
Opportunities of Digital Infrastructures for Disease Management—Exemplified on COVID-19-Related Change in Diagnosis Counts for Diabetes-Related Eye Diseases

 ,
,  , , and
, , and
Abstract
:1. Introduction
- (1)
- Technical view: The paper focuses on the ability to establish a concept and infrastructure that uses OMOP CDM across 3 different sites within MIRACUM and the MiHUBx project. We aim to answer the question whether OMOP can be successfully used by both university and non-university healthcare providers to support feasibility requests required to participate in multi-centric studies.
- (2)
- Medical view: We run a multi-centric study on the COVID-19-related change in diagnosis counts for diabetes-related eye diseases, based on the provided infrastructure components in (1). This paper aims to answer whether the number of diagnoses in Germany for diabetes mellitus type 1/2; for diabetic retinopathy and for diabetic macular edema changed in pandemic times (January 2020–December 2021) compared to the period before the SARS-CoV-2 pandemic (January 2018–December 2019).
2. Materials and Methods
2.1. Setting
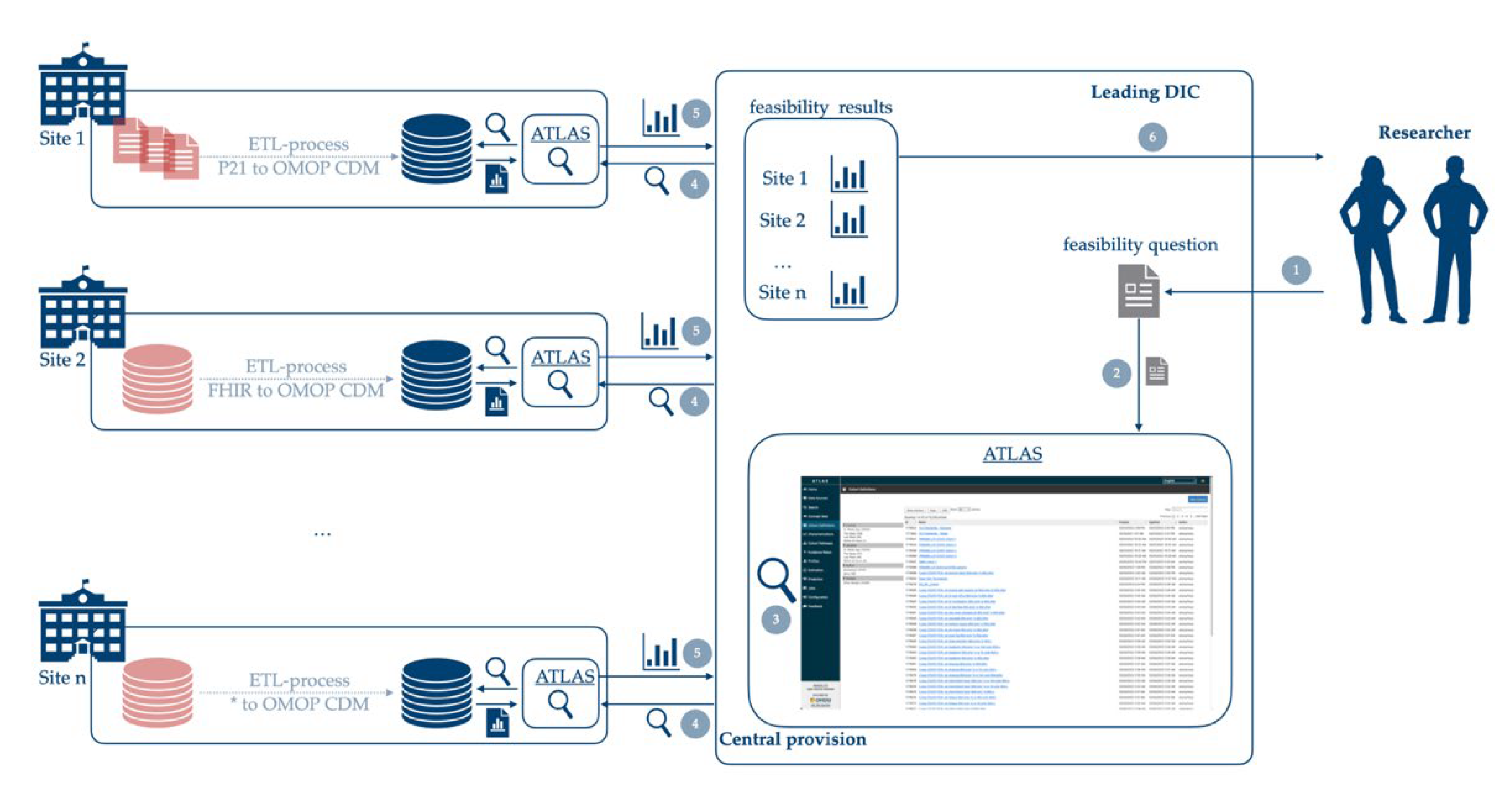
2.1.1. Infrastructural Concept
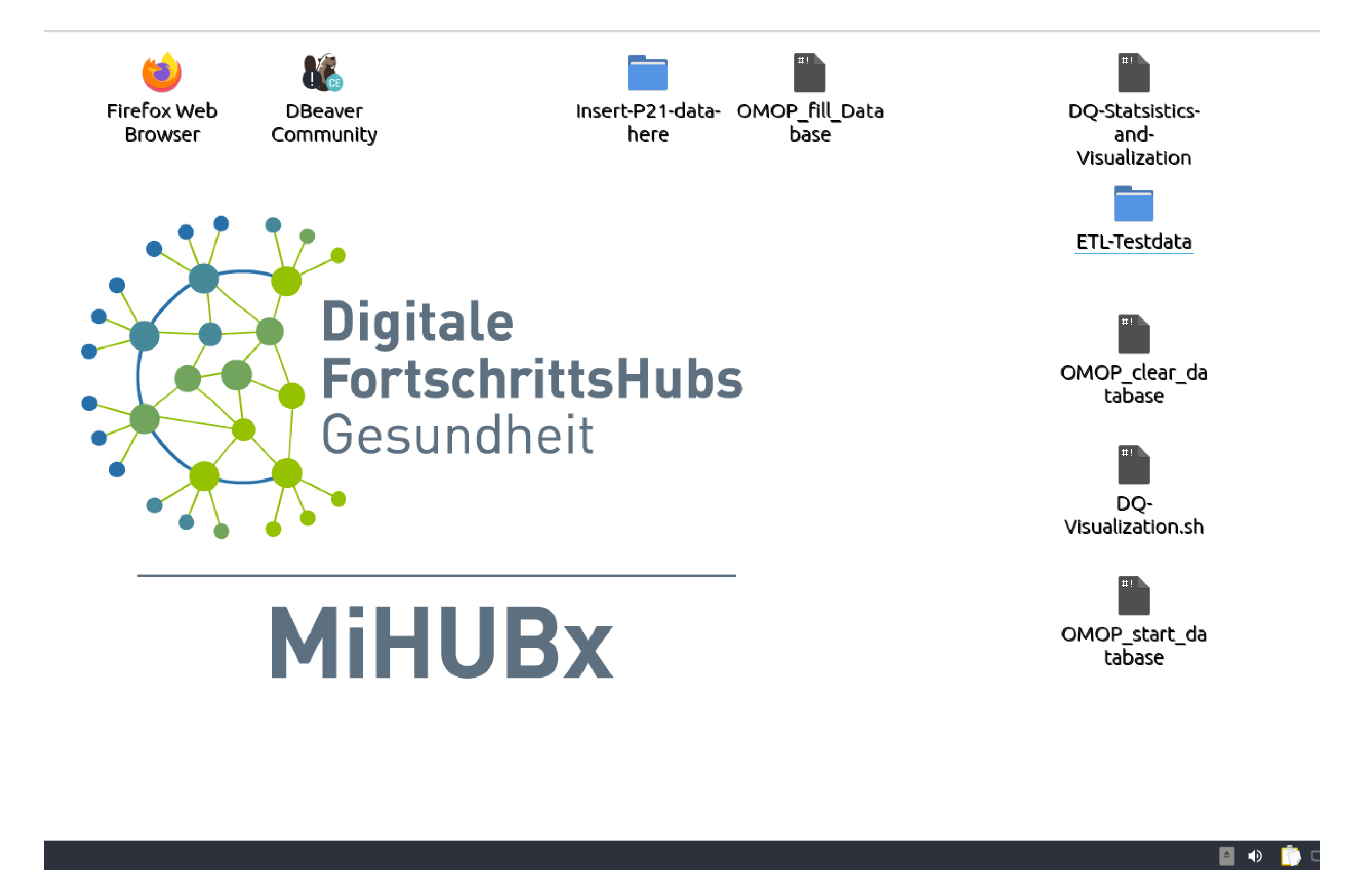
2.1.2. ETL-Processes and OHDSI Tools
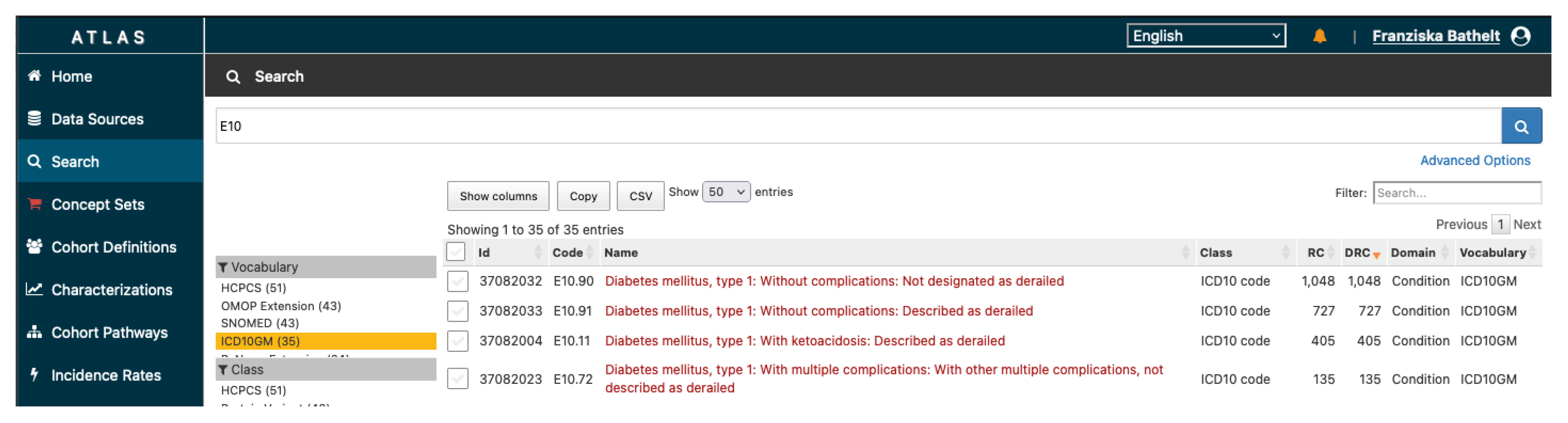
