COVID-19 Assessment with Bedside Lung Ultrasound in a Population of Intensive Care Patients Treated with Mechanical Ventilation and ECMO

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
Statistics
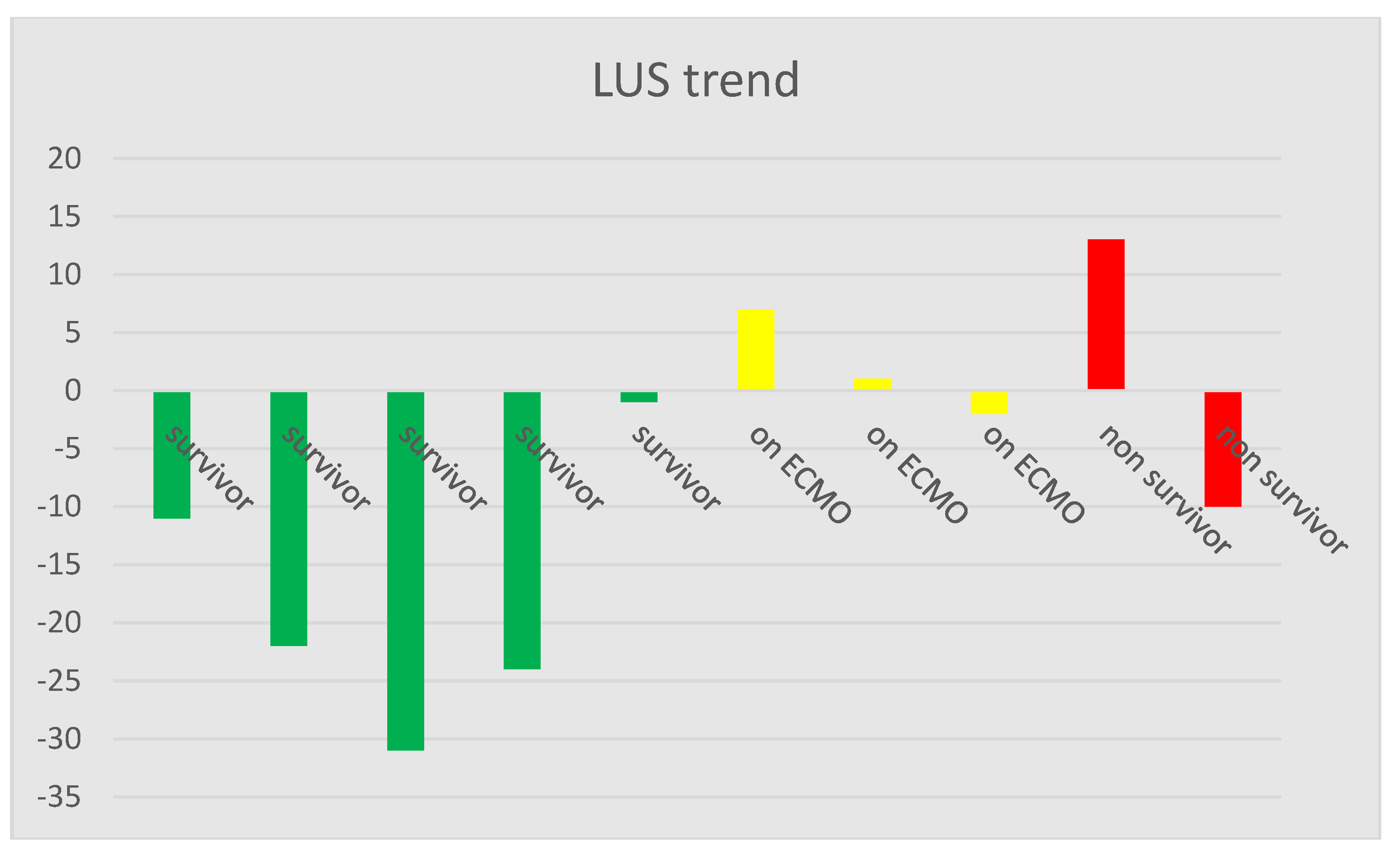
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Huang, C.; Wang, Y.; Li, X.; Ren, L.; Zhao, J.; Hu, Y.; Zhang, L.; Fan, G.; Xu, J.; Gu, X.; et al. Clinical features of patients infected with 2019 novel coronavirus in wuhan, china. Lancet 2020, 395, 497–506. [Google Scholar] [CrossRef] [Green Version]
- The species severe acute respiratory syndrome-related coronavirus: Classifying 2019-ncov and naming it sars-cov-2. Nat. Microbiol. 2020, 5, 536–544. [CrossRef] [PubMed] [Green Version]
- Li, M.; Lei, P.; Zeng, B.; Li, Z.; Yu, P.; Fan, B.; Wang, C.; Li, Z.; Zhou, J.; Hu, S.; et al. Coronavirus disease (covid-19): Spectrum of ct findings and temporal progression of the disease. Acad. Radiol. 2020, 27, 603–608. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, K.; Fang, Y.; Li, W.; Pan, C.; Qin, P.; Zhong, Y.; Liu, X.; Huang, M.; Liao, Y.; Li, S. Ct image visual quantitative evaluation and clinical classification of coronavirus disease (covid-19). Eur. Radiol. 2020. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wong, H.Y.F.; Lam, H.Y.S.; Fong, A.H.; Leung, S.T.; Chin, T.W.; Lo, C.S.Y.; Lui, M.M.; Lee, J.C.Y.; Chiu, K.W.; Chung, T.; et al. Frequency and distribution of chest radiographic findings in covid-19 positive patients. Radiology 2020. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Blaivas, M. Update on point of care ultrasound in the care of the critically ill patient. World J. Crit. Care Med. 2012, 1, 102–105. [Google Scholar] [CrossRef] [Green Version]
- Lichtenstein, D.A. Lung ultrasound in the critically ill. Ann. Intensive Care 2014, 4, 1. [Google Scholar] [CrossRef] [Green Version]
- Volpicelli, G.; Elbarbary, M.; Blaivas, M.; Lichtenstein, D.A.; Mathis, G.; Kirkpatrick, A.W.; Melniker, L.; Gargani, L.; Noble, V.E.; Via, G.; et al. International evidence-based recommendations for point-of-care lung ultrasound. Intensive Care Med. 2012, 38, 577–591. [Google Scholar] [CrossRef] [Green Version]
- Laursen, C.B.; Sloth, E.; Lassen, A.T.; Christensen, R.; Lambrechtsen, J.; Madsen, P.H.; Henriksen, D.P.; Davidsen, J.R.; Rasmussen, F. Point-of-care ultrasonography in patients admitted with respiratory symptoms: A single-blind, randomised controlled trial. Lancet. Respir. Med. 2014, 2, 638–646. [Google Scholar] [CrossRef]
