
COVID-19 Peritraumatic Distress as a Function of Age and Gender in a Spanish Sample


Abstract
:1. Introduction
- (1)
- To investigate the factorial structure of the CPDI via exploratory (EFA) and confirmatory factor analysis (CFA) and validate the questionnaire in a Spanish sample;
- (2)
- To quantify the prevalence and severity of COVID-related psychological distress in the Spanish population; and
- (3)
- To analyze age and gender differences in relation with the factorial structure of the questionnaire.
2. Materials and Methods
2.1. Participants
2.2. Instruments
2.3. Procedure
2.4. Ethical Considerations
2.5. Data Analysis
3. Results
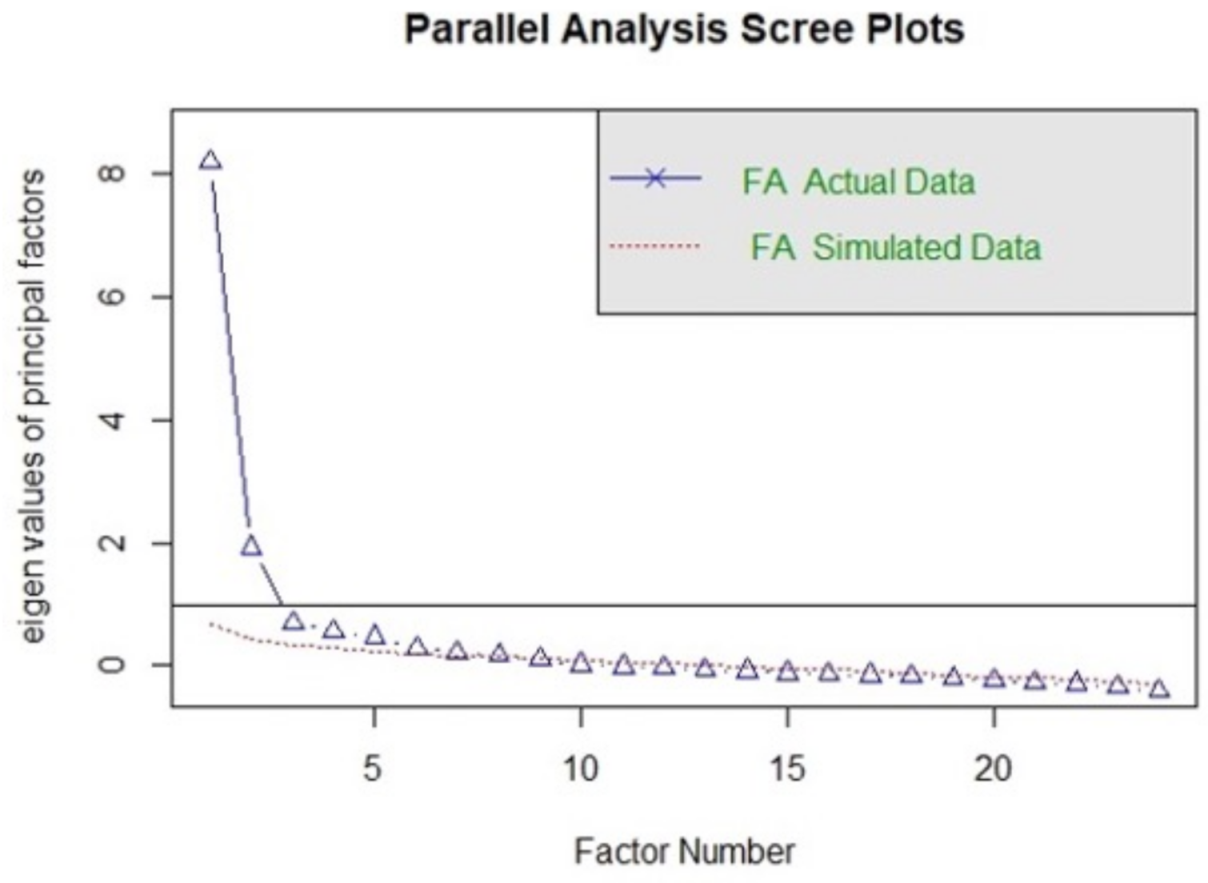
3.1. Exploratory Factor Analysis
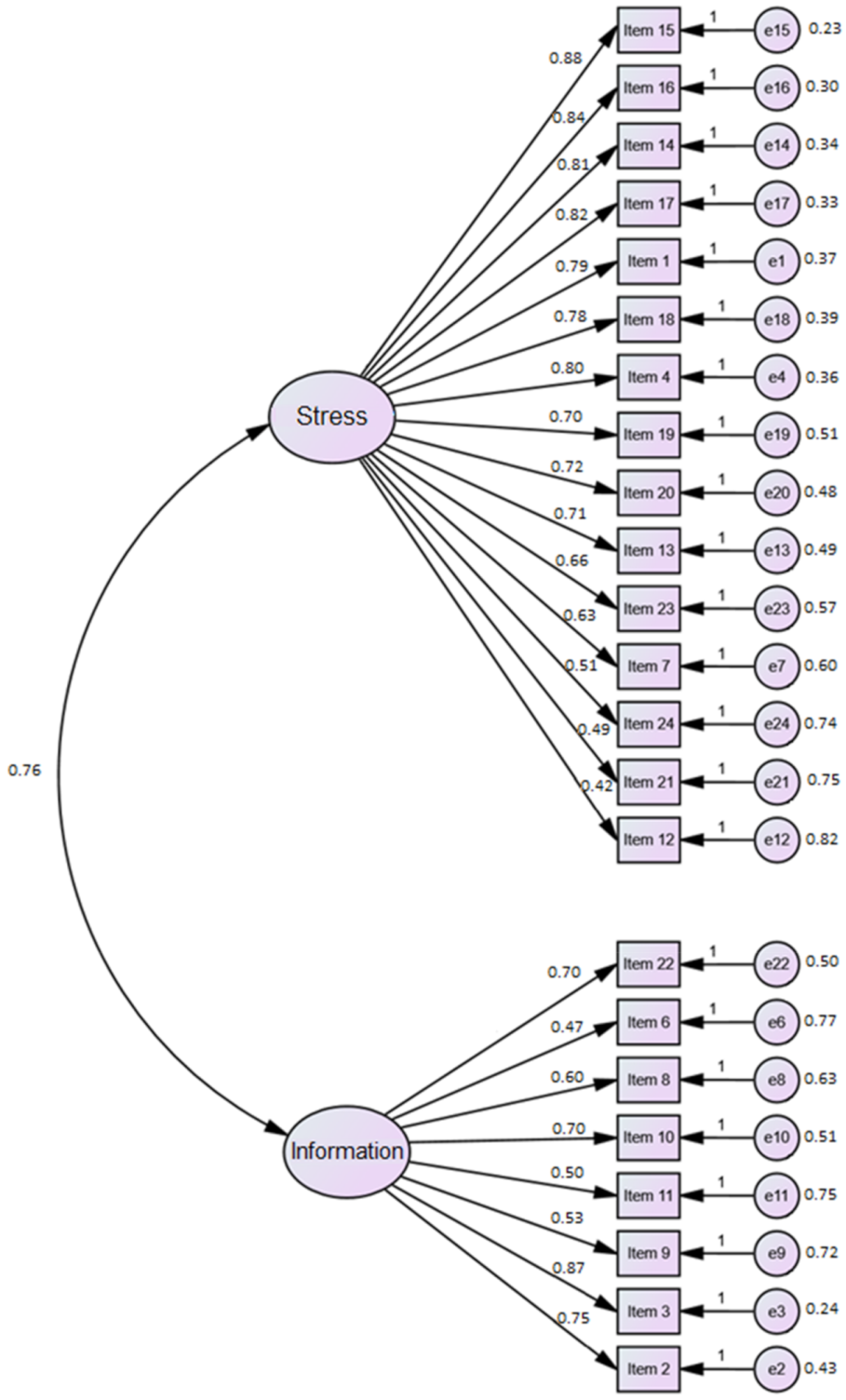
3.2. Confirmatory Factor Analysis
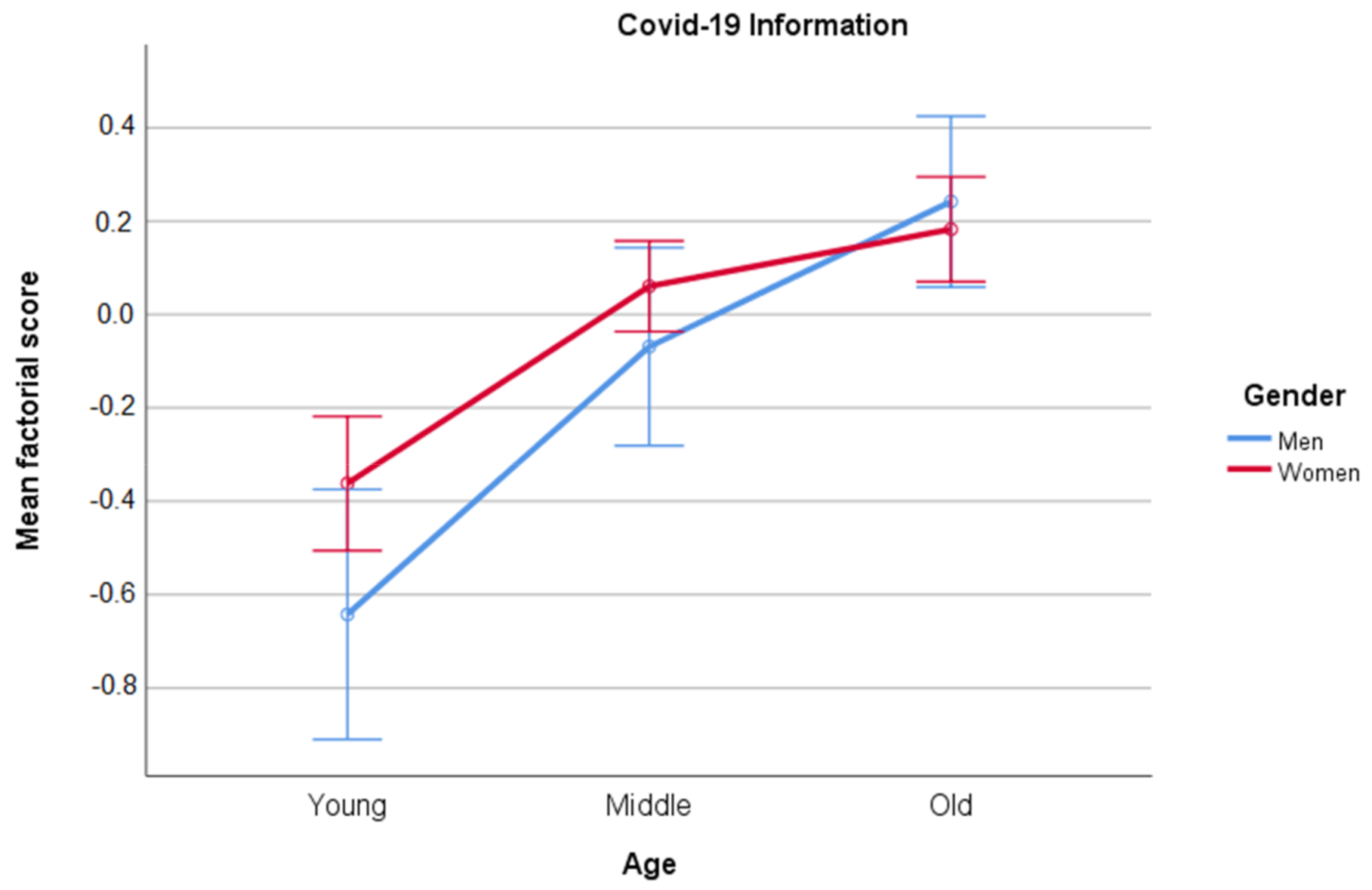
3.3. Gender and Age Group Differences on Psychological Distress
