INTRODUCTION COVID-19 sequelae, or the short-, medium-, and long-term manifestations of the disease are under continuous study. There are currently few reports on the evolution of hematological variables following a demonstrated absence of SARS-CoV-2 after infection.
OBJECTIVE Identify hematological alterations in Cuban adults recovered from SARS-CoV-2 infection, and their relation with disease severity.
METHODS We selected 348 persons recovered from COVID-19 residing in Havana, Cuba with an RT-PCR study negative for SARS-CoV-2 performed two weeks after hospital discharge; a structured survey was administered to obtain clinical–epidemiological data. Three groups were established according to COVID-19 clinical criteria: asymptomatic, mild/moderately symptomatic, and severely symptomatic, which, in turn, were divided according to hospital discharge date and blood sample collection date. We performed hemograms with differential leukocyte counts and compared results among groups. We then measured the associations between hematological variables, personal medical history, and relevant lifestyle habits (smoking).
RESULTS All hematological variables were within normal reference limits, although men from the group of severely ill patients had increased total leukocytes, neutrophils and lymphocytes, and decreased hemoglobin and eosinophils, which was also evident in those with a recovery time of 31–90 days.
CONCLUSIONS The relation between hematological variables and degree of clinical severity offers evidence as to persistence of systemic alterations (possibly inflammatory) associated with viral infection. Their identification and characterization can facilitate personalized patient followup and rehabilitation.
KEYWORDS COVID-19, SARS-CoV-2, hematology, leukocytosis, neutrophils, eosinophils, Cuba
ABSTRACT INTRODUCTION COVID-19 sequelae, or the short-, medium-, and long-term manifestations of the disease are under continuous study. There are currently few reports on the evolution of hematological variables following a demonstrated absence of SARS-CoV-2 after infection.
OBJECTIVE Identify hematological alterations in Cuban adults recovered from SARS-CoV-2 infection, and their relation with disease severity.
METHODS We selected 348 persons recovered from COVID-19 residing in Havana, Cuba with an RT-PCR study negative for SARS-CoV-2 performed two weeks after hospital discharge; a structured survey was administered to obtain clinical–epidemiological data. Three groups were established according to COVID-19 clinical criteria: asymptomatic, mild/moderately symptomatic, and severely symptomatic, which, in turn, were divided according to hospital discharge date and blood sample collection date. We performed hemograms with differential leukocyte counts and compared results among groups. We then measured the associations between hematological variables, personal medical history, and relevant lifestyle habits (smoking).
RESULTS All hematological variables were within normal reference limits, although men from the group of severely ill patients had increased total leukocytes, neutrophils and lymphocytes, and decreased hemoglobin and eosinophils, which was also evident in those with a recovery time of 31–90 days.
CONCLUSIONS The relation between hematological variables and degree of clinical severity offers evidence as to persistence of systemic alterations (possibly inflammatory) associated with viral infection. Their identification and characterization can facilitate personalized patient followup and rehabilitation.
KEYWORDS COVID-19, SARS-CoV-2, hematology, leukocytosis, neutrophils, eosinophils, Cuba
INTRODUCTION COVID-19, caused by the SARS-CoV-2 virus, is most frequently characterized by fever, malaise, cough, sore throat and muscle aches, occurring in approximately 95% of patients who develop symptoms following an incubation period of 4–5 days.[1–5] Severe presentations of the disease begin a week after symptom onset and present as dyspnea accompanied by hypoxemia, and can progress to respiratory failure, a clinical picture consistent with criteria for acute respiratory distress syndrome (ARDS).[5,6]
Laboratory, chemical and hematological variables have been characterized in multiple publications as predictors of clinical severity.[7–13] Variations in hematological and blood chemistry values during the disease’s active phase have been noted, especially in hospitalized patients and patients who progress to severe forms of the disease. The most common findings include lymphopenia, elevated D-dimer levels, and elevated levels of lactate dehydrogenase, C-reactive protein, and ferritin.[14,15]
IMPORTANCE Hematological alterations in patients recovered from SARS-CoV-2 infection confirm the persistence of inflammatory processes associated with viral infection and reveal the existence of pathological processes following, and possibly associated with, COVID-19.
Some of these variables are associated with poor prognoses, including increased total white blood count, increased neutrophil/lymphocyte ratio (NLR),[16,17] eosinopenia, prolonged prothrombin time, increased liver enzyme levels, and increased levels of interleukin-6 (IL-6) and procalcitonin.[8,15] Increased eosinophil levels prior to clinical discharge have been reported as indicators of improved outcomes.[8–21] However, there are few reports as to the status of these variables in individuals who are in stages of convalescence or recovery.
The Cuban Action Protocol for COVID-19 establishes how to manage recovering COVID-19 patients in primary health care (PHC),[22] emphasizing multidisciplinary collaboration and personalized followup, aimed at detecting complications or sequalae to adopt the most appropriate treatment, aid in rehabilitation and improve quality of life.
This study’s objective was to identify hematological variations in adult Cubans considered clinically recovered from SARS-CoV-2 infection.
METHODS Design and study group definition We carried out a cross-sectional analytical, observational study from June 25 through July 25, 2020, in all 15 municipalities of the Cuban capital, Havana. The study universe was comprised of all Cubans aged >18 years who were infected with SARS-CoV-2 from March 11 through June 11, 2020, with negative RT-PCR (real-time polymerase chain reaction) results two weeks after hospital discharge. Those who traveled outside their local community polyclinic’s geographic health area during the study period and those whose records showed either discrepancies between databases or a lack of information (provided by patients or attending physicians) were excluded. A final sample was obtained based on the sole criterion of willingness to participate in the study.
We established three study groups, according to the disease’s clinical characteristics and evolution: the asymptomatic group, composed of those who developed no symptoms or clinical signs of COVID-19; the mild–moderate group, of those patients who presented clinical signs of COVID-19 or reported symptoms, without presenting clinical complications; and severe group, denoting those who presented severe symptoms, with complications such as pneumonia, ARDS, cardiac arrhythmias, venous thrombosis and disseminated intravascular coagulation, who required intensive care due to alterations in respiratory rate, blood oxygen saturation, partial pressure of arterial oxygen or pulmonary infiltrates >50% in 24–48 hours, septic shock or multiple organ failure or dysfunction.
