
One Year of the COVID-19 Pandemic in Dental Medical Facilities in Germany: A Questionnaire-Based Analysis


 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
3. Results
3.1. Sample
3.2. Healthcare Worker Status
3.3. Source of Infection
3.4. Pre-Interventional Testing
3.5. Personal Protective Equipment
3.6. Types of Procedures
3.7. Air Ventilation Systems
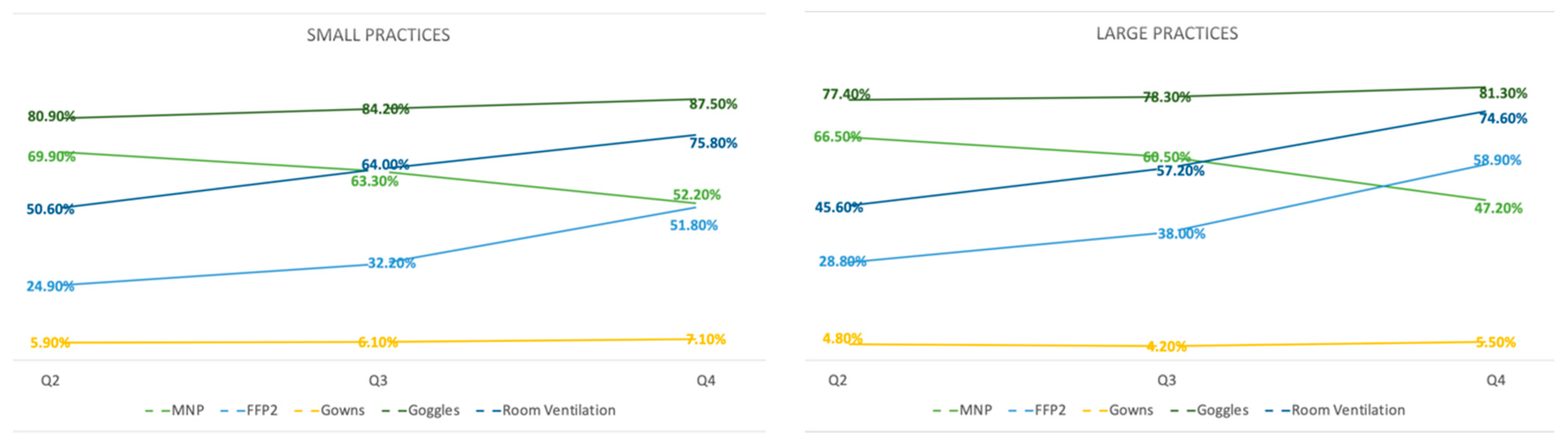
3.8. Development of Procedures
3.9. Economic Revenue and Employee Numbers
3.10. Vaccination Readiness
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Cucinotta, D.; Vanelli, M. WHO Declares COVID-19 a Pandemic. Acta Biomed. 2020, 91, 157–160. [Google Scholar] [PubMed]
- Budweiser, S.; Baş, S.; Jörres, R.A.; Engelhardt, S.; Thilo, C.; Delius, S.V.; Eckel, F.; Biller, U.; Lenherr, K.; Deerberg-Wittram, J.; et al. Comparison of the First and Second Waves of Hospitalized Patients with SARS-CoV-2. Dtsch. Arztebl. Int. 2021, 118, 326–327. [Google Scholar] [PubMed]
- Aufklärung, B.F.G. Bundeszentrale für Gesundheitliche Aufklärung. 2021. Available online: https://www.infektionsschutz.de/coronavirus/alltag-in-zeiten-von-corona.html (accessed on 12 May 2021).
