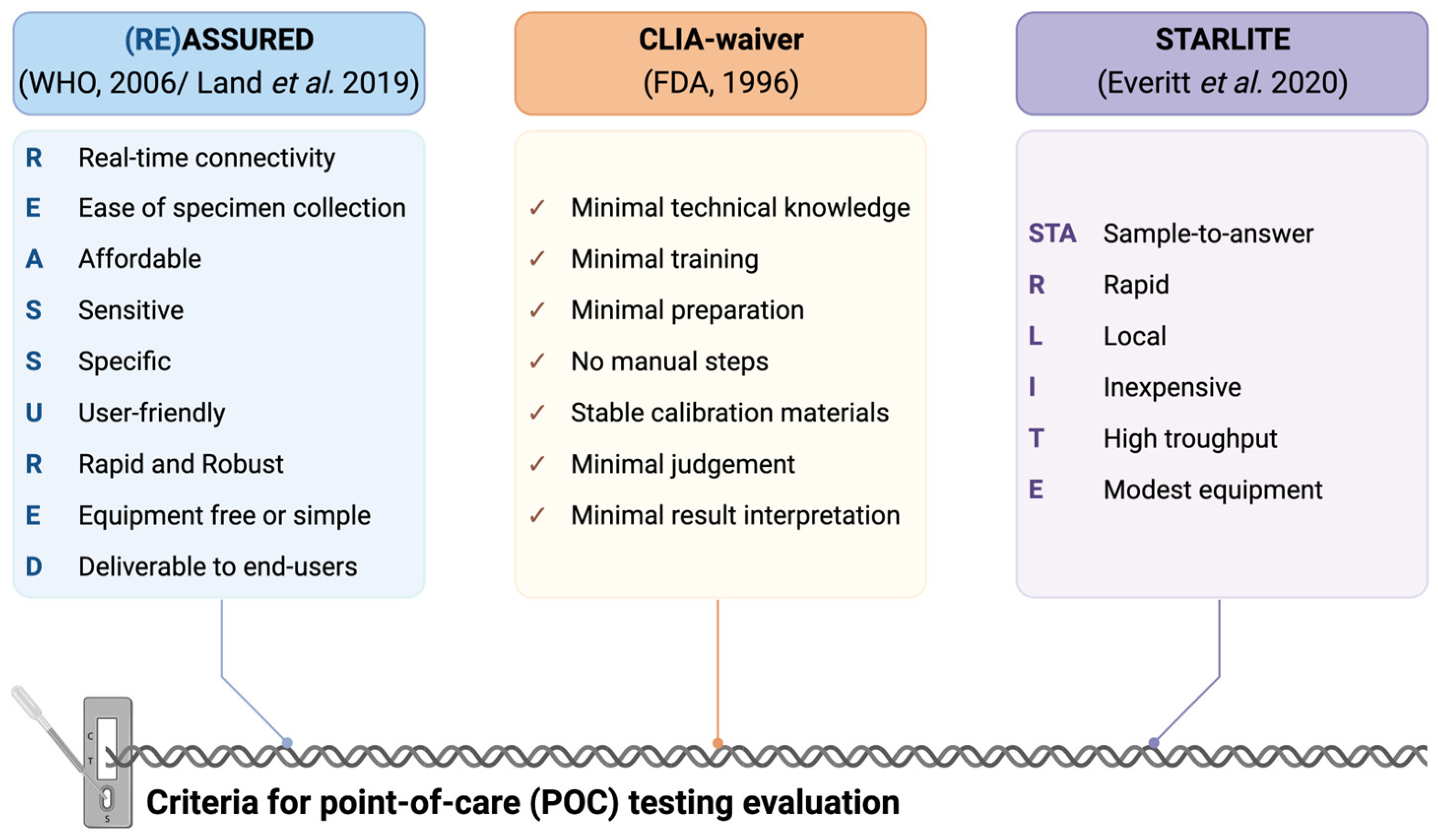
- Everitt, M.L.; Tillery, A.; David, M.G.; Singh, N.; Borison, A.; White, I.M. A critical review of point-of-care diagnostic technologies to combat viral pandemics. Anal. Chim. Acta 2021, 1146, 184–199. [Google Scholar] [CrossRef]
- Cheshmehzangi, A.; Zou, T. Discourse on COVID-19 Mass Testing vs. Rapid Testing Processing. Front. Public Health 2022, 10, 1–4. [Google Scholar] [CrossRef]
- Ghaffari, A.; Meurant, R.; Ardakani, A. COVID-19 point-of-care diagnostics that satisfy global target product profiles. Diagnostics 2021, 11, 115. [Google Scholar] [CrossRef]
- Kettler, H.; White, K.; Hawkes, S. Mapping the Landscape of Diagnostics for Sexually Transmitted Infections: Key Findings and Recommandations; WHO: Geneva, Switzerland, 2004; pp. 1–44. [Google Scholar]
- Land, K.J.; Boeras, D.I.; Chen, X.S.; Ramsay, A.R.; Peeling, R.W. REASSURED diagnostics to inform disease control strategies, strengthen health systems and improve patient outcomes. Nat. Microbiol. 2019, 4, 46–54. [Google Scholar] [CrossRef]
- U.S. Food & Drug Administration, Centre for Devices & Radiological Health. Recommendations for Clinical Applications for Manufacturers of in Amendments of 1988 (CLIA) Waiver Laboratory Improvement Vitro Diagnostic Devices; U.S. Food & Drug Administration, Centre for Devices & Radiological Health: Silver Spring, MD, USA, 2020.