Clinical groups were, in turn, divided according to the period between hospital discharge date and the date biological samples were taken. For study purposes, this variable was defined as ‘recovery time’ and was divided as follows: time-group 1 (≤30 days); time-group 2 (31–60 days); time-group 3 (61–90 days), and time-group 4 (>90 days). We thus ensured that comparisons were made between individuals with similar recovery times.
Data collection and biological sampling Each municipality established a schedule according to their territorial extension and number of reported cases.[23] Working groups were created, bringing together researchers and specialists from multiple polyclinic health areas of different municipalities, and databases of these areas were obtained from the Municipal Hygiene and Epidemiology Divisions, facilitating identification and selection of individuals who met research criteria. They were then visited by genetic counselors and primary healthcare physicians who provided them with information necessary to aid in their decision as to whether to participate in the research.
Interviews were conducted during the morning hours in selected polyclinics. During the interviews, participants received a brief explanation as to the study’s purpose and characteristics, signed informed consent forms, and participated in the structured survey. The survey included general personal data, medical history, relevant lifestyle habits and aspects related to the disease and its evolution, as well as the treatment received. This information was used to make definitive assignments to the corresponding study groups, since the databases consulted only provided relevant clinical information that was collected at the time positive diagnosis was made.
Biological samples were also taken during these interviews. People of advanced age, or those who had physical limitations were visited and interviewed in their homes. Blood samples (3 mL) were taken by polyclinic laboratory personnel at least two hours after eating. Samples were extracted via peripheral venous puncture, maintaining aseptic and antiseptic measures, guaranteeing patient safety and sample quality. Samples were stored in Vacutest tubes with the anticoagulant EDTA-K2 (Deltalab, Spain) at 8 ºC and protected from light until processing.
Variable definitions The following hematological variables were analyzed: hemoglobin concentration, platelet cell count, total leukocytes, lymphocytes, neutrophils, eosinophils, basophils and monocytes. Reference values for each variable by age and sex were adopted according to standardized equipment values and international units.[24] Medians and interquartile ranges (IQR) were collected for each variable, according to clinical group and recovery time. Results were classified as normal, low and high, and we used the semiological nomenclature corresponding to each condition.
Hematological studies All hematological studies were performed at the National Medical Genetics Center (CNGM) clinical laboratory (Havana, Cuba), using the BC-6800 Automatic Hematology Analyzer (Mindray, Spain) that performs a differential count of five leukocyte subpopulations.[25] All laboratory techniques were performed according to established operational regulatory procedures and followed good clinical laboratory practices.[26]
Data analysis and processing IBM SPSS, version 22, was used for statistical analysis, and GraphPad Prism, version 7.00 (GraphPad Software, San Diego, USA) was used to prepare the figures.
Odds ratios and 95% confidence intervals (95% CI) Odds ratios with their confidence intervals were calculated to evaluate the association of smoking and the most prevalent variables in medical histories with each hematological variable.
Ethical considerations This study is part of a research project approved by CNGM’s Scientific Council and Medical and Research Ethics Committee, and by the Cuban Ministry of Health’s Innovation Committee. All participants provided written informed consent. Individuals with cognitive disabilities were represented by their parents, guardians or legal representatives. Participant confidentiality was maintained through data encryption and limited access to information. Individual study results were communicated to patients and their attending physicians to facilitate better patient care and followup.
RESULTS From March 11 through June 11, 2020, 1183 confirmed positive cases of SARS-CoV-2 infection were diagnosed in Havana.[24] After applying selection criteria, we obtained a sample of 348 individuals, divided into the three clinical groups (Table 1).
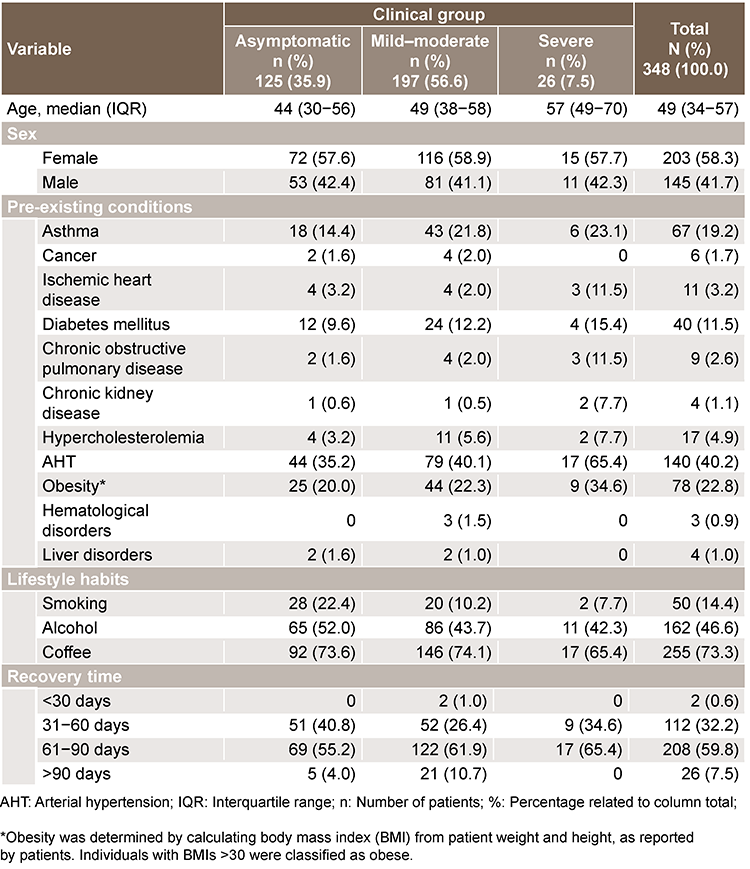
Table 1: Characteristics of patients recovered from SARS-CoV-2 infection, by clinical group
Most patients (56.6%; 197/348) had mild–moderate COVID-19 symptoms, and only 7.5% (26/348) presented with severe forms of the disease. Distribution by sex was similar in the three clinical groups, and there were more women in the sample (58.3%; 203/348) (Table 1). Patients who suffered severe forms of the disease tended to be older, and this group also had the highest percentage of pre-existing comorbidities and chronic diseases (data not shown).