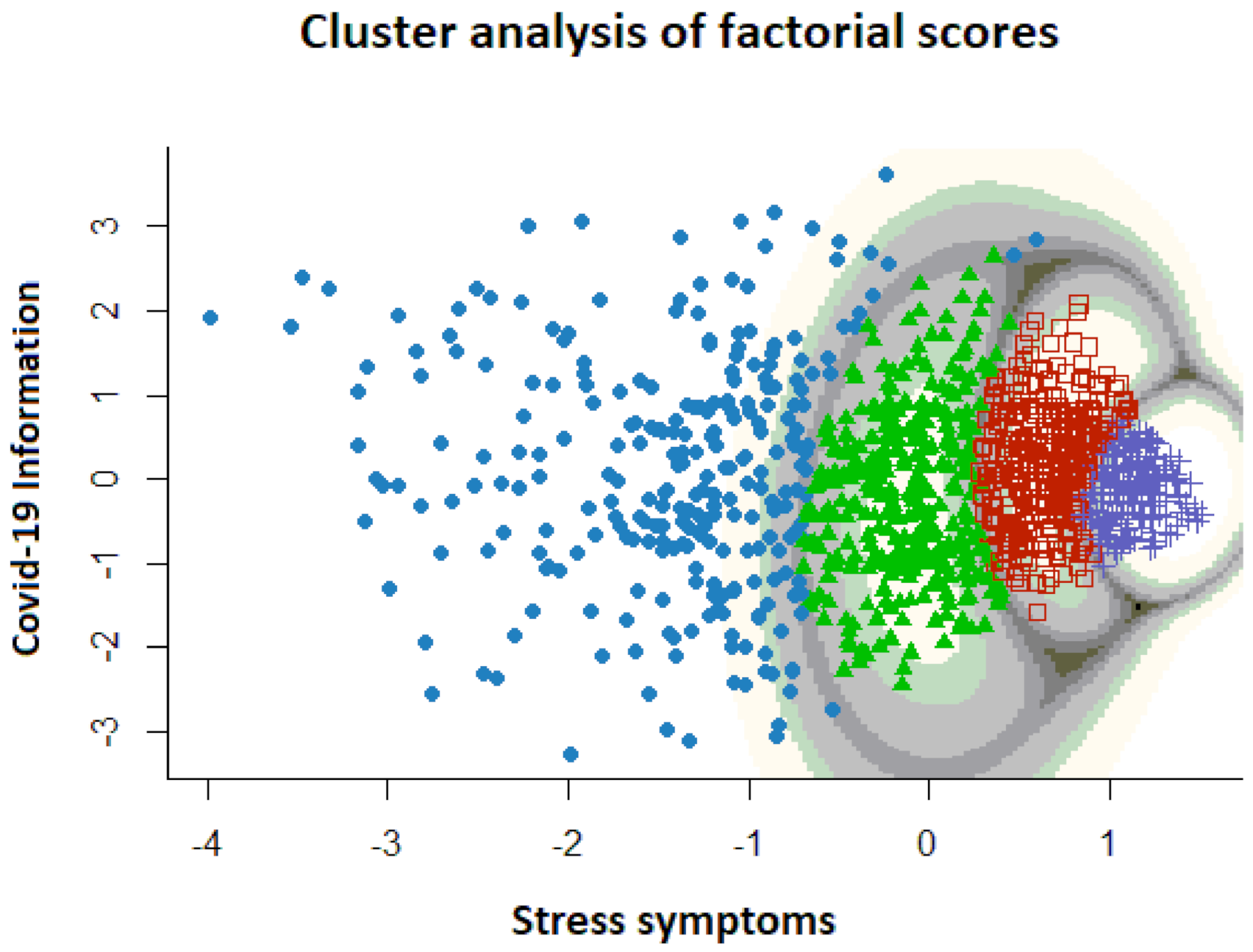
3.4. Clustering
4. Discussion
5. Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Who′Director-General’s Opening Remarks at the Mission Briefing on COVID-19. Available online: https://www.who.int/director-general/speeches/detail/who-director-general-s-opening-remarks-at-the-media-briefing-on-Covid-19---11-march-2020 (accessed on 13 January 2021).
- BOE. Boletín Oficial del Estado (BOE). Real Decreto 463/2020, de 14 de Marzo, por el que se Declara el Estado de Alarma Para la Gestión de la Situación de Crisis Sanitaria Ocasionada por el COVI-19. 2020. Available online: http://www.boe.es/eli/es/rd/2020/o3/14/463 (accessed on 16 January 2021).
- World Health Organization. WHO Coronavirus Disease (COVID-19) Dashboard. 2020. Available online: https://Covid19.who.int/table (accessed on 13 January 2021).