- Lisboa Bastos, M.; Tavaziva, G.; Abidi, S.K.; Campbell, J.R.; Haraoui, L.P.; Johnston, J.C.; Lan, Z.; Law, S.; MacLean, E.; Trajman, A.; et al. Diagnostic accuracy of serological tests for COVID-19: Systematic review and meta-analysis. BMJ 2020, 370, 1–13. [Google Scholar] [CrossRef]
- Arnaout, R.; Lee, R.A.; Lee, G.R.; Callahan, C.; Yen, C.F.; Smith, K.P.; Arora, R.; Kirby, J.E. SARS-CoV-2 testing: The limit of detection matters. bioRxiv 2020. [Google Scholar] [CrossRef]
- García-Bernalt Diego, J.; Fernández-Soto, P.; Domínguez-Gil, M.; Belhassen-García, M.; Bellido, J.L.M.; Muro, A. A simple, affordable, rapid, stabilized, colorimetric, versatile RT-LAMP assay to detect SARS-CoV-2. Diagnostics 2021, 11, 438. [Google Scholar] [CrossRef]
- Zhao, Y.; Chen, F.; Li, Q.; Wang, L.; Fan, C. Isothermal Amplification of Nucleic Acids. Chem. Rev. 2015, 115, 12491–12545. [Google Scholar] [CrossRef] [PubMed]
- Drain, P.K. Rapid Diagnostic Testing for SARS-CoV-2. N. Engl. J. Med. 2022, 386, 264–272. [Google Scholar] [CrossRef]
- Gupta, N.; Augustine, S.; Narayan, T.; O’Riordan, A.; Das, A.; Kumar, D.; Luong, J.H.T.; Malhotra, B.D. Point-of-care PCR assays for COVID-19 detection. Biosensors 2021, 11, 141. [Google Scholar] [CrossRef] [PubMed]
- U.S. Food & Drug Administration. In Vitro Diagnostics EUAs—Molecular Diagnostic Tests for SARS-CoV-2. Available online: https://www.fda.gov/medical-devices/coronavirus-disease-2019-covid-19-emergency-use-authorizations-medical-devices/in-vitro-diagnostics-euas-molecular-diagnostic-tests-sars-cov-2#individual-molecular (accessed on 7 June 2022).
- BioFire. BioFire® Respiratory Panel 2.1-EZ (RP2.1-EZ), Instructions for Use. Available online: https://www.fda.gov/media/142696/download (accessed on 20 July 2022).
- Hogan, C.A.; Garamani, N.; Lee, A.S.; Tung, J.K.; Sahoo, M.K.; Huang, C.H.; Stevens, B.; Zehnder, J.; Pinsky, B.A. Comparison of the accula SARS-CoV-2 test with a laboratory-developed assay for detection of SARS-CoV-2 RNA in clinical nasopharyngeal specimens. J. Clin. Microbiol. 2020, 58, 2–6. [Google Scholar] [CrossRef] [PubMed]
- Cepheid. GeneXpert System. 2022. Available online: https://cepheid.widen.net/content/nxaaerhcgx/pdf/Cepheid-GeneXpert-System-Brochure-US-IVD-0112-English.pdf?u=bk12mm (accessed on 18 July 2022).
- Mostafa, H.H.; Carroll, K.C.; Hicken, R.; Berry, G.J.; Manji, R.; Smith, E.; Rakeman, J.L.; Fowler, R.C.; Leelawong, M.; Butler-Wu, S.M.; et al. Multicenter evaluation of the cepheid xpert xpress SARS-CoV-2/Flu/RSV test. J. Clin. Microbiol. 2021, 59, e02955-20. [Google Scholar] [CrossRef] [PubMed]
- Wolters, F.; Grünberg, M.; Huber, M.; Kessler, H.H.; Prüller, F.; Saleh, L.; Langendoen, J.R.; Fébreau, C.; Thibault, V.; Melchers, W.J.G. European multicenter evaluation of Xpert® Xpress SARS-CoV-2/Flu/RSV test. J. Med. Virol. 2021, 93, 5798–5804. [Google Scholar] [CrossRef] [PubMed]
- Ho Kim, S.; AlMutawa, F. Tracheal Aspirate and Bronchoalveolar Lavage as Potential Specimen Types for COVID-19 Testing Using the Cepheid Xpert. Microbiol. Spectr. 2021, 10, 1–5. [Google Scholar]
- Creager, H.M.; Cabrera, B.; Schnaubelt, A.; Cox, J.L.; Cushman-vokoun, A.M.; Shakir, S.M.; Tardif, K.D.; Huang, M.; Rogatcheva, M.; Bourzac, K.M.; et al. Clinical evaluation of the BioFire® Respiratory Panel 2.1 and detection of SARS-CoV-2. J. Clin. Virol. 2020, 129, 1–4. [Google Scholar] [CrossRef]
- Chang, Y.-C.; Hsiao, C.-T.; Chen, W.-L.; Su, Y.-D.; Hsueh, P.-R. BioFire FilmArray respiratory panel RP2.1 for SARS-CoV-2 detection: The pitfalls. J. Infect. 2022, 5, e1–e3. [Google Scholar] [CrossRef]
- GeneXpert. Xpert® Xpress CoV-2 Plus, Instructions for Use. Available online: https://www.fda.gov/media/158407/download (accessed on 20 July 2022).
- GeneXpert. Xpert® Xpress SARS-CoV-2, Instructions for Use. Available online: https://www.fda.gov/media/136315/download (accessed on 20 July 2022).
- Phan, T.; Mays, A.; McCullough, M.; Wells, A. Evaluation of the Cepheid Xpert Xpress SARS-CoV-2 test for bronchoalveolar lavage. J. Clin. Virol. Plus 2022, 2, 100067. [Google Scholar] [CrossRef]
- Cobas®Liat. Cobas® SARS-CoV-2, Instructions for Use. Available online: https://www.fda.gov/media/150278/download (accessed on 20 July 2022).
- MicroGEM. MicroGEM Sal6830 SARS-CoV-2 Saliva Test Instructions for Use. Available online: https://www.fda.gov/media/157754/download (accessed on 20 July 2022).