Recovery for the vast majority of patients (92%; 320/348) was 31–90 days (time-groups 2 and 3). In the other two time-groups (≤30 days and >90 days) there were few or no cases in at least one clinical group, limiting comparative analysis by clinical severity (Table 1)
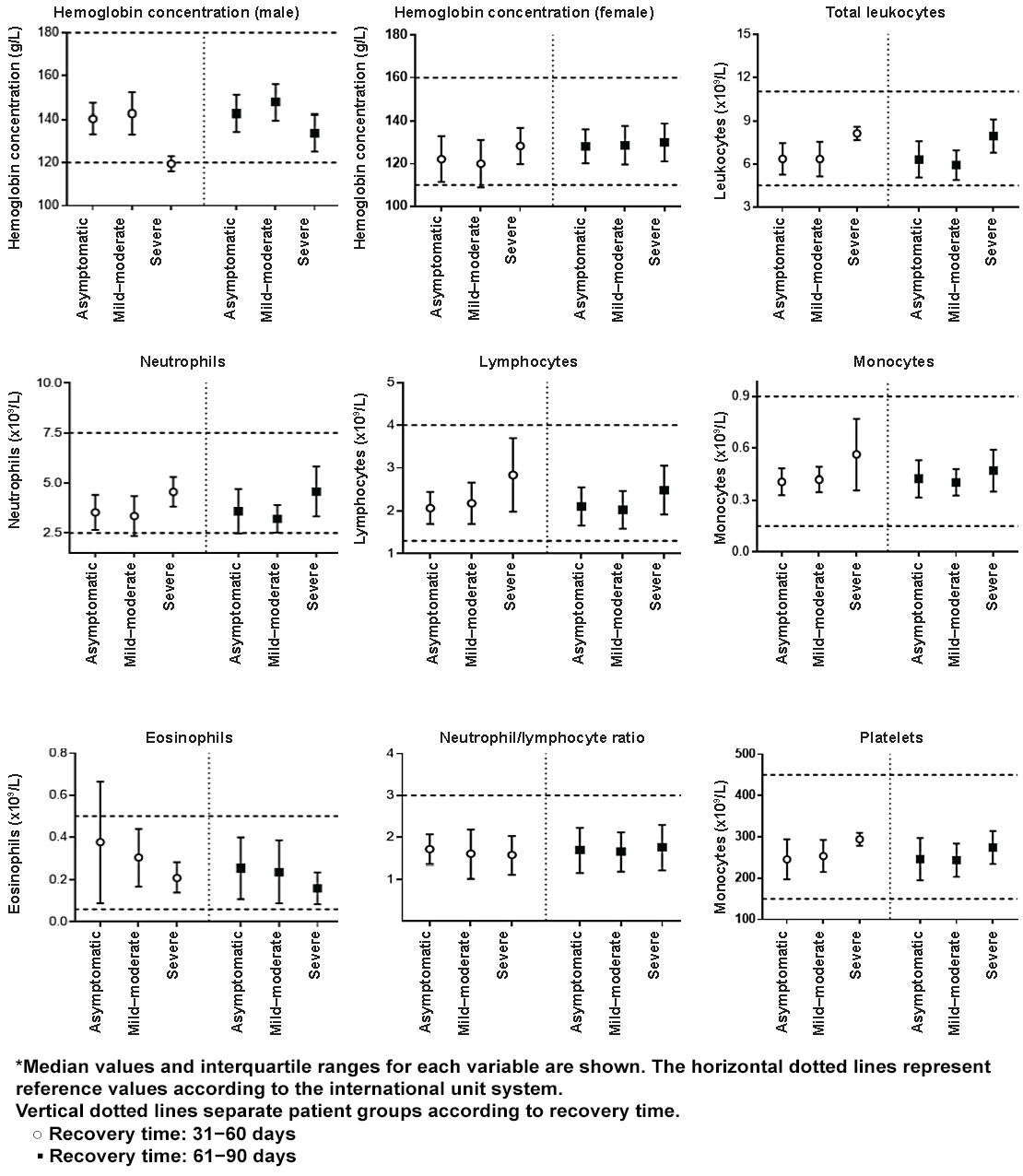
Hematological parameter results Medians and IQRs of hematological variables by clinical group (asymptomatic, mild–moderate and severe) for those in two of the recovery groups (31−60 day time-group and 61−90 day time group) are shown in Figure 1. With the exception of hemoglobin concentrations in men with a severe form of the disease, values are within reference ranges. However, appreciable differences were found in values of patients who presented severe disease forms when compared to the other two clinical groups (asymptomatic and mild–moderate), in both the 31–60 day time-group and the 61–90 day time-group. The neutrophil/lymphocyte ratio in both time-groups and the hemoglobin concentration in women in the 61–90 day time-group are exceptions; these two variables present similar values in all three clinical groups.
Patients with severe disease presentations had higher numbers of total leukocytes, neutrophils, lymphocytes and monocytes, and lower numbers of eosinophils. These differences were greater in the 31−60 day time group, when comparing the severe group’s leukocyte and neutrophil levels with those of the asymptomatic group and the mild–moderate symptomatic group. Differences in lymphocyte and monocyte levels were remarkably large between severe and asymptomatic groups.
Severely-ill patients in the 61−90 day time-group also had higher total leukocyte and neutrophil levels than asymptomatic and mild–moderate symptomatic patients.
