
Convalescent Plasma Therapy, Therapeutic Formulations of Repurposed Drugs in 20th Century Epidemics against COVID-19: A Systematic Review

 ,
, 
Abstract
:1. Introduction
2. Method
2.1. Search Strategy and Study Selection
2.2. Selection of Articles: Inclusion Criteria
2.3. Assessment of Methodological Quality
2.4. Data Extraction
3. Results
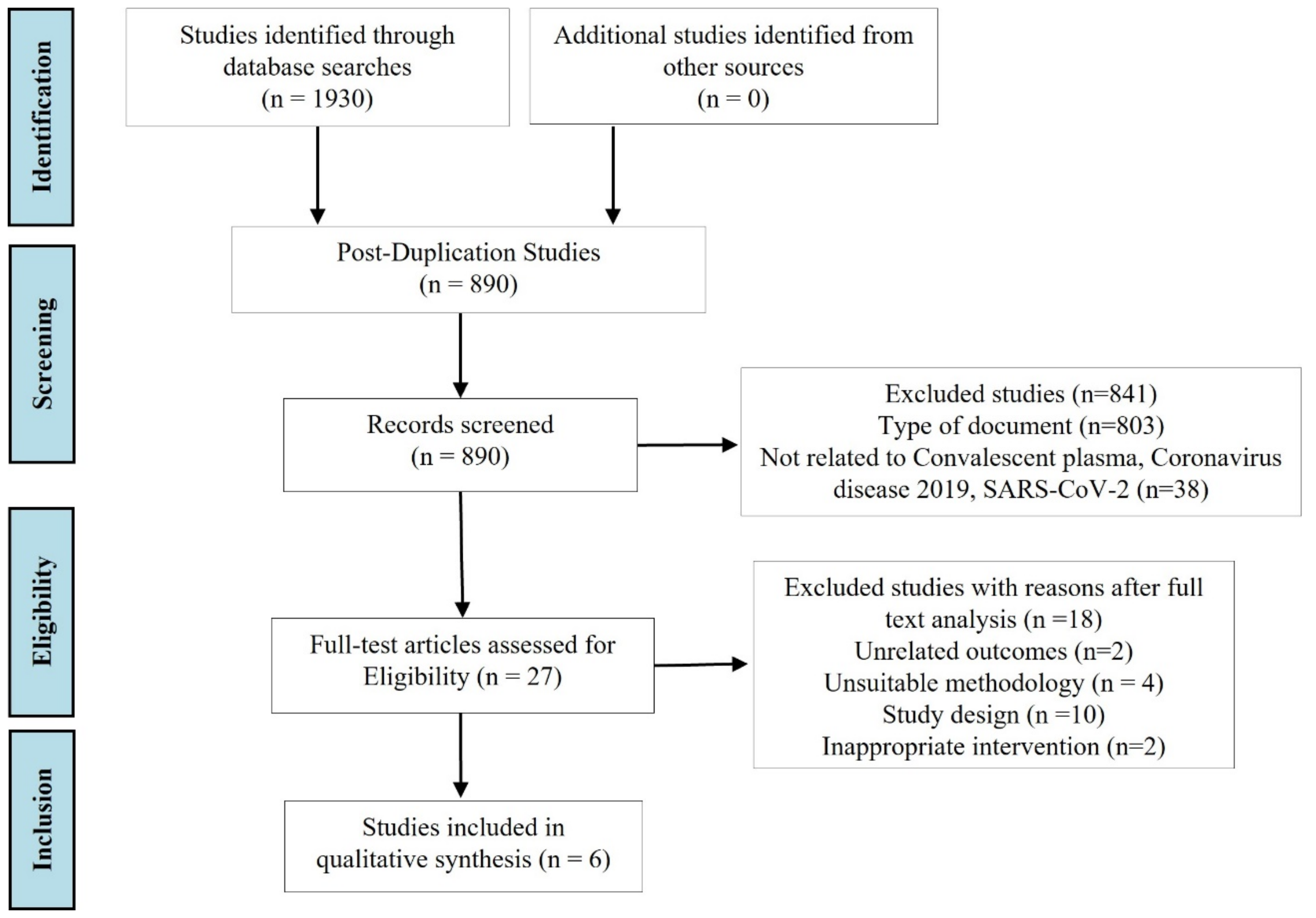
3.1. Selection of Studies
3.2. Results of the Quality Assessment
3.3. Descriptive Information of the Selected Articles Included in the Systematic Review
3.4. Clinical Measures
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A. Search Terms Used for the Selection of Articles
- #1 “convalescent plasma”[Mesh]
- #2 “antibodies”[tiab] OR “blood transfusion”[tiab] OR “immunoglobulins”[tiab] OR “neutralizing antibodies”[tiab] OR “cytokines”[tiab] OR “plasma therapy” [tiab]
- #3 #1 OR #2
- #4 “COVID-19”[Mesh]
- #5 “SARS-CoV-2”[tiab] OR “coronavirus”[tiab] OR “Coronavirus disease 2019”[tiab] OR “acute respiratory syndrome coronavirus 2”[tiab]
- #6 #4 OR #5
- #7 “patients hospitalized”[Mesh]
- #8 “critically ill patients”[tiab] OR “immune response”[tiab] OR “Survival rate”[tiab]OR “duration of infection”[tiab] OR “Virus shedding”[tiab] OR “disease progression”[tiab] OR “oxygen therapy”[tiab] OR “mortality”[tiab]
- #9 #7 OR #8
- #20 #3 AND #6 AND #9 AND
References
- Fernández-Lázaro, D.; Sánchez-Serrano, N.; Mielgo-Ayuso, J.; Luis García-Hernández, J.; González-Bernal, J.J.; Seco-Calvo, J. Long COVID a New Derivative in the Chaos of SARS-CoV-2 Infection: The Emergent Pandemic? J. Clin. Med. 2021, 10, 5799. [Google Scholar] [CrossRef] [PubMed]