- Minute Molecular. DASH SARS-CoV-2/S Test, Instructions for Use. Available online: https://www.fda.gov/media/156979/download (accessed on 20 July 2022).
- Achenbach, C.J.; Caputo, M.; Hawkins, C.; Balmert, L.C.; Qi, C.; Odorisio, J.; Dembele, E.; Jackson, A.; Abbas, H.; Frediani, J.K.; et al. Clinical evaluation of the Diagnostic Analyzer for Selective Hybridization (DASH): A point-of-care PCR test for rapid detection of SARS-CoV-2 infection. medRxiv 2022. [Google Scholar] [CrossRef] [PubMed]
- Visby Medical. COVID-19 Point of Care. Available online: https://www.fda.gov/media/145917/download (accessed on 20 July 2022).
- Katzman, B.M.; Wockenfus, A.M.; Kelley, B.R.; Karon, B.S.; Donato, L.J. Evaluation of the Visby medical COVID-19 point of care nucleic acid amplification test. Clin. Biochem. 2021. [Google Scholar] [CrossRef] [PubMed]
- Accula. Accula SARS-CoV-2 Test, Instructions for Use. Available online: https://www.fda.gov/media/136355/download (accessed on 20 July 2022).
- Cepheid. Xpert® Xpress CoV-2/Flu/RSV Plus, Instructions for Use. Available online: https://www.fda.gov/media/152164/download (accessed on 25 July 2022).
- Cepheid. GeneXpert Xpert® Xpress SARS-CoV-2/Flu/RSV, Instructions for Use. Available online: https://www.fda.gov/media/142438/download (accessed on 25 July 2022).
- Roche. cobas SARS-CoV-2 & Influenza A/B—Nucleic Acid Test for Use on the Cobas Liat System, Instructions for Use. Available online: https://www.fda.gov/media/142193/download (accessed on 25 July 2022).
- Gibani, M.M.; Toumazou, C.; Sohbati, M.; Sahoo, R.; Karvela, M.; Hon, T.K.; De Mateo, S.; Burdett, A.; Leung, K.Y.F.; Barnett, J.; et al. Assessing a novel, lab-free, point-of-care test for SARS-CoV-2 (CovidNudge): A diagnostic accuracy study. Lancet Microbe 2020, 1, e300–e307. [Google Scholar] [CrossRef]
- PreciGenome, LLC. FastPlex Triplex SARS-CoV-2 Detection Kit (RT-Digital PCR) Instructions for Use. Available online: https://www.fda.gov/media/139523/download (accessed on 25 July 2022).
- Xu, J.; Kirtek, T.; Xu, Y.; Zheng, H.; Yao, H.; Ostman, E.; Oliver, D.; Malter, J.S.; Gagan, J.R.; Sorelle, J.A.; et al. Digital Droplet PCR for SARS-CoV-2 Resolves Borderline Cases. Am. J. Clin. Pathol. 2021, 155, 815–822. [Google Scholar] [CrossRef] [PubMed]
- Islam, M.M.; Koirla, D. Toward a next-generation diagnostic tool: A review on emerging isothermal nucleic acid amplification techniques for the detection of SARS-CoV-2 and other infectious viruses. Anal. Chim. Acta 2021, 1209, 339338. [Google Scholar] [CrossRef] [PubMed]
- Notomi, T.; Okayama, H.; Masubuchi, H.; Yonekawa, T.; Watanabe, K.; Amino, N.; Hase, T. Loop-mediated isothermal amplification of DNA. Nucleic Acids Res. 2000, 28, e63. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, S.Q.; Tan, B.; Li, P.; Wang, F.X.; Guo, L.; Yang, Y.; Sun, N.; Zhu, H.W.; Wen, Y.J.; Cheng, S.P. Comparison of conventional RT-PCR, reverse-transcription loop-mediated isothermal amplification, and SYBR green I-based real-time RT-PCR in the rapid detection of bovine viral diarrhea virus nucleotide in contaminated commercial bovine sera batches. J. Virol. Methods 2014, 207, 204–209. [Google Scholar] [CrossRef]
- Kidd, S.P.; Burns, D.; Armson, B.; Beggs, A.D.; Howson, E.L.A.; Williams, A.; Snell, G.; Wise, E.L.; Goring, A.; Vincent-Mistiaen, Z.; et al. Reverse-Transcription Loop-Mediated Isothermal Amplification Has High Accuracy for Detecting Severe Acute Respiratory Syndrome Coronavirus 2 in Saliva and Nasopharyngeal/Oropharyngeal Swabs from Asymptomatic and Symptomatic Individuals. J. Mol. Diagn. 2022, 24, 320–336. [Google Scholar] [CrossRef]
- Rödel, J.; Egerer, R.; Suleyman, A.; Sommer-Schmid, B.; Baier, M.; Henke, A.; Edel, B.; Löffler, B. Use of the VariplexTM SARS-CoV-2 RT-LAMP as a rapid molecular assay to complement RT-PCR for COVID-19 diagnosis. J. Clin. Virol. 2020, 132, 104616. [Google Scholar] [CrossRef]
- García-Bernalt Diego, J.; Fernández-Soto, P.; Muñoz-Bellido, J.L.; Febrer-Sendra, B.; Crego-Vicente, B.; Carbonell, C.; López-Bernús, A.; Marcos, M.; Belhassen-García, M.; Muro, A. Detection of SARS-CoV-2 RNA in urine by RT-LAMP: A very rare finding. J. Clin. Med. 2022, 11, 158. [Google Scholar] [CrossRef]
- Beggs, A.D.; Manzoor, S.E.; Zaman, S.; Whalley, C.; Inglis, D.; Bosworth, A.; Kidd, M.; Shabir, S.; Quraishi, N.; Green, C.A.; et al. Multi-modality detection of SARS-CoV-2 in faecal donor samples for transplantation and in asymptomatic emergency surgical admissions. F1000Research 2021, 10, 1–13. [Google Scholar]