In both time-groups, eosinophil levels were somewhat lower in severe patients. Basophil levels were normal and similar in all three clinical groups and at all recovery times (data not shown). On the other hand, platelet counts were higher in the severe group at both recovery times, although striking differences were only observed in the 31−60 day time-group.
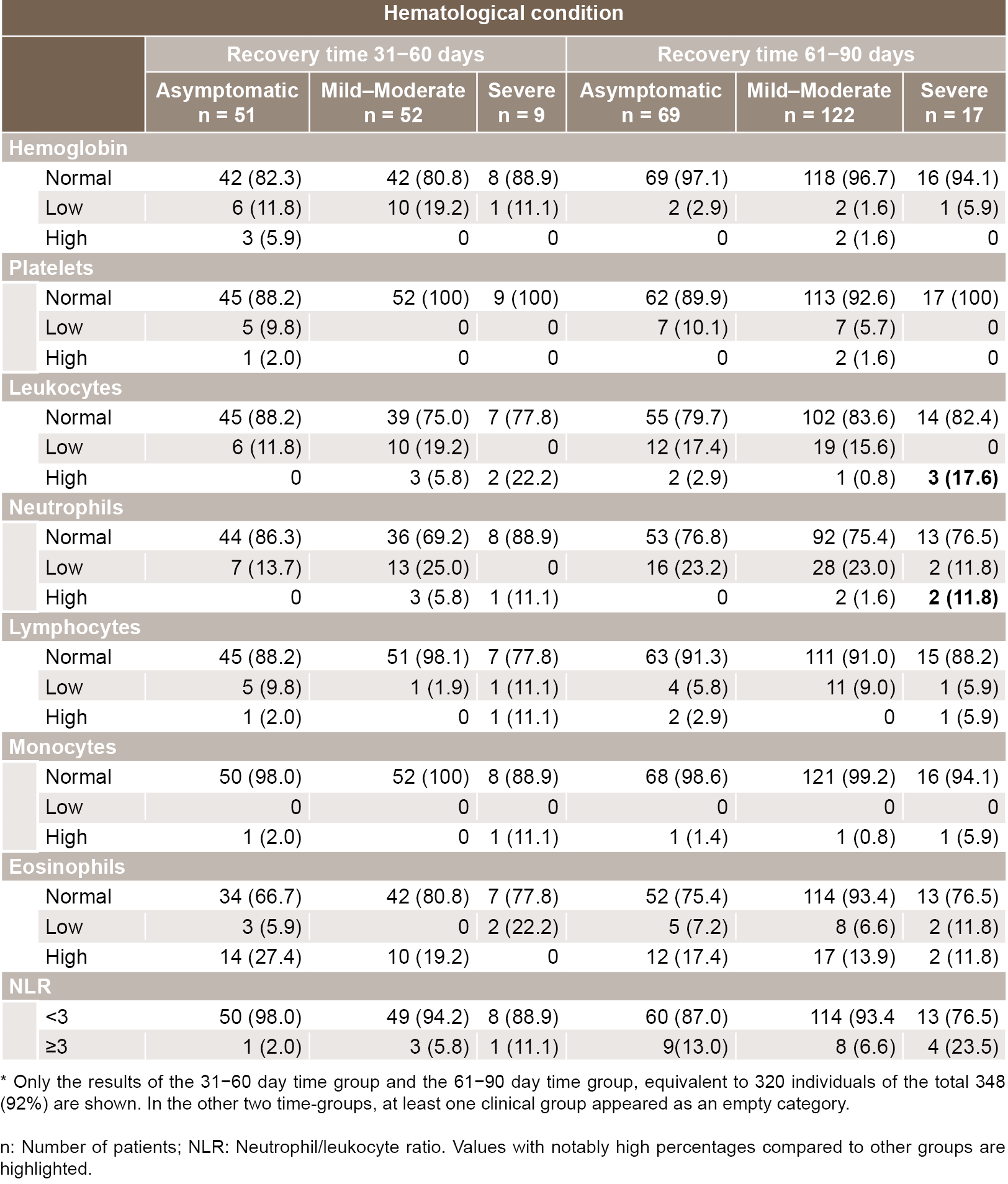
Positive hematological variable results analysis Median and IQR variable values fell within reference ranges (except hemoglobin concentrations in men); however, a relatively high percentage of individuals had values outside the reference ranges. Table 2 shows the absolute frequencies and percentages of individuals with values above or below the reference range for each variable according to clinical group and recovery time. In 31−60 day time-group, 15.2% (17/112) presented with anemia, distributed among three clinical groups, compared to 2.4% (5/208) of those in the 61−90 day time-group who suffered from anemia.
Persons with >90 days of recovery time who presented with asymptomatic SARS-CoV-2 infection had normal hematological values. Only 2 of the 21 individuals with mild–moderate COVID-19 presented leukopenia with neutropenia, and another 2 presented with eosinophilia (values not shown).