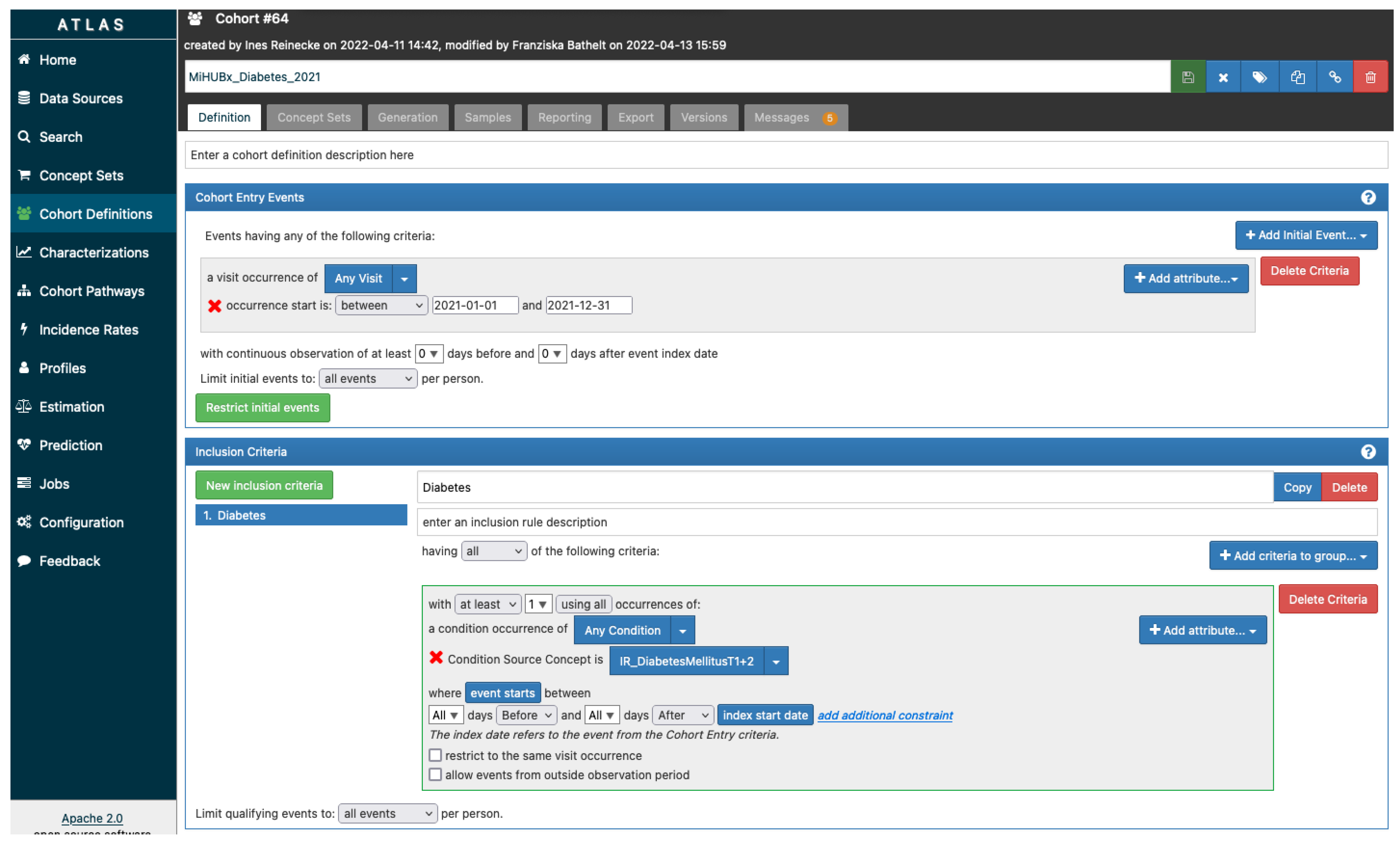
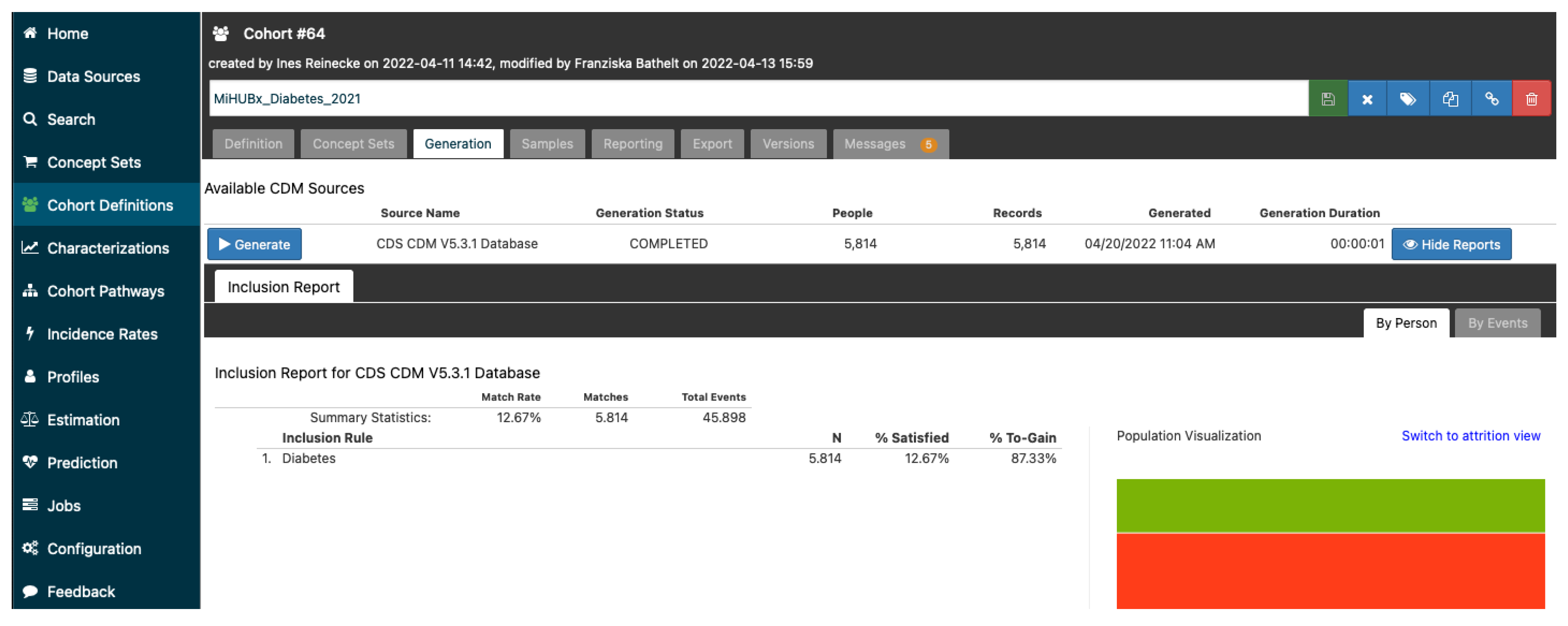
2.1.3. Technical Data Acquisition and Cohort Definition
2.2. Study Design
2.2.1. Eligibility Criteria
2.2.2. Sample Size
2.2.3. Ethics
2.3. Primary and Secondary Outcome
2.4. Data Analyses
3. Results
3.1. Technical View
3.2. Medical View
3.2.1. Feasibility Results
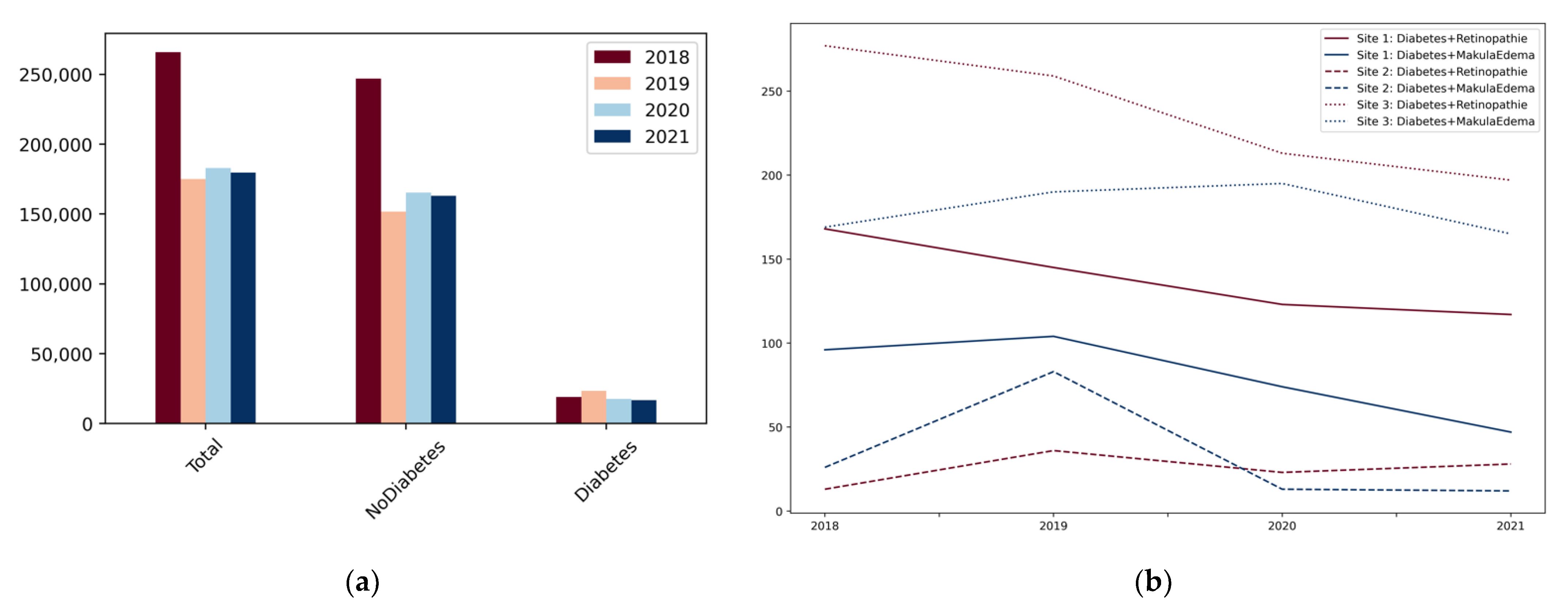
3.2.2. Change in Diagnosis Numbers