- Ongerth, J.E.; Danielson, R.E. RT qLAMP—Direct Detection of SARS-CoV-2 in Raw Sewage. J. Biomol. Tech. 2021, 32, 206–213. [Google Scholar] [CrossRef] [PubMed]
- Guadalupe, J.J.; Rojas, M.I.; Pozo, G.; Erazo-Garcia, M.P.; Vega-Polo, P.; Terán-Velástegui, M.; Rohwer, F.; de Torres, M.L. Presence of SARS-CoV-2 RNA on surfaces of public places and a transportation system located in a densely populated urban area in South America. Viruses 2022, 14, 19. [Google Scholar] [CrossRef]
- Wang, W.; Xu, Y.; Gao, R.; Lu, R.; Han, K.; Wu, G.; Tan, W. Detection of SARS-CoV-2 in Different Types of Clinical Specimens. JAMA J. Am. Med. Assoc. 2020, 323, 1843–1844. [Google Scholar] [CrossRef] [Green Version]
- Li, Z.; Bruce, J.L.; Cohen, B.; Cunningham, C.V.; Jack, W.E.; Kunin, K.; Langhorst, B.W.; Miller, J.; Moncion, R.A.; Poole, C.B.; et al. Development and Implementation of a Simple and Rapid Extraction-Free Saliva SARS-CoV-2 RT-LAMP Workflow for Workplace Surveillance. medRxiv 2022. [Google Scholar] [CrossRef] [PubMed]
- Newman, C.M.; Ramuta, M.D.; McLaughlin, M.T.; Wiseman, R.W.; Karl, J.A.; Dudley, D.M.; Stauss, M.R.; Maddox, R.J.; Weiler, A.M.; Bliss, M.I.; et al. Initial Evaluation of a Mobile SARS-CoV-2 RT-LAMP Testing Strategy. J. Biomol. Tech. 2021, 32, 137–147. [Google Scholar] [CrossRef]
- Baba, M.M.; Bitew, M.; Fokam, J.; Lelo, E.A.; Ahidjo, A.; Asmamaw, K.; Beloumou, G.A.; Bulimo, W.D.; Buratti, E.; Chenwi, C.; et al. Diagnostic performance of a colorimetric RT-LAMP for the identification of SARS-CoV-2: A multicenter prospective clinical evaluation in sub-Saharan Africa. eClinicalMedicine 2021, 40, 101101. [Google Scholar] [CrossRef]
- Detect. DetectTM Covid-19 Test Instructions for Use for Healthcare Providers. Available online: https://www.fda.gov/media/153746/download (accessed on 2 September 2022).
- Bruijns, B.; Folkertsma, L.; Tiggelaar, R. FDA authorized molecular point-of-care SARS-CoV-2 tests: A critical review on principles, systems and clinical performances. Biosens. Bioelectron. X 2022, 11, 100158. [Google Scholar] [CrossRef]
- Lucira Health LuciraTM COVID-19 Instruction for Use. Available online: https://www.fda.gov/media/147495/download (accessed on 2 September 2022).
- Ball, C.S.; Light, Y.K.; Koh, C.Y.; Wheeler, S.S.; Coffey, L.L.; Meagher, R.J. Quenching of Unincorporated Amplification Signal Reporters in Reverse-Transcription Loop-Mediated Isothermal Amplification Enabling Bright, Single-Step, Closed-Tube, and Multiplexed Detection of RNA Viruses. Anal. Chem. 2016, 88, 3562–3568. [Google Scholar] [CrossRef]
- Ma, X.; Shu, Y.; Nie, K.; Qin, M.; Wang, D.; Gao, R.; Wang, M.; Wen, L.; Han, F.; Zhou, S.; et al. Visual detection of pandemic influenza A H1N1 Virus 2009 by reverse-transcription loop-mediated isothermal amplification with hydroxynaphthol blue dye. J. Virol. Methods 2010, 167, 214–217. [Google Scholar] [CrossRef]
- Ding, S.; Chen, G.; Wei, Y.; Dong, J.; Du, F.; Cui, X.; Huang, X.; Tang, Z. Sequence-specific and multiplex detection of COVID-19 virus (SARS-CoV-2) using proofreading enzyme-mediated probe cleavage coupled with isothermal amplification. Biosens. Bioelectron. 2021, 178, 113041. [Google Scholar] [CrossRef] [PubMed]
- Xu, C.; Wang, H.; Jin, H.; Feng, N.; Zheng, X.; Cao, Z.; Li, L.; Wang, J.; Yan, F.; Wang, L.; et al. Visual detection of Ebola virus using reverse transcription loop-mediated isothermal amplification combined with nucleic acid strip detection. Arch. Virol. 2016, 161, 1125–1133. [Google Scholar] [CrossRef] [PubMed]
- Chow, F.W.N.; Chan, T.T.Y.; Tam, A.R.; Zhao, S.; Yao, W.; Fung, J.; Cheng, F.K.K.; Lo, G.C.S.; Chu, S.; Aw-Yong, K.L.; et al. A Rapid, simple, inexpensive, and mobile colorimetric assay COVID-19-LAMP for mass on-site screening of COVID-19. Int. J. Mol. Sci. 2020, 21, 5380. [Google Scholar] [CrossRef] [PubMed]
- Rodriguez-Manzano, J.; Malpartida-Cardenas, K.; Moser, N.; Pennisi, I.; Cavuto, M.; Miglietta, L.; Moniri, A.; Penn, R.; Satta, G.; Randell, P.; et al. Handheld point-of-care system for rapid detection of SARS-CoV-2 extracted RNA in under 20 min. ACS Cent. Sci. 2021, 7, 307–317. [Google Scholar] [CrossRef]