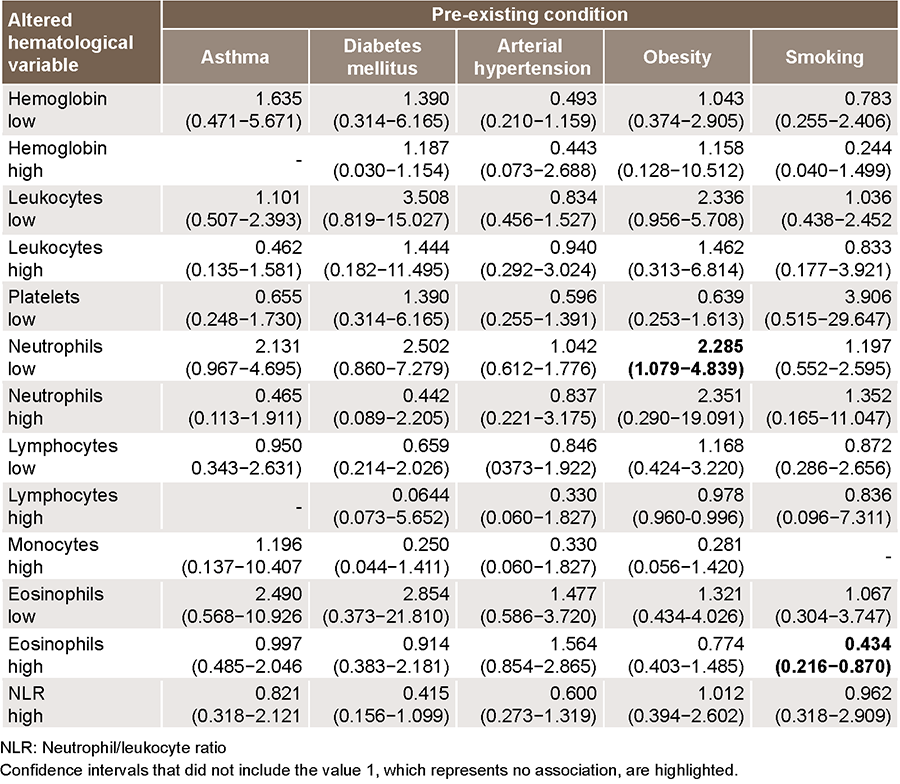
Association analysis We calculated odds ratio values (95% CI) to asses association between medical history (bronchial asthma, diabetes mellitus, arterial hypertension, obesity and smoking) with changes in hematological variables (Table 3). Among obese individuals, neutropenia was 2.28 times more frequent than for those in other weight groups. Smokers, however, were less likely to have high eosinophil levels.
DISCUSSION Scientific publications and case reports on COVID-19 have increased exponentially since the appearance of the first cases in 2019. Reports have characterized COVID-19’s infectious agent, the various presentations of the disease and the pathophysiological mechanisms behind the disease’s complications;[5,27] treatments and their efficacy;[28,29] and more recently, vaccine development and clinical trials.[30] However, scarcity of labora tory studies of patients recovered from the disease makes it difficult to compare this study’s results.
Figure 1: Characteristics of patients recovered from SARS-CoV-2 infection, by clinical group and recovery time (31−60 days and 61−90 days)
Our study participants were mostly reintegrated into their family, community and working lives, although they complied with clinical–epidemiological followup through community health services, in accordance with the Cuban protocol for convalescent patient care.[22] The fact that the medians and IQRs of most hematological values fell within reference limits indicates that most study participants had normal values at the time of sampling.
However, it is noteworthy that patients who presented with severe forms of the disease had higher levels of leukocytes, neutrophils and monocytes, decreased hemoglobin concentrations, and decreased eosinophil levels. Severely ill patients were also more likely to have leukocytosis, neutrophilia, eosinophilia, and a higher percentage of them had NLR values greater than 3 at two and three months after clinical discharge. From these results, it could be interpreted that the immunological and inflammatory mechanisms triggered in these patients and that motivated the torpid evolution of the disease continued to be stimulated over time, even after the infection had disappeared.[10,31–33] This is similar to reports by Sherina,[34] which confirm persistence of an immune response eight months after SARS-CoV-2 diagnosis. On the other hand, the group of patients who presented with severe disease also presented with a greater number and likelihood of associated comorbidities, which makes their care more complex and slower evolution more likely. The influence of age and comorbidities on hematological alterations cannot be ruled out, even when statistical analyses have not shown a clear association.[6,35]
Table 2: Absolute frequencies and percentages of patients recovered from SARS-CoV-2 infection, by hematological variable reference values, according to clinical groups and recovery time*
Studies in convalescent patients or in patients recovered from infection have referred mainly to the presence of symptoms, pulmonary alterations, immune responses and, to a lesser extent, changes in hematological parameters. Shaw[36] reported persistence of pathological images in chest tomography and demonstrated that disease consequences can persist for over a month after clinical discharge, including the appearance of other infections and alterations in laboratory findings such as progressive lymphopenia and neutrophilia. Similar results were reported by Sonnwber,[37] who described persistence of symptoms in a group of recovered patients, with decreased capillary pO2 in 37% of study participants, as well as increased levels of C-reactive protein (12%), IL-6 (6%), procalcitonin (9%), D-dimer (27%) and ferritin (17%), 100 days after the infection was diagnosed. In the present study, only the results of a complete leukogram are available; determinations of specific and other non-specific inflammatory response variables were not performed, preventing comparison of these results with those of other authors.
Zhao[33] found decreased lymphocytes and increased neutrophils in COVID-19 patients in the recovery stage up to four weeks after hospital discharge (similar to influenza infection). They also found increased neutrophil levels in critically ill patients, consistent with our study’s results. They conclude that COVID-19 patients have decreased antiviral immunity and increased anti-inflammatory responses, which are maintained during the recovery stage.
Table 3: Odds ratios values (95% confidence intervals) between pre-existing conditions and altered hematological variables
Rodriguez[31] reported that increases in NLR during the disease’s acute phase undergo a slow reversal during recovery. These results are similar to those of our study and could reinforce the hypothesis that inflammatory and immunological processes are stimulated in patients with more severe forms of the disease.
Although variables related to medications used during the disease’s acute stage were not analyzed in this study, treatments for patients were uniform and governed by approved protocols established for the entire country, even for patients who had asymptomatic forms of the disease. These protocols include the use of steroids in intensive care units.[22] Medical literature reports an association between leukocytosis and steroid treatments, especially with high doses. These treatments can cause extreme and persistent leukocytosis, which may be associated with monocytosis, neutrophilia, lymphopenia and eosinopenia, conditions seen in the severe-illness group.[38,39]
The low levels of hemoglobin concentration in men, mainly in the 31−60 day time group, also seem to be related to the processes associated with infection. It is noteworthy that individuals with a longer recovery time (both men and women) had higher hemoglobin concentrations and a lower likelihood of anemia. One possible conjecture is that a longer recovery time led to the removal of factors—including direct alterations to iron metabolism or distribution—that were still present in shorter recovery periods.[40–42]
Identifying the causes or factors related to the eosinophil alterations found in this study is difficult, as these alterations were found not only in the severe group, but also the asymptomatic group, which included younger people and high percentages of eosinophilia. In this case, eosinophilia’s various causes (and presence of intestinal parasites or allergies, common in this age group) must be ruled out by complementary testing.