- Peris, A.; Tutino, L.; Zagli, G.; Batacchi, S.; Cianchi, G.; Spina, R.; Bonizzoli, M.; Migliaccio, L.; Perretta, L.; Bartolini, M.; et al. The use of point-of-care bedside lung ultrasound significantly reduces the number of radiographs and computed tomography scans in critically ill patients. Anesth. Analg. 2010, 111, 687–692. [Google Scholar] [CrossRef]
- Chavez, M.A.; Shams, N.; Ellington, L.E.; Naithani, N.; Gilman, R.H.; Steinhoff, M.C.; Santosham, M.; Black, R.E.; Price, C.; Gross, M.; et al. Lung ultrasound for the diagnosis of pneumonia in adults: A systematic review and meta-analysis. Respir. Res. 2014, 15, 50. [Google Scholar] [CrossRef] [Green Version]
- Sezgin, C.; Gunalp, M.; Genc, S.; Acar, N.; Ustuner, E.; Oguz, A.B.; Tanriverdi, A.K.; Demirkan, A.; Polat, O. Diagnostic value of bedside lung ultrasonography in pneumonia. Ultrasound Med. Biol. 2020, 46, 1189–1196. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Z.; Liu, S.; Xiang, M.; Li, S.; Zhao, D.; Huang, C.; Chen, S. Protecting healthcare personnel from 2019-ncov infection risks: Lessons and suggestions. Front. Med. 2020, 14, 229–231. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Peng, Q.Y.; Wang, X.T.; Zhang, L.N. Findings of lung ultrasonography of novel corona virus pneumonia during the 2019–2020 epidemic. Intensive Care Med. 2020, 46, 849–850. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Soldati, G.; Smargiassi, A.; Inchingolo, R.; Buonsenso, D.; Perrone, T.; Briganti, D.F.; Perlini, S.; Torri, E.; Mariani, A.; Mossolani, E.E.; et al. Is there a role for lung ultrasound during the covid-19 pandemic? J. Ultrasound Med. 2020, 39, 1459–1462. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pivetta, E.; Goffi, A.; Lupia, E.; Tizzani, M.; Porrino, G.; Ferreri, E.; Volpicelli, G.; Balzaretti, P.; Banderali, A.; Iacobucci, A.; et al. Lung ultrasound-implemented diagnosis of acute decompensated heart failure in the ed: A simeu multicenter study. Chest 2015, 148, 202–210. [Google Scholar] [CrossRef] [Green Version]
- Lichtenstein, D.A.; Meziere, G.A. Relevance of lung ultrasound in the diagnosis of acute respiratory failure: The blue protocol. Chest 2008, 134, 117–125. [Google Scholar] [CrossRef] [Green Version]