- Fernández Lázaro, D.; Sanz Gómez, N.; Sánchez Serrano, N.; Alaoui Sosse, A.; Aldea Mansilla, C. Estandarización de Emergencia para el Diagnóstico del virus SARS-CoV-2 mediante la Reacción en Cadena de la Polimerasa de Transcripción Reversa en Tiempo Real (RT-PCR) en situación de pandemia de COVID-19. Rev. Madrileña Salud Pública 2020, 4, 1–11. [Google Scholar] [CrossRef]
- Fernández-Lázaro, D.; Garrosa, M. Identification, Mechanism, and Treatment of Skin Lesions in COVID-19: A Review. Viruses 2021, 13, 1916. [Google Scholar] [CrossRef] [PubMed]
- Fernández-Lázaro, D.; Fernandez-Lazaro, C.I.; Mielgo-Ayuso, J.; Adams, D.P.; García Hernández, J.L.; González-Bernal, J.; González-Gross, M. Glycophosphopeptical AM3 Food Supplement: A Potential Adjuvant in the Treatment and Vaccination of SARS-CoV-2. Front. Immunol. 2021, 12, 698672. [Google Scholar] [CrossRef] [PubMed]
- Migo, W.; Boskovic, M.; Likic, R. The development of biologics to target SARS-CoV2: Treatment potential of antibodies in patient groups with poor immune response. Curr. Res. Pharmacol. Drug Discov. 2021, 2, 100064. [Google Scholar] [CrossRef] [PubMed]
- Centers for Disease Control and Prevention. Vaccines for COVID-19|CDC. 2022. Available online: https://www.cdc.gov/coronavirus/2019-ncov/vaccines/index.html (accessed on 16 January 2022).
- Döbler, N.A.; Carbon, C.-C. Vaccination against SARS-CoV-2: A human enhancement story. Transl. Med. Commun. 2021, 6, 27. [Google Scholar] [CrossRef] [PubMed]
- COVID-19 Map—Johns Hopkins Coronavirus Resource Center. 2022. Available online: https://coronavirus.jhu.edu/map.html (accessed on 27 January 2022).