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
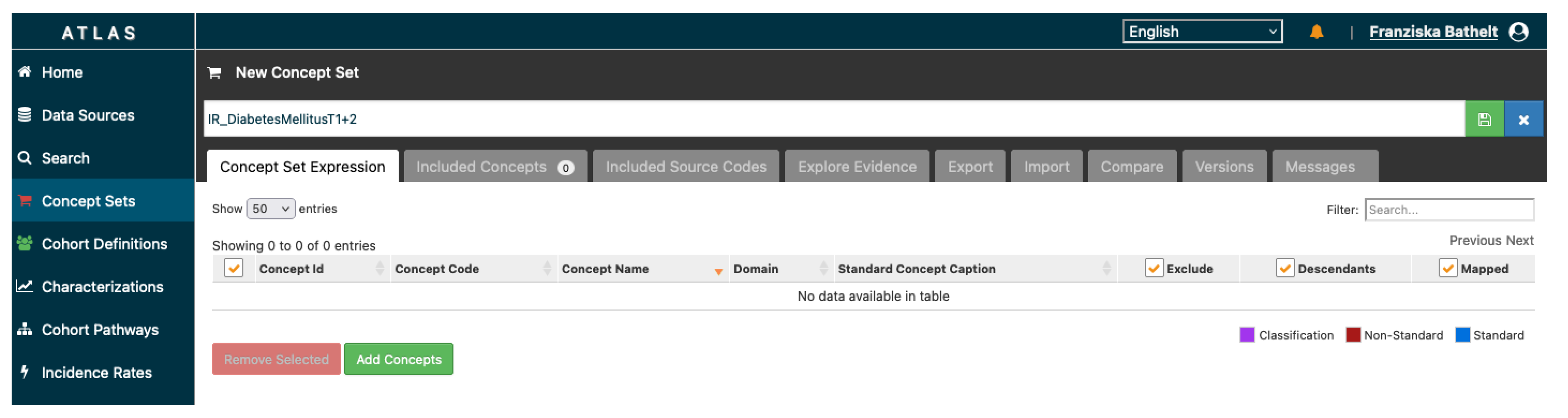
Appendix A. Cohort Definition Using OHDSI ATLAS




References
- Schneeweiss, S.; Patorno, E. Conducting Real-world Evidence Studies on the Clinical Outcomes of Diabetes Treatments. Endocr. Rev. 2021, 42, 658–690. [Google Scholar] [CrossRef] [PubMed]
- EHDEN. European Health Data & Evidence Network. Available online: https://www.ehden.eu/ (accessed on 1 April 2022).