- Chung, M.; Bernheim, A.; Mei, X.; Zhang, N.; Huang, M.; Zeng, X.; Cui, J.; Xu, W.; Yang, Y.; Fayad, Z.A.; et al. Ct imaging features of 2019 novel coronavirus (2019-ncov). Radiology 2020, 295, 202–207. [Google Scholar] [CrossRef] [Green Version]
- Volpicelli, G.; Mussa, A.; Garofalo, G.; Cardinale, L.; Casoli, G.; Perotto, F.; Fava, C.; Frascisco, M. Bedside lung ultrasound in the assessment of alveolar-interstitial syndrome. Am. J. Emerg. Med. 2006, 24, 689–696. [Google Scholar] [CrossRef]
- Moshavegh, R.; Hansen, K.L.; Moller-Sorensen, H.; Nielsen, M.B.; Jensen, J.A. Automatic detection of b-lines in in vivo lung ultrasound. IEEE Trans. Ultrason. Ferroelectr. Freq. Control 2019, 66, 309–317. [Google Scholar] [CrossRef]
- Kim, D.J.; Jelic, T.; Woo, M.Y.; Heslop, C.; Olszynski, P. Just the facts: Recommendations on point of care ultrasound use and machine infection control during the covid-19 pandemic. Can. J. Emerg. Med. 2020. [Google Scholar] [CrossRef] [Green Version]
- Lichtenstein, D. Novel approaches to ultrasonography of the lung and pleural space: Where are we now? Breathe 2017, 13, 100–111. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Via, G.; Storti, E.; Gulati, G.; Neri, L.; Mojoli, F.; Braschi, A. Lung ultrasound in the icu: From diagnostic instrument to respiratory monitoring tool. Minerva Anestesiol. 2012, 78, 1282–1296. [Google Scholar]
- Anderson, K.L.; Fields, J.M.; Panebianco, N.L.; Jenq, K.Y.; Marin, J.; Dean, A.J. Inter-rater reliability of quantifying pleural b-lines using multiple counting methods. J. Ultrasound Med. 2013, 32, 115–120. [Google Scholar] [CrossRef]
- Bobbia, X.; Chabannon, M.; Chevallier, T.; de La Coussaye, J.E.; Lefrant, J.Y.; Pujol, S.; Claret, P.G.; Zieleskiewicz, L.; Roger, C.; Muller, L. Assessment of five different probes for lung ultrasound in critically ill patients: A pilot study. Am. J. Emerg. Med. 2018, 36, 1265–1269. [Google Scholar] [CrossRef] [PubMed]
- Koratala, A.; Ronco, C.; Kazory, A. The promising role of lung ultrasound in assessment of volume status for patients receiving maintenance renal replacement therapy. Blood Purif. 2020. [Google Scholar] [CrossRef] [PubMed]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Table for LUS Findings of Left/Right Lung | Scoring System for LUS Findings | |||||
|---|---|---|---|---|---|---|