Fraisse[21] suggests that COVID-19 may be either directly or indirectly responsible for eosinophilia, resulting from recovery mechanisms activated by a hyperstimulated immune system during the so-called ‘cytokine storm.’ These mechanisms could be influencing the high percentages of eosinophilia observed in our study. Liu[43] links eosinophilia to therapies combining lopinavir and interferon alpha 2b, and Mateos González[19] reported a relationship between eosinophilia and prescribed COVID-19 treatments involving lopinavir, ritonavir, azithromycin or low-molecular-weight sodium heparin.
One of the striking study results is the paradoxical negative association between smoking and high eosinophil levels. This directly contradicts previous reports by Hartl,[44] who found high levels of eosinophils in smokers in a study of over 11,000 Australians, and Caspard,[45] who reported elevated levels of peripheral blood eosinophils in current and former smokers with asthma, compared with never-smokers.
Exposure to tobacco and cigarette smoke causes alterations to airways and lung parenchyma, with direct cellular damage to the alveolar epithelium and other cells, leading to a localized inflammatory response that recruits other immune system cells, including eosinophils.[46] The negative association between smoking and high eosinophil levels found in this study may be due to direct acute damage caused to lung tissue by the virus, damage exacerbated by smoking, resulting in localized eosinophil recruitment to the lungs and lower circulating eosinophil levels in peripheral blood.
One limitation of this study is its cross-sectional characterization of recovered individuals, and the lack of comparison to the acute phase of the disease. There is also no information as to the status of the measured variables before infection, so some of the study’s results could be related to pre-existing disease or concomitant inflammatory or infectious processes (which could be undiagnosed). It is also not possible to rule out infections or other inflammatory processes in the period between the acute phase of the disease and the time of the study. Additionally, only complete leukograms were considered, and we did not examine other specific or non-specific inflammatory response variables. Another limitation of this study was the use of a structured survey to obtain information, which is prone to errors and recall bias, especially in individuals with severe forms of the disease.
However, the results presented provided evidence which can aid in developing improved strategies for followup care of patients recovering from COVID-19 in Cuba and their multidisciplinary management.
CONCLUSIONS In persons recovered from SARS-CoV-2 infection, hematological changes and their relation to disease clinical severity suggest persistence of systemic changes—possibly inflammatory—associated with viral infection. Identification and characterization of such changes facilitate personalized COVID-19 followup care and rehabilitation.
ACKNOWLEDGEMENTS The authors thank the Cuban Public Health Ministry for funding this research, Havana’s Municipal Hygiene and Epidemiology Division for access to patient information databases, and all primary healthcare personnel who provided support during this research.
Xu J, Ma XP, Bai L, Wang M, Deng W, Ning N. A systematic review of etiology, epidemiology, clinical manifestations, image findings, and medication of 2019 Corona Virus Disease-19 in Wuhan, China. Medicine [Internet]. 2020 [cited 2020 Dec 18];99:42(e22688). http://dx.doi.org/10.1097/MD.0000000000022688
Dhama K, Khan S, Tiwari R, Sircar S, Bhat S, Malik YS, et al. Coronavirus Disease 2019–COVID-19. Clin Microbiol Rev [Internet]. 2020 [cited 2020 Oct 28];33(4):e00028-20. Available at: https://journals.asm.org/doi/full/10.1128/CMR.00028-20
Berlin DA, Gulik RM, Martínez FJ. Severe Covid-19. N Engl J Med. 2020;383:2451‒60. https://doi.org/10.1056/NEJMcp2009575
Fan BE, Chong VCL, Chan SSW, Lim GH, Lim KGE, Tan GB, et al. Hematologic parameters in patients with COVID-19 infection. Am J Hematol. 2020;95(6):E131‒E134. https://doi.org/10.1002/ajh.25774
Lippi G, Plebani M. Laboratory abnormalities in patients with COVID-2019 infection. Clin Chem Lab Med. 2020;58(7):1131–4. https://doi.org/10.1515/cclm-2020-0198
Yun H, Sun Z, Wu J, Tang A, Hu M, Xiang Z. Laboratory data analysis of novel coronavirus (COVID-19) screening in 2510 patients. Clin Chimica Acta. 2020;507:94–7. https://doi.org/10.1016/j.cca.2020.04.018
Lu G, Wang J. Dynamic changes in routine blood parameters of a severe COVID-19 case. Clinica Chimica Acta. 2020;508:98–102. https://doi.org/10.1016/j.cca.2020.04.034
Chen J, Pan Y, Li G, Xu W, Zhang L, Yuan S, et al. Distinguishing between COVID‐19 and influenza during the early stages by measurement of peripheral blood parameters. J Med Virol [Internet]. 2020 [cited 2020 Dec 18];1–9. Available at: https://doi.org/10.1002/jmv.26384
Liao D, Zhou F, Luo L, Xu M, Wang H, Xia J, et al. Haematological characteristics and risk factors in the classification and prognosis evaluation of COVID-19: a retrospective cohort study. Lancet Haematol. 2020;7(9):e671-e678. https://doi.org/10.1016/S2352-3026(20)30217-9