- Chew, Q.H.; Wei, K.C.; Vasoo, S.; Chua, H.C.; Sim, K. Narrative synthesis of psychological and coping responses towards emerging infectious disease outbreak in the general population: Practical considerations for the COVID-19 pandemic. Singap. Med. J. 2020, 61, 350–356. [Google Scholar] [CrossRef]
- Torales, J.; O’Higgins, M.; Castaldelli-Maia, J.M.; Ventriglio, A. The outbreak of coronavirus and its impact on global mental health. Int. J. Soc. Psychiatry 2020, 66, 317–320. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brooks, S.K.; Webster, R.K.; Smith, L.E.; Woodland, L.; Wessely, S.; Greenberg, N.; Rubin, G.J. The psychological impact of quarantine and how to reduce it: Rapid review of the evidence. Lancet 2020, 395, 912–920. [Google Scholar] [CrossRef] [Green Version]
- Rajkumar, R.P. Covid-19 and mental health: A review of the existing literature. Asian J. Psychiatry 2020, 52, 102066. [Google Scholar] [CrossRef] [PubMed]
- Wang, C.; Pan, R.; Wan, X.; Tan, Y.; Xu, L.; Ho, C.; Ho, R.C. Immediate psychological responses and associated factors during the Initial Stage of the 2019 coronavirus disease (COVID-19) epidemic among the general population in China. Int. J. Environ. Res. Public Health 2020, 17, 1729. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Qiu, J.; Shen, B.; Zhao, M.; Wang, Z.; Xie, B.; Xu, Y. A nationwide survey of psychological distress among Chinese people in the COVID-19 epidemic: Implications and policy recommendations. Gen. Psychiatry 2020, 33, e100213. [Google Scholar] [CrossRef] [Green Version]
- Salary, N.; Hosseinian-Far, A.; Jalali, R.; Vaisu-Raygani, A.; Rasoulpur, S.; Mohammadi, M.; Rasoulpoor, S.; Khaledi-Paveh, B. Prevalence of stress, anxiety, depression among the general population during the COVID-19 pandemic: A systematic review and meta-analysis. Glob. Health 2020, 16, 57. [Google Scholar] [CrossRef]
- Santabárbara, J.; Lasheras, I.; Lipnicki, D.M.; Bueno-Notivol, J.; Pérez-Moreno, M.; López-Antón, R.; De la Cámara, C.; Lobo, A.; Gracia-García, P. Prevalence of anxiety in the COVID-19 pandemic: An updated meta-analysis of community-based studies. Prog. Neuropsychopharmacol. Biol. Psychiatry 2020, 109, 110207. [Google Scholar] [CrossRef]
- Bueno-Notivol, J.; Gracia-García, P.; Olaya, B.; Lasheras, D.; López-Antónc, R. Prevalence of depression during the COVID-19 outbreak: A meta-analysis of community-based studies. Int. J. Clin. Health Psychol. 2021, 1. [Google Scholar] [CrossRef]
- Rodríguez-Rey, R.; Garrido-Hernansaiz, H.; Collado, S. Psychological impact and associated factors during the initial stage of the coronavirus (COVID-19) pandemic among the general population in Spain. Front. Psychol. 2020, 11, 1540. [Google Scholar] [CrossRef]
- Ozamiz-Etxebarria, N.; Idoiaga Mondragon, N.; Dosil Santamaría, M.; Picaza Gorrotxategi, M. Psychological symptoms during the two of stages of lockdown in response to the COVID-19 outbreak: An investigation in a sample of citizens in northern Spain. Front. Psychol. 2020, 11, 1491. [Google Scholar] [CrossRef]
- Gómez-Salgado, J.; Andrés-Villas, M.; Domínguez-Salas, S.; Díaz-Milanés, D.; Ruiz-Frutos, C. Related Health Factors of Psychological Distres During the COVID-19 Pandemic in Spain. Int. J. Environ. Res. Public Health 2020, 17, 3947. [Google Scholar] [CrossRef] [PubMed]
- Talevi, D.; Pacitti, F.; Socci, V.; Renzi, G.; Alessandrini, M.C.; Trabbi, E.; Rossi, R. The COVID-19 outbreak: Impact on mental health and intervention strategies. J. Psychopathol. 2020, 26, 162–168. [Google Scholar] [CrossRef]
- Ahorsu, D.K.; Lin, C.-Y.; Imani, V.; Saffari, M.; Griffiths, M.D.; Pakpourt, A.H. The fear of COVID-19 scale: Development and initial validation. Int. J. Ment. Health Addict. 2020. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, S.A. Coronavirus Anxiety Scale: A brief mental health screener for COVID-19 related anxiety. Death Stud. 2020, 44, 393–401. [Google Scholar] [CrossRef] [PubMed]