- Ge, A.; Liu, F.; Teng, X.; Cui, C.; Wu, F.; Liu, W.; Liu, Y.; Chen, X.; Xu, J.; Ma, B. A Palm Germ-Radar (PaGeR) for rapid and simple COVID-19 detection by reverse transcription loop-mediated isothermal amplification (RT-LAMP). Biosens. Bioelectron. 2022, 200, 113925. [Google Scholar] [CrossRef]
- Rohaim, M.A.; Clayton, E.; Sahin, I.; Vilela, J.; Khalifa, M.E.; Al-natour, M.Q.; Bayoumi, M.; Poirier, A.C.; Branavan, M.; Tharmakulasingam, M.; et al. Artificial intelligence-assisted loop mediated isothermal amplification (AI-LAMP) for rapid detection of SARS-CoV-2. Viruses 2020, 12, 972. [Google Scholar] [CrossRef]
- García-Bernalt Diego, J.; Fernández-Soto, P.; Márquez-Sánchez, S.; Santos Santos, D.; Febrer-Sendra, B.; Crego-Vicente, B.; Muñoz-Bellido, J.L.; Belhassen-García, M.; Corchado Rodríguez, J.M.; Muro, A. SMART-LAMP: A smartphone-operated handheld device for real-time colorimetric point-of-care diagnosis of infectious diseases via loop-mediated isothermal amplification. Biosensors 2022, 12, 424. [Google Scholar] [CrossRef]
- Lobato, I.M.; O’Sullivan, C.K. Recombinase polymerase amplification: Basics, applications and recent advances. TrAC-Trends Anal. Chem. 2018, 98, 19–35. [Google Scholar] [CrossRef]
- Euler, M.; Wang, Y.; Nentwich, O.; Piepenburg, O.; Hufert, F.T.; Weidmann, M. Recombinase polymerase amplification assay for rapid detection of Rift Valley fever virus. J. Clin. Virol. 2012, 54, 308–312. [Google Scholar] [CrossRef]
- Zaghloul, H.; El-Shahat, M. Recombinase polymerase amplification as a promising tool in hepatitis C virus diagnosis. World J. Hepatol. 2014, 6, 916–922. [Google Scholar] [CrossRef]
- Xiong, E.; Jiang, L.; Tian, T.; Hu, M.; Yue, H.; Huang, M.; Lin, W.; Jiang, Y.; Zhu, D.; Zhou, X. Simultaneous Dual-Gene Diagnosis of SARS-CoV-2 Based on CRISPR/Cas9-Mediated Lateral Flow Assay. Angew. Chem.-Int. Ed. 2021, 60, 5307–5315. [Google Scholar] [CrossRef] [PubMed]
- Xiong, D.; Dai, W.; Gong, J.; Li, G.; Liu, N.; Wu, W.; Pan, J.; Chen, C.; Jiao, Y.; Deng, H.; et al. Rapid detection of SARS-CoV-2 with CRISPRCas12a. PLoS Biol. 2020, 18, e3000978. [Google Scholar] [CrossRef] [PubMed]
- Cao, G.; Huo, D.; Chen, X.; Wang, X.; Zhou, S.; Zhao, S.; Luo, X.; Hou, C. Talanta Automated, portable, and high-throughput fluorescence analyzer (APHF-analyzer) and lateral flow strip based on CRISPR/Cas13a for sensitive and visual detection of SARS-CoV-2. Talanta 2022, 248, 123594. [Google Scholar] [CrossRef] [PubMed]
- Fan, X.; Li, L.; Zhao, Y.; Liu, Y.; Liu, C.; Wang, Q.; Dong, Y.; Wang, S.; Chi, T.; Song, F.; et al. Clinical Validation of Two Recombinase-Based Isothermal Amplification Assays (RPA/RAA) for the Rapid Detection of African Swine Fever Virus. Front. Microbiol. 2020, 11, 1696. [Google Scholar] [CrossRef]
- Wang, J.; Cai, K.; He, X.; Shen, X.; Liu, J.; Xu, J.; Qiu, F.; Lei, W.; Cui, L.; Ge, Y.; et al. Multiple-centre clinical evaluation of an ultrafast single-tube assay for SARS-CoV-2 RNA. Clin. Microbiol. Infect. 2020, 26, 1076–1081. [Google Scholar] [CrossRef]
- Shen, X.; Wang, J.; Li, J.; He, A.; Liu, H.; Ma, X. Field validation of a rapid recombinase aided amplification assay for SARS-CoV-2 RNA at customs—Zhejiang Province, China, January 2021. China CDC Wkly. 2021, 3, 973–976. [Google Scholar] [CrossRef]
- Yu, F.; Xie, G.; Zheng, S.; Han, D.; Bao, J.; Zhang, D.; Feng, B.; Wang, Q.; Zou, Q.; Wang, R.; et al. Assessment of the Diagnostic Ability of Four Detection Methods Using Three Sample Types of COVID-19 Patients. Front. Cell. Infect. Microbiol. 2021, 11, 497. [Google Scholar] [CrossRef]
- Li, J.; Macdonald, J. Advances in isothermal amplification: Novel strategies inspired by biological processes. Biosens. Bioelectron. 2015, 64, 196–211. [Google Scholar] [CrossRef]
- James, A.S.; Alwneh, J.I. COVID-19 Infection Diagnosis: Potential Impact of Isothermal Amplification Technology to Reduce Community Transmission of SARS-CoV-2. Diagnostics 2020, 10, 399. [Google Scholar] [CrossRef]
- Qian, C.; Wang, R.; Wu, H.; Ji, F.; Wu, J. Nicking enzyme-assisted amplification (NEAA) technology and its applications: A review. Anal. Chim. Acta 2019, 1050, 1–15. [Google Scholar] [CrossRef]
- Wang, L.; Qian, C.; Wu, H.; Qian, W.; Wang, R.; Wu, J. Technical aspects of nicking enzyme assisted amplification. Analyst 2018, 143, 1444–1453. [Google Scholar] [CrossRef] [PubMed]
- Abbott. Id NowTM Covid-19, Instructions for Use. Available online: https://www.fda.gov/media/136525/download (accessed on 3 September 2022).