- Erdem, H.; Lucey, D.R. Healthcare worker infections and deaths due to COVID-19: A survey from 37 nations and a call for WHO to post national data on their website. Int. J. Infect. Dis. 2021, 102, 239–241. [Google Scholar] [CrossRef] [PubMed]
- Dong, E.; Du, H.; Gardner, L. An interactive web-based dashboard to track COVID-19 in real time. Lancet Infect. Dis. 2020, 20, 533–534. [Google Scholar] [CrossRef]
- Supady, A.; Curtis, J.R.; Abrams, D.; Lorusso, R.; Bein, T.; Boldt, J.; Brown, C.E.; Duerschmied, D.; Metaxa, V.; Brodie, D.; et al. Allocating scarce intensive care resources during the COVID-19 pandemic: Practical challenges to theoretical frameworks. Lancet Respir. Med. 2021, 9, 430–434. [Google Scholar] [CrossRef]
- Melman, G.J.; Parlikad, A.K.; Cameron, E.A.B. Balancing scarce hospital resources during the COVID-19 pandemic using discrete-event simulation. Health Care Manag. Sci. 2021, 24, 356–374. [Google Scholar] [CrossRef] [PubMed]
- Schwaben, Z.B. Zahnärztliche Nachrichten Schwaben. April 2020. Ausgabe 4-20. Available online: https://www.zbv-schwaben.de/wp-content/uploads/2020/03/ZNS-4-2020.pdf (accessed on 13 November 2021).
- Gallagher, J.E.; Sukriti, K.C.; Johnson, I.G.; Al-Yaseen, W.; Jones, R.; McGregor, S.; Robertson, M.; Harris, R.; Innes, N.; Wade, W.G. A systematic review of contamination (aerosol, splatter and droplet generation) associated with oral surgery and its relevance to COVID-19. BDJ Open 2020, 6, 1–17. [Google Scholar] [CrossRef] [PubMed]
- Khader, Y.; Nsour, M.A.; Al-Batayneh, O.B.; Saadeh, R.; Bashier, H.; Alfaqih, M.; AlShurman, B.A.; Abed, R.E.; Alkhatib, Z.; Samaranayake, L.P. Dentists’ Awareness, Perception, and Attitude Regarding COVID-19 and Infection Control: Cross-Sectional Study among Jordanian Dentists. JMIR Public Health Surveill. 2020, 6, e18798. [Google Scholar] [CrossRef] [PubMed]
- Jamal, M.; Shah, M.; Almarzooqi, S.H.; Aber, H.; Khawaja, S.; El Abed, R.; Alkhatib, Z.; Samaranayake, L.P. Overview of transnational recommendations for COVID-19 transmission control in dental care settings. Oral Dis. 2021, 27 (Suppl. 3), 655–664. [Google Scholar] [CrossRef] [PubMed]
- Bundeszahnärztekammer. Klartext 10/19. Available online: https://www.bzaek.de/fileadmin/PDFs/klartext/19/191029_KT_10.pdf (accessed on 13 November 2021).
- Boger, B.; Fachi, M.M.; Vilhena, R.O.; Cobre, A.F.; Tonin, F.S.; Pontarolo, R. Systematic review with meta-analysis of the accuracy of diagnostic tests for COVID-19. Am. J. Infect. Control 2021, 49, 21–29. [Google Scholar] [CrossRef] [PubMed]
- DGZMK. Umgang Mit Zahnmedizinischen Patienten Bei Belastung Mit Aerosol-übertragbaren Erregern, Langversion, 2020, AWMF-Registiernummer: 083-046. Available online: https://www.awmf.org/leitlinien/detail/II/083-046.html (accessed on 13 November 2021).
- Barabari, P.; Moharamzadeh, K. Novel Coronavirus (COVID-19) and Dentistry-A Comprehensive Review of Literature. Dent. J. 2020, 8, 53. [Google Scholar] [CrossRef] [PubMed]
- Römmele, C.; Ebigbo, A.; Kahn, M.; Zellmer, S.; Muzalyova, A.; Hammel, G.; Bartenschlager, C.; Beyer, A.; Rosendahl, J.; Schlittenbauer, T.; et al. Health-care workers in gastrointestinal endoscopy are at higher risk for SARS-CoV-2 infection compared to other aerosol-generating disciplines. MedRxiv 2021. [Google Scholar] [CrossRef]
- Sozkes, S.; Olszewska-Czyz, I. Effects of COVID-19 Pandemic on Working Conditions of Dentists in Poland and Turkey. Medicina 2021, 57, 1082. [Google Scholar] [CrossRef] [PubMed]
- Sinjari, B.; Rexhepi, I.; Santilli, M.; D’Addazio, G.; Chiacchiaretta, P.; Carlo, P.D.; Caputi, S. The Impact of COVID-19 Related Lockdown on Dental Practice in Central Italy-Outcomes of A Survey. Int. J. Environ. Res. Public Health 2020, 17, 5780. [Google Scholar] [CrossRef] [PubMed]
- DGZMK. Umgang Mit Zahnmedizinischen Patienten bei Belastung Mit Aerosol-übertragbaren Erregern, Langfassung 2.0, 2021, AWMF-Registiernummer: 083-046. Available online: https://www.awmf.org/leitlinien/detail/ll/083-046LG.html (accessed on 13 November 2021).
