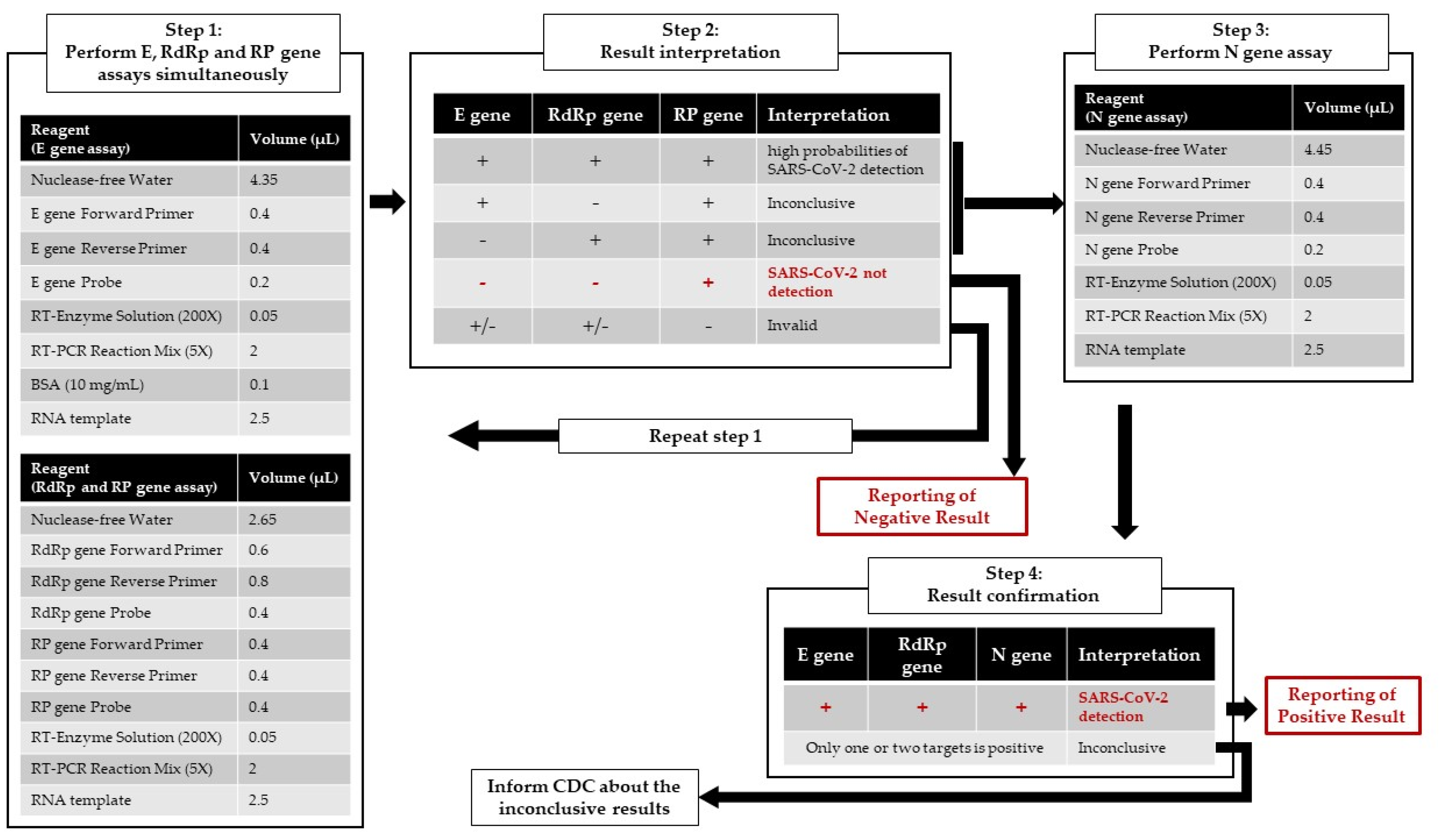
Optimization of the CDC Protocol of Molecular Diagnosis of COVID-19 for Timely Diagnosis

 ,
,
Abstract
:
Author Contributions
Funding
Conflicts of Interest
References
- Zhu, N.; Zhang, D.; Wang, W.; Li, X.; Yang, B.; Song, J.; Zhao, X.; Huang, B.; Shi, W.; Lu, R.; et al. A Novel Coronavirus from Patients with Pneumonia in China, 2019. N. Engl. J. Med. 2020, 382, 727–733. [Google Scholar] [CrossRef] [PubMed]
- Gorbalenya, A.E.; Baker, S.C.; Baric, R.S.; de Groot, R.J.; Drosten, C.; Gulyaeva, A.A.; Haagmans, B.L.; Lauber, C.; Leontovich, A.M.; Neuman, B.W.; et al. The species Severe acute respiratory syndrome-related coronavirus: Classifying 2019-nCoV and naming it SARS-CoV-2. Nat. Microbiol. 2020, 5, 536–544. [Google Scholar] [CrossRef] [Green Version]
- WHO. Coronavirus Disease 2019 (COVID-19) Situation Report—53; WHO: Geneva, Switzerland, 2020. [Google Scholar]
- WHO. Coronavirus Disease 2019 (COVID-19) Situation Report—10; WHO: Geneva, Switzerland, 2020. [Google Scholar]
- Diagnostic Detection of Wuhan Coronavirus 2019 by Real-Time RT-PCR. Available online: https://www.who.int/docs/default-source/coronaviruse/wuhan-virus-assay-v1991527e5122341d99287a1b17c111902.pdf (accessed on 10 April 2020).