Yan B, Yang J, Xie Y, Tang X. Relationship between blood eosinophil levels and COVID-19 mortality. World Allergy Organization Journal [Internet]. 2021;14(3):100521. http://doi.org/10.1016/j.waojou.2021.100521
Stone JR, Tran KM, Conklin J, Mino-Kenudson M. Case record of the Massachusetts General Hospital. Case 23-2020: a 76-year-old woman who died from Covid-19. N Engl J Med [Internet]. 2020 [cited 2020 Oct 28];383:380−7. Available at: https://www.nejm.org/doi/full/10.1056/NEJMcpc2004974
Terpos E, Ntanasis-Stathopoulos I, Elalamy I, Kastritis E, Sergentanis TN, Politou M, et al. Hematological findings and complications of COVID-19. Am J Hematol [Internet]. 2020 [cited 2020 Oct 28];95(7):834−47. https://doi.org/10.1002/ajh.25829
Liu J, Liu Y, Xiang P, Pu L, Xiong H, Li C, et al. Neutrophil to lymphocyte ratio predicts critical illness patients with 2019 coronavirus disease in the early stage. J Transl Med. 2020;18:206. https://doi.org/10.1186/s12967-020-02374-0
Lagunas-Rangel FA. Neutrophil‐to‐lymphocyte ratio and lymphocyte‐to‐C‐reactive protein ratio in patients with severe coronavirus disease 2019 (COVID‐19): A meta-analysis. J Med Virol. 2020;92:1733–4. https://doi.org/ 10.1002/jmv.25819
Rodrigo-Muñoz JM, Sastre B, Cañas JA, Gil-Martínez M, Redondo N, del Pozo V. Eosinophil response against classical and emerging respiratory viruses: COVID-19. J Investig Allergol Clin Immunol. 2021;31(2). https://doi.org/10.18176/jiaci.0624
Mateos González M, Sierra Gonzalo E, Casado Lopez I, Arnalich Fernández F, Beato Pérez JL, Monge Monge D, et al. The prognostic value of eosinophil recovery in COVID-19: A multicentre, retrospective cohort study on patients hospitalised in Spanish hospitals. J. Clin. Med. 2021;10(2):305. https://doi.org/10.3390/jcm10020305
Xie G, Ding F, Han L, Yin D, Lu H, Zhang M. The role of peripheral blood eosinophil counts in COVID-19 Patients. Allergy. 2020;10:1–12. https://doi.org/10.1111/all.14465
Fraisse M, Logre E, Mentec H, Cally R, Plantefeve G, Contou D. Eosinophilia in critically ill COVID‑19 patients: a French monocenter retrospective study. Crit Care. 2020;24:635. https://doi.org/10.1186/s13054-020-03361-z
COVID-19 Cuba Data [Internet]. Havana: CubaData; c2020 [updated 2021 Sep 10; cited 2020 Jun 15]. Available at: https://covid19cubadata.github.io/#cuba. Spanish
Escobar Carmona E. Valores de referencia del Laboratorio Clínico más empleados en Cuba. Año 2011. Gaceta Médica Espirituana [Internet] [cited 2020 Aug 31]; 2011;13(2). Available at: http://revgmespirituana.sld.cu/index.php/gme/article/view/257. Spanish
Mindray Bio-Medical Electronics Co [Internet]. Madrid: Mindray; c2020. Productos. Diagnóstico in vitro. Analizadores hematológicos y reactivos. 5-Diff Hematología. BC-6800 analizador automático para hematología; [cited 2020 Oct 26]; [about 3 p.]. Available at: https://www.mindray.com/es/product/BC-6800.html. Spanish.
Liu L, Shan H, Lei C, Hui DSC, Du B, Li L, et al. Clinical characteristics of coronavirus disease 2019 in China. N Engl J Med [Internet]. 2020 [cited 2020 Oct 28];382:1708−20. Available at: https://www.nejm.org/doi/full/10.1056/neJMoa2002032
Dubey AK, Singh A, Prakash S, Kumar M, Singh AK. Race to arsenal COVID-19 therapeutics: Current alarming status and future directions. Chem Biol Interact. 2020;332:109298. https://doi.org/10.1016/j.cbi.2020.109298
Poland GA, Ovsyannikova IG, Kennedy RB. SARS-CoV-2 immunity: review and applications to phase 3 vaccine candidates. Lancet. 2020;4:396(10262):1595−606. https://doi.org/10.1016/S0140-6736(20)32137-1
Rodriguez L, Pekkarinen PT, Lakshmikanth T, Tan Z, Consiglio CR, Pou C, et al. Systems-level immunomonitoring from acute to recovery phase of severe COVID-19. Cell Rep Med. 2020;1(5):100078. https://doi.org/10.1016/j.xcrm.2020.100078.
Wang C, Deng R, Gou L, Fu Z, Zhang X, Shao F, et al. Preliminary study to identify severe from moderate cases of COVID-19 using combined hematology parameters. Ann Transl Med. 2020;8(9):593. https://doi.org/10.21037/atm-20-3391
Zhao G, Su Y, Sun X, Cui X, Dang L, Zhao L, et al. A comparative study of the laboratory features of COVID-19 and other viral pneumonias in the recovery stage. J Clin Lab Anal . 2020;34(10):e23483. https://doi.org/10.1002/jcla.23483
Sherina N, Piralla A, Du L, Wan H, Kumagai-Braesch M, Andréll J, et al. Persistence of SARS-CoV-2-specific B and T cell responses in convalescent COVID-19 patients 6-8 months after the infection. Med (NY). 2021;2(3):281−95. https://doi.org/10.1016/j.medj.2021.02.001
Liang J, Nong S, Jiang L, Chi X, Bi D, Cao J, et al. Correlations of disease severity and age with hematology parameter variations in patients with COVID-19 pre- and post-treatment. J Clin Lab Anal. 2021;35(1):e23609. https://doi.org/10.1002/jcla.23609
Shaw B, Daskareh M, Gholamrezanezhad A. The lingering manifestations of COVID-19 during and after convalescence: update on long-term pulmonary consequences of coronavirus disease 2019 (COVID-19). Radiol Med. 2021;126(1):40−6. https://doi.org/10.1007/s11547-020-01295-8
Sonnweber T, Sahanic S, Pizzini A, Luger A, Schwabl C, Sonnweber B, et al. Cardiopulmonary recovery after COVID-19: an observational prospective multicentre trial. Eur Respir J. 2021;57(4):2003481. https://doi.org/10.1183/13993003.03481-2020