- Tzoutzas, I.; Maltezou, H.C.; Barmparesos, N.; Tasios, P.; Efthymiou, C.; Assimakopoulos, M.N.; Tseroni, M.; Vorou, R.; Tzermpos, F.; Antoniadou, M.; et al. Indoor Air Quality Evaluation Using Mechanical Ventilation and Portable Air Purifiers in an Academic Dentistry Clinic during the COVID-19 Pandemic in Greece. Int. J. Environ. Res. Public Health 2021, 18, 8886. [Google Scholar] [CrossRef] [PubMed]
- Ren, Y.-F.; Huang, Q.; Marzouk, T.; Richard, R.; Pembroke, K.; Martone, P.; Venner, T.; Malmstrom, H.; Eliav, E. Effects of mechanical ventilation and portable air cleaner on aerosol removal from dental treatment rooms. J. Dent. 2021, 105, 103576. [Google Scholar] [CrossRef] [PubMed]
- Teichert-Filho, R.; Baldasso, C.N.; Campos, M.M.; Gomes, M.S. Protective device to reduce aerosol dispersion in dental clinics during the COVID-19 pandemic. Int. Endod. J. 2020, 53, 1588–1597. [Google Scholar] [CrossRef] [PubMed]
- Sarapultseva, M.; Hu, D.; Sarapultsev, A. SARS-CoV-2 Seropositivity among Dental Staff and the Role of Aspirating Systems. JDR Clin. Trans. Res. 2021, 6, 132–138. [Google Scholar] [CrossRef] [PubMed]
- Schwendicke, F.; Krois, J.; Gomez, J. Impact of SARS-CoV2 (COVID-19) on dental practices: Economic analysis. J. Dent. 2020, 99, 103387. [Google Scholar] [CrossRef] [PubMed]
- Wolf, T.G.; Deschner, J.; Schrader, H.; Bührens, P.; Kaps-Richter, G.; Cagetti, M.G. Dental Workload Reduction during First SARS-CoV-2/COVID-19 Lockdown in Germany: A cross-sectional Survey. Int. J. Environ. Res. Public Health 2021, 18, 3164. [Google Scholar] [CrossRef]
- KZVB, E. March 22nd 2021 Statement, “Pandemiezuschlag” für Vertragszahnärztliche Praxen. Available online: https://www.kzbv.de/informationen-fuer-praxen.1371.de.html (accessed on 19 May 2021).
- Robert-Koch-Institut, Impfquotenmonitoring. Available online: https://www.rki.de/DE/Content/InfAZ/N/Neuartiges_Coronavirus/Daten/Impfquoten-Tab.html (accessed on 21 June 2021).