- European Medical Agency. Data Analysis and Real World Interrogation Network (DARWIN EU). Available online: https://www.ema.europa.eu/en/about-us/how-we-work/big-data/data-analysis-real-world-interrogation-network-darwin-eu (accessed on 1 April 2022).
- Reinecke, I.; Zoch, M.; Reich, C.; Sedlmayr, M.; Bathelt, F. The Usage of OHDSI OMOP—A Scoping Review. In Studies in Health Technology and Informatics; Röhrig, R., Beißbarth, T., König, J., Ose, C., Rauch, G., Sax, U., Schreiweis, B., Sedlmayr, M., Eds.; IOS Press: Amsterdam, The Nethderlands, 2021; ISBN 978-1-64368-206-8. [Google Scholar]
- Semler, S.; Wissing, F.; Heyder, R. German Medical Informatics Initiative: A National Approach to Integrating Health Data from Patient Care and Medical Research. Methods Inf. Med. 2018, 57, e50–e56. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- HL7.org, Health Level Seven International Fast Healthcare Interoperability Resources (HL7 FHIR). Available online: https://www.hl7.org/fhir/ (accessed on 1 April 2022).
- Henke, E.; Peng, Y.; Reinecke, I.; Zoch, M.; Sedlmayr, M. Development of an ETL Process for Bulk and Incremental Load of German Patient Data into OMOP CDM Using FHIR. Available online: https://www.ohdsi.org/2021-global-symposium-showcase-44/ (accessed on 19 April 2022).
- Prokosch, H.-U.; Acker, T.; Bernarding, J.; Binder, H.; Boeker, M.; Boerries, M.; Daumke, P.; Ganslandt, T.; Hesser, J.; Höning, G.; et al. MIRACUM: Medical Informatics in Research and Care in University Medicine: A Large Data Sharing Network to Enhance Translational Research and Medical Care. Methods Inf. Med. 2018, 57, e82–e91. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Teo, Z.L.; Tham, Y.-C.; Yu, M.; Chee, M.L.; Rim, T.H.; Cheung, N.; Bikbov, M.M.; Wang, Y.X.; Tang, Y.; Lu, Y.; et al. Global Prevalence of Diabetic Retinopathy and Projection of Burden through 2045. Ophthalmology 2021, 128, 1580–1591. [Google Scholar] [CrossRef] [PubMed]
- Abdelhafiz, A.H.; Emmerton, D.; Sinclair, A.J. Diabetes in COVID-19 pandemic-prevalence, patient characteristics and adverse outcomes. Int. J. Clin. Pract. 2021, 75, e14112. [Google Scholar] [CrossRef] [PubMed]
- Lindeke-Myers, A.; Zhao, P.Y.C.; Meyer, B.I.; Liu, E.A.; Levine, D.A.; Bennett, O.M.; Ji, S.; Newman-Casey, P.A.; Rao, R.C.; Jain, N. Patient Perceptions of SARS-CoV-2 Exposure Risk and Association With Continuity of Ophthalmic Care. JAMA Ophthalmol. 2021, 139, 508. [Google Scholar] [CrossRef] [PubMed]
- Al-Dwairi, R.A.; Rwashdeh, H.; Otoom, M. The Influence of COVID-19 Lockdown in Jordan on Patients with Diabetic Retinopathy: A Case–Control Study. Ther. Clin. Risk Manag. 2021, 17, 1011–1022. [Google Scholar] [CrossRef] [PubMed]
- Chatziralli, I.; Dimitriou, E.; Kazantzis, D.; Machairoudia, G.; Theodossiadis, G.; Theodossiadis, P. Effect of COVID-19-Associated Lockdown on Patients With Diabetic Retinopathy. Cureus 2021, 13, e14831. [Google Scholar] [CrossRef] [PubMed]
- Gruhl, M.; Reinecke, I.; Sedlmayr, M. Specification and Distribution of Vocabularies Among Consortial Partners. Stud. Health Technol. Inform. 2020, 270, 1393–1394. [Google Scholar] [PubMed]
- Observational Health Data Sciences and Informatics. In The Book of OHDSI; independently published; 2021; Available online: https://ohdsi.github.io/TheBookOfOhdsi/ (accessed on 19 April 2022).