- Sharma, A.; Tiwari, S.; Deb, M.K.; Louis Marty, J. Severe acute respiratory syndrome coronavirus-2 (SARS-CoV-2): A global pandemic and treatment strategies. Int. J. Antimicrob. Agents 2020, 56, 106054. [Google Scholar] [CrossRef]
- Sanders, J.M.; Monogue, M.L.; Jodlowski, T.Z.; Cutrell, J.B. Pharmacologic Treatments for Coronavirus Disease 2019 (COVID-19): A Review. JAMA 2020, 323, 1824–1836. [Google Scholar] [CrossRef]
- Cheng, Y.; Wong, R.; Soo, Y.O.Y.; Wong, W.S.; Lee, C.K.; Ng, M.H.L.; Chan, P.; Wong, K.C.; Leung, C.B.; Cheng, G. Use of convalescent plasma therapy in SARS patients in Hong Kong. Eur. J. Clin. Microbiol. Infect. Dis. 2005, 24, 44–46. [Google Scholar] [CrossRef]
- Ko, J.H.; Seok, H.; Cho, S.Y.; Ha, Y.E.; Baek, J.Y.; Kim, S.H.; Kim, Y.J.; Park, J.K.; Chung, C.R.; Kang, E.S.; et al. Challenges of convalescent plasma infusion therapy in Middle East respiratory coronavirus infection: A single centre experience. Antivir. Ther. 2018, 23, 617–622. [Google Scholar] [CrossRef]
- Lee, P.I.; Hsueh, P.R. Emerging threats from zoonotic coronaviruses-from SARS and MERS to 2019-nCoV. J. Microbiol. Immunol. Infect. 2020, 53, 365–367. [Google Scholar] [CrossRef]
- Rojas, M.; Rodríguez, Y.; Monsalve, D.M.; Acosta-Ampudia, Y.; Camacho, B.; Gallo, J.E.; Rojas-Villarraga, A.; Ramírez-Santana, C.; Díaz-Conrado, J.C.; Manrique, R.; et al. Convalescent plasma in Covid-19: Possible mechanisms of action. Autoimmun. Rev. 2020, 19, 102554. [Google Scholar] [CrossRef]
- Roback, J.D.; Guarner, J. Convalescent Plasma to Treat COVID-19: Possibilities and Challenges. JAMA 2020, 323, 1561–1562. [Google Scholar] [CrossRef] [Green Version]
- Garraud, O.; Heshmati, F.; Pozzetto, B.; Lefrere, F.; Girot, R.; Saillol, A.; Laperche, S. Plasma therapy against infectious pathogens, as of yesterday, today and tomorrow. Transfus. Clin. Biol. 2016, 23, 39–44. [Google Scholar] [CrossRef]
- Fernández-Lázaro, D.; González-Bernal, J.J.; Sánchez-Serrano, N.; Navascués, L.J.; Del Río, A.A.; Mielgo-Ayuso, J. Physical Exercise as a Multimodal Tool for COVID-19: Could It Be Used as a Preventive Strategy? Int. J. Environ. Res. Public Health 2020, 17, 8496. [Google Scholar] [CrossRef]
- Duan, K.; Liu, B.; Li, C.; Zhang, H.; Yu, T.; Qu, J.; Zhou, M.; Chen, L.; Meng, S.; Hu, Y.; et al. Effectiveness of convalescent plasma therapy in severe COVID-19 patients. Proc. Natl. Acad. Sci. USA 2020, 117, 9490–9496. [Google Scholar] [CrossRef] [Green Version]
- Shen, C.; Wang, Z.; Zhao, F.; Yang, Y.; Li, J.; Yuan, J.; Wang, F.; Li, D.; Tang, M.; Xing, L.; et al. Treatment of 5 Critically Ill Patients with COVID-19 with Convalescent Plasma. JAMA 2020, 323, 1582–1589. [Google Scholar] [CrossRef]
- Piechotta, V.; Chai, K.L.; Valk, S.J.; Doree, C.; Monsef, I.; Wood, E.M.; Lamikanra, A.; Kimber, C.; McQuilten, Z.; So-Osman, C.; et al. Convalescent plasma or hyperimmune immunoglobulin for people with COVID-19: A living systematic review. Cochrane Database Syst. Rev. 2020, 7, CD013600. Available online: https://pubmed.ncbi.nlm.nih.gov/32648959/ (accessed on 26 January 2020).