- Arpaci, I.; Karatas, K.; Baloglu, M. The development and initial test for the psychometric properties of the COVID-19 Phobia Scale (C19P-S). Pers. Individ. Dif. 2020, 11, 164. [Google Scholar] [CrossRef]
- Chandu, V.C.; Marella, Y.; Panga, G.S.; Pachava, S.; Vadapalli, V. Measuring the impact of COVIDCOVID-19 on mental health: A scoping review of the existing scales. Indian J. Psychol. Med. 2020, 42, 421–427. [Google Scholar] [CrossRef] [PubMed]
- Ramasubramanian, V.; Mohandoss, A.A.; Rajendhiran, G.; Pandian, P.R.S.; Ramasubramanian, C. Statewide survey of psychological distress among people of Tamil Nadu in the COVID-19 pandemic. Indian J. Psychol. Med. 2020, 42, 368–373. [Google Scholar] [CrossRef]
- Jahanshahi, A.A.; Dinami, M.M.; Madavani, A.N.; Li, J.; Zhan, S.X. The distress during the Covid-19 pandemic—More distressed than the Chinese and with different predictors. Brain Behav. Immun. 2020, 87, 124–125. [Google Scholar] [CrossRef]
- Liu, S.; Heinz, A. Cross-Cultural Validity of Psychological Distress Measurement during the Coronavirus Pandemic. Pharmacopsychiatry 2020. [Google Scholar] [CrossRef]
- Constantiny, A.; Mazzotti, E. Italian validation of Covid-19 Peritraumatic Distress Index and preliminary data in a sample of general population. Riv. Psichiatr. 2020, 55, 145–151. [Google Scholar] [CrossRef]
- Bonati, M.; Campi, R.; Zanetti, M.; Cartabia, M.; Scarpellini, F.; Clavenna, A.; Segre, G. Psychological distress among Italians during the 2019 coronavirus disease (COVID-19) quarantine. BMC Psychiatry 2021, 21. [Google Scholar] [CrossRef] [PubMed]
- Zhang, S.X.; Wang, Y.; Jahanshahi, A.A.; Li, J.; Schmitt, V.G.H. Early evidence and predictors of mental distress of adults one month in the COVID-19 epidemic in Brazil. J. Psychosom. Res. 2021, 142, 110366. [Google Scholar] [CrossRef] [PubMed]
- Marzo, R.R.; Singh, A.; Mukti, R.F. A survey of psychological distress among Bangladeshi people during the COVID-19 pandemic. Clin. Epidemiol. Glob. Health 2021, 10, 100693. [Google Scholar] [CrossRef] [PubMed]
- Megalakaki, O.; Kokou-Kpolou, C.K.; Vaudé, J.; Park, S.; Iorfa, S.K.; Cénat, J.M.; Derivois, D. Does peritraumatic distress predict PTSD, depression and anxiety symptoms during and after COVID-19 lockdown in France? A prospective longitudinal study. J. Psychiatr. Res. 2021, 137, 81–88. [Google Scholar] [CrossRef] [PubMed]
- Shrestha, D.B.; Thapa, B.B.; Katuwal, N.; Shrestha, B.; Pant, C.; Basnet, B.; Mandal, P.; Gurung, A.; Agrawal, A.; Runiyar, R. Psychological distress in Nepalese residents during COVID-19 pandemic: A community level survey. BMC Psychiatry 2020, 20, 491. [Google Scholar] [CrossRef]
- Abad, A.; da Silva, J.A.; de Paiva Teixeira, L.E.P.; Antonelli-Ponti, M.; Bastos, S.; Mármora, C.H.C.; Campos, L.A.M.; Paiva, S.; de Freitas, R.L.; da Silva, J.A. Evaluation of Fear and Peritraumatic Distress during COVID-19 Pandemic in Brazil. Adv. Infect. Dis. 2020, 10, 184–194. [Google Scholar] [CrossRef]
- Weiss, D.S.; Marmar, C.R. The Impact of Event Scale—Revised. In Assessing Psychological Trauma and PTSD; Wilson, J.P., Keane, T.M., Eds.; Guilford Press: New York, NY, USA, 1997; pp. 399–411. [Google Scholar]
- Landi, G.; Pakenham, K.I.; Boccolini, G.; Tossani, E. Health anxiety and mental health outcome during Covid-19 lockdown in Italy: The mediating and moderating roles of psychological flexibility. Front. Psychol. 2020, 11, 2195. [Google Scholar] [CrossRef]
- Qualtrics. Qualtrics Software (Version 37,892) [Computer Software]; Qualtrics Research Suite: Provo, UT, USA, 2013. [Google Scholar]
- Ley Orgánica 3/2018, de 5 de Diciembre, de Protección de Datos Personales y Garantía de los Derechos Digitales. BOE-A-2018-16673. Available online: https://www.boe.es/eli/es/lo/2018/12/05/3/con (accessed on 13 January 2021).