{kind=link}
| N | % | ||
|---|---|---|---|
| Total | 1114 | 100 | |
| Hospital | 20 | 1.8 | |
| Private Practice | 1094 | 98.2 | |
| Small (<600 ppq) | 425 | 38.2 | |
| Large (>600 ppq) | 669 | 60.1 |
| Employees (Total) | Employees (SARS-CoV-2-Positive) | |||||
|---|---|---|---|---|---|---|
| N | HCW | N | HCW | Rate of SARS-CoV-2-Positive HCWs | p | |
| Hospital | 20 | 670 | 6 | 14 | 2.1 | <0.01 |
| Private Practice | 1094 | 11,334 | 235 | 382 | 3.4 | |
| Small (<600 ppq) | 425 | 2534 | 61 | 78 | 3.1 | n.s. |
| Large (>600 ppq) | 669 | 8800 | 175 | 304 | 3.5 | |
| Overall | 1114 | 12,004 | 241 | 396 | 3.3 | |
| Private Practices | ||||||
|---|---|---|---|---|---|---|
| Small (<600 ppq) | Large (>600 ppq) | |||||
| N | % | N | % | p | ||
| Total | 425 | 100.0 | 669 | 100.0 | ||
| Facilities with no SARS-CoV-2-positive HCW | 364 | 85.6 | 494 | 73.8 | ||
| Facilities with SARS-CoV-2-positive HCWs | 61 | 14.4 | 175 | 26.2 | <0.01 | |
| During interventions | 0 | 0.0 | 3 | 1.7 | n.s. | |
| At work (with patient contact) | 0 | 0.0 | 4 | 2.3 | n.s. | |
| At work (without patient contact) | 7 | 11.5 | 7 | 4.0 | n.s. | |
| Unclear origin | 7 | 11.5 | 22 | 12.6 | n.s. | |
| Private environment | 56 | 91.8 | 157 | 89.7 | <0.01 | |
| Private Practices | ||||||
|---|---|---|---|---|---|---|
| Small (<600 ppq) | Large (>600 ppq) | |||||
| N | % | N | % | p | ||
| Total | 425 | 100 | 669 | 100 | n.s. | |
| Internal PCR | 0 | 0.0 | 4 | 0.6 | n.s. | |
| Internal antigen | 20 | 4.7 | 25 | 3.7 | n.s. | |
| External PCR | 6 | 1.4 | 5 | 0.7 | n.s. | |
| External antigen | 2 | 0.5 | 6 | 0.9 | n.s. | |
| No testing | 397 | 93.4 | 629 | 94.0 | n.s. | |
| Private Practices | ||||||
|---|---|---|---|---|---|---|
| Share of Procedures | Small (<600 ppq) | Large (>600 ppq) | p-Value | |||
| % | N | % | N | % | ||
| Aerosol-generating procedures | 425 | 100 | 669 | 100 | ||
| <20 | 205 | 48.2 | 293 | 43.8 | n.s. | |
| 20–<40 | 152 | 35.8 | 254 | 38.0 | n.s. | |
| 40–<60 | 48 | 11.3 | 91 | 13.6 | n.s. | |
| 60–<80 | 12 | 2.8 | 21 | 3.1 | n.s. | |
| >80 | 8 | 1.9 | 10 | 1.5 | n.s. | |
| Rubber dam | 425 | 100 | 669 | 100 | ||
| <20 | 283 | 66.6 | 479 | 71.6 | n.s. | |
| 20–<40 | 69 | 16.2 | 111 | 16.6 | n.s. | |
| 40–<60 | 36 | 8.5 | 47 | 7.0 | n.s. | |
| 60–<80 | 20 | 4.7 | 18 | 2.7 | n.s. | |
| >80 | 17 | 4.0 | 14 | 2.1 | n.s. | |
| Private Practices | ||||||
|---|---|---|---|---|---|---|
| Small (<600 ppq) | Large (>600 ppq) | p-Value | ||||
| N | % | N | % | |||
| Total | 423 | 100 | 666 | 100 | ||
| Yes | 185 | 43.7 | 339 | 50.9 | <0.05 | |
| Air handling units (AHU) in the recirculation mode | 25 | 13.5 | 60 | 17.7 | n.s. | |
| Air handling units (AHU) with air filter (e.g., HEPA filter) with/without recirculation mode | 71 | 38.4 | 136 | 40.1 | n.s. | |
| Fans/mobile air conditioners without air filter/fan heaters | 53 | 28.6 | 78 | 23.0 | n.s. | |