- China NHC of the PR of Diagnosis and Treatment of COVID-19 (Trial 8th Edition). 2022. Available online: http://www.nhc.gov.cn/yzygj/s7653p/202008/0a7bdf12bd4b46e5bd28ca7f9a7f5e5a.shtml (accessed on 27 January 2022).
- Fernández-Lázaro, D.; Mielgo-Ayuso, J.; Lázaro Asensio, M.P.; Córdova Martínez, A.; Caballero-García, A.; Fernanadez-Lazaro, C.I. Intradialytic physical exercise in chronic kidney disease: A systematic review of health outcomes. Arch. Med. Deporte 2020, 37, 419–429. [Google Scholar] [CrossRef]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gøtzsche, P.C.; Ioannidis, J.P.A.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: Explanation and elaboration. PLoS Med. 2009, 6, e1000100. [Google Scholar] [CrossRef]
- Law, M.; Stewart, C.; Pollock, N.; Letts, L.; Bosch, J.; Westmorland, M. Guidelines for Critical Review of Qualitative Studies; McMaster University Occupational Therapy Evidence-Based Practice Research Group: Hamilton, ON, Canada, 1998; pp. 1–9. [Google Scholar]
- Liu, S.T.H.; Lin, H.M.; Baine, I.; Wajnberg, A.; Gumprecht, J.P.; Rahman, F.; Rodriguez, D.; Tandon, P.; Bassily-Marcus, A.; Bander, J.; et al. Convalescent plasma treatment of severe COVID-19: A propensity score–matched control study. Nat. Med. 2020, 26, 1708–1713. [Google Scholar] [CrossRef]
- Zeng, Q.; Yu, Z.; Gou, J.; Li, G.; Ma, S.H.; Zhang, G.F.; Xu, J.H.; Lin, W.B.; Zhang, M.M.; Li, C.; et al. Effect of convalescent plasma therapy on viral shedding and survival in patients with coronavirus disease 2019. J. Infect. Dis. 2020, 222, 38–43. [Google Scholar] [CrossRef]
- Libster, R.; Pérez Marc, G.; Wappner, D.; Coviello, S.; Bianchi, A.; Braem, V.; Esteban, I.; Caballero, M.T.; Wood, C.; Berrueta, M.; et al. Early High-Titer Plasma Therapy to Prevent Severe COVID-19 in Older Adults. N. Engl. J. Med. 2021, 384, 610–618. [Google Scholar] [CrossRef]
- Simonovich, V.A.; Burgos Pratx, L.D.; Scibona, P.; Beruto, M.V.; Vallone, M.G.; Vázquez, C.; Savoy, N.; Giunta, D.H.; Pérez, L.G.; Sanchez, M.d.L.; et al. A Randomized Trial of Convalescent Plasma in COVID-19 Severe Pneumonia. N. Engl. J. Med. 2021, 384, 619–629. [Google Scholar]
- Li, L.; Zhang, W.; Hu, Y.; Tong, X.; Zheng, S.; Yang, J.; Kong, Y.; Ren, L.; Wei, Q.; Mei, H.; et al. Effect of convalescent plasma therapy on time to clinical improvement in patients with severe and life-threatening COVID-19: A randomized clinical trial. JAMA 2020, 324, 460–470. [Google Scholar] [CrossRef]
- Rasheed, A.; Fatak, D.; Hashim, H.; Maulood, M.F.; Kabah, K.K.; Almusawi, Y.A.; Abdulamir, A.S. The therapeutic potential of convalescent plasma therapy on treating critically ill COVID-19 patients residing in respiratory care units in hospitals in Baghdad. Infez. Med. 2020, 28, 357–366. [Google Scholar]
- Wooding, D.J.; Bach, H. Treatment of COVID-19 with convalescent plasma: Lessons from past coronavirus outbreaks. Clin. Microbiol. Infect. 2020, 26, 1436–1446. [Google Scholar] [CrossRef] [PubMed]
- Bloch, E.M.; Shoham, S.; Casadevall, A.; Sachais, B.S.; Shaz, B.; Winters, J.L.; van Buslirk, C.; Grosssman, B.J.; Joyner, M.; Henderson, J.P.; et al. Deployment of convalescent plasma for the prevention and treatment of COVID-19. J. Clin. Investig. 2020, 130, 2757–2765. [Google Scholar] [CrossRef] [Green Version]
- Estcourt, L.J. Passive immune therapies: Another tool against COVID-19. Hematol. Am. Soc. Hematol. Educ. Progr. 2021, 1, 628–641. [Google Scholar] [CrossRef] [PubMed]
- US Food and Drug. Recommendations for Investigational COVID-19 Convalescent Plasma|FDA. 2022. Available online: https://www.fda.gov/vaccines-blood-biologics/investigational-new-drug-applications-inds-cber-regulated-products/recommendations-investigational-covid-19-convalescent-plasma (accessed on 20 January 2022).