- InEK—Institut für das Entgeltsystem im Krankenhaus GmbH Data Set Description (§21 KHEntG). Available online: https://www.g-drg.de/Datenlieferung_gem._21_KHEntgG/Datenlieferung_gem._21_Abs.1_KHEntgG/Dokumente_zur_Datenlieferung/Datensatzbeschreibung (accessed on 20 April 2022).
- Lang, L. Mapping eines deutschen, klinischen Datensatzes nach OMOP Common Data Model. 2020. Available online: https://opus4.kobv.de/opus4-fau/frontdoor/index/index/docId/14831 (accessed on 19 April 2022).
- Goffrier, B.; Mandy, S.; Bätzing-Feigenbaum, J. Administrative Prävalenzen und Inzidenzen des Diabetes mellitus von 2009 bis 2015. 2017. Available online: https://www.versorgungsatlas.de/fileadmin/ziva_docs/79/VA-79-Bericht_Final.pdf (accessed on 19 April 2022).
- Manuwald, U.; Schoffer, O.; Kugler, J.; Riemenschneider, H.; Kapellen, T.M.; Kiess, W.; Rothe, U. Trends in incidence and prevalence of type 1 diabetes between 1999 and 2019 based on the Childhood Diabetes Registry of Saxony, Germany. PLOS ONE 2021, 16, e0262171. [Google Scholar] [CrossRef] [PubMed]
- Altun, F.B.; Folz, M.; Reinert, D.; Pinnau, M.; Walther, D.; Mate, S.; Reinecke, I.; Vengadeswaran, A.; Schaaf, J.; Kadioglu, D.; et al. IT support for cross-site data sharing of research inquiries. 2021. Available online: https://www.egms.de/static/en/meetings/gmds2021/21gmds070.shtml (accessed on 19 April 2022).
- Sun, J.K.; Jampol, L.M. The Diabetic Retinopathy Clinical Research Network (DRCR.net) and Its Contributions to the Treatment of Diabetic Retinopathy. Ophthalmic Res. 2019, 62, 225–230. [Google Scholar] [CrossRef]
- Maier, C.; Lang, L.; Storf, H.; Vormstein, P.; Bieber, R.; Bernarding, J.; Herrmann, T.; Haverkamp, C.; Horki, P.; Laufer, J.; et al. Towards Implementation of OMOP in a German University Hospital Consortium. Appl. Clin. Inform. 2018, 9, 54–61. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Roberts, P.K.; Vogl, W.-D.; Gerendas, B.S.; Glassman, A.R.; Bogunovic, H.; Jampol, L.M.; Schmidt-Erfurth, U.M. Quantification of Fluid Resolution and Visual Acuity Gain in Patients With Diabetic Macular Edema Using Deep Learning: A Post Hoc Analysis of a Randomized Clinical Trial. JAMA Ophthalmol. 2020, 138, 945–953. [Google Scholar] [CrossRef] [PubMed]
- Wu, J.-H.; Liu, T.Y.A.; Hsu, W.-T.; Ho, J.H.-C.; Lee, C.-C. Performance and Limitation of Machine Learning Algorithms for Diabetic Retinopathy Screening: Meta-analysis. J. Med. Internet Res. 2021, 23, e23863. [Google Scholar] [CrossRef] [PubMed]
- Voets, M.; Møllersen, K.; Bongo, L.A. Reproduction study using public data of: Development and validation of a deep learning algorithm for detection of diabetic retinopathy in retinal fundus photographs. PLoS ONE 2019, 14, e0217541. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Cohort Category | Cohort ID | Year | Diagnosis |
|---|---|---|---|
| I | Diagnosis of Diabetes type 1 or type 2 in corresponding year | ||
| 1 | 2018 | ICD-Code E10. × or E11. × | |
| 2 | 2019 | ICD-Code E10. × or E11. × | |
| 3 | 2020 | ICD-Code E10. × or E11. × | |
| 4 | 2021 | ICD-Code E10. × or E11. × | |
| II | Diagnosis of Diabetes type 1 or type 2 with Diagnosis Retinopathia diabetica in corresponding year | ||
| 5 | 2018 | (ICD-Code E10. × or E11. ×) AND (ICD-Secondary-Code H36. ×) | |
| 6 | 2019 | (ICD-Code E10. × or E11. ×) AND (ICD-Secondary-Code H36. ×) | |
| 7 | 2020 | (ICD-Code E10. × or E11. ×) AND (ICD-Secondary-Code H36. ×) | |
| 8 | 2021 | (ICD-Code E10. × or E11. ×) AND (ICD-Secondary-Code H36. ×) | |