- 2019-Novel Coronavirus (2019-nCoV) Real-Time rRT-PCR Panel Primers and Probes. Available online: https://www.cdc.gov/coronavirus/2019-ncov/lab/rt-pcr-panel-primer-probes.html (accessed on 10 April 2020).
- Taiwan CDC. 2019-nCoV Virus Nucleic Acid Test. Available online: https://www.cdc.gov.tw/File/Get/BIHQoIEBjlFZ5tsjfij2Gg (accessed on 10 April 2020).
- Mahase, E. China coronavirus: WHO declares international emergency as death toll exceeds 200. BMJ 2020, 368, m408. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nagai, M.; Yoshida, A.; Sato, N. Additive effects of bovine serum albumin, dithiothreitol, and glycerol on PCR. Biochem. Mol. Biol. Int. 1998, 44, 157–163. [Google Scholar] [CrossRef] [PubMed]
- Nitsche, A.; Steuer, N.; Schmidt, C.A.; Landt, O.; Siegert, W. Different real-time PCR formats compared for the quantitative detection of human cytomegalovirus DNA. Clin. Chem. 1999, 45, 1932–1937. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Plante, D.; Bélanger, G.; Leblanc, D.; Ward, P.; Houde, A.; Trottier, Y.L. The use of bovine serum albumin to improve the RT-qPCR detection of foodborne viruses rinsed from vegetable surfaces. Lett. Appl. Microbiol. 2011, 52, 239–244. [Google Scholar] [CrossRef] [PubMed]
- Yang, T.; Wang, Y.C.; Shen, C.F.; Cheng, C.M. Point-of-Care RNA-Based Diagnostic Device for COVID-19. Diagnostics (Basel) 2020, 10, 165. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Decaro, N.; Lorusso, A. Novel human coronavirus (SARS-CoV-2): A lesson from animal coronaviruses. Vet. Microbiol. 2020, 244, 108693. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Description | Oligonucleotide Sequence (5′ > 3′) | Reference |
|---|---|---|
| E gene F’ | ACAGGTACGTTAATAGTTAATAGCGT | [5] |
| E gene R’ | ATATTGCAGCAGTACGCACACA | |
| E gene probe | FAM-ACACTAGCCATCCTTACTGCGCTTCG-BBQ | |
| RdRp gene F’ | GTGARATGGTCATGTGTGGCGG | [5] |
| RdRp gene R’ | CARATGTTAAASACACTATTAGCATA | |
| RdRp gene probe | FAM-CAGGTGGAACCTCATCAGGAGATGC-BBQ | |
| N gene F’ | CACATTGGCACCCGCAATC | [5] |
| N gene R’ | GAGGAACGAGAAGAGGCTTG | |
| N gene probe | FAM-ACTTCCTCAAGGAACAACATTGCCA-BBQ | |
| RP gene F’ | AGATTTGGACCTGCGAGCG | [6] |
| RP gene R’ | GAGCGGCTGTCTCCACAAGT | |
| RP gene probe | HEX-TTCTGACCTGAAGGCTCTGCGCG-BHQ |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chen, C.-J.; Hsieh, L.-L.; Lin, S.-K.; Wang, C.-F.; Huang, Y.-H.; Lin, S.-Y.; Lu, P.-L. Optimization of the CDC Protocol of Molecular Diagnosis of COVID-19 for Timely Diagnosis. Diagnostics 2020, 10, 333. https://doi.org/10.3390/diagnostics10050333
Chen C-J, Hsieh L-L, Lin S-K, Wang C-F, Huang Y-H, Lin S-Y, Lu P-L. Optimization of the CDC Protocol of Molecular Diagnosis of COVID-19 for Timely Diagnosis. Diagnostics. 2020; 10(5):333. https://doi.org/10.3390/diagnostics10050333
Chicago/Turabian StyleChen, Chao-Ju, Li-Ling Hsieh, Shu-Kai Lin, Chu-Feng Wang, Yi-Hui Huang, Shang-Yi Lin, and Po-Liang Lu. 2020. "Optimization of the CDC Protocol of Molecular Diagnosis of COVID-19 for Timely Diagnosis" Diagnostics 10, no. 5: 333. https://doi.org/10.3390/diagnostics10050333