- Venkateswaran, T.V.S.J. India to Explore Novel Blood Plasma Therapy for COVID-19—The Hindu BusinessLine. 2022. Available online: https://www.thehindubusinessline.com/news/science/india-to-explore-novel-blood-plasma-therapy-for-covid-19/article31311466.ece (accessed on 27 January 2022).
- Llover, M.N.; Jiménez, M.C. Current status of treatments for COVID-19. FMC 2021, 28, 40–56. [Google Scholar] [PubMed]
- Diariofarma. EU Earmarks 36 Million for Projects to Collect Plasma from Convalescent Patients Recovered from COVID-19|@diariofarma. 2022. Available online: https://www.diariofarma.com/2021/01/11/la-ue-destina-36-millones-a-proyectos-para-recoger-plasma-de-convalecientes-recuperados-de-covid-19 (accessed on 27 January 2022).
- Wang, Y.; Huo, P.; Dai, R.; Lv, X.; Yuan, S.; Zhang, Y.; Guo, Y.; Li, R.; Yu, Q.; Zhu, K. Convalescent plasma may be a possible treatment for COVID-19: A systematic review. Int. Immunopharmacol. 2021, 9, 107262. [Google Scholar] [CrossRef]
- Wang, M.; Yang, X.; Yang, F.; Zhu, X.; Sun, Z.; Bao, P.; Yan, Y. Convalescent plasma therapy in critically ill coronavirus disease 2019 patients with persistently positive nucleic acid test, case series report. Medicine 2020, 99, e21596. [Google Scholar] [CrossRef]
- Joyner, M.J.; Bruno, K.A.; Klassen, S.A.; Kunze, K.L.; Johnson, P.W.; Lesser, E.R.; Wiggins, C.C.; Senefeld, J.W.; Klompas, A.M.; Hodge, D.O.; et al. Safety Update: COVID-19 Convalescent Plasma in 20,000 Hospitalized Patients. Mayo Clin. Proc. 2020, 95, 1888–1897. [Google Scholar] [CrossRef]
- Jafari, R.; Jonaidi-Jafari, N.; Dehghanpoor, F.; Saburi, A. Convalescent plasma therapy in a pregnant COVID-19 patient with a dramatic clinical and imaging response: A case report. World J. Radiol. 2020, 12, 137–141. [Google Scholar] [CrossRef]
- Zhang, B.; Liu, S.; Tan, T.; Huang, W.; Dong, Y.; Chen, L.; Che, Q.; Zhang, L.; Zhong, Q.; Zhang, X.; et al. Treatment with Convalescent Plasma for Critically Ill Patients with Severe Acute Respiratory Syndrome Coronavirus 2 Infection. Chest 2020, 158, e9. [Google Scholar] [CrossRef]
- Rajendran, K.; Krishnasamy, N.; Rangarajan, J.; Rathinam, J.; Natarajan, M.; Ramachandran, A. Convalescent plasma transfusion for the treatment of COVID-19: Systematic review. J. Med. Virol. 2020, 92, 1475–1483. [Google Scholar] [CrossRef]
- Pandey, S.; Vyas, G.N. Adverse effects of plasma transfusion. Transfusion 2012, 52, 65S–79S. [Google Scholar] [CrossRef] [Green Version]
- Chen, X.; Pan, Z.; Yue, S.; Yu, F.; Zhang, J.; Yang, Y.; Li, R.; Liu, B.; Yang, X.; Gao, L.; et al. Disease severity dictates SARS-CoV-2-specific neutralizing antibody responses in COVID-19. Signal Transduct. Target. Ther. 2020, 5, 180. [Google Scholar] [CrossRef]
- Klassen, S.A.; Senefeld, J.W.; Johnson, P.W.; Carter, R.E.; Wiggins, C.C.; Shoham, S.; Grossman, B.J.; Henderson, J.P.; Musser, J.M.; Salazar, E.; et al. The Effect of Convalescent Plasma Therapy on COVID-19 Patient Mortality: Systematic Review and Meta-analysis. Mayo Clin. Proc. 2021, 96, 1262–1275. [Google Scholar] [CrossRef]