| III | Diagnosis of Diabetes type 1 or type 2 with Diagnosis makula edema in corresponding year | ||
| 9 | 2018 | (ICD-Code E10. × or E11. ×) AND (ICD-Code H35. ×) | |
| 10 | 2019 | (ICD-Code E10. × or E11. ×) AND (ICD-Code H35. ×) | |
| 11 | 2020 | (ICD-Code E10. × or E11. ×) AND (ICD-Code H35. ×) | |
| 12 | 2021 | (ICD-Code E10. × or E11. ×) AND (ICD-Code H35. ×) | |
| IV | Other Diagnoses than defined in 1–12 in corresponding year | ||
| 13 | 2018 | NOT (ICD-Code E10. × or E11. ×) | |
| 14 | 2019 | NOT (ICD-Code E10. × or E11. ×) | |
| 15 | 2020 | NOT (ICD-Code E10. × or E11. ×) | |
| 16 | 2021 | NOT (ICD-Code E10. × or E11. ×) | |
| Cohort Category | Cohort ID | Year | Site 1 | Site 2 | Site 3 |
|---|---|---|---|---|---|
| diagnosis of diabetes type 1 or type 2 in corresponding year | |||||
| 1 | 2018 | 6.168 | 4.073 | 8.877 | |
| I | 2 | 2019 | 6.272 | 8.177 | 8.946 |
| 3 | 2020 | 6.024 | 3.670 | 7.870 | |
| 4 | 2021 | 5.814 | 3.763 | 7.123 | |
| diagnosis of diabetes type 1 or type 2 with diagnosis retinopathia diabetica in corresponding year | |||||
| 5 | 2018 | 168 | 13 | 277 | |
| II | 6 | 2019 | 145 | 36 | 259 |
| 7 | 2020 | 123 | 23 | 213 | |
| 8 | 2021 | 117 | 28 | 197 | |
| diagnosis of diabetes type 1 or type 2 with diagnosis makula edema in corresponding year | |||||
| 9 | 2018 | 96 | 26 | 169 | |
| III | 10 | 2019 | 104 | 83 | 190 |
| 11 | 2020 | 74 | 13 | 195 | |
| 12 | 2021 | 47 | 12 | 165 | |
| other diagnoses than defined in 1–12 in corresponding year | |||||
| 13 | 2018 | 42.759 | 151.239 | 52.771 | |
| IV | 14 | 2019 | 43.446 | 56.114 | 51.954 |
| 15 | 2020 | 41.223 | 78.844 | 45.213 | |
| 16 | 2021 | 40.084 | 78.566 | 43.613 | |
| Cohort Category | Site 1 | Site 2 | Site 3 | Total |
|---|---|---|---|---|
| changes between year groups for diagnosis of diabetes type 1 or 2 | ||||
| I | −4.84% | −39.32% | −15.88% | −19.40% |
| changes between year groups for diagnosis of diabetes type 1 or 2 with diagnosis retinopathia diabetica | ||||
| II | −23.32% | +4.08% | −23.51% | −21.94% |
| changes between year groups for diagnosis of diabetes type 1 or 2 with diagnosis macula edema | ||||
| III | −39.50% | −77.06% | +0.28% | −24.25% |
| changes between year groups for other diagnoses than defined in 1–12 | ||||
| IV | −4.79% | −24.12% | −15.18% | −17.59% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bathelt, F.; Reinecke, I.; Peng, Y.; Henke, E.; Weidner, J.; Bartos, M.; Gött, R.; Waltemath, D.; Engelmann, K.; Schwarz, P.E.; et al. Opportunities of Digital Infrastructures for Disease Management—Exemplified on COVID-19-Related Change in Diagnosis Counts for Diabetes-Related Eye Diseases. Nutrients 2022, 14, 2016. https://doi.org/10.3390/nu14102016
Bathelt F, Reinecke I, Peng Y, Henke E, Weidner J, Bartos M, Gött R, Waltemath D, Engelmann K, Schwarz PE, et al. Opportunities of Digital Infrastructures for Disease Management—Exemplified on COVID-19-Related Change in Diagnosis Counts for Diabetes-Related Eye Diseases. Nutrients. 2022; 14(10):2016. https://doi.org/10.3390/nu14102016
Chicago/Turabian StyleBathelt, Franziska, Ines Reinecke, Yuan Peng, Elisa Henke, Jens Weidner, Martin Bartos, Robert Gött, Dagmar Waltemath, Katrin Engelmann, Peter EH Schwarz, and et al. 2022. "Opportunities of Digital Infrastructures for Disease Management—Exemplified on COVID-19-Related Change in Diagnosis Counts for Diabetes-Related Eye Diseases" Nutrients 14, no. 10: 2016. https://doi.org/10.3390/nu14102016