- Rosseel, Y. Lavaan: Latent Variable Analysis 2018. Available online: https://CRAN.R-project.org/package=lavaan (accessed on 11 January 2021).
- Horn, J.L. A rationale and test for the number of factors in factor analysis. Psychometrika 1965, 30, 179–185. [Google Scholar] [CrossRef]
- Scrucca, L.; Fop, M.; Murphy, T.B.; Raftery, A.E. Mclust 5: Clustering, classification and density estimation using Gaussian finite mixture models. R J. 2016, 8, 205–233. [Google Scholar] [CrossRef] [Green Version]
- Mazza, C.; Ricci, E.; Biondi, S.; Colasanti, M.; Ferracuti, S.; Napoli, C.; Roma, P. A Nationwide Survey of Psychological Distress among Italian People during the COVID-19 Pandemic: Immediate Psychological Responses and Associated Factor. Int. J. Environ. Res. Public. Health 2020, 17, 3165. [Google Scholar] [CrossRef] [PubMed]
- Bonanad, C.; García-Blas, S.; Tarazona-Santabalbina, F.; Sanchis, J.; Bertomeu-González, V.; Fácila, L.; Ariza, A.; Núñez, J.; Cordero, A. The effect of age on mortality in Patiens with COVID-19. A Meta-Analysis with 611.583 subjects. J. Am. Med. Dir. Assoc. 2020, 21, 915–918. [Google Scholar] [CrossRef] [PubMed]
- García-Fernández, L.; Romero-Ferreiro, V.; López-Roldán, P.D.; Padilla, S.; Rodriguez-Jimenez, R. Mental Health in Elderly Spanish People in Times of COVID-19 Outbreak. Am. J. Geriatr. Psychiatry 2020, 28, 1040–1045. [Google Scholar] [CrossRef]
- Nwachukwu, I.; Nkire, N.; Shalaby, R.; Hrabok, M.; Vuong, W.; Gusnowski, A.; Surood, S.; Urichuk, L.; Greenshaw, A.J.; Agyapong, V.I.O. COVID-19 Pandemic: Age-Related Differences in Measures of Stress, Anxiety and Depression in Canada. Int. J. Environ. Res. Public Health 2020, 17, 6366. [Google Scholar] [CrossRef]
- Knepple Carney, A.; Graf, A.; Hudson, G.; Wilson, E. Age Moderates Perceived COVID-19 Disruption on Well-Being. Gerontologist 2021, 61, 30–35. [Google Scholar] [CrossRef]
- López, J.; Perez-Rojo, G.; Noriega, C.; Carretero, I.; Velasco, C.; Martínez-Huertas, J.; López-Frutos, P.; Galarraga, L. Psychological well-being among older adults during the COVID-19 outbreak: A comparative study of the young–old and the old–old adults. Int. Psychogeriatr. 2020, 32, 1365–1370. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Level | n (%) | M (SD) |
|---|---|---|---|
| Gender | Men | 241 (22%) | |
| Women | 853 (78%) | ||
| Age | Total | 52.55 (14.19) | |
| 18 to 39 years | 228 (20.8%) | 31.69 (5.87) | |
| 40 to 59 years | 468 (42.8%) | 49.82 (5.88) | |
| ≥60 years | 398 (36.4%) | 67.04 (5.22) | |
| Education 1 | Total | 5.2 (1.18) | |
| University degree or higher | 658 (60.1%) | ||
| High school diploma | 181 (16.5%) | ||
| Vocational training | 134 (12.2%) | ||
| Senior high school | 62 (5.7%) | ||
| Junior high school or less | 59 (59%) | ||
| Employment status 2 | Total | 1.46 (0.81) | |
| Employed | 747 (68.3%) | ||
| Unemployed or housekeeper | 66 (6%) | ||
| Student | 22 (2%) | ||
| Retired | 259 (23.7%) | ||
| Place of residence | Autonomous Community of Madrid | 538 (49.2%) | |
| Rest of Autonomous Communities | 379 (34.6%) | ||
| N/A | 177 (16.2) | ||
| Professional occupation 3, 4 | Armed forces occupations | 6 (0.8%) | |
| Clerical support workers | 169 (22.6) | ||
| Craft and related trades workers | 7 (0.9%) | ||
| Elementary occupations | 32 (4.3%) | ||
| Managers | 13 (1.7%) | ||
| Professionals | 317 (42.4%) | ||
| Service and sales workers | 76 (10.1%) | ||
| Technicians | 87 (11.6%) |
| n (%) | M (SD) | |
|---|---|---|