- Aviani, J.K.; Halim, D.; Soeroto, A.Y.; Achmad, T.H.; Djuwantono, T. Current views on the potentials of convalescent plasma therapy (CPT) as Coronavirus disease 2019 (COVID-19) treatment: A systematic review and meta-analysis based on recent studies and previous respiratory pandemics. Rev. Med. Virol. 2021, 31, e2225. [Google Scholar] [CrossRef]
- Axfors, C.; Janiaud, P.; Schmitt, A.M.; van’t Hooft, J.; Smith, E.R.; Haber, N.A.; Abayomi, A.; Abduljalil, M.; Abdulrahman, A.; Acosta-Ampudia, Y.; et al. Association between convalescent plasma treatment and mortality in COVID-19: A collaborative systematic review and meta-analysis of randomized clinical trials. BMC Infect. Dis. 2021, 21, 1170. [Google Scholar] [CrossRef] [PubMed]
- Snow, T.A.; Saleem, N.; Ambler, G.; Nastouli, E.; McCoy, L.E.; Singer, M.; Arulkumaran, N. Convalescent plasma for COVID-19: A meta-analysis, trial sequential analysis, and meta-regression. Br. J. Anaesth. 2021, 127, 834–844. [Google Scholar] [CrossRef] [PubMed]
- Troxel, A.B.; Petkova, E.; Goldfeld, K.; Liu, M.; Tarpey, T.; Wu, Y.; Wu, D.; Agarwal, A.; Avendaño-Solá, C.; Bainbridge, E.; et al. Association of Convalescent Plasma Treatment with Clinical Status in Patients Hospitalized with COVID-19: A Meta-analysis. JAMA Netw. Open 2022, 5, e2147331. [Google Scholar] [CrossRef] [PubMed]
- Bacova, B.; Kohutova, Z.; Zubata, I.; Gaherova, L.; Kucera, P.; Heizer, T.; Mikesova, M.; Karel, T.; Novak, J. Cellular and humoral immune response to SARS-CoV-2 mRNA vaccines in patients treated with either Ibrutinib or Rituximab. Clin. Exp. Med. 2022, 29, 1–9. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Author/s | Items | T1 | % | MQ | |||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | 12 | 13 | 14 | 15 | 16 | ||||
| Rasheed et al. [30] | 1 | 1 | 1 | 0 | 1 | 1 | 1 | 1 | 0 | 1 | 1 | 1 | 1 | 1 | 0 | 1 | 13 | 81.25 | VG |
| Li et al. [29] | 1 | 1 | 1 | 1 | 1 | 1 | 0 | 1 | 0 | 1 | 0 | 1 | 1 | 1 | 1 | 0 | 12 | 75 | G |
| Simonovich et al. [28] | 1 | 1 | 1 | 1 | 0 | 1 | 1 | 1 | 1 | 0 | 0 | 1 | 1 | 1 | 0 | 1 | 12 | 75 | G |
| Libster et al. [27] | 0 | 1 | 1 | 1 | 0 | 0 | 1 | 1 | 0 | 0 | 0 | 1 | 1 | 1 | 1 | 1 | 10 | 62.5 | A |
| Zeng et al. [26] | 0 | 1 | 1 | 1 | 0 | 1 | 1 | 0 | 1 | 1 | 1 | 1 | 1 | 0 | 0 | 1 | 11 | 68.75 | G |
| Liu et al. [25] | 1 | 1 | 1 | 1 | 0 | 0 | 1 | 1 | 0 | 0 | 0 | 1 | 1 | 1 | 0 | 1 | 10 | 62.5 | A |
| T2 | 4 | 6 | 6 | 5 | 2 | 4 | 5 | 5 | 2 | 3 | 2 | 6 | 6 | 5 | 2 | 5 | |||
| Characteristics | Type | Study Reference |
|---|---|---|
| Clinical status of hospitalized patient COVID-19 | moderate | [27,28] |
| critical/severe | [25,26,29,30] | |
| Quantity/Volume of convalescent plasma with positive immunoglobulins G (IgG+) | 500 mL | [28] |
| 400 mL | [30] | |
| 300 mL | [26] | |
| 250 mL | [25,27] | |
| 200 mL | [29] | |
| Dose of intravenous transfusion of convalescent plasma | Single dose | [25,26,27,28,29,30] |
| Frequency of intravenous transfusion of convalescent plasma | Continued in 2 h | [30] |
| 10 mL (first 15 min)–100 mL/hour | [29] | |
| Continuous between 1–2 h | [25,27] |
| Author/s—Year—Country | Study Design | Population | Clinical Biomarkers | Results CP vs. CG | Main Conclusions |
|---|---|---|---|---|---|