| Other types | 24 | 13.0 | 38 | 11.2 | n.s. | |
| Unknown | 12 | 6.5 | 27 | 8.0 | n.s. | |
| No | 237 | 56.0 | 319 | 47.9 | <0.01 | |
| Unknown | 1 | 0.2 | 8 | 1.2 | n.s. | |
| Private Practices | ||||||
|---|---|---|---|---|---|---|
| Small (<600 ppq) | Large (>600 ppq) | |||||
| N | % | N | % | p | ||
| Total | 424 | 100.0 | 664 | 100.0 | ||
| Increase over 50% | 10 | 2.4 | 11 | 1.7 | n.s. | |
| Increase less than 50% | 24 | 5.7 | 45 | 6.8 | n.s. | |
| Stable | 144 | 34.0 | 307 | 46.2 | <0.01 | |
| Decrease less than 50% | 223 | 52.6 | 295 | 44.4 | <0.01 | |
| Decrease over 50% | 23 | 5.4 | 6 | 0.9 | <0.01 | |
| Private Practice | ||||||
|---|---|---|---|---|---|---|
| Small (<600 ppq) | Large (>600 ppq) | |||||
| N | % | N | % | p | ||
| Revenue | 423 | 100 | 667 | 100 | ||
| Increase over 50% | 3 | 0.7 | 0 | 0 | n.s. | |
| Increase less than 50% | 16 | 3.8 | 59 | 8.8 | <0.01 | |
| Stable | 105 | 24.8 | 228 | 34.2 | <0.01 | |
| Decrease less than 50% | 273 | 64.5 | 369 | 55.3 | <0.05 | |
| Decrease over 50% | 26 | 6.1 | 11 | 1.6 | <0.01 | |
| Employees | 425 | 100 | 669 | 100 | ||
| Increase | 26 | 6.1 | 68 | 10.2 | <0.05 | |
| Stable | 321 | 75.5 | 514 | 76.8 | n.s. | |
| Decrease | 78 | 18.4 | 87 | 13 | <0.05 | |
| Private Practice | ||||||
|---|---|---|---|---|---|---|
| Vaccination Readiness | Small (<600 ppq) | Large (>600 ppq) | ||||
| % | N | % | N | % | p | |
| Total | 425 | 100 | 669 | 100 | ||
| <20 | 27 | 6.4 | 40 | 6.0 | n.s. | |
| 20–<40 | 46 | 10.8 | 70 | 10.5 | n.s. | |
| 40–<60 | 101 | 23.8 | 154 | 23.0 | n.s. | |
| 60–<80 | 91 | 21.4 | 213 | 31.8 | <0.01 | |
| 80–100 | 160 | 37.6 | 192 | 28.7 | <0.01 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zellmer, S.; Bachmann, E.; Muzalyova, A.; Ebigbo, A.; Kahn, M.; Traidl-Hoffmann, C.; Frankenberger, R.; Eckstein, F.M.; Ziebart, T.; Meisgeier, A.; et al. One Year of the COVID-19 Pandemic in Dental Medical Facilities in Germany: A Questionnaire-Based Analysis. Int. J. Environ. Res. Public Health 2022, 19, 175. https://doi.org/10.3390/ijerph19010175
Zellmer S, Bachmann E, Muzalyova A, Ebigbo A, Kahn M, Traidl-Hoffmann C, Frankenberger R, Eckstein FM, Ziebart T, Meisgeier A, et al. One Year of the COVID-19 Pandemic in Dental Medical Facilities in Germany: A Questionnaire-Based Analysis. International Journal of Environmental Research and Public Health. 2022; 19(1):175. https://doi.org/10.3390/ijerph19010175
Chicago/Turabian StyleZellmer, Stephan, Ella Bachmann, Anna Muzalyova, Alanna Ebigbo, Maria Kahn, Claudia Traidl-Hoffmann, Roland Frankenberger, Fabian M. Eckstein, Thomas Ziebart, Axel Meisgeier, and et al. 2022. "One Year of the COVID-19 Pandemic in Dental Medical Facilities in Germany: A Questionnaire-Based Analysis" International Journal of Environmental Research and Public Health 19, no. 1: 175. https://doi.org/10.3390/ijerph19010175