- Abbott. ID NOW COVID-19 2.0, Instructions for Use. Available online: https://www.fda.gov/media/158402/download (accessed on 3 September 2022).
- Compton, J. Nucleic acid sequence-based amplification. Nature 1991, 350, 91–92. [Google Scholar] [CrossRef]
- Wu, Q.; Suo, C.; Brown, T.; Wang, T.; Teichmann, S.A.; Bassett, A.R. INSIGHT: A population-scale COVID-19 testing strategy combining point-of-care diagnosis with centralized high-throughput sequencing. Sci. Adv. 2021, 7, eabe5054. [Google Scholar] [CrossRef] [PubMed]
- Qian, J.; Ferguson, T.M.; Shinde, D.N.; Ramírez-Borrero, A.J.; Hintze, A.; Adami, C.; Niemz, A. Sequence dependence of isothermal DNA amplification via EXPAR. Nucleic Acids Res. 2012, 40, e87. [Google Scholar] [CrossRef] [PubMed]
- Carter, J.G.; Iturbe, L.O.; Duprey, J.L.H.A.; Carter, I.R.; Southern, C.D.; Rana, M.; Whalley, C.M.; Bosworth, A.; Beggs, A.D.; Hicks, M.R.; et al. Ultrarapid detection of SARS-CoV-2 RNA using a reverse transcription-free exponential amplification reaction, RTF-EXPAR. Proc. Natl. Acad. Sci. USA 2021, 118, e2100347118. [Google Scholar] [CrossRef] [PubMed]
- Song, Y.; Chao, Y.; Guo, Y.; Zhang, F.; Mao, C.; Guan, C.; Chen, G.; Feng, C. Paper-based netlike rolling circle amplification (NRCA) for ultrasensitive and visual detection of SARS-CoV-2. Sens. Actuators B Chem. 2022, 358, 131460. [Google Scholar] [CrossRef] [PubMed]
- Park, G.S.; Maeng, J.S. A novel isothermal method for amplification of long specific amplicon from linear template. Sci. Rep. 2022, 12, 2756. [Google Scholar] [CrossRef]
- Zasada, A.A.; Mosiej, E.; Prygiel, M.; Polak, M.; Wdowiak, K.; Marchlewicz, K.; Nowi, A.; Rastawicki, W.; Nowi, J. Detection of SARS-CoV-2 Using Reverse Transcription Helicase Dependent Amplification and Reverse Transcription Loop-Mediated Amplification Combined with Lateral Flow Assay. Biomedicines 2022, 10, 2329. [Google Scholar] [CrossRef]
- Microbiol, C.; Wu, S.; Shi, X.; Chen, Q.; Jiang, Y.; Zuo, L.; Wang, L.; Jiang, M.; Lin, Y.; Fang, S.; et al. Comparative evaluation of six nucleic acid amplification kits for SARS-CoV-2 RNA detection. Ann. Clin. Microbiol. Antimicrob. 2021, 20, 1–6. [Google Scholar]
- Dierks, S.; Bader, O.; Schwanbeck, J.; Groß, U.; Weig, M.S.; Mese, K.; Lugert, R.; Bohne, W.; Hahn, A.; Feltgen, N.; et al. Diagnosing SARS-CoV-2 with Antigen Testing, Transcription-Mediated Amplification and Real-Time PCR. J. Clin. Med. 2021, 10, 2404. [Google Scholar] [CrossRef]
- Uh-Oh LABS. UOL COVID-19 Test, Instructions for Use. Available online: https://www.fda.gov/media/156102/download (accessed on 4 September 2022).
- DxLab. DxLab COVID-19 Test, Instructions for Use. Available online: https://www.fda.gov/media/158980/download (accessed on 4 September 2022).
- Babic, N.; Garner, K.S.; Hirschhorn, J.W.; Zebian, R.; Nolte, F.S. Evaluation of Abbott ID NOW COVID-19 POC test performance characteristics and integration in the regional health network workflows to improve health care delivery. Clin. Biochem. 2021. [Google Scholar] [CrossRef] [PubMed]
- Cue Health. The CueTM COVID-19 Test for Home and Over The Counter (OTC) Use. Instructions for Use. Available online: https://www.fda.gov/media/146471/download (accessed on 4 September 2022).
- Talis Biomedical Corporation. Talis One COVID-19 Test System, Instructions for Use. Available online: https://www.fda.gov/media/153943/download (accessed on 4 September 2022).