Frenkel A, Kachko E, Cohen K, Novack V, Maimon N. Estimations of a degree of steroid induced leukocytosis in patients with acute infections. Am J Emerg Med. 2018 ;36(5):749−53. https://doi.org/10.1016/j.ajem.2017.10.003
Shoenfeld Y, Gurewich Y, Gallant LA, Pinkhas J. Prednisone-induced leukocytosis. Influence of dosage, method and duration of administration on the degree of leukocytosis. Am J Med. 1981;71(5):773−8. https://doi.org/10.1016/0002-9343(81)90363-6
Taneri PE, Gómez-Ochoa SA, Llanaj E, Raguindin PF, Rojas LZ, Roa-Díaz ZM, et al. Anemia and iron metabolism in COVID-19: a systematic review and meta-analysis. Eur J Epidemiol. 2020;35(8):763−73. https://doi.org/10.1007/s10654-020-00678-5
Cavezzi A, Troiani E, Corrao S. COVID-19: hemoglobin, iron, and hypoxia beyond inflammation. A narrative review. Clin Pract. 2020;10(2):1271. https://doi.org/10.4081/cp.2020.1271
Tao Z, Xu J, Chen W, Yang Z, Xu X, Liu L, et al. Anemia is associated with severe illness in COVID-19: A retrospective cohort study. J Med Virol. 2021;93(3):1478−88. https://doi.org/10.1002/jmv.26444
Liu F, Xu A, Zhang Y, Xuan W, Yan T, Pan K, et al. Patients of COVID-19 may benefit from sustained Lopinavir-combined regimen and the increase of Eosinophil may predict the outcome of COVID-19 progression. Int J Infect Dis. 2020;95:183−91. https://doi.org/10.1016/j.ijid.2020.03.013
Hartl S, Breyer MK, Burghuber OC, Ofenheimer A, Schrott A, Urban MH, et al. Blood eosinophil count in the general population: typical values and potential confounders. Eur Respir J. 2020;55(5):1901874. https://doi.org/10.1183/13993003.01874-2019
Caspard H, Ambrose CS, Tran TN, Chipps BE, Zeiger RS. Associations between individual characteristics and blood eosinophil counts in adults with asthma or COPD. J Allergy Clin Immunol Pract. 2020;8(5):1606‒13. https://doi.org/10.1016/j.jaip.2019.12.019
Kumar A, Cherian SV, Vassallo R, Yi ES, Ryu JH. Current concepts in pathogenesis, diagnosis, and management of smoking-related interstitial lung diseases. Chest. 2018;154(2):394‒408. https://doi.org/10.1016/j.chest.2017.11.023
THE AUTHORS
Nayade Pereira-Roche (Corresponding author: nayade.pereira@infomed.sld.cu), physician specializing in clinical biochemistry, with a master’s degree in atherosclerosis research. Assistant professor and adjunct researcher, National Medical Genetics Center (CNGM), Havana, Cuba. https://orcid.org/0000-0002-3801-5609
Hilda Roblejo-Balbuena, physician specializing in clinical genetics, with a master’s degree in pediatrics and a doctorate in the medical sciences. Associate professor and associate researcher, CNGM, Havana, Cuba. https://orcid.org/0000-0002-5895-8057
Lilia Caridad Marín-Padrón, healthcare technologist, with a master’s degree in laboratory science. Adjunct researcher. CNGM, Havana, Cuba. https://orcid.org/0000-0001-9819-4648
Rodolfo Izaguirre-Rodríguez, physician specializing in internal medicine. Assistant professor, Medical–Surgical Research Center (CIMEQ), Havana, Cuba. https://orcid.org/0000-0002-0387-0197
Francisco Sotomayor-Lugo, physician specializing in clinical genetics. Assistant professor and adjunct researcher, CNGM, Havana, Cuba. https://orcid.org/0000-0001-9854-8688
Yaima Zúñiga-Rosales, physician specializing in immunology. Associate professor and adjunct researcher, CNGM, Havana, Cuba. https://orcid.org/0000-0001-9483-9971
María de los Ángeles González-Torres, engineer specializing in information science. Adjunct researcher, CNGM, Havana, Cuba. https://orcid.org/0000-0002-7793-507X
Yudelmis Álvarez-Gavilán, biologist with a master’s degree in medical genetics. Associate professor and associate researcher, CNGM, Havana, Cuba. https://orcid.org/0000-0003-4990-9023
Bárbara Torres-Rives, physician specializing in immunology with a master’s degree in medical genetics. Associate professor and associate researcher, CNGM, Havana, Cuba. https://orcid.org/0000-0001-9729-5172
Yudelkis Benítez-Codero, physician specializing in clinical genetics, with a master’s degree in clinical genetics. Assistant professor and adjunct researcher, CNGM, Havana, Cuba. https://orcid.org/0000-0002-9688-7501
Giselle Monzón-Benítez, physician specializing in clinical genetics. Assistant professor and adjunct researcher, CNGM, Havana, Cuba. https://orcid.org/0000-0001-9324-0772
Luis Carlos Silva-Ayçaguer, mathematician with a doctorate in the mathematical sciences and an advanced doctorate in science. Senior professor and senior researcher, National School of Public Health, Havana, Cuba. https://orcid.org/0000-0002-0734-0054
Beatriz Marcheco-Teruel, physician specializing in clinical genetics with a doctorate in medical sciences. Senior professor and senior researcher, CNGM, Havana, Cuba. https://orcid.org/0000-0001-6009-0405
Submitted: October 04, 2021 Approved: April 04, 2022 Disclosures: None
Pereira-Roche N, Roblejo-Balbuena H, Marín-Padrón LC, Izaguirre-Rodríguez R, Sotmomayor-Lugo F, Zúñiga-Rosales Y, et al. Hematological alterations in patients recovered from SARS-CoV-2 infection in Havana, Cuba. MEDICC Rev. 2022 Apr;24(2):7–14. https://doi.org/10.37757/mr2021.v24.n2.1
No new Early Online articles at this time. The most recent articles are listed in the Current Issue Table of Contents. Early Online articles are added as soon as they are available, so please check back later.