| Total Sample | 1094 | 26.15 (15.28) |
| Gender | ||
| Men | 241 (22%) | 19.75 (12.37) |
| Women | 853 (77%) | 27.95 (15.53) |
| Age groups | ||
| Young Adults | 228 (20.8) | 26.46 (15.69) |
| Middle-aged Adults | 468 (42.7) | 29.01 (16.23) |
| Older Adults | 398 (36.3) | 22.61 (13.06) |
| Range of COVID-19 distress | ||
| No Distress | 636 (58.13) | 15.59 (5.93) |
| Mild to moderate | 279 (25.50) | 33.11 (4.29) |
| Severe | 179 (16.36) | 53.84 (9.50) |
| Items | Factor Loading | Communality | |
|---|---|---|---|
| 1 | 2 | ||
| 15. Due to feelings of anxiety, my reactions are becoming sluggish | 0.811 | 0.681 | |
| 16. I find it hard to concentrate | 0.772 | 0.602 | |
| 14. I feel tired and sometimes even exhausted | 0.770 | 0.593 | |
| 17. I find it hard to make any decisions | 0.727 | 0.568 | |
| 1. Compared to usual, I feel more nervous and anxious | 0.703 | 0.542 | |
| 18. During this COVID-19 period, I often feel dizzy or have back pain and chest distress | 0.715 | 0.519 | |
| 13. I am more irritable and have frequent conflicts with my family | 0.701 | 0.495 | |
| 4. I feel empty and helpless no matter what I do | 0.657 | 0.308 | 0.527 |
| 19. During this COVID-19 period, I often feel stomach pain, bloating, and other stomach discomfort | 0.612 | 0.380 | |
| 20. I feel uncomfortable when communicating with others | 0.634 | 0.416 | |
| 23. I lost my appetite | 0.590 | 0.363 | |
| 7. I am losing faith in the people around me | 0.437 | 0.241 | |
| 24. I have constipation or frequent urination | 0.422 | 0.178 | |
| 21. Recently, I rarely talk to my family | 0.366 | 0.138 | |
| 22. I cannot sleep well. I always dream about myself or my family being infected by COVID-19 | 0.350 | 0.385 | 0.271 |
| 12. I avoid watching COVID-19 news, since I am scared to do so | 0.332 | 0.113 | |
| 6. I feel helpless and angry about people around me, governors, and media | 0.331 | 0.338 | 0.244 |
| 8. I collect information about COVID-19 all day. Even if it’s not necessary, I can’t stop myself | 0.720 | 0.518 | |
| 11. I am constantly sharing news about COVID-19 (mostly negative news) | 0.654 | 0.439 | |
| 3. I can’t stop myself from imagining myself or my family being infected and feel terrified and anxious about it | 0.315 | 0.632 | 0.498 |
| 2. I feel insecure and bought a lot of masks, medications, sanitizer, gloves and/or other home supplies | 0.614 | 0.413 | |
| 9. I will believe the COVID-19 information from all sources without any evaluation | 0.612 | 0.375 | |
| 10. I would rather believe in negative news about COVID-19 and be skeptical about the good news | 0.552 | 0.390 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jiménez, M.P.; Rieker, J.A.; Reales, J.M.; Ballesteros, S. COVID-19 Peritraumatic Distress as a Function of Age and Gender in a Spanish Sample. Int. J. Environ. Res. Public Health 2021, 18, 5253. https://doi.org/10.3390/ijerph18105253
Jiménez MP, Rieker JA, Reales JM, Ballesteros S. COVID-19 Peritraumatic Distress as a Function of Age and Gender in a Spanish Sample. International Journal of Environmental Research and Public Health. 2021; 18(10):5253. https://doi.org/10.3390/ijerph18105253
Chicago/Turabian StyleJiménez, María Pilar, Jennifer A. Rieker, José Manuel Reales, and Soledad Ballesteros. 2021. "COVID-19 Peritraumatic Distress as a Function of Age and Gender in a Spanish Sample" International Journal of Environmental Research and Public Health 18, no. 10: 5253. https://doi.org/10.3390/ijerph18105253