- Gasiunas, G.; Barrangou, R.; Horvath, P.; Siksnys, V. Cas9—crRNA ribonucleoprotein complex mediates speci fi c DNA cleavage for adaptive immunity in bacteria. Proc. Natl. Acad. Sci. USA 2012, 109, E2579–E2586. [Google Scholar] [CrossRef] [Green Version]
- Kaminski, M.M.; Abudayyeh, O.O.; Gootenberg, J.S.; Zhang, F.; Collins, J.J. CRISPR-based diagnostics. Nat. Biomed. Eng. 2021, 5, 643–656. [Google Scholar] [CrossRef] [PubMed]
- Joung, J.; Ladha, A.; Saito, M.; Kim, N.-G.; Woolley, A.E.; Segel, M.; Barretto, R.P.; Ranu, A.; Macrae, R.K.; Faure, G.; et al. Detection of SARS-CoV-2 with SHERLOCK One-Pot Testing To. N. Engl. J. Med. 2020, 383, 1492–1494. [Google Scholar] [CrossRef]
- Wang, R.; Qian, C.; Pang, Y.; Li, M.; Yang, Y.; Ma, H.; Zhao, M.; Qian, F.; Yu, H.; Liu, Z.; et al. opvCRISPR: One-pot visual RT-LAMP-CRISPR platform for SARS-CoV-2 detection. Biosens. Bioelectron. 2021, 172, 112766. [Google Scholar] [CrossRef] [PubMed]
- Mahas, A.; Wang, Q.; Marsic, T.; Mahfouz, M.M. A Novel Miniature CRISPR-Cas13 System for SARS-CoV-2 Diagnostics. ACS Synth. Biol. 2021, 10, 2541–2551. [Google Scholar] [CrossRef] [PubMed]
- De Puig, H.; Lee, R.A.; Najjar, D.; Tan, X.; Soekensen, L.R.; Angenent-Mari, N.M.; Donghia, N.M.; Weckman, N.E.; Ory, A.; Ng, C.F.; et al. Minimally instrumented SHERLOCK (miSHERLOCK) for CRISPR-based point-of-care diagnosis of SARS-CoV-2 and emerging variants. Sci. Adv. 2021, 7, 23–26. [Google Scholar] [CrossRef]
- Ackerman, C.M.; Myhrvold, C.; Thakku, S.G.; Freije, C.A.; Metsky, H.C.; Yang, D.K.; Ye, S.H.; Boehm, C.K.; Kosoko-Thoroddsen, T.S.F.; Kehe, J.; et al. Massively multiplexed nucleic acid detection with Cas13. Nature 2020, 582, 277–282. [Google Scholar] [CrossRef]
- Welch, N.L.; Zhu, M.; Hua, C.; Weller, J.; Mirhashemi, M.E.; Nguyen, T.G.; Mantena, S.; Bauer, M.R.; Shaw, B.M.; Ackerman, C.M.; et al. Multiplexed CRISPR-based microfluidic platform for clinical testing of respiratory viruses and identification of SARS-CoV-2 variants. Nat. Med. 2022, 28, 1083–1094. [Google Scholar] [CrossRef]
- Lu, S.; Tong, X.; Han, Y.; Zhang, K.; Zhang, Y.; Chen, Q.; Duan, J.; Lei, X.; Huang, M.; Qiu, Y.; et al. Fast and sensitive detection of SARS-CoV-2 RNA using suboptimal protospacer adjacent motifs for Cas12a. Nat. Biomed. Eng. 2022, 6, 286–297. [Google Scholar] [CrossRef]
- Yu, Y.; Su, G.; Zhang, W.S.; Pan, J.; Li, F.; Zhu, M.; Xu, M.; Zhu, H. Reverse transcription recombinase polymerase amplification coupled with CRISPR-Cas12a for facile and highly sensitive colorimetric SARS-CoV-2 detection. Anal. Chem. 2021, 93, 4126–4133. [Google Scholar]
- Sun, Y.; Yu, L.; Liu, C.; Ye, S.; Chen, W.; Li, D.; Huang, W. One-tube SARS-CoV-2 detection platform based on RT-RPA and CRISPR/Cas12a. J. Transl. Med. 2021, 19, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Wang, R.; Hozumi, Y.; Yin, C.; Wei, G.W. Mutations on COVID-19 diagnostic targets. Genomics 2020, 112, 5204–5213. [Google Scholar] [CrossRef] [PubMed]
- Alves, P.A.; de Oliveira, E.G.; Franco-Luiz, A.P.M.; Almeida, L.T.; Gonçalves, A.B.; Borges, I.A.; de Rocha, F.S.; Rocha, R.P.; Bezerra, M.F.; Miranda, P.; et al. Optimization and clinical validation of colorimetric reverse transcription loop-mediated isothermal amplification, a fast, highly sensitive and specific COVID-19 molecular diagnostic tool that is robust to detect SARS-CoV-2 variants of concern. Front. Microbiol. 2021, 12, 713713. [Google Scholar] [CrossRef]
- Jamwal, V.L.; Kumar, N.; Bhat, R.; Jamwal, P.S.; Singh, K.; Dogra, S.; Kulkarni, A.; Bhadra, B.; Shukla, M.R.; Saran, S.; et al. Optimization and validation of RT-LAMP assay for diagnosis of SARS-CoV-2 including the globally dominant Delta variant. Virol. J. 2021, 18, 1–14. [Google Scholar] [CrossRef]
- Lim, J.; Stavins, R.; Kindratenko, V.; Baek, J.; Wang, L.; White, K.; Kumar, J.; Valera, E.; King, W.P.; Bashir, R. Microfluidic point-of-care device for detection of early strains and B.1.1.7 variant of SARS-CoV-2 virus. Lab Chip 2022, 22, 1297–1309. [Google Scholar] [CrossRef]
- Nguyen, L.T.; Macaluso, N.C.; Pizzano, B.L.M.; Cash, M.N.; Spacek, J.; Karasek, J.; Miller, M.R.; Lednicky, J.A.; Dinglasan, R.R.; Salemi, M.; et al. A thermostable Cas12b from Brevibacillus leverages one-pot discrimination of SARS-CoV-2 variants of concern. eBioMedicine 2022, 77, 103926. [Google Scholar] [CrossRef]
- Iijima, T.; Ando, S.; Kanamori, D.; Kuroda, K.; Nomura, T.; Tisi, L.; Kilgore, P.E.; Percy, N.; Kohase, H.; Hayakawa, S.; et al. Detection of SARS-CoV-2 and the L452R spike mutation using reverse transcription loopmediated isothermal amplification plus bioluminescent assay in real-time (RT-LAMPBART). PLoS ONE 2022, 17, e0265748. [Google Scholar] [CrossRef]