| Anterior | Lateral | Posterior | ||||
| Pleural thickening (Y/N) | Yes +3 | No 0 | ||||
| Lung sliding (Y/N) | No +3 | Yes 0 | ||||
| B-line appearance (none/multifocal/few) | None +3 | Multifocal +2 | Few +1 | |||
| A-line appearance (Y/N) | No +3 | Yes 0 | ||||
| Subpleural consolidation (Y/N) | Yes +2 | No 0 | ||||
| Lobar consolidation (Y/N) | Yes +2 | No 0 | ||||
| Pleural fluid (Y/N) | Yes +1 | No 0 | ||||
| Total (n = 10) | Survivor (n = 5) | On ECMO (n = 3) | Non-Survivor (n = 2) | |
|---|---|---|---|---|
| LUS score | 62.7 (9.9) | 60.4 (9.1) | 68.8 (8.0) | 61.2 (11.5) |
| CRP [mg/L] | 205.1 (107.6) | 189.5 (116.6) | 238.8 (81.4) | 202.3 (114.7) |
| Compliance [Cdyn] | 24.7 (18.4) | 25.7 (17.0) | 14.8 (5.2) | 33.9 (26.0) |
| Patient No. | Patient Status | LUS Start | LUS End | CRP Start [mg/L] | CRP End [mg/L] | Compliance Start [Cdyn] | Compliance End [Cdyn] |
|---|---|---|---|---|---|---|---|
| 1 | survivor | 74 | 63 | 334 | 191 | 18 | 25 |
| 2 | survivor | 69 | 47 | 291 | 56 | 19 | 24 |
| 3 | survivor | 72 | 41 | 80 | 44 | 14 | 75 |
| 4 | survivor | 66 | 42 | 354 | 89 | 46 | 45 |
| 5 | survivor | 59 | 58 | 448 | 128 | 12 | 35 |
| 6 | on ECMO | 63 | 70 | 180 | 216 | 22 | 14 |
| 7 | on ECMO | 61 | 62 | 130 | 106 | 16 | 9 |
| 8 | on ECMO | 71 | 69 | 330 | 280 | 14 | 9 |
| 9 | non-survivor | 63 | 76 | 307 | 56 | 9 | 7 |
| 10 | non-survivor | 57 | 47 | 380 | 219 | 43 | 46 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Møller-Sørensen, H.; Gjedsted, J.; Lind Jørgensen, V.; Lindskov Hansen, K. COVID-19 Assessment with Bedside Lung Ultrasound in a Population of Intensive Care Patients Treated with Mechanical Ventilation and ECMO. Diagnostics 2020, 10, 447. https://doi.org/10.3390/diagnostics10070447
Møller-Sørensen H, Gjedsted J, Lind Jørgensen V, Lindskov Hansen K. COVID-19 Assessment with Bedside Lung Ultrasound in a Population of Intensive Care Patients Treated with Mechanical Ventilation and ECMO. Diagnostics. 2020; 10(7):447. https://doi.org/10.3390/diagnostics10070447
Chicago/Turabian StyleMøller-Sørensen, Hasse, Jakob Gjedsted, Vibeke Lind Jørgensen, and Kristoffer Lindskov Hansen. 2020. "COVID-19 Assessment with Bedside Lung Ultrasound in a Population of Intensive Care Patients Treated with Mechanical Ventilation and ECMO" Diagnostics 10, no. 7: 447. https://doi.org/10.3390/diagnostics10070447