| Rasheed et al. [30] 2020 Iraq | Randomized controlled clinical trial | Hospitalized patient COVID-19: Clinical status: critical n = 49 → CP = 21; CG = 28 Age: 47–56 years Plasma Donors: <50 years; healthy habits; non-pregnant; without comorbidities and recovered from COVID-19 (two negative tests: test two weeks; test two days before donation). IgG ≥ 1.25 of anti-SARS-CoV-2 IgG antibodies | IgM (day three) | ↑* | Convalescent plasma therapy is an effective mode of therapy if donors with high level of SARS-CoV-2 antibodies are selected and if recipients were at their early stage of critical illness |
| IgG (day three) | ↑* | ||||
| Recovery time | ↓* | ||||
| Duration of infection | ↓* | ||||
| Death rate | ↓* | ||||
| Adverse Events | ↔ | ||||
| Li et al. [29] 2020 China | Randomized controlled clinical trial | Hospitalized patient COVID-19: Clinical status: severe/critical CP: n = 23 severe/29 critical CG: n = 22 severe/29 critical n = 103 → CP: n = 52; CG: n = 51 Age: 62–78 years; Sex: 60♂; 43♀ Plasma Donors: Age: 18–55 years; two negative CPR test results, two weeks from hospital discharge, no Long-COVID-19 symptoms S-RBD–specific IgG ≥1:640 titer | Rate of clinical improvement | Day 7: ↔ Day 14:↑ Day 28: ↑ | Convalescent plasma therapy added to standard treatment, compared with standard treatment alone, did not result in a statistically significant improvement in time to clinical improvement within 28 days |
| Hospital discharge rate | Day 28: ↑ | ||||
| Mortality at 28 days | ↓ | ||||
| Negative rate of SARS-CoV-2 nucleic acid | 24 h: ↑ 48 h: ↑ 72 h: ↑* | ||||
| Adverse Events | ↑ | ||||
| Simonovich et al. [28] 2020 Argentina | Randomized controlled clinical trial → Multicenter & double-blind | Hospitalized patient COVID-19: Clinical status: mild/moderate n = 333 → CP: n = 228; Age: 52–73.5 years; Sex:67♀ 161♂ CG: n = 103; Age: 49–71 years; Sex: 41♀ 62♂ Plasma Donors: A single donor or a pool of two to five donors Specific SARS-CoV-2 IgG ≥ 1:800 titer | Need for invasive ventilatory support | ↔ | No significant differences were observed in clinical status or overall mortality between CP and CG. However, CP was a trend towards improvement but without full recovery of baseline physical function. |
| Oxygen requirement | ↔ | ||||
| Individuals at discharge with full return to baseline physical function | ↔ | ||||
| Discharge without full return to baseline physical function | ↑ | ||||
| Time from intervention to clinical improvement | ↔ | ||||
| Mortality | ↔ | ||||
| Adverse Events | ↔ | ||||
| Libster et al. [27] 2020 Argentina | Randomized controlled clinical trial → double-blind | Hospitalized patient COVID-19: Clinical status: mild/moderate n = 160 → CP: n = 80; Age: 76.4 ± 8.7 years; Sex: 68%♀ 32%♂ CG: n = 80; Age: 77.9 ± 8.4 years; Sex: 58%♀ 42%♂ Plasma Donors: n = 135; SARS-CoV-2 S IgG ≥ 1:1000 titer, Patients SARS-CoV-2 infection ≥10 days and have been asymptomatic for at least three days with two negative PCR tests | Development of severe respiratory disease | ↓* | Early administration of convalescent plasma of titer ≥ 1:1000 against SARS-CoV-2 to mildly infected older adults reduced the progression of COVID-19 and could stimulate recovery of at-risk patients. |