- Daar, A.S.; Thorsteinsdóttir, H.; Martin, D.K.; Smith, A.C.; Nast, S.; Singer, P.A. Top ten biotechnologies for improving health in developing countries. Nat. Genet. 2002, 32, 229–232. [Google Scholar] [CrossRef]
- Wilson, M.L.; Fleming, K.A.; Kuti, M.A.; Looi, L.M.; Lago, N.; Ru, K. Access to pathology and laboratory medicine services: A crucial gap. Lancet 2018, 391, 1927–1938. [Google Scholar] [CrossRef]
- Kleinert, S.; Horton, R. Can COVID-19 help accelerate and transform the diagnostics agenda? Lancet 2021, 398, 1945–1947. [Google Scholar] [CrossRef]
- Wu, S.L.; Mertens, A.N.; Crider, Y.S.; Nguyen, A.; Pokpongkiat, N.N.; Djajadi, S.; Seth, A.; Hsiang, M.S.; Colford, J.M.; Reingold, A.; et al. Substantial underestimation of SARS-CoV-2 infection in the United States. Nat. Commun. 2020, 11, 4507. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. A Coordinated Global Research Roadmap: 2019 Novel Coronavirus; WHO: Geneva, Switzerland, 2020. [Google Scholar]
- Yadav, H.; Shah, D.; Sayed, S.; Horton, S.; Schroeder, L.F. Availability of essential diagnostics in ten low-income and middle-income countries: Results from national health facility surveys. Lancet Glob. Health 2021, 9, e1553–e1560. [Google Scholar] [CrossRef]
- Bustin, S.; Mueller, R.; Shipley, G.; Nolan, T. Covid-19 and diagnostic testing for SARS-CoV-2 by RT-qPCR—Facts and fallacies. Int. J. Mol. Sci. 2021, 22, 2459. [Google Scholar] [CrossRef] [PubMed]
- Vindeirinho, J.M.; Pinho, E.; Azevedo, N.F.; Almeida, C. SARS-CoV-2 Diagnostics Based on Nucleic Acids Amplification: From Fundamental Concepts to Applications and Beyond. Front. Cell. Infect. Microbiol. 2022, 12, 263. [Google Scholar] [CrossRef]
- Mattioli, I.A.; Hassan, A.; Oliveira, O.N.; Crespilho, F.N. On the challenges for the diagnosis of SARS-CoV-2 based on a review of current methodologies. ACS Sens. 2020, 5, 3655–3677. [Google Scholar] [CrossRef]
- Sheikh, J.A.; Malik, A.A.; Quadir, N.; Ehtesham, N.Z.; Hasnain, S.E. Learning from COVID-19 to tackle TB pandemic: From despair to hope. Lancet Reg. Health-Southeast Asia 2022, 2, 100015. [Google Scholar] [CrossRef]
- Fleming, K.A.; Horton, S.; Wilson, M.L.; Atun, R.; DeStigter, K.; Flanigan, J.; Sayed, S.; Adam, P.; Aguilar, B.; Andronikou, S.; et al. The Lancet Commission on diagnostics: Transforming access to diagnostics. Lancet 2021, 398, 1997–2050. [Google Scholar] [CrossRef]
- Cunningham, C.H.; Hennelly, C.M.; Lin, J.T.; Ubalee, R.; Boyce, R.M.; Mulogo, E.M.; Hathaway, N.; Thwai, K.L.; Phanzu, F.; Kalonji, A.; et al. A novel CRISPR-based malaria diagnostic capable of Plasmodium detection, species differentiation, and drug-resistance genotyping. EBioMedicine 2021, 68, 103415. [Google Scholar] [CrossRef]
- Lee, R.A.; de Puig, H.; Nguyen, P.Q.; Angenent-mari, N.M.; Donghia, N.M. Ultrasensitive CRISPR-based diagnostic for field-applicable detection of Plasmodium species in symptomatic and asymptomatic malaria. Proc. Natl. Acad. Sci. USA 2020, 117, 25722–25731. [Google Scholar] [CrossRef]
- World Health Organization. The Selection and Use of Essential In Vitro Diagnostics; WHO: Geneva, Switzerland, 2021; Volume 1031. [Google Scholar]


| Technique | Acronym | Temp. (°C) | Time (min) | Efficiency a |
|---|---|---|---|---|
| Loop-mediated isothermal amplification | LAMP | 60–65 | 30–60 | 109 |
| Recombinase polymerase amplification | RPA | 37–42 | 30–90 | 107–108 |
| Recombinase aided amplification | RAA | 39 | 30–90 | 107–108 |
| Nicking endonuclease amplification reaction | NEAR | 60 | 15–30 | 109 |
| Nucleic acid sequence-based amplification | NASBA | 41 | 90–120 | 106–109 |
| Exponential amplification reaction | EXPAR | 60 | <30 | 106–108 |
| Rolling circle amplification | RCA | 60 | 90 | 103 |
| Helicase dependent amplification | HDA | 37–65 | 30–120 | 106 |
| Transcription mediated amplification | TMA | 37 | 60–120 | 106 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
García-Bernalt Diego, J.; Fernández-Soto, P.; Muro, A. The Future of Point-of-Care Nucleic Acid Amplification Diagnostics after COVID-19: Time to Walk the Walk. Int. J. Mol. Sci. 2022, 23, 14110. https://doi.org/10.3390/ijms232214110
García-Bernalt Diego J, Fernández-Soto P, Muro A. The Future of Point-of-Care Nucleic Acid Amplification Diagnostics after COVID-19: Time to Walk the Walk. International Journal of Molecular Sciences. 2022; 23(22):14110. https://doi.org/10.3390/ijms232214110
Chicago/Turabian StyleGarcía-Bernalt Diego, Juan, Pedro Fernández-Soto, and Antonio Muro. 2022. "The Future of Point-of-Care Nucleic Acid Amplification Diagnostics after COVID-19: Time to Walk the Walk" International Journal of Molecular Sciences 23, no. 22: 14110. https://doi.org/10.3390/ijms232214110