| Development of critical respiratory illness | ↓ | ||||
| IgG (at 24 h) | ↑ | ||||
| Development of critical systemic disease | ↔ | ||||
| Mortality | ↓ | ||||
| Adverse Events | ↔ | ||||
| Zeng et al. [26] 2020 China | Randomized controlled clinical trial | Hospitalized patient COVID-19: Clinical status: severe/critical 100% ICU admission n = 21→ CP: n = 6; Age: 61.5 years (31.5–77.8); Sex:1♀ 5♂ CG: n = 15; Age 73 years (60–79); Sex: 4♀ 11♂ Plasma Donors: Recovered from COVID-19 1 or two weeks ago, two negative COVID-19 tests, SARS-CoV-2 IgM−/IgG+ by gold immunochromatography tests (Innovita Biotech). | Duration of COVID-19 | ↓* | CP therapy could stop SARS-CoV-2 shedding and extend survival in patients with COVID-19. However, cannot reduce the mortality rate in critically ill patients with end-stage disease. CP therapy in critically ill patients with COVD-19 early in the course of disease |
| Viral spread | ↓ | ||||
| Hospital discharges | ↑ | ||||
| Viral load disappearance | ↑* | ||||
| Mortality | ↓ | ||||
| Adverse Events | ↔ | ||||
| Liu et al. [25] 2020 USA | Randomized controlled clinical trial | Hospitalized patient COVID-19: Clinical status: severe/critical Life-threatening COVID-19 → medical criteria n = 195 → CP: n = 39; Age: 55 ± 13 years; Sex: 25♂ 14♀; BMI: 31.7 ± 6 Kg·m−2 CG: n = 156 Plasma Donors: n = 25 Recovered from COVID-19, 2 negative COVID-19 tests, anti-spike SARS-CoV-2 IgG ≥ 1:320 titers | Worsening rate of oxygenation (at 14 days) | ↓* | CP significantly increases survival. CP is most effective in the early phase of the disease with no significant difference between non-intubated and intubated recipient patients |
| Need for oxygen therapy | ↓ | ||||
| Probability of survival | ↑* | ||||
| Death rate in patients with noninvasive ventilation | ↓ | ||||
| Death rate in patients with invasive ventilation | ↔ | ||||
| Adverse Events | ↔ |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fernández-Lázaro, D.; Ortega, C.D.; Sánchez-Serrano, N.; Beddar Chaib, F.; Jerves Donoso, D.; Jiménez-Callejo, E.; Rodríguez-García, S. Convalescent Plasma Therapy, Therapeutic Formulations of Repurposed Drugs in 20th Century Epidemics against COVID-19: A Systematic Review. Pharmaceutics 2022, 14, 1020. https://doi.org/10.3390/pharmaceutics14051020
Fernández-Lázaro D, Ortega CD, Sánchez-Serrano N, Beddar Chaib F, Jerves Donoso D, Jiménez-Callejo E, Rodríguez-García S. Convalescent Plasma Therapy, Therapeutic Formulations of Repurposed Drugs in 20th Century Epidemics against COVID-19: A Systematic Review. Pharmaceutics. 2022; 14(5):1020. https://doi.org/10.3390/pharmaceutics14051020
Chicago/Turabian StyleFernández-Lázaro, Diego, Carlos Domínguez Ortega, Nerea Sánchez-Serrano, Fahd Beddar Chaib, David Jerves Donoso, Elena Jiménez-Callejo, and Saray Rodríguez-García. 2022. "Convalescent Plasma Therapy, Therapeutic Formulations of Repurposed Drugs in 20th Century Epidemics against COVID-19: A Systematic Review" Pharmaceutics 14, no. 5: 1020. https://doi.org/10.3390/pharmaceutics14051020